
Abstract
Psychosocial dimensions are essential to guarantee an optimal approach to improve emotional well-being in patients with cardiovascular disease (CVD). There is evidence of sex differences regarding these dimensions. Thus, the connections between them are crucial to implement personalized therapies. Network model analyses were conducted on data from 593 CVD patients. The models included scores from the Hospital Anxiety and Depression Scale (HADS), positive (PA) and negative affect (NA), positivity (PS), satisfaction of life (SLS), social support (SS), self-efficacy on emotion regulation (RESE), cardiac self-efficacy (CSE) and the Short Form-12 Health Survey. The main sex differences were found in: PA-PS (p = 0.03), SS-RESE (p = 0.04), for which the positive associations are stronger for men than for women and PA-RESE (p < 0.01) for which the positive association is stronger for women than for men. These nuances should be considered to implement tailored and integrative therapies for each CVD patient.
Introduction
One of the goals in the United Nations 2030 Agenda for Sustainable Development is the reduction of premature deaths associated with poor cardiovascular health in the population (Collins et al., 2018), as cardiovascular disease (CVD) is the leading cause of death worldwide, according to the European Society of Cardiology (Timmis et al., 2018). The origins and subsequent evolution of CVD are due not only to genetic or biological factors, but also to other aspects that can be modifiable by changing habits (Greco et al., 2020) or attitudes (Kessing et al., 2016). Therefore, the psychological dimension is crucial to improve the mental as well as physical facets of quality of life for patients with CVD. For instance, in their meta-analysis, DuBois et al. (2015) have shown the correlation between positive emotions and the reduction of mortality in CVD, which is an unequivocal sign that both positive affect and maintaining a personal disposition towards positivity (Tabernero et al., 2021) can benefit psychological well-being and life satisfaction and, consequently, prognosis and cardiovascular health (CVH).
In this sense, Caprara and Steca (2005) presented an explanatory model of perceived health according to which self-efficacy beliefs, understood as confidence in one’s own ability to carry out a specific behavior at a specific time, are directly linked to emotional state, positivity or life satisfaction. Actually, the self-efficacy perceived for the regulation of affect and for the management of social relationships influences the well-being of individuals. Thus, those people who have greater confidence in their own ability or self-efficacy have greater resilience and when they encounter adversity are able to persist over time in their decision to adhere to treatments and healthy habits, which is necessary in the face of chronic diseases such as CVD (DuBois et al., 2015). Consistent with these findings, Maeda et al. (2013) related self-efficacy beliefs to manage symptoms associated with CVD. Research argues that women have greater self-efficacy to express and regulate positive emotions (Caprara and Steca, 2005), while self-efficacy to regulate negative emotions improves over time, whereas men have greater positivity, which allows them to maintain a better appraisal of both themselves and their life satisfaction.
Besides, several studies have showed that clinical manifestations of CVD (Grazzi et al., 2020) as well as care and outcomes (Humphries et al., 2017) differ significantly between men and women. Indeed, an inequality in the assessment of the disease and for the prescription of medication could exist (Hyun et al., 2017), leading to a possible underestimation of the risk of CVD in women (Gao et al., 2019), even when a greater risk of CVD has been associated with women in different countries and ethnicities (Harris et al., 2022; Walli-Attaei et al., 2022). Hence, the incorporation of a gender approach is required within current cross-cultural research designs and global public policies to define a tailored management of the CVH according to sex differences (Kouvari et al., 2020; Mensah and Fuster, 2022) and also to identify vulnerable groups who could benefit from adapted prevention strategies (Bolijn et al., 2022).
As mentioned, not only the biological substrate is relevant (Humphries et al., 2017), but also the psychosocial factors must be taken into consideration to cope with the sex differences in CVH. Specifically, research works dealing with psychological distress and CVH have demonstrated some sex differences. Women with CVD reported greater and more severe symptomatology of anxiety and depression than men with CVD (Allabadi et al., 2019; Serpytis et al., 2018). This fact is not surprising given that many studies corroborate a higher anxiety prevalence in women, which explain the inequality according to both biological and socialization factors (Farhane-Medina et al., 2022). Nonetheless, the findings on the link between depression and CVD depending on the sex are not conclusive (Möller-Leimkühler, 2007). Hence, although a corpus of literature deals with the comparison in isolated variables to check sex differences, further analysis on this topic is desirable. The advances in network model analysis permit us to explore the links among personality dispositions in emotion regulation and well-being to explain CVH in women and men.
