
Abstract
While religious group membership is often linked to positive health outcomes, it can also influence engagement with health advice in ways that present challenges. The role of religious group membership in long COVID prevalence and severity therefore warrants closer examination. This study used cross-sectional data from Round 11 of the European Social Survey (N = 25,124) across 24 countries. Multilevel multinomial logistic mediation models tested whether the association between religious group membership and long COVID was mediated by two divergent pathways: religious attendance (enactment) and religiosity (significance of beliefs). Results showed that membership was indirectly associated with a lower likelihood of reporting long COVID symptoms via more frequent attendance at religious services. By contrast, greater religiosity was associated with a higher likelihood of reporting persistent symptoms. These findings suggest that the health advantages of religious group membership may lie in opportunities for social connection.
Introduction
Religious group membership represents a common and enduring form of social connection worldwide. Beyond offering spiritual guidance, religious communities create structured opportunities for shared identity and meaningful interpersonal engagement (Haslam et al., 2008; King, 2019). These forms of involvement have been linked to a range of positive health outcomes, including reduced stress, improved immune function, and lower psychological distress (Koenig and Büssing, 2010; Rosmarin and Koenig, 2020). In particular, participation in religious communities has been associated with better recovery outcomes for people living with chronic illnesses such as cardiovascular disease and cancer (Masters and Hooker, 2013; Roger and Hatala, 2018).
These insights are especially relevant in the context of long COVID, a condition characterised by symptoms that persist for 3 months or more following acute COVID-19 infection (Davis et al., 2021). Unlike acute COVID-19, which typically resolves within a short period, long COVID involves ongoing health problems such as fatigue, cognitive impairment, respiratory difficulties, and reduced physical functioning (Shanbehzadeh et al., 2021; Tabacof et al., 2022). These symptoms can fluctuate over time and may substantially disrupt daily activities, employment, and psychological wellbeing (Burton et al., 2022; Petker and Ogden, 2025; Spence et al., 2023), leading many researchers to conceptualise long COVID as an emerging chronic health condition (de Oliveira Almeida et al., 2023). A recent meta-analysis estimates the global prevalence of long COVID at approximately 35%, underscoring the significant public health burden it presents (Hou et al., 2025). While medical treatment is essential, effective management also requires sustained social and psychological support. Previous research shows that people frequently draw on existing group memberships to manage chronic symptoms and promote recovery (Foran et al., 2021, 2024; Haslam et al., 2008; Walsh et al., 2015). Given that religious communities are often built around regular group participation and shared meaning, they may represent a valuable, yet underexplored, source of support for people navigating long COVID.
The social identity approach to health (Jetten et al., 2012) offers a useful framework for explaining this protective potential. This perspective emphasises that it is not simply group membership itself, but the extent to which people actively engage with and derive meaning from their group memberships, that predicts health outcomes (Haslam et al., 2018). Within religious contexts, this aligns with longstanding conceptualisations distinguishing between outward enactment through participation and the internalised significance of religious beliefs (i.e. religiosity; Allport and Ross, 1967; Koenig and Büssing, 2010). Although religiosity has traditionally received greater emphasis in religion-health research, recent evidence suggests that the health benefits of religion are largely derived from its social components (Shattuck and Muehlenbein, 2020). For example, frequent attendance at religious services has been associated with stronger antibody responses to the COVID-19 vaccine, lower psychological distress, and reduced inflammation (McMahon et al. 2024; Ysseldyk et al., 2018). Based on this evidence, it is anticipated that the social engagement afforded through religious group membership may function as a protective resource for people navigating long COVID.
