
Abstract
There is an increase in use of cosmetic procedures (CP) worldwide. Research suggests that people might develop addictive cosmetic procedures use (ACPU). We aimed to assess the prevalence of ACPU and explore associated risk factors. We collected cross-sectional data from a large sample of Jewish women in Israel aged 25–71 (N = 1614). We measured self-reported ACPU, personality measures (body- and self-esteem, attachment security), attitudes (feminism, anti-aging) and problematic social media use (PSMU). Among women who had CP (n = 710), 20% reported moderate-severe risk for ACPU during their lifetime and 15.4% in the past year. Multiple regression analyses indicated that higher ACPU was associated with lower body esteem and feminist attitudes and with higher PSMU. The association between body esteem and ACPU was primarily among women with higher PMSU. Findings indicate that ACPU is prevalent and emphasizes the importance of various risk factors, especially low body esteem and PSMU.
Introduction
In recent years there has been a steady worldwide increase in use of cosmetic procedures (CP; Triana et al., 2024). Motivations for using CP are various and may include desire to improve physical appearance, enhance self-confidence, or improve emotional wellbeing (e.g. Ashley et al., 2024; Małolepsza et al., 2023). However, these procedures may also involve physical or psychological complications (e.g. Aljerian et al., 2024; Jones et al., 2022). Moreover, there may be a component of addictive use in repeated CP (e.g. Gorbis and Kim, 2017; Shah et al., 2021; Wagenaar and Hermans, 2025). In the current study, we used a scale based on diagnostic criteria for addictive behaviors modified for CP (Shah et al., 2021) to examine the prevalence of the potentially addictive use of cosmetic procedures (ACPU) in the general population of Jewish women in Israel. We also tested several hypotheses regarding potential factors that may be associated with risk for ACPU. We focused on the role of low body esteem and problematic use of social media (PSMU) as well as other personality, attitudinal, and behavioral factors. By doing so, this study may advance the understanding of psychological aspects related to ACPU among women.
Addictive cosmetic procedures use
Cosmetic procedures refer to typically elective interventions, such as surgical procedures (e.g. liposuction), face and head procedures (e.g. facelift), body and extremities procedures (e.g. buttock lift) and nonsurgical procedures (e.g. botulinum toxin; e.g. Triana et al., 2024). According to the data of the International Society of Aesthetic Plastic Surgery, the overall increase in CP worldwide from 2019 to 2023 was 40% (Triana et al., 2024). Cosmetic procedures are increasingly common in Israel, but their overall prevalence is difficult to determine since many cosmetic treatments, particularly nonsurgical ones, are performed in private clinics and are not systematically recorded (Knesset Research and Information Center, 2022). Although esthetic medicine offers opportunities to enhance self-image, boost confidence, and improve overall quality of life (Małolepsza et al., 2023), there may also be a negative side to this phenomenon. Previous research indicates that undergoing repeated CP may represent potentially addictive behavior (e.g. Gorbis and Kim, 2017; Naheed and Yousuf, 2024; Shah et al., 2021; for a review see Wagenaar and Hermans, 2025), prompting calls to address “addiction in cosmetic dermatology” (Sharifi and Jafferany, 2026).
Addiction is characterized by compulsive pursuit and engagement in behaviors despite experiencing negative consequences (American Psychological Association (APA), 2023). While traditionally, addiction was associated with substances, in recent years there has been a growing number of behaviors that are considered addictive. For example, internet gaming and gambling are now formally categorized with substances in the International Classification of Diseases version 11 (World Health Organization (WHO), 2022, ICD-11). Additional behaviors such as compulsive sexual behavior, compulsive buying-shopping, and problematic use of social media may also be considered addictive behaviors (e.g. Brand et al., 2025). Similar underlying mechanisms tend to contribute to the development and maintenance of both substance-use disorders and addictive behaviors. This includes heightened reactivity and craving, compulsive motivations and habitual behaviors, and deficits in self-control (Brand et al., 2025), all of which may also serve as maladaptive coping mechanism for some individuals.
Based on this premise, Shah et al. (2021) developed a scale grounded in the DSM-5 diagnostic criteria for substance-related disorder to measure ACPU. Findings showed that 6.6% of participants in their study (American adults visiting a cosmetic dermatology clinic) met the criteria for moderate or severe risk of ACPU. It is therefore important to assess the prevalence of ACPU in different nations and cultures, as well as to identify risk and resilience factors associated with this potentially addictive behavior. In the following sections, we briefly review several key personality, attitudinal, and behavioral factors that may be related to ACPU: body esteem, self-esteem, feminist attitudes, attachment security, attitudes toward aging, and problematic social media use (PSMU).
Personality factors
Body esteem
Body image concerns are considered important factors influencing the decision to seek cosmetic treatments (e.g. Sarwer, 2019), with lower body esteem predicting greater use of these procedures (Pearlman et al., 2022; Sarwer, 2019). Dissatisfaction with one’s physical appearance may drive people to seek surgical interventions as a means to enhance self-image, self-confidence, and social acceptance (reviewed in Mironica et al., 2024).
A substantial body of research documented high prevalence rates of Body Dysmorphic Disorder (BDD) among individuals undergoing CP (Kaleeny and Janis, 2024; Salari et al., 2022), linking this disorder to more repeated use of these procedures (e.g. Gorbis and Kim, 2017). BDD is characterized by preoccupation with perceived defects in appearance and repetitive behaviors and/or mental acts aimed at reducing distress related to body image (American Psychiatric Association, 2022). However, the global rise in CP use highlights that repetitive and problematic engagement with such procedures is not limited to people with BDD.
Self-esteem
Global self-esteem may also be associated with ACPU. Self-esteem can serve as a resilience factor against ACPU, much like it buffers against other addictive behaviors (e.g. Köse and Doğan, 2019; Uba et al., 2013). Moreover, because self-esteem is related to body esteem (feelings about one’s appearance and physical condition, e.g. Olchowska-Kotala, 2018), concerns about self-worth might lead people to engage in more CP as a compensatory action to enhance their perceived value. Several studies have reported associations between CP use and lower self-esteem (e.g. Fares et al., 2019; Furnham and Levitas, 2012). Therefore, we examined whether lower self-esteem would be associated with higher prevalence of ACPU.
Attachment security
Another major personality factor related to resilience and self-image is the sense of attachment security (i.e. confidence in the availability of support when needed; Bowlby, 1973). This sense, which develops through interactions with supportive partners in times of need, has been shown to foster psychological stability, enhance resilience, and promote overall mental health (e.g. Mikulincer and Shave, 2016). Individuals with a strong sense of attachment security also tend to exhibit higher self-esteem (e.g. Schmitt and Allik, 2005), greater body esteem (e.g. Szalai et al., 2017) and lower rates of problematic substances use (e.g. Fairbairn et al., 2018; ) and behavioral addictions (e.g. D’Arienzo et al., 2019; Niu et al., 2023). Moreover, Davis and Vernon (2002) found that lower scores of attachment security were associated with greater use of CP among women. Thus, attachment security may serve as a protective factor against ACPU.