As demonstrated in other issues of health psychology, network analysis provides valuable insight, for instance to understand affective disorders, from a new standpoint which is interested in the links between constructs rather than in the latent variables (Schmittmann et al., 2013). Actually, a network analysis perspective circumvents some problems inherent in making sense of diagnostic systems, for example, how to explain that specific constructs are the cause of their indicators. Besides, it is not based on the possible arbitrary nature of some formative models, since all groups of variables are empirically equally defensible, although some of them are more convenient for our purposes than others. This approach is becoming prominent in health psychology to examine anxiety and depression (Jurado-González et al., 2023; Zavlis et al., 2022) and to determine the most relevant variables to make the interventions more efficient (Elovainio et al., 2020; Stochl et al., 2019). Other applications of network analysis in psychology cover the research on personality disorders (Peters et al., 2022), addictive behaviors (Poon et al., 2022) or have aimed to incorporate the psychological aspects together with biomarkers in different diseases (e.g., Fried et al., 2020). Furthermore, although scarcely, between subject analysis have been carried out to compare different populations, foe example, to study sex or gender differences (Lee et al., 2023; Rucci et al., 2021), differences linked to the history of parental psychological abuse (Wang et al., 2021) or maltreatment (Su et al., 2023), among others. The use of a holistic approach in the treatment of the data will allow us to have a global view of the multiple interactions between psychosocial variables that will help us to understand CVH and the strength of individual, group, or social differences.
To our knowledge, the study of sex differences, in terms of emotion regulation and psychological well-being associated to CVH, by using this approach has never been explored to date. This is the main contribution of the present paper, where data from a CVD population has been analyzed. The objective is twofold, firstly to build a network model containing variables related to emotions, which have shown to play an important role in the psychological well-being of CVD patients, such as positivity or self-efficacy, and to verify the invariance of the model when the same measurements are taken several months later. Secondly, to check the sex differences in the model to explore the links among depressive, anxious symptoms, global health, and psychosocial factors.
Materials and method
Sample
This study included 593 CVD patients (64.75 ± 9.07 years), 85 women, recruited from the Cardiology Unit of the University Reina Sofía Hospital (Cordoba, Spain) using a convenience sampling method. The inclusion and exclusion criteria as well as the detailed sample characteristics can be found in Delgado-Lista et al. (2022). Sociodemographic variables, such as educational level or socioeconomic status, were not required for the present study, since the aim was to obtain relationships between emotional and psychosocial factors associated with perceived health. Patients who had already suffered a first cardiac event and were diagnosed with an established coronary heart disease, such as unstable coronary disease, acute myocardial infarction, chronic coronary disease, or hospitalization for unstable angina, were included. In contrast, CVD patients who had experienced a clinical event, in the last 6 months (e.g., complications in the CVD or an eating disorder) that prevented them from following a long-term dietary intervention, which was the focus of the main study in which the patients were participating, were excluded.
Procedure
A longitudinal study was designed with data collection at two points in time over a 9-month interval (starting in January 2017), all in order to test the reliability of the model and the possible evolution of the results. Participants were contacted from the hospital where they had their medical history associated with CVD. Their participation was voluntary and to ensure anonymity the data were not linked to their history. The participants were informed of the objective of the study, after which they signed an informed consent form. The data were collected in a hospital ward through a battery |of questions presented by a member of the research team on a tablet, taking an average of 60 minutes.
All procedures contributing to this work comply with the ethical standards on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study was approved by the Andalusian Health Service’s Research Ethics Committee and the Reina Sofía Hospital in June 2015 (Act 242, Ref. 2886, 29 June 2015).
Measurements
A battery of questionnaires was administered to the participants to assess psychological well-being and emotion regulation.