At the same time, however, not all aspects of religious group membership may support recovery from chronic symptoms. In particular, the significance people attribute to their religious beliefs may, in some cases, shape health behaviours in ways that are not fully aligned with health advice (Foran et al., 2025). When significance is attributed to religious beliefs, people may be more likely to turn to trusted figures within their religious communities, such as religious leaders or fellow congregants, for guidance on health-related issues (Baruth et al., 2015; Ysseldyk et al., 2010, 2013). If these ingroup members do not actively promote health advice, people may be less inclined to adopt it (Pirutinsky et al., 2020; Tippins et al., 2023). This does not necessarily reflect scepticism towards science, but rather the influence of alternative, belief-consistent guidance from familiar and trusted sources (Greenfield and Marks, 2007). In this context, the significance people attribute to their religious beliefs may lead people to prioritise advice from religious ingroup members over that of medical professionals or public health experts. Over time, such patterns may be associated with reduced engagement with health-promoting behaviours and associated with poorer recovery outcomes. Religiosity, then, may represent a pathway through which religious group membership is associated with a greater likelihood of persistent long COVID symptoms.
The present study
The present study examines the role of religious group membership in the context of long COVID, with a specific focus on how it relates to the prevalence and severity of persistent symptoms. Drawing on the evidence outlined above, we propose that long COVID prevalence and severity may be shaped by the social and psychological resources associated with religious group membership. Specifically, we compare two separate mechanisms: the enactment of religious group membership, operationalised as frequency of religious service attendance, and religiosity, operationalised as the significance people attribute to their religious beliefs. By testing these parallel pathways, we aim to clarify whether religious group membership functions as a protective resource, a risk factor, or both for people managing the long-term effects of COVID-19. Because religious participation opportunities and the importance people attribute to religion vary across national contexts, we also examined whether the observed associations were consistent across countries.
Method
Participants
The study utilised data from Round 11 of the European Social Survey (ESS11). 1 Fieldwork occurred in 2023–2024 (timing varied by country). In accordance with the Statutes of the ESS European Research Infrastructure Consortium (ESS ERIC; Article 23.3), the ESS adheres to the Declaration on Professional Ethics of the International Statistical Institute. Ethical oversight for ESS-commissioned work is provided by the ESS Research Ethics Board, and each participating country ensures compliance with national ethics and data protection requirements. All participants provided informed consent prior to data collection.
Our analytic sample comprised 25,124 people (Mage = 49.7 years, SD = 17.9, and range = 15–90 years) across 24 countries. 54.6% of participants were women (N = 13,711). Participants were selected based on people who reported having COVID-19 at any time since the start of 2020 and who had complete data for long COVID prevalence and severity questions. In total, 5259 participants reported experiencing symptoms lasting 3 months or longer after a COVID-19 infection (20.7%). Of these, 2747 reported experiencing current symptoms (10.8%). 17,343 (68.4%) reported no symptoms lasting 3 months or longer. Our analytic sample therefore included respondents both with and without long COVID, with the latter serving as the reference group in analyses. See Figure 1 for information on reported religious affiliation and denomination across countries.
