
Abstract
We explored South African university students’ perceptions of the COVID-19 vaccine. Twenty-eight students (mean age: 26.2 years; age range 18–43; females = 20, males = 7, other = 1) from a university in the Western Cape participated in semi-structured interviews. Data were thematically analysed using ATLAS.ti (Version 25). Five themes were identified: (1) Between hope and hesitation; (2) Navigating a saturated information ecosystem; (3) Low risk, low priority; (4) Barriers and mandates; and (5) Vaccinating for the greater good: Responsibility and social tension. Findings are discussed in relation to the 5C model of vaccine hesitancy and reveal a nuanced co-existence of hope and mistrust, influenced by concerns about safety, rapid vaccine development, institutional motives, conflicting information, low perceived personal risk, and tensions between collective responsibility and social division. These insights illuminate the complexity of vaccine perceptions among university students and the need for targeted, contextually informed strategies to address hesitancy.
Introduction
The development and distribution of vaccines have long been central pillars of public health, with an extensive history of preventing infectious diseases and significantly reducing global mortality (Montero et al., 2024; World Health Organisation (WHO), 2025a). The WHO (2025a) estimates that vaccines prevent between 3.5 and 5 million deaths annually from illnesses such as diphtheria, tetanus, pertussis, influenza, and measles. Vaccines are biological agents that activate the immune system to produce antigen-specific immunity, thereby preventing infection or reducing disease severity (Montero et al., 2024). Their development involves a rigorous, evidence-based process, including pre-clinical research, multi-phase clinical trials, and comprehensive assessments of safety and efficacy (Artaud et al., 2019). Despite the strong scientific basis for vaccination and its proven effectiveness (Artaud et al., 2019), vaccine hesitancy, defined as the delay in acceptance or refusal of vaccines even when they are readily available, remains a pressing global health challenge (MacDonald, 2015; Nuwarda et al., 2022). Indeed, even prior to the emergence of COVID-19, the WHO identified vaccine hesitancy as one of the top 10 threats to global health (WHO, 2019). Importantly, vaccine hesitancy is complex and context specific, varying across time, place and vaccines and is influenced by several factors such as complacency, convenience and confidence (MacDonald, 2015).
Systematic reviews and metanalytic evidence indicate that university students represent a particularly vaccine-hesitant subgroup, especially in the context of COVID-19 (Geng et al., 2022; Min Htike et al., 2025; Roy et al., 2022). Paradoxically, despite being at the forefront of scientific discourse and with heightened access to information, students often exhibit reluctance or ambivalence towards vaccination. This hesitancy is driven by a range of factors including exposure to misinformation, a low perceived risk of infection, mistrust in pharmaceutical institutions and health authorities, and concerns regarding vaccine safety, side effects and long-term consequences (Bouloukaki et al., 2025; Khubchandani et al., 2022; Min Htike et al., 2025).
Studies focussing on understanding vaccine hesitancy among university students are of particular public health interest. As a demographic group, university students are typically embedded within densely populated, socially dynamic campus environments, which can facilitate rapid disease transmission (Mussetto et al., 2025). Furthermore, university students occupy influential social roles within their peer groups, families, and broader social communities, positioning them as key agents in shaping public perceptions and health behaviours (Frieden, 2010). Moreover, at this stage of life, university students are in the process of forming independent health-related beliefs from their parents or caregivers and are capable of making autonomous medical decisions, which make them an appropriate group to receive vaccine education and public health interventions (Kecojevic et al., 2021; Mussetto et al., 2025; Xu et al., 2021).
While global research on COVID-19 vaccine hesitancy among university students is expanding (see Min Htike et al., 2025), there remains a paucity of studies focussed specifically on student populations in low- and middle-income countries (LMICs), including South Africa. This gap is significant considering evidence suggesting that vaccine attitudes and behaviours are shaped by distinct sociocultural, economic, and informational contexts (Sallam, 2021; Solís Arce et al., 2021). For example, in Roy et al.’s (2022) systematic review, the global pooled prevalence of COVID-19 vaccine hesitancy among university students was 29.8%, with substantially higher rates observed in Africa (55.9%).
Vaccination coverage patterns reflect these disparities. By 30 June 2022 (just 3 months prior to the onset of data collection in the present study) approximately 66.4% of the global population had received at least one dose of a COVID-19 vaccine (Mathieu et al., 2024). In contrast, vaccination coverage in the WHO African Region remained considerably lower, with only 24.7% of the population having received at least one vaccine dose by late June 2022 (Impouma et al., 2022). South Africa mirrored this broader regional trend. Although national vaccination coverage had reached 50% of the adult population by mid-2022, uptake among younger adults remained notably lower, with only 37% of individuals aged 18–34 years vaccinated, compared with nearly 70% of those aged 60 years and older (UNICEF South Africa, 2022). These findings are concerning given that young adults comprise a large proportion of the university student population and were consistently identified as a group with lower vaccine uptake both globally and within South Africa. Despite this, empirical research exploring COVID-19 vaccine perceptions and decision-making among South African university students remains limited.