• Positive and Negative Affect Schedule (PANAS, Watson et al., 1988). A brief, 10-item version validated to Spanish population by Tabernero et al. (2019) was used to evaluate positive affect (PA, 5 items, e.g., “enthusiastic”) and negative affect (NA, 5 items, e.g., “afraid”). Participants indicated the frequency of their experience of each affect ranging from 1 (totally disagree) to 5 (totally agree). In the current sample, Cronbach’s values for reliability were adequate, α = 0.79 (PA) and α = 0.83 (NA).
• Positivity Scale (PS, Caprara et al., 2012). This scale evaluates the tendency to interpret life and vital experiences from a positive perspective. It is a unidimensional scale that contains 8 items (e.g., “I have great faith in the future”) ranging from 1 (strongly disagree) to 5 (strongly agree). A higher score indicates greater positivity. Previous studies have reported adequate internal consistency in different countries (Caprara et al., 2008), including Spain, with a Cronbach’s α = 0.81. In the current sample, Cronbach’s value for reliability was adequate, α = 0.76.
• Cardiac Self-Efficacy scale (CSE, Maeda et al., 2013) was administrated to assess the patient’s degree of confidence in the own abilities to follow treatment recommendations such as diet or exercise (Maeda et al., 2013). In this work, a brief 10-items version was used, ranging from 1 (no confidence) to 7 (total confidence), for example, “How confident I was in my ability to take my medication.” It is a unidimensional scale with higher scores indicating higher self-efficacy, with a Cronbach’s α = 0.87. In the current sample, internal consistency reliability was adequate, Cronbach’s α = 0.79.
• Regulatory Emotional Self-Efficacy Scale (RESE, Caprara and Gerbino, 2001) was used to evaluate the perceived self-efficacy in managing negative and expressing positive affect. Participants responded to their capability to manage emotions along 12-items from the Spanish version Caprara et al. (2008), ranging from 1 (not well at all) and 7 (very well) to evaluate the self-efficacy for both, express positive and manage negative affect, for example, “How confident are you that you can express joy when good things happen to you?” or “How confident are you that you can avoid discouragement in the face of difficulties?” The global scale with higher scores indicating higher regulatory self-efficacy with an adequate internal consistency, in both the original study and the current sample, Cronbach’s α = 0.89 and 0.90, respectively.
• Brief Resilience Scale (BRS, Smith et al., 2008) was administrated to evaluate the capacity of the individual to recover from adversity. The scale was development along 6-items ranging from 1 (strongly disagree) to 5 (strongly agree), for example, “I tend to bounce back quickly after hard times.” The relevance of resilience to guarantee well-being in chronic disease had been demonstrated previously (Kim et al., 2019). In the current sample, internal consistency reliability was adequate, Cronbach’s α = 0.79.
• Satisfaction with Life Scale (SLS, Diener et al., 1985) is an instrument psychometrically suitable to use in patients with CVD (Apers et al., 2016). Participants respond to 5-items (e.g., “In most ways life is close to my ideal”) ranging from 1 (strongly disagree) to 7 (totally agree), with higher scores indicating higher global life satisfaction. Cronbach’s α = 0.86.
• Hospital Anxiety and Depression Scale (HADS, Bjelland et al., 2002) is a self-administered 14-items scale that allows the evaluation of psychological well-being. The Spanish validation from Terol-Cantero and Cabrera-Perona (2015) has been employed to assessed the level of depression (HADS-Dep; e.g., “I feel as if I am slowed down”), and anxiety (HADS-Anx; e.g., “I get sort of a frightened feeling as if something awful is about to happen”) in patients with CVD. Every item, from the 7-items for each dimension, ranges from 1 (never) to 7 (every day). Cronbach α = 0.78 in HADS-Anx, α = 0.82 in HADS-Dep.
• The Social Support survey (MOS Social Support, Sherbourne and Stewart, 1991) was used to assess the perception of the availability of having someone nearby to provide help or emotional support when needed. The 6-items of the dimension assessing emotional/informational support relating to the degree to which a chronically ill patient perceives the availability of emotional or informational social support were administrated. The items asked How often is each of the following types of support available if you need it? For example, “Someone you can count on to listen to you when you need to talk” or “Do you have someone available to give you good advice about a problem?” Responses were expressed using a 7-point Likert-type scale ranges from 1 (never) to 7 (always). The reliability of the scale was adequate Cronbach α = 0.88.