Based on this literature, we expected that lower levels of body esteem, self-esteem and attachment security would relate to higher levels of ACPU.
Attitudinal factors
Feminist attitudes
Feminist attitudes take on nuanced and complex forms that vary across cultural, sociopolitical, and historical contexts (Siegel and Calogero, 2021). Over the years, the feminist movement has evolved through several waves, with second-wave radical feminists viewing feminine beautification practices and CP as manifestations of patriarchal oppression and disempowerment (Heggenstaller et al., 2018). This perspective is grounded in the belief that beautifying the female body primarily serves to attract male approval through the male gaze. In contrast, more recent liberal feminist perspectives emphasize gender equality through collaboration with men and regard CP as a potentially empowering act through which an individual’s physical body can be brought into greater alignment with her inner sense of self (Heggenstaller et al., 2018). However, we still considered that feminist non-acceptance of classic gender roles may be associated with less ACPU, as it defines woman’s classic passive roles in society. Thus, we expected higher feminist attitudes to relate to lower levels of ACPU.
Attitudes toward aging
Attitudes toward aging may represent another influential factor in the decision to undergo cosmetic treatments. The desire to prevent or conceal signs of aging has been identified as a common motive for pursuing CP (for review, see Honelová and Vidovićová, 2023; Martinez et al., 2023). The perception of aging is often accompanied by fears of diminished attractiveness, which may further encourage individuals to seek cosmetic interventions (Honelová and Vidovićová, 2023). Accordingly, we assumed that negative attitudes toward aging may be associated with higher levels of ACPU.
Problematic social media use
Social media may play a crucial role in shaping individuals’ decisions to pursue cosmetic treatments, given its strong emphasis on appearance through images, videos, celebrity influence, advertisements, and interactive features, such as likes, comments, and shares (Arab et al., 2019; Mironica et al., 2024). Arab et al. (2019) found that watching cosmetic surgery–related material on social media, spending longer hours on these platforms, and experiencing negative self-perceptions while online were all associated with an increased likelihood of considering CP. Similarly, a meta-analysis revealed that individuals who spent more than 3 hours per day on social media were twice as likely to consider undergoing CP compared to those who used this platform less frequently (Rahman et al., 2024). On the other hand, women who had undergone breast augmentation surgery reported higher rates of PSMU than those who had not (Öztürk et al., 2021). Thus, there may be bidirectional links between PSMU and ACPU.
A growing body of research indicates that social media use can affect attitudes toward CP by negatively affecting body esteem (e.g. Dde Valle et al., 2021; Mironica et al., 2024; Mohammadi et al., 2023). Thus, social media usage and body image concerns may each contribute to ACPU, and they may also interact such that individuals with low body esteem who spend considerable time on social media might be especially vulnerable to ACPU. We therefore expected that higher levels of PSMU would relate to higher ACPU, especially among those with relatively low levels of body esteem, self-esteem and attachment security, and possibly low feminist attitudes.
Sociodemographic characteristics
Several sociodemographic factors may relate to CP use. Because the desire to prevent or conceal signs of aging is a common motivation to pursue cosmetic interventions (Honelová and Vidovićová, 2023; Martinez et al., 2023), it is important to examine age-related differences in ACPU. Other sociodemographic characteristics, such as economic status (Ahmadi et al., 2022) and religiosity (Furnham and Levitas, 2012), may also be relevant to attitudes toward, and engagement, in CP. Religious beliefs about body modification, sexuality, and science may discourage individuals from undergoing cosmetic interventions and thereby serve as protective factors against ACPU (e.g. Coyne et al., 2023; Muslu and Demir, 2020). We therefore expected higher religiosity to relate to lower levels of ACPU.
The current research
The goal of the current study was to examine the prevalence of ACPU in a general population sample of Jewish women in Israel and explore associated risk and protective factors. We focused specifically on women, as they constitute the majority of CP clients (Alotaibi, 2021).
First, we examined the prevalences of ACPU in the general sample and among women who had procedures. We also examined ACPU distribution and associations with age, economic status, and religiosity.
Second, considering the substantial increase in CP use and the emerging research exploring its potentially addictive aspects, we examined associations between ACPU and an array of personality, attitudinal, and behavioral factors. Based on the literature review, we hypothesized that women who report more ACPU would report:
(1) Lower personality-level resilience in terms of (a) lower body esteem, (b) lower self-esteem, and (c) lower attachment security;
(2) lower feminist attitudes (higher passive acceptance of gender roles);
(3) more negative attitudes toward aging;
(4) higher levels of PSMU.
Furthermore, given that the relationship between social media and attitudes toward CP is often related to body-esteem concerns (e.g. de Valle et al., 2021; Mironica et al., 2024; Mohammadi et al., 2023), we also hypothesized that:
(5) body esteem and PSMU may interact to contribute to ACPU. Specifically, we expected that women with low body esteem and high levels of PSMU would exhibit more ACPU compared to those with high body esteem or low levels of PSMU. We also examined whether other assessed variables, such as global self-esteem, attachment security, and feminist attitudes, may moderate the association between PSMU and ACPU.
The five hypotheses are summarized in the conceptual model presented in Figure 1.