Rather, existing South African studies have primarily focussed on the general public (e.g. Engelbrecht et al., 2022; Katoto et al., 2022), healthcare workers (e.g. George et al., 2023, 2024) or youth more broadly with varying levels of age and education (aged 15–35: e.g. Casale et al., 2025; Chauke et al., 2021; Muthoni et al., 2023). Notable exceptions include work by Mashau and Shibambo (2023), George et al. (2022), Potgieter et al. (2022) and Mthembu et al. (2023). George et al. (2022), for example, quantitatively surveyed 1262 students and 541 staff at a university in KwaZulu-Natal and found significantly lower vaccination rates among students (57%) compared to staff (79%). According to George et al. (2022) the most frequently cited reasons for vaccine refusal were doubts about vaccine effectiveness (22%) and safety (21%), along with low enthusiasm for booster doses. Similarly, Mashau and Shibambo (2023) quantitatively surveyed 181 students at a university in Limpopo and found that while 70% were willing to be vaccinated, a majority opposed mandatory vaccination policies. Comparably, Potgieter et al. (2022) quantitatively surveyed 205 dental students in the Western Cape and found a vaccine hesitancy rate of 16.9%, driven largely by safety concerns and social pressure from family, peers, and institutional mandates. Mthembu et al. (2023) qualitatively explored the influences of COVID-19 vaccination policy on 10 female health science students’ vaccine acceptance. These authors found that mandatory vaccination policies negatively influenced participants’ academic performance, wellbeing, and autonomy.
While these studies make valuable contributions, they hold several notable limitations. First, three were quantitative, using cross-sectional surveys (George et al., 2022; Mashau & Shibambo, 2023; Potgieter et al., 2022). Although these surveys offer insights into vaccination rates and general drivers of hesitancy, they lack the depth and nuance that qualitative methods provide. For example, Mashau and Shibambo (2023) asked only closed-ended questions, such as whether participants had been vaccinated (yes/no) and whether they supported mandatory vaccination. As a result, interpretation relied largely on the researchers’ assumptions rather than participants’ detailed accounts. Second, two studies focused solely on health science students (Potgieter et al., 2022; Mthembu et al., 2023), despite evidence that this group is typically less vaccine hesitant than students in other disciplines (Min Htike et al., 2025). Third, the only South African qualitative study to date included a small, homogenous sample of ten female health science students and focused narrowly on exploring the influence of institutional vaccination policies on vaccine uptake (Mthembu et al., 2023). A clear gap remains for research that explores vaccine perceptions among students from diverse faculties and gender backgrounds, capturing rich, first-hand narratives. This study sought to address these gaps by qualitatively investigating COVID-19 vaccine perceptions among a diverse sample of university students at a public university in the Western Cape.
Conceptual framework
The WHO’s (2014) 3C model, comprising complacency, convenience, and confidence, has been widely applied as a simple and pragmatic framework to understand vaccine hesitancy, particularly among younger populations such as university students (e.g. Min Htike et al., 2025). While the 3C model offers a useful foundation, it has been critiqued for not fully capturing the range of psychological factors that shape vaccination behaviour. To address these limitations, Betsch et al. (2018) proposed an expanded 5C model, which adds two additional dimensions: calculation, referring to an individual’s propensity to seek and process extensive information about vaccines, and collective responsibility, reflecting a person’s willingness to protect others through vaccination and contribute to herd immunity. Arguably, the 5C model offers a more comprehensive psychological lens for examining vaccine decisions, particularly in populations where both individual and social factors may influence hesitancy (Betsch et al., 2018).
Despite the model’s relevance, none of the existing South African studies examining student vaccine hesitancy and uptake (George et al., 2022; Mashau and Shibambo, 2023; Mthembu et al., 2023; Potgieter et al., 2022) have drawn on either the 3C or 5C frameworks to conceptualise their studies. This study thus makes a novel contribution by employing the 5C model to conceptualise our findings.
Methods
Participants and Procedure
This study forms part of a broader mixed-methods project investigating the psychosocial impact of the COVID-19 pandemic across five vulnerable groups in South Africa: university students, nurses, teachers, high school learners, and patients living with hypertension and diabetes. The broader study employed a sequential explanatory design comprising a quantitative first phase followed by a qualitative second phase (for each separate group). For the university student group, as outlined in Figure S1 in the Supplemental Material, participants were recruited into the first phase through university mailing lists via SUNSurvey. Eligible participants were students currently registered at the university, aged 18 years or older, could complete the survey in English and able to provide informed consent. The survey comprised a demographic section, as well as a range of psychological report measures. At the end of the survey, participants were invited to indicate whether they would be willing to participate in a follow-up interview. Of the 303 students who completed the survey, 30 expressed willingness to participate further, and 28 were ultimately interviewed after two individuals did not respond to follow-up contact attempts.