• Short Form-12 Health Survey (SF-12) is a self-report questionnaire that assesses Health-Related Quality of Life (HRQoL), which has already used in CVD patients (Abu et al., 2018). The Spanish validation from Failde et al. (2010) was administrated in this study. It consists of 12 items measuring eight health domains: general health perceptions, physical functioning, vitality, social functioning, role limitations due to physical problems, bodily pain, role limitations due to emotional problems, and mental health. These domains are subdivided in a mental health component, for example, “have you had any problems with your work or other regular daily activities as a result of your emotional problem (such as feeling depressed or anxious)?” and a physical health component, for example, “Does your health now limit you in walking several blocks?” From the 12 items, eight use a 5-point Likert-type scale and the other four are dichotomous (yes/no response). Higher scores indicate better HRQoL, the scale showed an adequate internal reliability, Cronbach α = 0.85, where the physical and mental health components also showed adequate indices, α = 0.85 and 0.78, respectively.
Network model analysis
For the statistical analyses, R version 4.03 was used. The models were represented by network graphs, where “nodes” refers to the measured variables, and the “edges” represent the correlations between them (Epskamp and Fried, 2018). The illustrations of the networks were made by JASP v.14.
Network estimation: The statistical parameters were computed using the Fruchterman–Reingold algorithm from the qgraph R-package (Epskamp et al., 2012) and the mixed graphical model (MGM) from the mgm R-package (Haslbeck and Waldorp, 2020). The MGM estimation employs the least absolute shrinkage and selection operator (LASSO) (Tibshirani, 1996), which consists of a penalty approach in order to control for spurious associations which would lead to false-positive finding. LASSO reduces smaller edges to zero. The procedure chooses the most adequate network according to the Extended Bayesian Information Criterion (EBIC) (Foygel and Drton, 2010), setting its hyperparameter to default (γ = 0.5) to ensure a more conservative network estimation.
Network inference: The bootnet R-package was used to check the stability of the centrality (nodes) and edge weight values. The two models corresponding to men and women populations were compared by means of the network comparison test (NCT) from the NetworkComparisonTest R-package (Van Borkulo et al., 2022), by using 100 permutations. NCT assesses for differences in terms of global strength (summed edge-weights of the networks), and structural invariance (statistically significant changes in the relations between variables).
Results
Objective 1: Network model invariance over time
At baseline (first measure), the sample was composed of 593 patients, and at follow-up (second measure after 9 months) of 323 CVD patients, who have responded the full questionnaire (54 women participated in the follow-up). The networks for the first and second measures were compared in order to verify the stability of the model.
The two networks did not differ significantly neither in their Global Strength (GS) values (4.798 for the first measure and 4.646 for the second measure; S = 0.1523; p = 0.68) nor in the structure, since the test was not significant (M = 0.1290; p = 0.77). Regarding the centrality invariance test, no differences were evidenced in expected influence, whereas HADS-Depression showed significant differences in strength (p = 0.02), showing a higher value for the first measure. According to the edge invariance test, only one edge or association was at the point of significance, Cardiac Self-Efficacy—Satisfaction of Life (p = 0.05).
Given these results, the stability of the network can be assumed and further analysis will be based on the first measure time, including the study on sex differences. Overall, the variables showing the highest values of strength were HADS-Depression (1.298) and Positivity (1.207). The strongest associations were found for the edges: Negative Affect—HADS-Anxiety (r = 0.347), and Positive Affect—Positivity (r = 0.310).
Objective 2
The networks belonging to men and women were compared in order to verify the differences. In Figure 1, the networks obtained are depicted on a string layout (sparsity = 0.345 for both of them). By visual inspection, some potential differences can be remarked. For instance, the edges Social Support—Cardiac Self-Efficacy, Regulatory Emotional Self-Efficacy—HADS-Depression, or Satisfaction of Life—HADS-Depression. Indeed, the invariance tests are close to be significant both for Global Strength (S = 0.6423; p = 0.07; reaching 4.832 for men and 4.189 for women) and Network Invariance Test (M = 0.3277; p = 0.06).