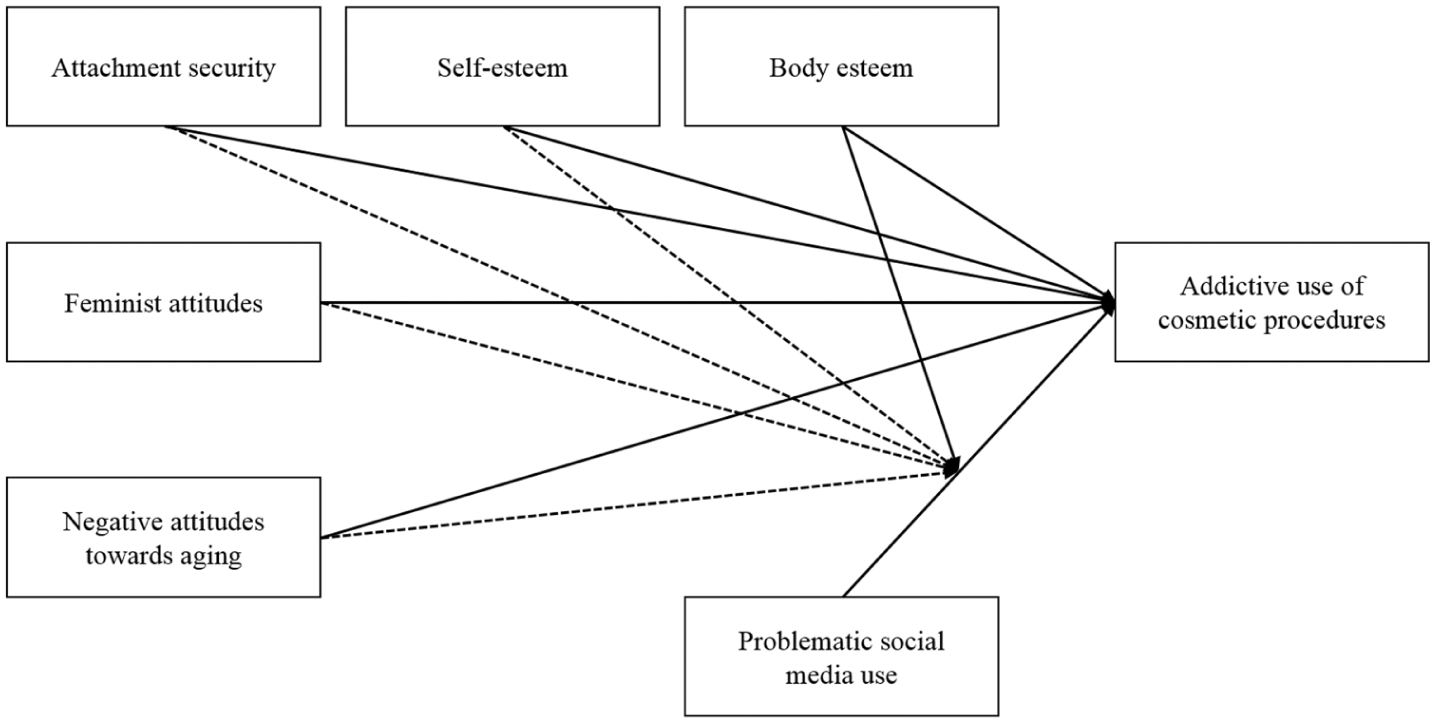
Conceptual model of study predictions.
Method
Transparency and openness
The study materials, code and anonymized data are publicly available at https://osf.io/349xn/overview.
Participants
The sample was constructed to match prevalence of age and religiosity to the adult women Jewish population in Israel (Israel Central Bureau of Statistics, 2024). Cross-sectional data were collected online during February 13–20, 2025. Inclusion criteria were being Jewish Hebrew speaking Israeli women aged 25–71. Participants were recruited from a diverse Web panel of individuals who participate in surveys for monetary compensation (i.Panel). After removing responses with missing data, failed attention checks, responded non-seriously (under 5 on a scale from 1 = not at all seriously, to 9 = totally seriously) or had other technical issues (n = 1143), the final sample included 1614 women (Mage = 45.71, SD = 12.99) with complete data (no missing value in any of the measures). Of these, 710 women reported undergoing CP in the past (Mage = 46.50, SD = 12.73). Demographic information of the sample and information of the CP history among women who undergone CP is presented in Appendix 1, Tables S1 and S2, of Supplemental Materials. A sensitivity power analysis using G*power (Faul et al., 2009) indicated that we could detect a very small effect size (f2 = 0.02) at 80% power in a hierarchical linear regression with the nine key variables and 12 total variables (including potential covariates).
Procedure
The study was approved by the Institutional Review Board at Reichman University, protocol number P_2025019. The survey was conducted online via the Qualtrics platform at a time and place of participants’ convenience. After providing electronic informed consent, participants answered questions regarding age, religiosity, and CP history (Shah et al., 2021). Participants who reported ever having CP (n = 710), completed a questionnaire regarding ACPU (Shah et al., 2021). All participants received a battery of self-report questionnaires measuring PSMU, self-esteem, body esteem, attachment security, feminist attitudes, and risky substance use. Part of the sample (n = 407) also received a questionnaire tapping attitudes toward ageing. 1 Finally, participants answered demographic questions (education level, family status, having children, economic status, perceived physical health). They were probed for attention and debriefed.
Materials
To measure ACPU, we used the Cosmetic Addiction Scale DSM-5 (CAS-DSM; Shah et al., 2021; Appendix 2 Table S3 of Supplemental Materials) – a self-report scale adapted from DSM-5 substance-use disorder criteria and modified for CP. This measure consists of one CP-history screening question, and 11 items assessing indicators/symptoms of ACPU (e.g. “Wanted to cut down on or stop having cosmetic procedures but couldn’t?”), with “yes” (1) or “no” (0) answers. In the current study, questions were phrased regarding lifetime experiences. We added a final question asking if the symptoms reported were also experienced in the last year (yes, no). In line with prior research, we computed a total score for each participant by summing up answers to the 11 items, with higher scores indicating more ACPU (α = 0.93). A score of 2–3 indicated mild, 4–5 moderate, and ⩾6 severe ACPU (Shah et al., 2021).
Personality factors
Body esteem was measured using the Appearance subscale of the Body-Esteem Scale for Adolescents and Adults (Mendelson et al., 2001). The subscale consists of 10 items assessing general feelings about individual appearance (e.g. “I like what I look like in pictures”: 1 = never, 5 = always). One item was removed from the analysis due to a typo and relatively low inter-item correlations. A total score was computed by averaging the responses to the remaining nine items, with higher scores indicating higher body-esteem (α = 0.91). Self-esteem was measured using the single self-report item (I have high self-esteem; Robins et al., 2001; 1 = not very true of me, 7 = very true of me), with higher scores indicating higher self-esteem. Attachment security was measured with the Security subscale of the State Adult Attachment Measure (Gillath et al., 2009). This self-report measure contains 7 items (e.g. “I feel loved”; 1 = disagree strongly, 7 = agree strongly). Scores were averaged, with higher scores indicating greater attachment security (α = 0.96).
Attitudinal factors
Feminist attitudes were measured with the Passive Acceptance subscale of the Feminist Identity Development Scale (Bargad and Hyde, 1991). This subscale consists of 12 items assessing individual’s acceptance of gender-role stereotypes (e.g. “I do not want to have equal status with men”; 1 = strongly disagree, 5 = strongly agree). Two items were removed from the analysis due to low inter-item correlations. Scores were averaged, with higher scores indicating greater non-acceptance of the gender-role stereotypes – that is, higher propensity to feminist attitudes (α = 0.85).
Attitudes toward aging were measured with 7 items from two subscales of the Attitudes to Aging Questionnaire (Laidlaw et al., 2007). We selected items which reflect individuals’ attitudes toward aging in general (not based on personal experience): Three items from the psychosocial loss subscale (e.g. “old age is a time of loneliness”) and four items from the psychological growth subscale (e.g. “wisdom comes with age”; 1 = strongly disagree. 7 = strongly agree, reverse coded). One item was removed due to low inter-item correlations. Scores were averaged, with higher scores indicating more negative attitudes toward aging (α = 0.76).