Our final sample size of 28 was deemed sufficient based on the concept of information power (Malterud et al., 2016), which is likened to data saturation and indicates that the collected data adequately addressed the research questions. More specifically, information power proposes that the more relevant and information-rich the sample is in relation to a focussed research aim, the fewer participants are required. In this study, the specificity of the student population, the clearly defined research aim, the depth and richness of the semi-structured interviews, and the theoretically informed reflexive thematic analysis guided by the 5C model contributed to strong information power. Additionally, although reflexive thematic analysis does not require a fixed saturation threshold, evidence from qualitative methods suggests that thematic insights and meaning saturation tend to stabilise within samples of 12–24 in focussed studies (Guest et al., 2006; Hennink et al., 2017), which aligns with the information power framework that we applied (Malterud et al., 2016).
The final sample of 28 students, had a mean age of 26.2 years, with age ranging from 18 to 43. Of the sample, 20 self-identified as female, seven as male and one as other. Furthermore, of the sample, 18 were undergraduate and 10 were postgraduate students. At the time of data collection, 26 participants had received a COVID-19 vaccine, while two participants remained unvaccinated.
Instrument
A semi-structured interview guide was developed to explore participants’ experiences related to the COVID-19 pandemic, focussing on three key areas: (1) the challenges they encountered, (2) the strategies they employed to cope with these challenges, and (3) their perceptions of the COVID-19 vaccine. It is the third key area, perceptions of the COVID-19 vaccine, on which this paper is based. One-on-one interviews were conducted in English, audio-recorded with participants’ consent, and transcribed verbatim. Transcripts were stored electronically in password-protected files to ensure data security. Each interview lasted approximately 40 minutes, with durations ranging from 20 to 67 minutes. Prior to the interview, participants completed a brief demographic questionnaire. Data collection took place between September and November 2022.
Data Analysis
The data were analysed using reflexive thematic analysis (RTA), through ATLAS.ti version 25 (Braun and Clarke, 2021). RTA is appropriate for exploring participant perceptions of the COVID-19 vaccine, as it emphasises their subjective meanings, beliefs, attitudes, and lived experiences, and enables a flexible approach to identifying patterns within the data. An inductive coding strategy was employed by PH. Each participant’s transcript was initially coded individually to retain the depth and specificity of their personal narratives. Following this, themes and subthemes were generated, compared across transcripts, and refined to capture both commonalities and variations in experience. To further strengthen the rigour and trustworthiness of the analysis, all authors were involved in reviewing the iterative development of the thematic structure to ensure a robust and comprehensive interpretation of the data.
Ethical considerations
Ethical approval for the study was granted by the Health Research Ethics Committee of Stellenbosch University (Ref: N21/05/012-COVID-19). Participation was entirely voluntary and anonymous. Informed consent was obtained from all individuals prior to their involvement. To ensure the wellbeing of participants, contact details for free counselling services were provided should any psychological discomfort or distress arise as a result of participation in the study. No participants accessed the free counselling services. Anonymity and confidentiality were maintained through the use of participant codes and the exclusion of any personally identifiable information. All data were securely stored in password-protected digital files and backed up on OneDrive.