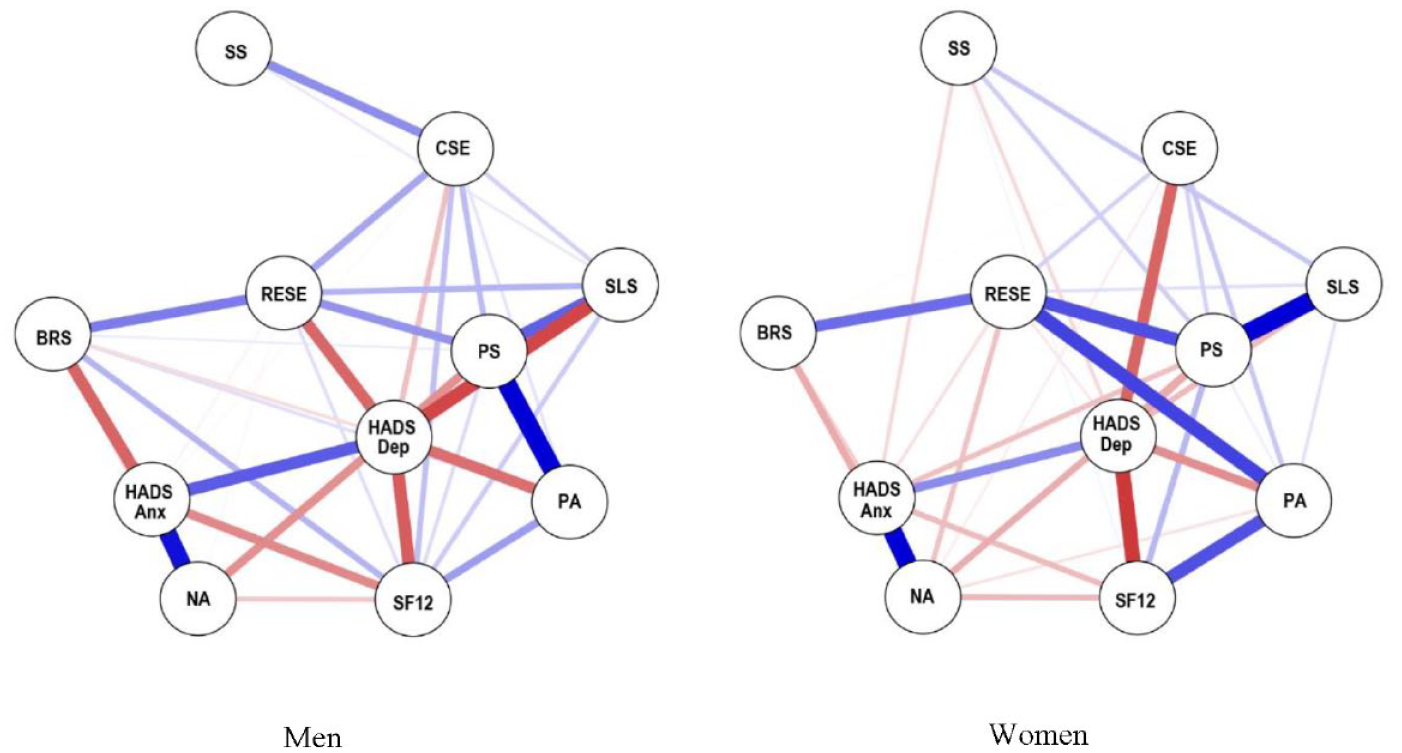
Network models for male (left) and female (right) CVD patients taking from the 1st measure time. Blue traits correspond to positive relation; red traits correspond to negative relations. PA : Positive Affect; NA : Negative Affect; PS: Positive Scale; CSE: Cardiac Self-Efficacy; SS: Social Support; RESE: Regulatory Emotional Self-Efficacy; BRS: Brief Resilience Scale; SLS: Satisfaction of Life Scale; HADS-Anx: Hospital Anxiety and Depression Scale – Anxiety factor; HADS-Dep: Hospital Anxiety and Depression Scale – Depression factor; SF12: Short Form-12 Health Survey.