Problematic social media use
To measure PSMU we used the Bergen Social Media Addiction Scale (BSMAS; Andreassen et al., 2016). This scale contains 6 items assessing the frequency of problematic social media behaviors in the past 12 months (e.g. “you feel the urge to use social media more and more”; 1 = very rarely, 5 = very often). A mean score was computed, with higher scores indicating greater PSMU (α = 0.86).
Results
Descriptive statistics of CAS-DSM prevalences
We first assessed distribution of the CAS-DSM score categories – no-symptom, mild, moderate, severe ACPU (Shah et al., 2021). Then, we present the means of the continuous CAS-DSM score and the percentage of women who reported moderate-severe levels of ACPU (defined as total CAS-DSM score ⩾ 4) during lifetime and in the past year. We did this for the general sample (N = 1614) and among women who ever had procedures (N = 710; “subsample”).
Table 1 presents the distribution of severity of ACPU (in the CAS-DSM score) for lifetime and past year among women who had underwent CP (N = 710). Among women who had underwent procedures, 20% reported moderate-severe ACPU during lifetime and 15.4% reported that their answers reflect symptoms during the past year.
Distribution of severity of ACPU by the CAS-DSM categories, for lifetime and past year, among women who had underwent cosmetic procedures (n = 710).
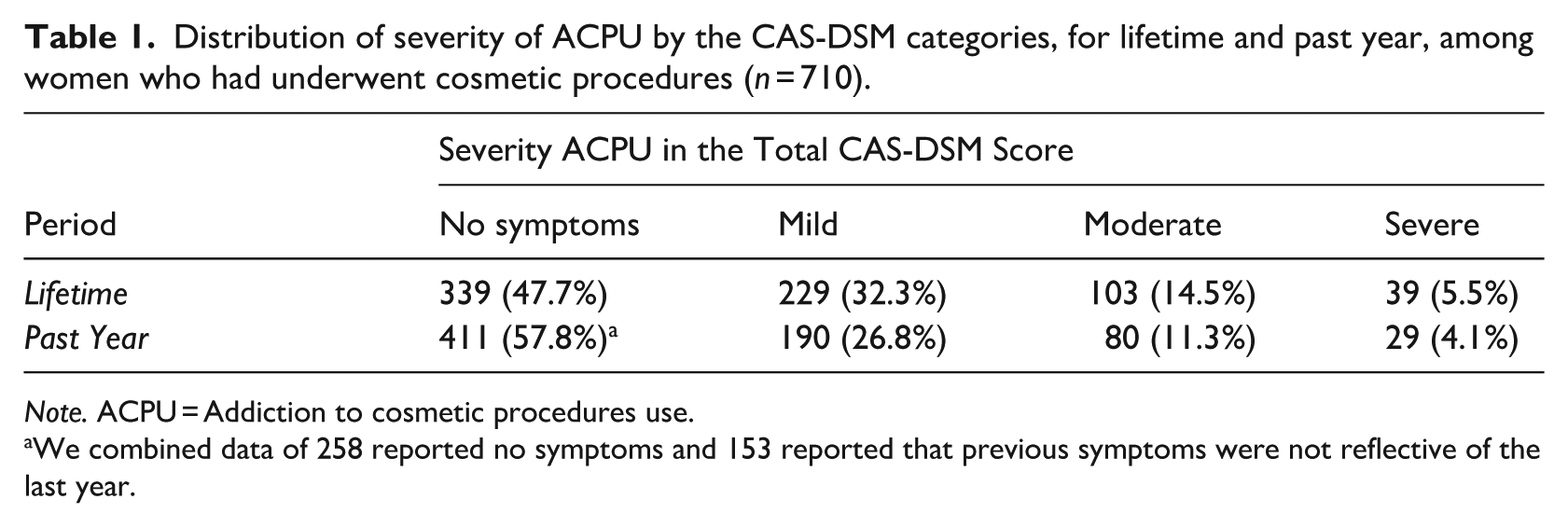
Note. ACPU = Addiction to cosmetic procedures use.
We combined data of 258 reported no symptoms and 153 reported that previous symptoms were not reflective of the last year.
Table 2 presents descriptive statistics for the continuous CAS-DSM score and percentage of women showing moderate-severe ACPU in the whole sample and subsample of women who had undergone CP. As shown in Table 2, the percentage of women in the whole sample that reported moderate-severe ACPU was 8.9% during lifetime and 6.8% in the past year. Positive correlations were found between the CAS-DSM score and the number of cosmetic interventions participants underwent in the whole sample and subsample (see Table 3).
Descriptive statistics for the continuous CAS-DSM score and percentage of women showing moderate-severe ACPU in the CAS-DSM.
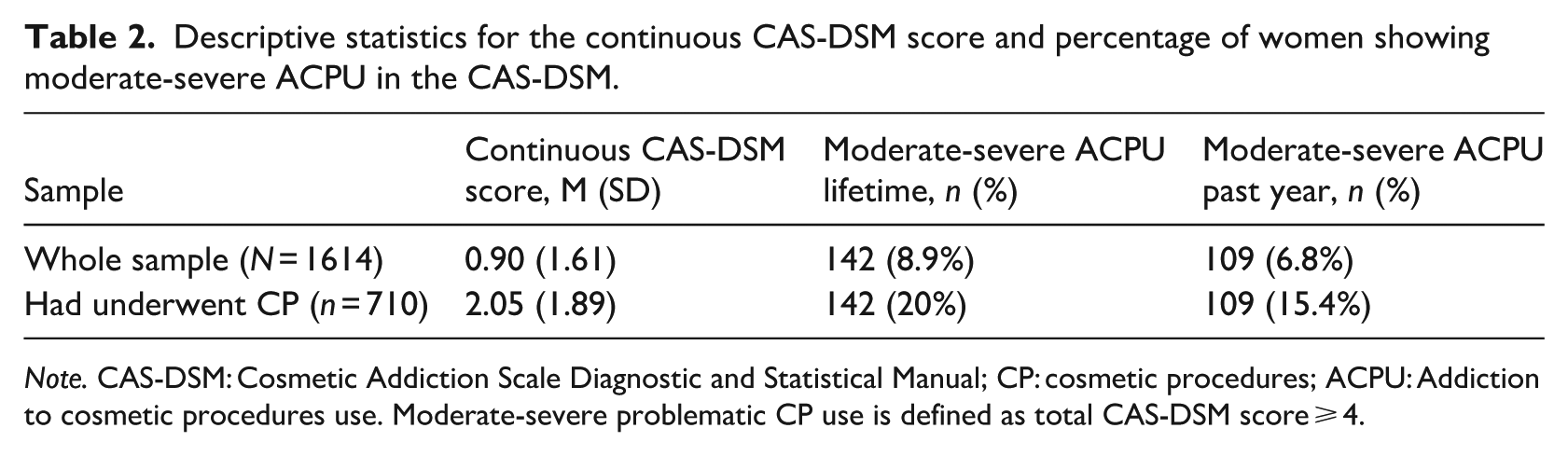
Note. CAS-DSM: Cosmetic Addiction Scale Diagnostic and Statistical Manual; CP: cosmetic procedures; ACPU: Addiction to cosmetic procedures use. Moderate-severe problematic CP use is defined as total CAS-DSM score ⩾ 4.