Results
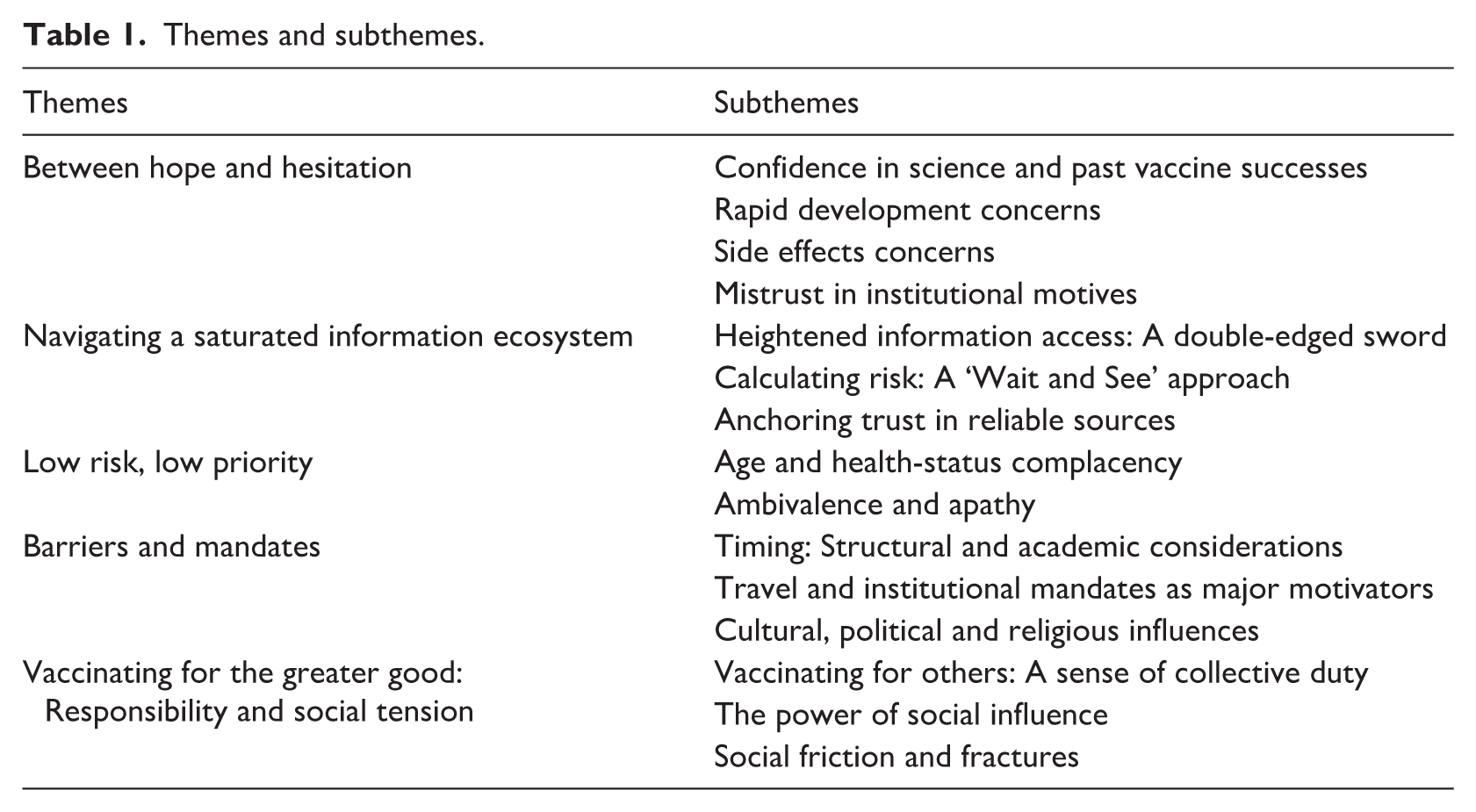
Five themes were identified (see Table 1): (1) Between hope and hesitation; (2) Navigating a saturated information ecosystem; (3) Low risk, low priority; (4) Barriers and mandates; and (5) Vaccinating for the greater good: Responsibility and social tension.
Themes and subthemes.
Theme 1: Between hope and hesitation
This theme captures participants’ mixed perceptions of the COVID-19 vaccine, including trust in science alongside concerns about rapid development, side effects, and institutional motives.
Subtheme 1: Confidence in science and past vaccine successes
Among those who received the vaccine, twelve participants alluded to a baseline trust in science by reflecting on historical vaccine successes and prior personal vaccination experiences. For these participants, a foundational confidence in science contributed to a sense of security and optimism about COVID-19 vaccination. One participant reflected: I’ve always had my flu shot once a year, tetanus if you scratch yourself in the dirt. So I’m familiar and happy with vaccines. (Participant 3, vaccinated)
Many framed the vaccine as a scientific milestone and a long-awaited solution to the pandemic. Consequently, participants described feelings of hope and relief upon learning that vaccines would become available. One participant shared: I was like ‘Oh, thank goodness,’ something is gonna maybe end the pandemic. (Participant 27, vaccinated)
Subtheme 2: Side effect concerns
Twenty participants, eighteen of whom received the vaccine, stated that they were fearful and uncertain about short- and long-term side effects, which contributed to hesitance in accepting the vaccine. One participant mentioned: When I started hearing about the vaccine, I wasn’t comfortable taking it at all, because I thought of all the risks that were attached to it. (Participant 8, vaccinated)
These concerns were often tied to feelings of vulnerability in the absence of long-term data. One participant revealed this concern as follows:
I just read like the history of other vaccines where maybe their effects are only felt years later. (Participant 13, vaccinated)
Likewise, an unvaccinated participant questioned: What if in 20 years, I suffer side effects? (Participant 26, unvaccinated)
Subtheme 3: Rapid development concerns
Another prominent source of hesitancy involved the unprecedented speed of vaccine development and approval. Fourteen participants, all of whom were vaccinated, questioned whether safety protocols had been bypassed and expressed scepticism about how quickly trials were completed. One participant stated: I’m suspicious, because like generally vaccines take a long time to develop. . . like years of testing and human testing and I do think these were rushed. (Participant 20, vaccinated)
Similarly, another participant expressed: There was a very big conversation right at the start about them developing it so quickly and whether that’s like viable. (Participant 28, vaccinated)
Subtheme 4: Mistrust in institutional motives
Eight participants, of whom six were vaccinated, expressed scepticism toward government and pharmaceutical companies not always rejecting the vaccine itself, but doubting the intentions behind its promotion. Demonstrating an initial major mistrust in government motives, one participant stated: We’re going to die! The government is injecting something into us! (Participant 21, vaccinated) Similarly, another participant doubted the legitimacy of government messaging: People mentioned how when the president vaccinated on camera, it looked fake. It looked like it’s water. (Participant 14, vaccinated)
Financial motives were also cited as a major source of mistrust in the pharmaceutical industry: I do think that people in charge have made millions more off of the vaccines. (Participant 20, vaccinated)