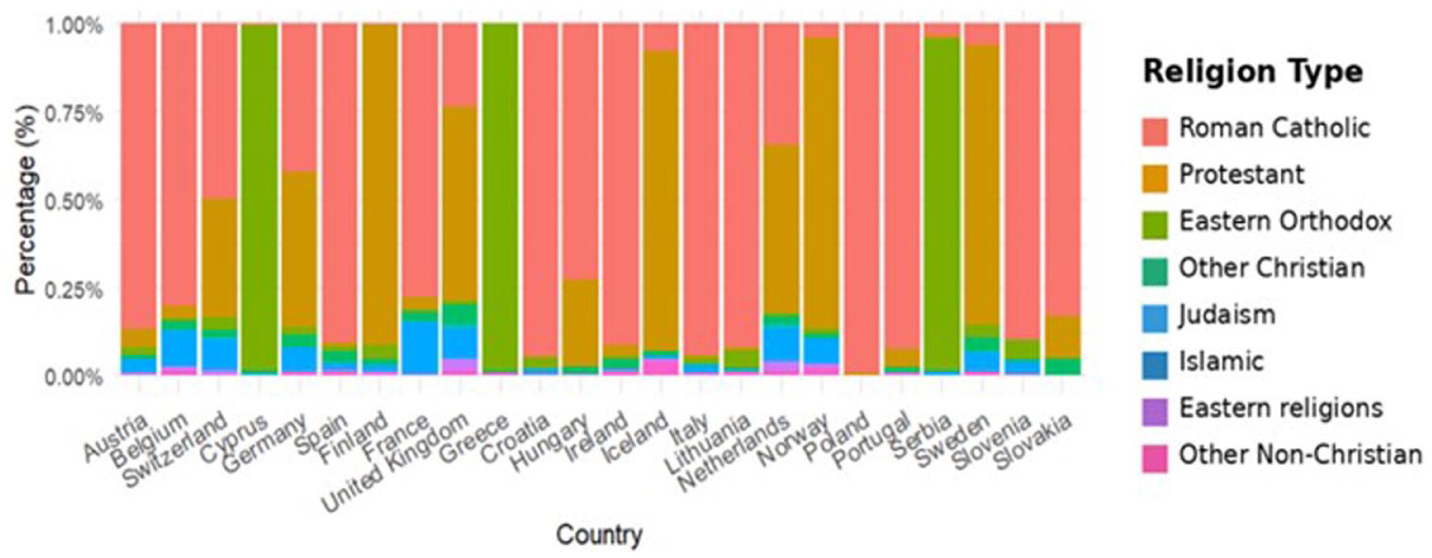
Self-reported religious affiliation by country.
Measures
Religious group membership
Religious group membership was assessed with one item: “Do you consider yourself as belonging to any particular religion or denomination” (0 = no, 1 = yes).
Frequency of religious attendance
Attendance at religious services, a measure of enactment of religious group membership, was assessed using one item: “Apart from special occasions such as weddings and funerals, about how often do you attend religious services nowadays” (1 = does not attend at all, 7 = attends religious services every day). Higher scores indicate more frequent attendance.
Religiosity
Religiosity, operationalised as the significance people attribute to their religious beliefs was assessed using two items: “How religious are you?,” measured on a 0 (not at all) to 10 (very religious) scale, and “Apart from when you are at religious services, how often, if at all, do you pray?,” originally measured on a 1 (never) to 7 (everyday) scale.
The two items were strongly correlated (r = 0.70, p < 0.001) and demonstrated high internal consistency (Cronbach’s α = 0.81), supporting their combination into a single measure. A composite significance of religious beliefs score was created by averaging the standardised scores of these two items. Our religiosity measure captures personal belief importance and private religious behaviour rather than formal theological doctrine or institutional teachings (i.e. doctrinal belief). Higher scores indicate a greater significance of religious beliefs.
Long COVID prevalence and severity
Self-reported long COVID prevalence and severity was derived from two survey items (yes/no) asking participants: (1) whether they had experienced symptoms lasting 3 months or longer after a COVID-19 infection and (2) whether they were still experiencing such symptoms. Responses were categorised into three mutually exclusive groups: 0 (no symptoms), 1 (past symptoms only), and 2 (current symptoms).
Covariates
To account for potential confounding influences, several theoretically relevant covariates were included: age, gender, ethnicity, perceived household income, pre-existing health conditions and COVID-19 vaccination status. These variables were selected based on prior evidence linking demographic and social factors to both religious involvement and health outcomes (e.g. Bengtson et al., 2015; Mansell et al., 2022), including susceptibility to long COVID. Inclusion of these covariates in our models allowed for a more robust test of our indirect effects.
Analytic approach
We estimated two-level multinomial logistic mediation models using Mplus Version 8.11. Country was specified as the clustering variable in order to account for the nested structure of individuals within 24 national samples. Religious group membership was modelled as the predictor (X), and long COVID prevalence and severity was modelled as the outcome (Y). Frequency of religious service attendance (M1) and the significance people attribute to religious beliefs (M2) were tested as separate mediators. Long COVID prevalence and severity was treated as a nominal categorical variable with three levels: no symptoms, past symptoms, and current symptoms. The “no symptoms” category was used as the reference group, which yielded two contrasts: past symptoms versus no symptoms, and current symptoms versus no symptoms. Models were estimated using robust maximum likelihood (MLR) with Monte Carlo numerical integration, based on 3250 integration points. Missing data were handled with full-information maximum likelihood (FIML). Indirect, direct, and total effects were estimated on the logit scale. Standard errors were computed using the delta method, and 95% confidence intervals were reported for all estimates. To aid interpretability, odds ratios (OR) with corresponding 95% confidence intervals were presented alongside unstandardised log-odds coefficients (b).