Descriptive statistics and Spearman Rank-Order correlations of key measures in the whole sample (below the diagonal, N = 1614) and subsample of women who had procedures in the past (above the diagonal n = 710).
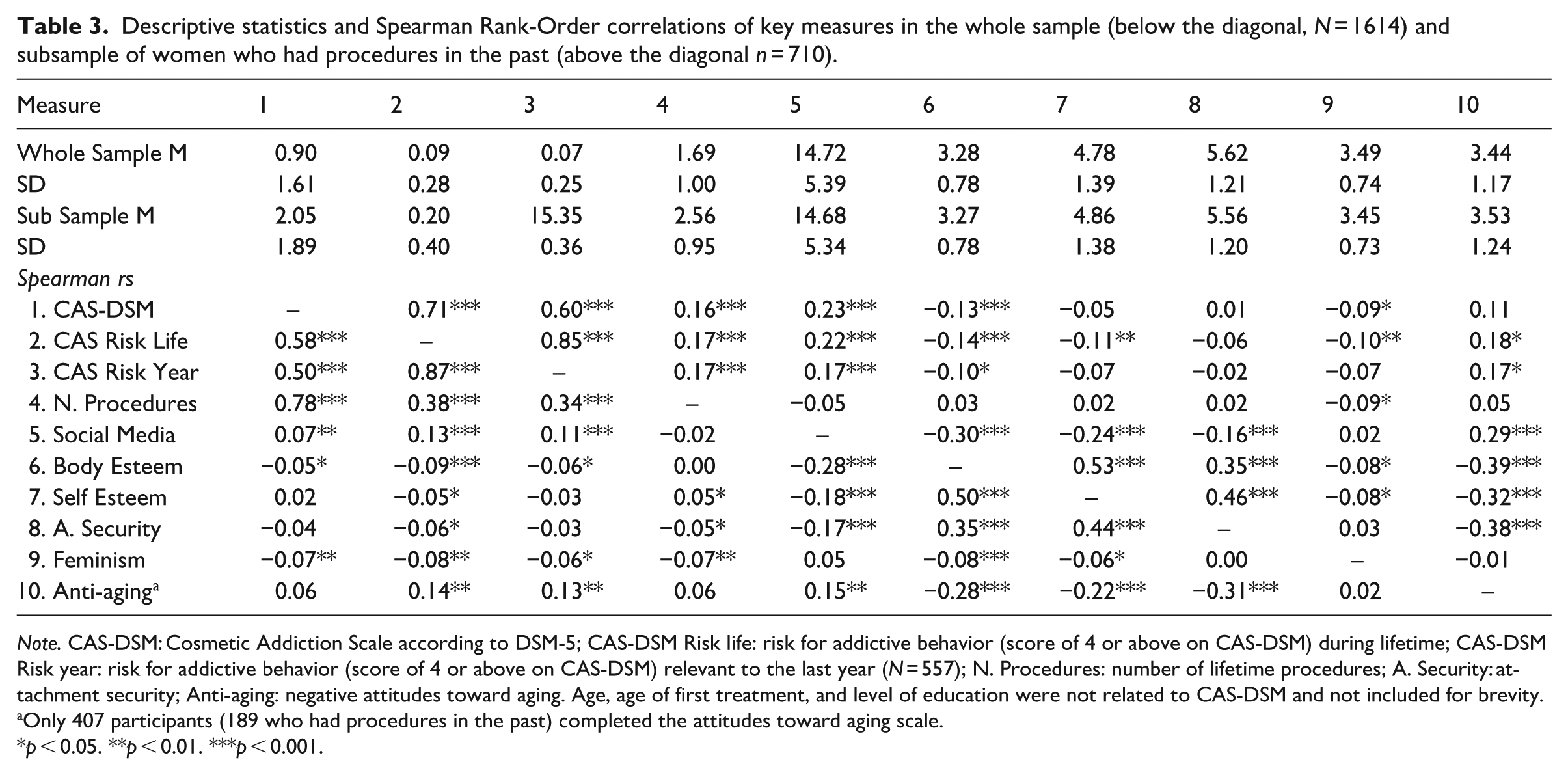
Note. CAS-DSM: Cosmetic Addiction Scale according to DSM-5; CAS-DSM Risk life: risk for addictive behavior (score of 4 or above on CAS-DSM) during lifetime; CAS-DSM Risk year: risk for addictive behavior (score of 4 or above on CAS-DSM) relevant to the last year (N = 557); N. Procedures: number of lifetime procedures; A. Security: attachment security; Anti-aging: negative attitudes toward aging. Age, age of first treatment, and level of education were not related to CAS-DSM and not included for brevity.
Only 407 participants (189 who had procedures in the past) completed the attitudes toward aging scale.
p < 0.05. **p < 0.01. ***p < 0.001.
Additional analyses indicated that there were no differences in CAS-DSM scores or risk category prevalence (lifetime or past year) across the different age groups (young adults, 25–39; adults, 40–54; older adults, 55–71), Fs < 1.27, ps > 0.282. For the religious categories (ultra-orthodox, religious, traditional, secular), there was a statistically significant difference in the whole sample in lifetime (but not past-year) CAS-DSM scores, F(3, 1610) = 11.66, p < 0.001, ηp2 = 0.021, and lifetime (but not past-year) risk category prevalence, F(3, 1610) = 4.17, p = 0.006, ηp2 = 0.008. Traditional women reported higher CAS-DSM scores and risk-prevalence than secular women and both were higher in CAS-DSM scores than religious and ultra-orthodox women (see Appendix 3, Figures S1 and S2, of Supplemental Materials). These differences were not statistically significant in the subsample of only women who had CP.
Zero-order correlations
Preliminary analyses indicated that CAS-DSM scores were not normally distributed (Skewness = 12.14, Kurtosis = 6.47), as most indexes of addictions. We therefore used Spearman Rank-Order correlations to investigate zero-order correlations, and applied bootstrapping with 5000 resamples to our regression analyses.
Means, SDs, and (non-confirmatory) zero-order correlations of the continuous CAS-DSM score and lifetime and past-year risk category and the assessed personality, attitude, and behavioral factors are presented in Table 3. As predicted, the CAS-DSM score and both lifetime and past-year risk category prevalences were significantly associated with lower body esteem and higher levels of PSMU in both the total sample and the subsample of women who had underwent CP. There were also small-sized correlations of ACPU with lower self-esteem (only in the subsample), lower attachment security (only lifetime risk), lower feminist attitudes, and more negative attitudes toward aging (see Table 3). Age and education were not significantly associated with CAS-DSM continuous or categorical scores. All these correlations were the same, only of larger magnitude in the subsample of women who had underwent CP.