These suspicions eroded institutional trust, especially when combined with a lack of clear, consistent communication from institutional authorities. Participant 5 expressed: It was even worse when you would do your research and you would get even politicians and health specialists who are also opposing each other. (Participant 5, vaccinated)
Theme 2: Navigating a saturated information ecosystem
This theme captures how participants navigated an overwhelming and often contradictory information environment. For some, this led to initial vaccine hesitancy as they grappled with competing narratives and weighed risk.
Subtheme 1: Heightened information access: A double-edged sword
Twenty-two participants, twenty of whom were vaccinated, spoke to the COVID-19 vaccine information landscape, with social media serving as both a source of insight and major misinformation. For participants, conflicting claims and conspiracy theories often proved disorientating. One participant attributed their decision not to vaccinate to the information overload: There was so much information coming from all sides. And all of it seemed valid. Like the opposing sides seemed valid and I didn’t really know what to make of it. . . it kind of felt like it put me in a bit of a paralysis. (Participant 26, unvaccinated)
Likewise, another participant expressed: So much information, both false and true, was just out there on social media. So it took time. . . to read in between the lines and find the truth. (Participant 2, vaccinated)
Subtheme 2: Calculating risk: engaging critically to seek clarity
Twelve participants, ten of whom were vaccinated, framed themselves as active knowledge-seekers, expressing a sense of personal responsibility to think critically and make an informed choice, resulting in delayed uptake. Thus, rather than relying solely on public messaging, participants intentionally delayed getting the vaccine so they could engage in self-directed research, cross-reference multiple sources, and monitor the in-vivo effects of vaccination among others. One participant stated: I really had to sit down and do my own research to be able to make that decision for myself. (Participant 4, vaccinated)
This concern extended to observational learning, where some preferred a ‘wait and see’ approach. This involved first observing how others responded to the vaccine before acting themselves. One participant described: I remember thinking. . . I’m gonna wait and see how other people will react to it before I do it. (Participant 9, vaccinated)
Subtheme 3: Anchoring trust in reliable sources
Thirteen vaccinated participants described gaining clarity by relying more heavily on trusted information sources such as government updates, academic instruction, or credible news media: [Our president], he did another state of the nation address. That’s when he announced that they got a batch [of vaccines] coming over and how things were going to work. (Participant 1, vaccinated) Comparably, one participant mentioned:
We were watching the news religiously. (Participant 6, vaccinated)
Many participants also drew on their academic or scientific exposure, describing how being embedded in a university setting enabled access to accurate and intelligible information: In my environment, people can talk about the science [behind vaccines]. . . I was like privy to that information, and I was in a position to understand it. (Participant 1, vaccinated)
Theme 3: Low risk, low priority
This theme reflects a form of vaccine hesitancy rooted in low perceived vulnerability. A handful of participants (all of whom were vaccinated), questioned the need for vaccination or displayed ambivalence toward it. Rather than being overtly resistant, these participants described a lack of urgency or motivation to get vaccinated, suggesting that complacency, rather than concern, shaped their decision-making.