Because the ESS is a multinational survey, we also examined whether the observed associations were consistent across countries, recognising that opportunities for the enactment of one’s religion and the significance of one’s religion may differ across national contexts. To evaluate this, we specified random slopes for the paths from religious group membership to the mediators and from the mediators to long COVID prevalence and severity. Random intercepts were specified for country, and slopes were allowed to correlate with intercepts.
We also estimated reverse-direction models to explore the plausibility of alternative pathways. In these models, long COVID prevalence and severity (no symptoms, past symptoms, current symptoms) was specified as the predictor, and the proposed mediators were specified as the outcomes. We examined whether long COVID was associated with frequency of religious attendance and with religiosity, which was assessed in terms of significance people attribute to their religious beliefs. We also tested the indirect association from long COVID to religiosity through attendance. These models were estimated using the same covariates, clustering variable, and estimator as the primary analyses. Given the cross-sectional nature of the ESS, these models are interpreted strictly as associations rather than causal pathways.
Results
Frequency of religious attendance
Our results revealed that the indirect effect of religious group membership on long COVID prevalence and severity via religious attendance, though small, was significant: past versus none, b = −0.08, SE = 0.03, z = −3.04, p = 0.002, 95% CI [−0.13, −0.03], OR = 0.93, 95% CI [0.88, 0.97]; current versus none, b = −0.05, SE = 0.03, z = −2.18, p = 0.030, 95% CI [−0.10, −0.01], OR = 0.95, 95% CI [0.900, 0.995]. Specifically, those who reported belonging to a religion were more likely to attend religious services, and higher attendance was associated with lower odds of reporting both past and current long COVID symptoms (see Figure 2). Overall, these findings indicate that a pathway through which religious group membership is associated with a lower likelihood of long COVID is through the enactment of one’s religious group membership, namely attendance at religious services.
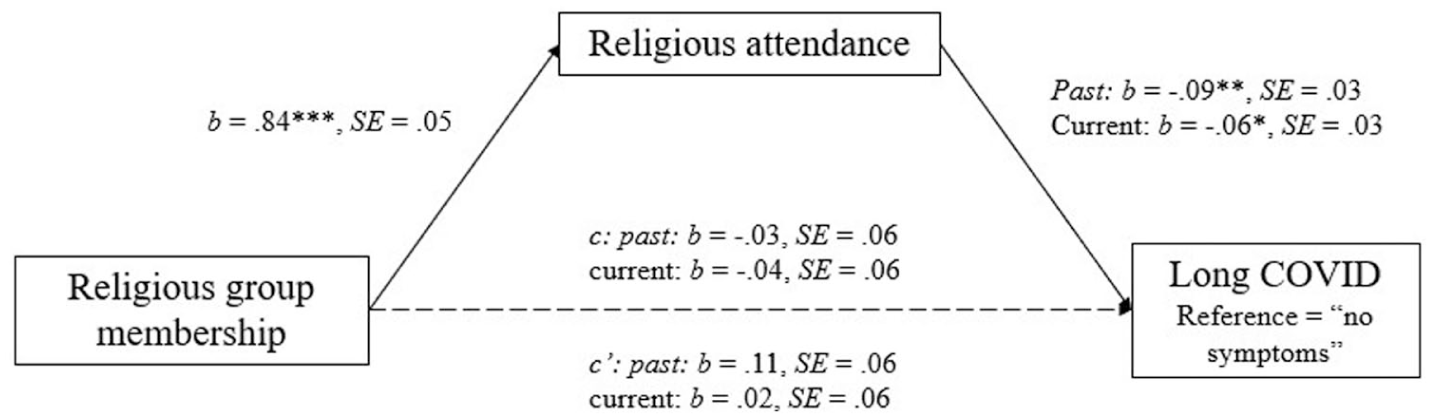
Religious attendance mediates the association between religious group membership and long COVID prevalence and severity.