Regression analyses
To test Hypotheses 1–4, we conducted hierarchical multiple regressions examining the individual contribution and potential interactions between personality, attitudinal, and behavioral factors (mean centered at +1 and −1 SD) to CAS-DSM score. To better account for non-linearity and reduce Type 1 error, we used bootstrapping with 5000 resamples for 95% Confidence Intervals.
As detailed in Table 4, these analyses indicated that in both the whole sample and subsample of those who had underwent CP, only body esteem, PSMU, and feminist attitudes, had significant unique associations with CAS-DSM scores. Self-esteem and attachment security were not statistically significant in these inclusive models. Parallel analyses indicated that attitudes toward aging were not related to CAS-DSM scores in the full sample, b = 0.14, t(400) = 1.83, p = 0.068, β = 0.09, and subsample, b = 0.14, t(182) = 0.76, p = 0.446, β = 0.06.
Multiple regression for CAS-DSM scores as a function of key study variables in the whole sample (N = 1614) and subsample of women who had procedures in the past (n = 710).
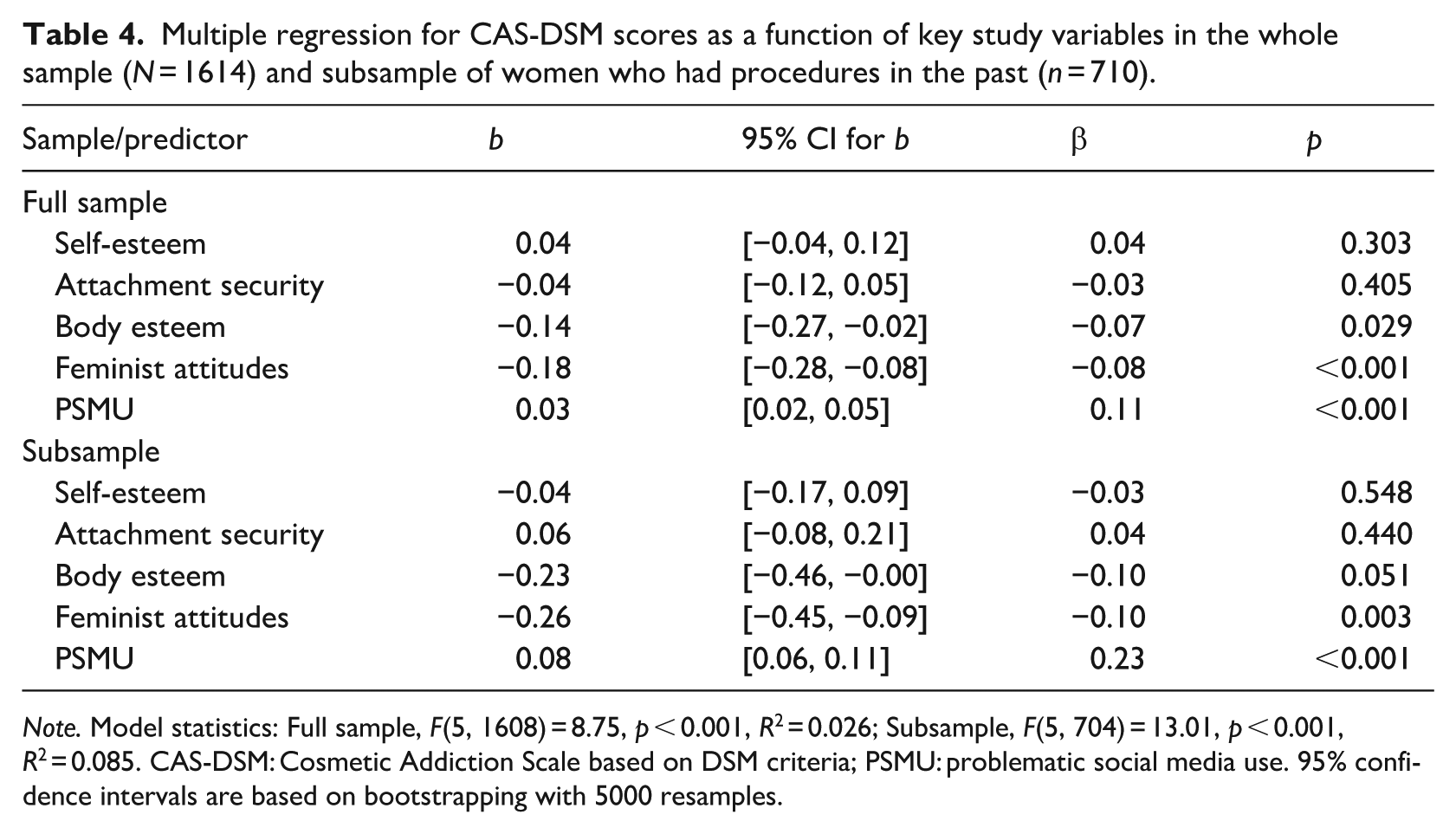
Note. Model statistics: Full sample, F(5, 1608) = 8.75, p < 0.001, R2 = 0.026; Subsample, F(5, 704) = 13.01, p < 0.001, R2 = 0.085. CAS-DSM: Cosmetic Addiction Scale based on DSM criteria; PSMU: problematic social media use. 95% confidence intervals are based on bootstrapping with 5000 resamples.
Next, we proceeded to examine Hypothesis 5, regarding the interactive contribution of body esteem and PSMU (mean centered at +1 and −1 SD) on CAS-DSM scores in a hierarchical regression analysis (for the whole sample and for the subsample of women who had underwent CP). We repeated this test while controlling for variables that were significantly associated with the key variables in the regression – feminist attitudes and number of lifetime procedures – as covariates in the model (initial analyses indicated no interactions with feminism or number of lifetime procedures; other variables were not statistically significant moderators or covariates).
As detailed in Table 5, these analyses yielded statistically significant regression models, for both the first and second regression steps, in the whole sample and in the subsample of women who had CP. In both samples, there were statistically significant main effects for PSMU and body esteem (marginally significant), and a statistically significant two-way interaction between PSMU and body esteem.
Hierarchical regression for CAS-DSM scores as a function of problematic social media use and body esteem (mean centered) in the whole sample (N = 1614) and subsample of women who had procedures in the past (n = 710).