Subtheme 1: Age and health status-based complacency
Despite all ultimately becoming vaccinated, five participants considered themselves as being at low risk of contracting COVID-19 due to their age, good health, and minimal contact with others during lockdown. This perceived invulnerability led to low prioritisation of vaccination, with these participants stating that vaccination felt unnecessary or irrelevant to them as individuals. Participant 2 stated: I never thought of myself as a risk because of my young age. (Participant 2, vaccinated)
In some cases, other preventive measures (e.g. mask-wearing, online learning) were viewed as sufficient. One participant expressed: It wasn’t that I was hesitant to get it. I was just wondering if it was necessary. Because from my standpoint, I wasn’t interacting with a lot of people anyway. Having everything online, and I had no problem wearing a mask. . . So it shouldn’t have been an issue, or a necessity for me. (Participant 1, vaccinated)
Subtheme 2: Ambivalence and apathy
Nine vaccinated participants described a passive or indifferent attitude towards the vaccine, rather than active resistance. One participant shared: I don’t have any feelings about vaccination. (Participant 6, vaccinated)
In some cases, this apathy appeared to stem from a limited understanding of herd immunity or how individual decisions contribute to collective health outcomes. One participant noted: Most students were. . . either they didn’t care. Or they thought, ‘If I don’t get it, I’m just one person, it’s not going to make a difference’. (Participant 5, vaccinated)
Theme 4: Barriers and mandates
This theme captures the structural and sociocultural factors that shaped vaccine timing and uptake, including academic pressures, policy mandates, and broader social influences.
Subtheme 1: Timing: Structural and academic considerations
Among four participants, all of whom were vaccinated, academic calendars directly influenced the timing of their vaccination. Specifically, the fear of experiencing side effects amidst important academic assessments and deadlines led to strategic delays in vaccination. One participant explained: When they opened up the vaccines for people my age, it was smack bang in the middle of exams. . . I was scared that I would get side effects. . . and it will affect my ability to write or study. So that’s why initially, I didn’t get the vaccine. (Participant 2, vaccinated)
In addition to academic pressures, eight participants stated that structural rollout timelines limited access for ‘young adults’. Several participants referenced this staged access as a delaying factor: It was the elderly and the immune-compromised, and then the retirees and then. . . middle-aged people, and then it was us. So it took a long time to be our turn. (Participant 1, vaccinated)
Two participants also contextualised this delay in relation to South Africa’s status as a LMIC. One participant shared: I was very realistic about when it would be available. . . knowing our capabilities of, you know, manufacturing and distributing. . . and also our experience with the AIDS medication. (Participant 5, vaccinated)
Notably, despite these initial structural challenges, once vaccines became available to the age group, four participants reflected on the ease with which the vaccines were accessed. One participant stated: It was surprisingly easy to get it. . . waited maybe 10 minutes in the line, went through, I got the vaccine. (Participant 9, vaccinated)
Subtheme 2: Travel and institutional mandates as major motivators
Twelve participants, all of whom were vaccinated, stated that vaccine uptake was heavily driven by institutional or policy mandates rather than personal conviction. University requirements and travel restrictions thus acted as external pressures that tipped hesitant students towards vaccination. This was mentioned by participant 22: If you don’t get vaccinated, you can’t study. I know a few of my friends who wanted to get vaccinated but couldn’t because of their parents’ views. . . ended up just getting vaccinated so that they could continue their studies. (Participant 22, vaccinated)
Similarly, another participant reflected on travel mandates, and the university’s use of an incentive as a motivating factor towards vaccination: I think the main reason that most people vaccinated for was travelling. And I think the university gave us free airtime so that really worked. (Participant 7, vaccinated)
Subtheme 3: Cultural, political and religious considerations
A smaller subset of ten participants, all of whom were vaccinated, described cultural, religious, or political messages that shaped vaccine perceptions, often resulting in hesitancy. Reflecting on the influence of religion, one participant stated: There was so much like vaccine hesitancy in the Christian world and conspiracy theories and denial of Covid. (Participant 7, vaccinated)
Political discourse also emerged as a source of concern or confusion, with one participant mentioning: I see political parties like the African Christian Democratic Party. . . they led protests to boycott vaccines. (Participant 2, vaccinated)
Three participants further reported racialised narratives around vaccine safety and side effects. One participant reported the following concern discussed within their community: They want to kill Africans, they want to reduce our population. (Participant 3, vaccinated)
Theme 5: Vaccinating for the greater good: Responsibility and social tension
This theme captures the social motivations, interpersonal pressures, and emotional complexities that shaped vaccine perceptions. While many participants described feeling a moral duty to protect others, especially vulnerable family members, vaccine uptake was also influenced by peer and familial dynamics, ranging from encouragement to pressure. Importantly, vaccine perceptions and decisions were not always socially harmonious, resulting in social shifts, division, and relational strain.