In terms of covariates, older adults reported slightly lower attendance at religious services, b = −0.01, SE = 0.001, p < 0.001. Regarding gender, women reported lower attendance than men, b = −0.10, SE = 0.03, p < 0.001, a finding that contrasts with prior research suggesting higher rates of religious service attendance among women (e.g. Pew Research Center, 2015). This discrepancy may reflect contextual variation across countries or pandemic-related shifts in religious engagement. Women were also more likely to report long COVID symptoms (b = 0.14, SE = 0.02, p < 0.001). People who reported pre-existing health conditions were more likely to report long COVID symptoms, b = 0.21, SE = 0.01, p < 0.001. Ethnic minorities were also more likely to report long COVID symptoms, b = −0.07, SE = 0.03, p = 0.012. People who were vaccinated were less likely to report long COVID symptoms, b = −0.10, SE = 0.03, p < 0.001.
Variability across countries
The variance of the random slope for the relation between religious group membership and religious attendance was modest (σ2 = 0.035, SD = 0.19), indicating some cross-country variability in the strength of this association. A weak positive correlation between the random intercept and slope (r = 0.20) suggests that in countries with higher average religious attendance, religious group membership’s effect was slightly stronger. This may reflect the greater availability of social engagement opportunities in more religious contexts, where a larger presence of fellow attendees could enhance the social value of participation.
Turning to the path from religious attendance to long COVID, variability across countries was limited. The random slope variance for the “past versus none” contrast was small (σ2 = 0.026, SD = 0.16), while the slope for the “current versus none” contrast showed only slightly greater variability (σ2 = 0.037, SD = 0.19). The protective association of attendance with past symptoms (b = −0.54, p < 0.001) was robust across countries, whereas the effect on current symptoms (b = −0.05, p = 0.63) was weaker and less consistent. Taken together, these results indicate that the religious attendance–long COVID pathway is largely consistent across national contexts.
Religiosity
The indirect effect of religious group membership on long COVID prevalence and severity via religiosity, though small, was significant: past versus none, b = 0.20, SE = 0.02, z = 8.19, p < 0.001, 95% CI [0.15, 0.24], OR = 1.22, 95% CI [1.16, 1.27]; and current versus none, b = 0.40, SE = 0.05, z = 7.95, p < 0.001, 95% CI [0.30, 0.49], OR = 1.49, 95% CI [1.35, 1.63]. Specifically, those who belonged to a religion were more likely to report greater religious beliefs, which in turn was associated with a greater likelihood of reporting both past and current long COVID symptoms (see Figure 3). Notably, religious group membership had a significant negative direct effect on long COVID, past: b = −0.22, SE = 0.07, p = 0.001, OR = 0.80, 95% CI [0.71, 0.91]; current: b = −0.36, SE = 0.06, p < 0.001, OR = 0.70, 95% CI [0.61, 0.74]. This pattern is consistent with the protective association of religious group membership on long COVID is partly attenuated by the significance people attribute to religious beliefs.