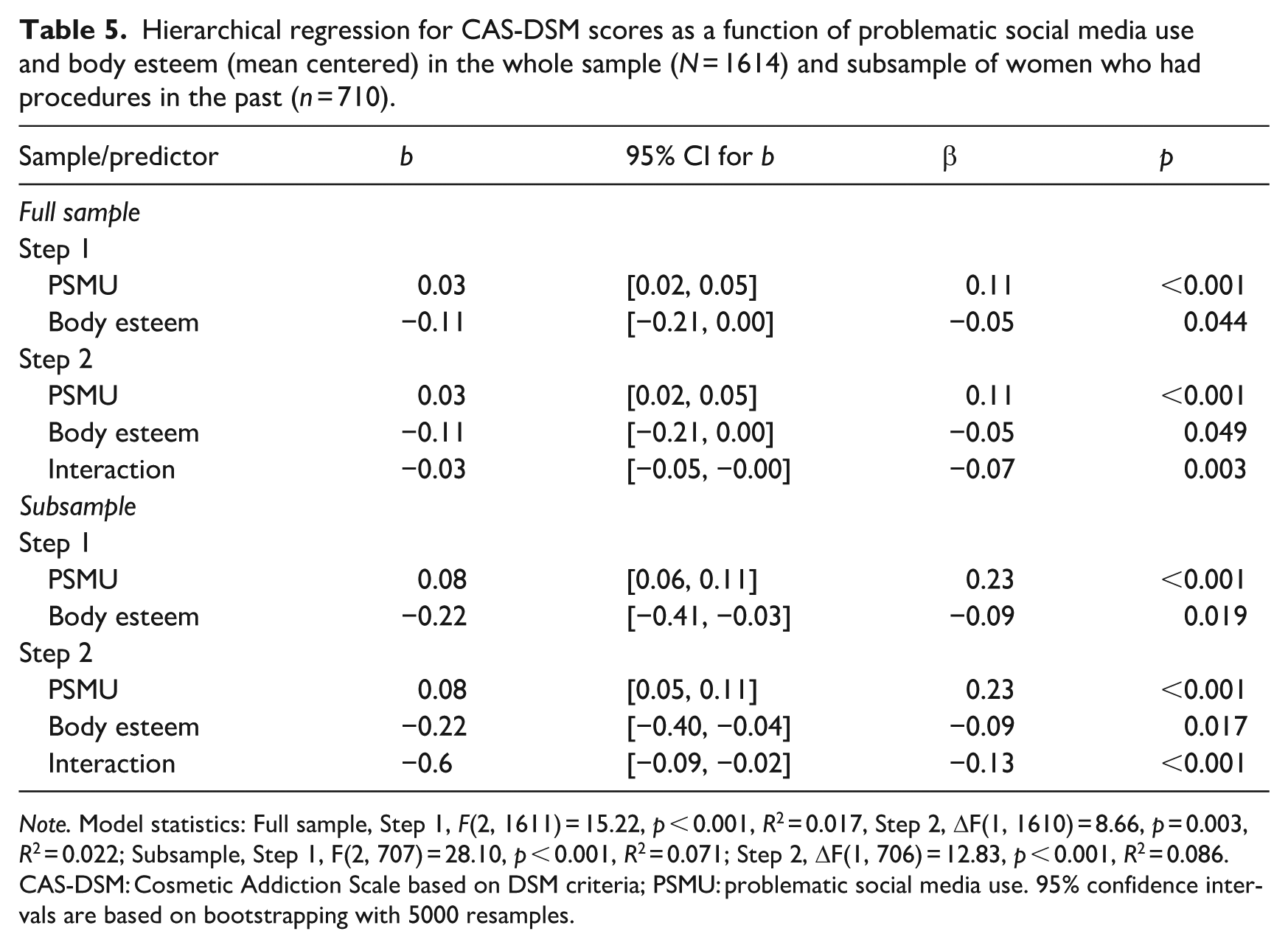
Note. Model statistics: Full sample, Step 1, F(2, 1611) = 15.22, p < 0.001, R2 = 0.017, Step 2, ΔF(1, 1610) = 8.66, p = 0.003, R2 = 0.022; Subsample, Step 1, F(2, 707) = 28.10, p < 0.001, R2 = 0.071; Step 2, ΔF(1, 706) = 12.83, p < 0.001, R2 = 0.086. CAS-DSM: Cosmetic Addiction Scale based on DSM criteria; PSMU: problematic social media use. 95% confidence intervals are based on bootstrapping with 5000 resamples.
As shown in Figures 2 and 3, PROCESS analyses (Hayes, 2022, Model 1) bootstrapping with 5000 resamples, indicated that among women with high BSMAS scores (+1 SD), low body esteem (−1 SD) was associated with more ACPU (higher CAS-DSM scores) in the whole sample, b = −0.25 [−0.40, −0.11], t(1610) = 3.48, p < 0.001, and the subsample, b = −0.53 [−0.78, −0.28], t(706) = 4.19, p < 0.001. However, among women low in BSMAS (−1 SD), body esteem was not related to CAS-DSM scores in both the whole sample and subsample, bs < 0.09, ts < 0.74, ps > 0.458. These results remained the same when feministic attitudes or number of lifetime procedures were included as in the model.

Cosmetic Addiction Scale DSM (CAS-DSM) scores by Social Media Addiction (BSMAS) and body esteem in the whole sample (N = 1614).

Cosmetic Addiction Scale DSM (CAS-DSM) by Social Media Addiction (BSMAS) and body esteem among women who previously had cosmetic procedures (N = 710).
We also conducted parallel analyses only among participants who reported that their responses to the CAS-DSM reflect their experience in the past year (n = 557). These analyses yielded similar results, with a statistically significant PSMU and body esteem interaction, b = −0.06, t(553) = 3.26, p < 0.001, β = −0.13, ΔR2 = 0.02; and the same pattern of simple slope comparison (Appendix 4, Figure S3 of Supplemental Materials).
Discussion
The goal of this study was to assess the prevalence of ACPU and explore its associations with personality, attitudinal, and behavioral factors, using the CAS-DSM scale to determine ACPU in a large general population sample of Jewish Israeli women. ACPU had a prevalence of 8.8% in the total sample and 20% among women who had underwent such procedures. These results were similar but lower for the past year reports. These rates did not differ by age. More religious women reported lower ACPU compared to traditional and secular ones, with traditional women reporting more risk prevalence scores than all other groups.
Our hypotheses regarding contributors to ACPU were partially supported. Zero-order correlational analyses indicated that ACPU was associated with more PSMU, lower levels of body esteem, self-esteem, and attachment security, weaker feminist attitudes, and more negative attitudes to aging. However, multiple regressions indicated that only body esteem, PSMU and feminism had unique associations with ACPU. Thus, Hypotheses 1, 2, and 4 were supported, but the effect sizes were generally small.
Supporting Hypothesis 5, findings indicated that among women with high PSMU, lower body esteem was associated with higher ACPU. This association was not significant among women with lower levels of PSMU.
The current findings suggest that ACPU may be relatively prevalent among Israeli women who engage in cosmetic interventions, underscoring the need for greater awareness of the potential addictive component such procedures may entail. Notably, 15% of women who had undergone CP reported moderate to severe symptoms of problematic use within the past year; a rate higher than that reported in Shah et al.’s (2021) American sample (although our ability to compare between these two non-representative samples is limited). Furthermore, 6.8% of women in the entire sample were identified as being at moderate-severe risk for addictive CP behavior during the past year, compared to the prevalence of other potentially addictive behaviors among women in Israel, such as gambling (2.6%) and gaming (2.9%) (Shmulewitz et al., 2025). These findings are concerning and emphasize the need for further research on ACPU both in Israel and around the globe.