Regarding the centrality values on the nodes, some minor differences are found in the strength, depicted in Figure 2. The nodes showing the highest strength values are Positivity and HADS-Depression for both sex, although in alternated order, taking the third position the Regulatory Emotional Self-Efficacy for women (with almost identical value than men) and Global Health (SF-12) for men. However, according to the invariance test, only a significant difference has been found in the expected influence for Cardiac Self-Efficacy (p = 0.02) being higher for men.

Strength values for every node in the network models from Figure 2. PA : Positive Affect; NA: Negative Affect; PS: Positive Scale; CSE: Cardiac Self-Efficacy; SS: Social Support; RESE: Regulatory Emotional Self-Efficacy; BRS: Brief Resilience Scale; SLS: Satisfaction of Life Scale; HADS-Anx: Hospital Anxiety and Depression Scale – Anxiety factor; HADS-Dep: Hospital Anxiety and Depression Scale – Depression factor; SF12: Short Form-12 Health Survey.
Note that these centrality values show the importance of the node for the network structure and they do not necessarily correlate with the obtained scores in the scales.
According to the edge invariance test (i.e., the invariance of the relationships between variables), three relationships show significant sex differences: Positive Affect—Positivity (p = 0.03), which is stronger in men than women; Positive Affect—Regulatory Emotional Self-Efficacy (p < 0.01), which is stronger in women than men, and, surprisingly, a significant difference was also found in the edge Social Support—Regulatory Emotional Self-Efficacy (p = 0.04), but the correlation values are too low to be represented in the network by using the by default options in JASP (edge size = 1 and min = 0, rounded at 0.0001), being higher for men than women. Besides, the edge Cardiac Self-Efficacy—Global Health was close to significance (p = 0.08), reaching higher values for women.
Discussion
In this work, the interrelation in differences individual abilities to cope with negative experiences, self-efficacy, emotion regulation skills and negative affect or depressive/anxious symptoms has been explored in CVD patients. The analysis focused on the differences between women and men raised by a network analysis.
Firstly, the stability of the model within two different moments, separated by 9 months, is corroborated, despite the potential progress of the CVD. This finding is in agreement with the results of other research by using clustering according to the perceived quality of life of patients with CVD (Castillo-Mayén et al., 2021).
Regarding sex differences, the comparisons did not reveal significant differences in terms of node centrality between women and men in the core nodes, for example, the relevance of the main dispositions shaping the magnitude of relationships, is similar in both sexes. In contrast, one of the psychological processes showing weaker influence on the network structure, with a less number of significant relationship (one of the least central nodes), corresponding to the cardiac self-efficacy, shows differences. It seems that this capacity is more linked (in a negative sense) with the depressive symptoms in women. These results could be influenced by the reinforcement of the emotion suppression and social expectation over men. They are expected to be strong and this role could have facilitated the development of resources to cope with these findngs, keeping higher self-efficacy (Stake and Eisele, 2010).
Despite the lack of statistical differences between groups according to our threshold (p = 0.05), there are differences that are observable in the network. The first result points out the importance of depressive symptoms and the positivity as the core of the network both for men and women. In the network analysis proposed by Everaert and Joormann (2019), the authors emphasized the link between both aspects, depression measured by the Beck Depression Inventory, and the positive reappraisal, which was related to affective, cognitive and somatic manifestations. Indeed, in our sample, positivity appears as the main disposition for women to form the other processes involved in the network, likely due to the stronger link to the emotional regulation and the satisfaction of life, which seems less connected in men. For men, the strongest dimension is depressive symptoms, whose negative relation with satisfaction of life is one of the most important in that network.