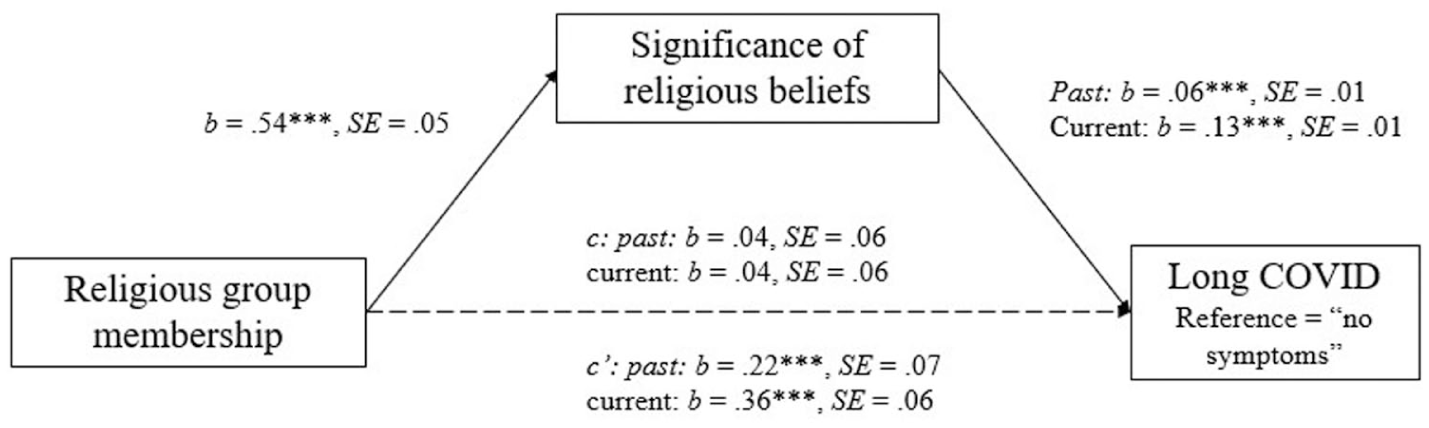
Religiosity mediates the association between religious group membership and long COVID prevalence and severity.
Regarding covariates, age was associated with stronger religious beliefs, b = 0.01, SE = 0.001, p < 0.001. Women reported stronger religious beliefs, b = 0.226, SE = 0.015, p < 0.001, and were more likely to report long COVID symptoms, b = 0.127, SE = 0.021, p < 0.001. People who reported pre-existing health conditions, b = 0.211, SE = 0.014, p < 0.001, and ethnic minorities, b = −0.165, SE = 0.034, p < 0.001, were more likely to report long COVID symptoms. People who had received the COVID-19 vaccine were less likely to report long COVID symptoms, b = –0.110, SE = 0.027, p < 0.001. Finally, greater perceived household income was associated with a reduced likelihood of reporting long COVID symptoms, b = –0.015, SE = 0.004, p = 0.001.
Variability across countries
The variance of the random slope indicated that the strength of the association between religious group membership and religiosity differed by context (σ2 = 0.01, SD = 0.10). The correlation between the random slope and the random intercept was positive and moderate, r = 0.52. This suggests that in countries where religiosity is generally higher, the association between religious group membership and the perceived significance of religious beliefs is stronger, indicating that the identity-reinforcing function of group membership may be amplified in more religious contexts.
Turning to the path from religiosity to long COVID, variability across countries was modest. The random slope variance for the “past versus none” contrast was small and non-significant (σ2 = 0.026, SD = 0.16), while the slope for the “current versus none” contrast showed slightly greater variability (σ2 = 0.037, SD = 0.19). The positive mean slope for past symptoms (b = 0.20, p < 0.001) was robust across countries, whereas the near-zero mean slope for current symptoms (b = 0.05, p = 0.63) indicated greater cross-national fluctuation. The correlation between slope and intercept for the “current versus none” contrast was positive and moderate (r = 0.65), indicating that in countries with higher levels of long COVID reporting, the risk-enhancing effect of religiosity was stronger.
Reverse direction models
We also considered an alternative account in which persistent symptoms are associated with reduced opportunities for service attendance and greater reliance on private religious practices. Because the ESS11 is cross-sectional, temporal ordering cannot be established, but we examined these associations in the reverse direction. Respondents with long COVID reported lower service attendance (past vs none: b = −0.16, OR = 0.85; current vs none: b = −0.12, OR = 0.89). In contrast, long COVID was not significantly associated with religiosity (b = 0.00–0.02, OR = 1.00–1.02). For the indirect pathway from long COVID to religiosity via attendance, the past versus none contrast produced a statistically significant but very small association (b = −0.01, 95% CI [−0.012, −0.003]), whereas the current vs none contrast was not significant (b = −0.003, 95% CI [−0.008, 0.003]). These results indicate that although reverse pathways are conceivable, they appear to have limited explanatory value. Taken together, this pattern lends greater support to the interpretation that the associations observed in our primary model provide a stronger account of the data. However, these models serve as sensitivity checks and are interpreted strictly as associations, not causal effects.