In line with hypotheses 4–5, body esteem emerged as an important factor associated with ACPU. These findings extend the existing literature by linking body esteem not only to motivation for and engagement in CP, but also to the potentially addictive nature of such use. These findings underscore the potentially crucial role of satisfaction with one’s own body and self in preventing the misuse of CP.
Our findings also highlighted the negative impact of PSMU on ACPU especially among women with low body esteem. Problematic social media use might have negative implications for body image, by fostering body dissatisfaction and social appearance anxiety or shaping beauty perceptions, all of which may, in turn, make CP more appealing especially among women with low body esteem (de Valle et al., 2021; Mironica et al., 2024; Mohammadi et al., 2023). Thus, future experimental research should test if reducing PSMU and enhancing body esteem may reduce ACPU. This may benefit future interventions for ACPU.
In our study, feminist attitudes were mildly related to ACPU and did not interact with other variables. This may be due to the conceptual complexity of feminist attitudes. In the present study, we operationalized feminist attitudes through non-acceptance of gender-role stereotypes. However, feminist attitudes are likely more nuanced and multidimensional, and non-acceptance of gender-role stereotypes may not fully capture the diverse ways in which feminism related to engagement in cosmetic interventions. Future research should therefore examine the relationship between ACPU and feminist identity or attitudes using broader and more comprehensive measures that reflect the evolution and diversity of feminist thought over time.
The observed association between ACPU and negative attitudes toward aging seemed to be consistent with our hypotheses, albeit the effect size was small, and it did not survive the multiple regressions. This may stem from the fact that our measure of attitudes toward aging assessed general perceptions of psychological loss and growth, rather than focusing specifically on appearance-related concerns. Future studies should further investigate this relationship across diverse populations, emphasizing perceptions of aging and beauty, especially given that the motivation to maintain a youthful appearance remains a central driver of cosmetic procedure use (Honelová and Vidovićová, 2023; Martinez et al., 2023).
Overall, our hypotheses regarding the factors associated with ACPU were partially supported, especially regarding body image, PSMU, and feminism. However, the relatively small effect sizes suggest that most of the variance associated with ACPU is still unknown.
Future studies may also examine the relationship between ACPU and mental health, given the established link between body dysmorphic disorder (BDD) and engagement in cosmetic interventions (e.g. Cleary et al., 2021). For instance, research could explore whether ACPU may contribute to the exacerbation of existing mental health problems, and conversely, whether preexisting psychological difficulties may increase vulnerability to ACPU. Future research should more comprehensively examine these relationships to better understand the addictive potential of engagement in cosmetic interventions (e.g. Shah et al., 2021; Wagenaar and Hermans, 2025). Such understanding could inform the development of prevention and intervention strategies aimed at supporting individuals, who may be vulnerable to ACPU.
Several limitations should be noted. First, given the cross-sectional design, causal relationships between body esteem, PSMU, and ACPU cannot be determined. Increased engagement in CP could influence body esteem (e.g. Kazeminia et al., 2023) or promote greater social media use, or a third confounding variable accounts for these associations. Longitudinal and experimental studies are needed to clarify the causal mechanisms underlying ACPU.
Second, although this study employed a large sample based on population-level quotas in Israel, it included only Jewish Israeli women and was conducted online. Furthermore, as participants were recruited through a web panel, the sample may be characterized by relatively higher engagement with social media. Thus, the findings may not fully represent the broader Israeli population or may potentially inflating associations between key variables. Future research should estimate the prevalence of ACPU and associations between variables using more representative (economically, geographically, etc.) and diverse samples.
Third, although the sample was large, considering that this was a single study, we should consider the possibility of Type 1 error rates. While we attempted to correct for this using bootstrapping, replication studies need to be more certain in these findings.
Fourth, although we employed a preexisting DSM-based measure of ACPU (CAS-DSM; Shah et al., 2021), additional research is required to further establish the construct validity of ACPU using alternative methodologies and measurement approaches. For example, future studies could incorporate objective indicators such as financial expenditure, social or occupational impairment, and clinically assessed psychological distress rather than relying solely on self-report data.
Fifth, although we examined a range of personality, attitudinal, and behavioral variables potentially associated with ACPU, other relevant factors warrant investigation. These may include additional personality traits (e.g. narcissism, neuroticism, or other Big Five dimensions; D’Agostino et al., 2018; Davis and Vernon, 2002), attitudinal variables (e.g. self-objectification, trust in science), and other behavioral or substance-related addictions (e.g. internet addiction, sex addiction, prescription medication misuse, or illicit drug use). Moreover, future studies should explore whether ACPU differs across types of procedures, as we did not distinguish between invasive and non-invasive procedures, nor between one-time and repeated procedures.
Sixth, future research should also examine the prevalence and correlates of ACPU among men as well as transgender and non-binary individuals. Although these rates are likely much higher in women, changes in technological advances and cultural norms could quickly change.
Finally, future research should examine additional key factors that may relate to ACPU. These include prior mental health treatment history, current mental health state, and exposure to cosmetic-related media and marketing, all of which may have an impact on ACPU.
To conclude, this research indicates that symptoms of ACPU were pervasive in a sample of Jewish Israeli women. Several personality, attitudes and behavioral addiction measures contributed to increased risk for ACPU. These findings, together with prior research, highlight the increasing need to research repeated engagement in CP as a potentially addictive behavior. We hope that this preliminary study contributes to raising awareness of this emerging phenomenon and encourages further research focused on understanding ACPU as well as the development of preventive and therapeutic interventions dealing with the negative implications of the potentially addictive behavior.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261444719 – Supplemental material for Prevalence of addictive use of cosmetic procedures and risk factors among Israeli women
Supplemental material, sj-docx-1-hpq-10.1177_13591053261444719 for Prevalence of addictive use of cosmetic procedures and risk factors among Israeli women by Vera Skvirsky, Uri Lifshin, Dvora Shmulewitz and Mario Mikulincer in Journal of Health Psychology
Footnotes
Ethical considerations
This research was approved by the Institutional Review Board (IRB) at Reichman University, protocol number: P_2025019, and followed the guidelines set forth by the APA’s Ethical Principles of Psychologists and Code of Conduct Standard 8.
Consent to participate
All participants signed informed consents.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
All four authors took part in conceptualization of the study and its methodology. Vera Skvirsky took lead in project administration and coordination, carried out data collection and curation. Uri Lifshin took the lead in formal analysis. Vera Skvirsky, Uri Lifshin and Dvora Shmulewitz took lead in writing the original draft of the manuscript. Mario Mikulincer took lead in providing resources and supervision. All authors provided critical feedback and helped shape the research, and final version of manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.