Following the two nodes mentioned above, the third strongest processes, for women is the regulatory emotional self-efficacy, whereas for men it is the global health. Nonetheless, the emotion regulation self-efficacy and the anxiety symptoms present similar level of strength. This important role of anxiety in men is interesting to note, since there is evidence supporting a higher prevalence of anxiety in women (Farhane et al., 2022). The influence of anxiety on the perception of global health in men is higher than in women suffering from CVD and, arguably, it can be explained, at least partially, by the psychosocial aspects linked to gender socialization. The different gender roles impact not only mental health, but also CVH, by hindering the acquisition and development of suitable and adaptive behaviours, thoughts and subjective feelings related to anxiety (Anyan and Hjemdal, 2018; Farhane et al., 2022).
The link between positivity and positive affect has been previously found in the literature. Alessandri et al. (2015) demonstrated that that positivity promotes positive affect and subsequently improves the subjective well-being and serves as a buffer to avoid depression and negative affect. However, this relationship is significantly higher for men than for women. In women, the positive affect is more strongly linked to the emotional regulation self-efficacy and, consequently, connecting in an indirect way the positivity to the positive affect. The relation between positive affect and emotional regulation has been stated in other works (Tabernero et al., 2021), while a deeper study on the positivity construct has been suggested (Luque et al., 2023), which could aid to understand the differences in pathways depending on sex.
Concerning the implication of social support in the network structure, according to the strength ranking, it seems that it does not participate significantly. This result may be surprising based on several findings in the literature (Anderson et al., 2006, 2007). For example, the rehabilitation interventions with social support have been found to be very helpful for cardiac patients (Caccamo et al., 2018) and a perceived weak social support has been associated with higher risk of cardiac events (Barth et al., 2010). Nevertheless, the statistical analysis suggest that social support is more important for men than women via the emotional regulation, whereas visually, social support seems to be linked with cardiac self-efficacy. Our results could suggest a slightly greater relevance of social support in men than women, but further analyses, maybe by employing other scales, are required to disentangle its actual influence in this network.
Finally, there is a construct that presents less strength than expected and, consequently it does not have a great influence on the psychological processes involved in the emotional well-being, which is the resilience. According to Hoorelbeke et al. (2019), resilience can play an important role via the reduction of depressive symptoms, but this link is not evident in the present network, since resilience is rather linked to emotional regulation or anxious symptoms. Although resilience is suggested to be beneficial to reduce severity of depression in young adults (Konradt et al., 2018), to establish the links to other variables in the CVD population, and particularly in women, remains challenging (Love et al., 2021).
This work presents some limitations. Firstly, the inequality on the simple size by sex, with a 6 to 1 ratio of male to female patients. This proportion of women has been found in many research works (e.g., Samayoa et al., 2018), which is consistent with the pattern of higher prevalence of CVD in men (Gao et al., 2019) and could hamper the generalization of the conclusions. In any case, the sample size is adequate for the number of nodes included in the networks and the bootstrapping technique allows for the extraction of more robust results.
An important issue that could be addressed in further works consists in the incorporation of biomarkers in order to estimate the mutual interaction in the network representing emotional well-being and CVH, and also to consider socioeconomic status and education level to assess their influence on health perception. On the same vein, a similar study in other chronic diseases, such as diabetes or hypertension could also provide valuable information, because this approach permits the capture of complex relationships and interactions between variables, provides a clear visual representation enhancing interpretability and identifies key variables (nodes) helping researchers pinpoint influential factors directly and focus on the most relevant factors linked to mental health in these conditions.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053241230263 – Supplemental material for Network analysis to examine sex differences linked to emotional well-being in cardiovascular disease
Supplemental material, sj-docx-1-hpq-10.1177_13591053241230263 for Network analysis to examine sex differences linked to emotional well-being in cardiovascular disease by Antonio R Hidalgo-Muñoz, Carmen Tabernero and Bárbara Luque in Journal of Health Psychology
Footnotes
Data sharing statement
Data are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Spanish Ministry of Economy and Competitiveness, grant number PSI2014–58609-R, and by the Spanish Ministry of Science, Innovation and Universities, grant number PDI2019-107304RB-I00/AEI/10.13039/501100011033.
Ethics approval
This study was approved by the Research Ethics Committee of the Servicio Andaluz de Salud and the Reina Sofia Hospital on 30 June 2015 (Acta 242, reference: 2886).
Informed consent
All participants provided informed consent prior to their participation in this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.