Discussion
The aim of this study was to examine whether religious group membership is associated with long COVID prevalence and severity and to identify the pathways through which this association might operate. Consistent with our predictions, we identified that religious group membership is linked to long COVID prevalence and severity through two distinct pathways. On one hand, enactment of religious group membership, operationalised as frequency of attendance at religious services, was associated with a lower likelihood of reporting persistent symptoms. On the other hand, religiosity, reflecting the significance people attribute to their religious beliefs, was associated with a greater likelihood of reporting persistent symptoms. These findings underscore the importance of distinguishing between the social engagement and belief-oriented nature of religious group membership, as they appear to have divergent implications for long COVID prevalence and severity.
Our findings are consistent with the interpretation that the enactment of religious group membership is associated with health protection (McMahon et al., 2024). Frequency of religious attendance was associated with a lower likelihood of reporting persistent long COVID symptoms and mediated the beneficial association between religious group membership and long COVID prevalence and severity. This aligns with previous social cure work demonstrating that frequent social engagement fosters well-being by enhancing social connection, identity continuity, and shared experiences (Haslam et al., 2018; Ysseldyk et al. 2018). Importantly, we found that the protective association of religious attendance with past long COVID symptoms was highly consistent across countries. This reinforces the idea that structured social engagement, whether religious or secular, may offer reliable protection in the context of past long COVID symptoms.
By contrast, religiosity was associated with a risk-enhancing pathway. People who placed greater significance on their religious beliefs were more likely to report persistent long COVID symptoms. This should not be interpreted as evidence that religious belief is inherently detrimental to health. Rather, these findings suggest that the belief-oriented nature of religious group membership may influence perceived boundaries between ingroup and outgroup sources of guidance (Ysseldyk et al., 2010). In this context, people may prioritise advice from religious leaders or fellow religious group members over medical professionals or public health experts (Greenfield and Marks, 2007). This dynamic may be associated with reduced adherence to health-promoting advice critical for recovery (Olagoke et al., 2021; Rutjens et al., 2018).
Importantly, the strength of the association between religiosity and symptom reporting varied across countries, suggesting that the health implications of religious belief may be context-dependent and shaped by broader national factors. In this light, it becomes especially important to distinguish between aspects of religious group membership that support health and those that may unintentionally undermine it. Cultural context may also influence how religious group membership and long COVID experiences are understood across settings (Bayeh et al. 2021). Differences in health beliefs, social norms, dominant religious traditions, and healthcare systems may shape both the reporting of long COVID symptoms and access to support during recovery (MacPpherson et al., 2022; Ting et al., 2021). Although the present study accounted for between-country variation statistically, future research could examine more directly how culturally specific understandings of illness and religion influence long COVID experiences across contexts.
Implications
The findings of this study highlight the importance of social factors in understanding the association between religion and chronic illness, particularly in the context of long COVID. Our results do not suggest that being religious or belonging to a religious group is inherently protective. Rather, they show that it is the enactment of religious group membership through structured participation that was associated with more favourable health patterns, in line with the social identity approach to health (Jetten et al., 2012). This also aligns with the idea that group-based resources may play a role in managing the psychological demands of chronic illness (Foran et al., 2024; Haslam et al., 2018).