Subtheme 1: Vaccinating for others: A sense of collective duty
Eight participants, all of whom were vaccinated, framed vaccination as a prosocial act, emphasising responsibility toward family and the broader community. This was expressed by participant 18: Get the vaccine. . . You’re saving other people. (Participant 18, vaccinated) Similarly, participant 27 stated: Whether you were at risk of COVID-19 or not, like it was kind of like your duty to take the COVID-19 vaccine. (Participant 27, vaccinated)
Among these participants, the sense of responsibility to vaccinate was largely driven by concern for vulnerable relatives. This was the case for participant 10: My gran is in her 80s. . . I want to protect her, I want to protect my mom who has chronic asthma. . . do everything that I can to make sure that the people I’m around aren’t at risk. (Participant 10, vaccinated)
Subtheme 2: The power of social influence
Nineteen participants, seventeen of whom were vaccinated, cited peer or familial influence as impacting vaccine perceptions. In some cases, vaccine acceptance was shaped by familial trust. In others, explicit pressure or group norms shaped vaccine perceptions. Indicating the influence of familial perceptions, participant 28 shared: I think because my parents were pro-vaccine, that definitely led to me being pro-vaccine. (Participant 28, vaccinated)
In contrast, participant 2 reported: I was being pressured by my family. (Participant 2, vaccinated)
Peer norms also played a major role in reinforcing vaccine-positive attitudes, as described by participant 7: Most of my friends had no issue with a Covid vaccine. . . I think my roommates and I all got it together. (Participant 7, vaccinated)
Similarly, an unvaccinated participant reflected on their peer influence: My friends didn’t believe in COVID. They thought it was a hoax. So, they were against taking the vaccine. (Participant 25, unvaccinated)
Subtheme 3: Social friction and fractures
Despite strong social motivations, vaccine decisions often resulted in conflict. Sixteen participants, fifteen of whom were vaccinated, described growing relational friction or breakdowns due to vaccine debates. Reflecting on social frustrations, one participant shared: I felt a lot of frustration with the conversations around vaccines for a big part of like COVID-19. (Participant 28, vaccinated)
For some, vaccination status even influenced dating and social interaction: If I want to go on a date with someone that says ‘I’m an unvaccinated person’, I would not want to interact with that person. It’s almost like it speaks to their personality now, of who they are. (Participant 2, vaccinated)
Others recounted the loss of friendships or tension within families: I’ve lost friendships because of Covid and the whole vaccine thing. (Participant 4, vaccinated)
Similarly, an unvaccinated participant expressed: My grandma’s sister and her son stopped talking for something like six months because of their opposing views on the vaccine. . . it actually caused a lot of conflicts in my family in South Africa. (Participant 26, unvaccinated)
Discussion
This study explored the COVID-19 vaccine perceptions of university students in the Western Cape, South Africa, during a period when vaccines were widely available. Guided by the 5C model of vaccine hesitancy (Betsch et al., 2018), the findings suggest that students weighed scientific trust, perceived risk, information overload, structural barriers, and social responsibility when deciding whether to vaccinate. Overall, the findings reinforce the importance of avoiding singular narratives about student perceptions and highlight the strong influence of sociocultural and political contexts on vaccine uptake and hesitancy. Table S1 in the Supplemental Material illustrates how our study themes map onto the 5C domains, which are fully delineated below.
Our first theme, ‘Between hope and hesitation’, maps onto the 5C model’s ‘confidence’ domain, which refers to trust in vaccine efficacy, safety, delivery systems, and the intentions of policymakers (Betsch et al., 2018). Many students conveyed a strong belief in science based on prior vaccine successes and personal experiences, echoing international findings that trust in scientific processes is a key facilitator of vaccine uptake (Achore et al., 2024). Similarly, local research by Engelbrecht et al. (2022) found that individuals with previous flu vaccine experience were more likely to accept the COVID-19 vaccine. Among participants, this scientific confidence was often associated with feelings of hope and relief, with the belief that the vaccine offered a means to reduce the number of infections.
However, despite students expressing hope and relief, anxieties surrounding the vaccine’s unknown long-term side effects and its rapid development persisted. Concerns surrounding the safety and efficacy of the vaccine given its rapid development were particularly salient. While Engelbrecht et al. (2022) clarify that the rapid vaccine progress was scientifically justified due to prior research, novel techniques, prioritisation and parallel trial funding, many participants remained sceptical. Participants’ scepticism therefore highlights the importance of transparent, accessible scientific communication within university settings, which effectively explains the unprecedented speed at which the vaccine could be developed and distributed in emergency situations. Our findings thus suggest that vaccine hesitancy in this group was not rooted in scepticism about science, but rather in the lack of clear, consistent explanations for scientific decisions that deviate from prior norms.
Institutional trust further influenced confidence. Some students voiced suspicion surrounding government and pharmaceutical motives, citing political theatre and perceived profiteering. Similar trends have been found in South African research linking vaccine attitudes to political trust (Cooper et al., 2021; Katoto et al., 2022). Such suspicion is significant in LMIC contexts such as South Africa, where a history of colonialism, apartheid, corruption and inequality has fostered scepticism toward authority (Bangalee and Bangalee, 2021; Rispel et al., 2016; Silubonde et al., 2023). This mistrust was thus not a rejection of vaccines themselves but of who was promoting them.