These insights also have important implications for public health. First, they demonstrate that religious group membership may support recovery from long COVID by fostering opportunities for meaningful social connection and participation. Faith-based communities could be valuable partners in promoting public health initiatives, particularly when they facilitate social engagement and reinforce positive health behaviours. However, the protective benefits associated with religious participation are not unique to religious settings. If social participation is the key driver of these benefits, similar patterns may also be observed through secular forms of community involvement, such as peer support groups, social clubs, and volunteer organisations. Public health interventions might therefore benefit from leveraging diverse social structures to provide accessible and inclusive forms of support for people with long COVID and other chronic conditions.
At the same time, the findings highlight potential challenges associated with religiosity and belief-driven forms of group membership. The association between higher religiosity and persistent symptom reporting may reflect greater reliance on ingroup norms and reluctance to engage with health advice and interventions. From a public health perspective, this suggests that fostering respectful and culturally sensitive dialogue with faith communities is crucial. Rather than positioning religious belief as inherently problematic, interventions might aim to work collaboratively with religious leaders and communities to promote health messages that align with both health recommendations and community values.
Limitations and future directions
Despite these insights, this study has several limitations. First, the use of secondary data restricted the measures available for assessing the enactment of religious group membership. While religious attendance provided a reasonable proxy, it did not capture the broader range of community-based interactions or informal support structures. Future research should include more comprehensive indicators that reflect both the quantity and quality of group engagement. Second, the dataset did not include measures of stress or coping style, both of which may be important in understanding how religious engagement relates to long COVID. We were also unable to control for perceived stress, which may confound these associations. For instance, stronger religiosity could reflect coping responses to the stress of long COVID rather than a predictor of symptom persistence. Incorporating such variables in future studies would help clarify underlying mechanisms.
Third, while country-level variance was accounted for, other contextual factors, such as healthcare access or differences in dominant religious traditions, may also shape these relationships and warrant further investigation. Fourth, long COVID prevalence and severity was based on self-reported symptoms rather than clinical diagnoses or medical records. Finally, because the ESS11 is cross-sectional, the mediation models cannot establish causal direction. Reverse-direction models suggested that long COVID may slightly reduce opportunities for service attendance but showed no meaningful associations with religiosity. Indirect effects through attendance were negligible, indicating that while reverse pathways are conceivable, their explanatory value is minimal. Our findings should therefore be interpreted as associations rather than causal effects.
Conclusion
Our study demonstrates that religious group membership is linked to long COVID prevalence and severity through two distinct pathways. Enactment of religious group membership through frequent attendance at religious services was associated with a lower likelihood of reporting persistent symptoms, underscoring the protective value of structured social engagement. In contrast, religiosity, reflecting the significance people attribute to religious beliefs, was associated with a greater likelihood of symptom reporting and severity, suggesting that reliance on ingroup norms and guidance may present challenges for public health. These findings highlight the need for public health strategies that foster inclusive and meaningful social connections while also addressing potential barriers associated with belief-driven group membership. Collaborative approaches that engage faith-based and secular communities alike may be key to supporting recovery and promoting health among people living with long COVID.
Footnotes
Ethical considerations
In accordance with the European Social Survey (ESS) ERIC Statutes (Article 23.3), the ESS subscribes to the Declaration on Professional Ethics of the International Statistical Institute. Ethical oversight for ESS-commissioned work is provided by the ESS Research Ethics Board (![]() ), and each participating country ensures compliance with national ethics and data protection requirements. This study involved the secondary analysis of anonymised data, which has been subject to ethical approval and informed consent procedures in each participating country. Therefore, no additional ethical approval was required for this analysis.
), and each participating country ensures compliance with national ethics and data protection requirements. This study involved the secondary analysis of anonymised data, which has been subject to ethical approval and informed consent procedures in each participating country. Therefore, no additional ethical approval was required for this analysis.
Consent to participate
Participation in the ESS is voluntary. Informed consent was obtained from all participants prior to data collection,
Consent for publication
All authors consented to the submission of this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Aoife-Marie Foran has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 101034345. Prof Orla Muldoon’s involvement in this project has been facilitated by a European Research Council Advanced Award (agreement # 884927). Prof Jolanda Jetten’s involvement in this project has been facilitated by an ARC Laureate Fellowship (FL180100094).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.