The second theme, ‘Navigating a saturated information ecosystem’, aligns with the ‘calculation’ component of the 5C model. Students described the information environment during the pandemic as overwhelming, contradictory, and cognitively taxing; a phenomenon recognised globally as the COVID-19 ‘infodemic’ (WHO, 2025b). While most participants did not subscribe to conspiracy theories in their entirety, participants’ decision-making was largely shaped by exposure to multiple sources, often with conflicting narratives. As such, our findings suggest that students did not passively absorb information. Instead, they engaged in active knowledge-seeking by conducting personal research, comparing sources, and monitoring peer experiences. This reflects a distinct characteristic of university students as an information-literate yet cognitively burdened group at the centre of an ‘infodemic’.
Maughan-Brown et al. (2023) note that social proof interventions in South Africa hold promise in improving vaccine uptake and overcoming safety concerns. In line with this, some participants described a ‘wait and see’ approach, observing peers’ vaccine responses before deciding. This reliance on trusted social circles emphasises the importance of social context in health decisions. While students largely consulted a multitude of sources, there were some which were perceived as more reliable than others. Specifically, several students reported anchoring trust in authoritative sources such as university instruction, national briefings, and mainstream news media. As highlighted by Shah and Wei (2022), access to and interpretation of information is not just about availability, but source credibility and information quality. Universities, thus, occupy a powerful position as both information gatekeepers and trust-builders in times of health crisis.
The third theme, ‘Low risk, low priority’, reflects the 5C domain of ‘complacency’, which arises when individuals perceive little personal risk from infection (Betsch et al., 2018). It is notable that some students dismissed their need for the vaccine based on their youth, satisfactory health-status, or commitment to existing prevention measures (e.g. social distancing, mask-wearing, online learning). This finding mirrors global reviews among student populations (Min Htike et al., 2025) and points to a unique challenge among youth populations, namely, passive hesitancy driven by apathy or ambivalence, rather than active resistance. Our findings thus suggest that vaccine messaging should centre on the collective impact of vaccination, rather than individual protection. This suggestion is supported by our fifth theme, which shows that uptake improved when vaccination was framed as serving the greater good.
The fourth theme, ‘Barriers and mandates’, connects to the ‘constraints’ domain of the 5C model, which refers to structural and psychological impediments to vaccination. Our findings demonstrate how institutional structures, particularly academic calendars and South Africa’s national COVID-19 vaccine rollout, significantly influenced the timing and motivation for vaccine uptake. Specifically, we found that students often delayed vaccination to avoid side effects during exam periods or near assessment deadlines. Our findings suggest that universities may benefit from explicitly scheduling vaccination drives around academic calendars (or vice versa) or encourage students to become vaccinated during holidays or over weekends. Additionally, South Africa’s national phased COVID-19 vaccine rollout implemented in February 2021 and prioritising healthcare workers, older and immune-compromised adults (Cooper et al., 2021), contributed to notable delays and reduced urgency among students.
Importantly, institutional mandates such as university policies and travel requirements emerged as major motivators of uptake, despite personal hesitation. However, mandates were also described as coercive by some, reflecting ethical tensions around autonomy, especially in academic settings which promote freedom of thought and are meant to foster critical inquiry. Nevertheless, as bioethical literature suggests (Giubilini et al., 2023; Savulescu et al., 2021), mandates are justifiable when threats to public health are grave and when implemented transparently and proportionately. In higher education institutions, this balance thus requires careful navigation and open communication.
Finally, the fifth theme, ‘Vaccinating for the greater good: Responsibility and social tension’ can be compared to the ‘collective responsibility’ domain of the 5C model. Many students described a sense of moral obligation to protect others, particularly older or immunocompromised family members, and viewed vaccination as a prosocial act. This altruistic framing was supported by peer norms and family influence but also gave rise to social tension. Almost all participants noted shifts in social dynamics based on vaccine perceptions, with several reporting friction or fractures in relationships with friends, dating relationships or among faith communities. While Cooper et al. (2021) describe the inherently social nature of COVID-19 vaccine hesitancy within South Africa, this finding is particularly noteworthy given that students occupy influential social roles within their peer groups, families, and broader social communities, positioning them as key agents in shaping public perceptions and health behaviours (Frieden, 2010).
Implications for public health and higher education institutions
Given universities’ dual role in health promotion and identity formation, several implications emerge. That said, the findings are also relevant, more broadly, to clinicians, counsellors, health psychologists, and public health practitioners, as they highlight how vaccine decision-making is shaped by mistrust, uncertainty, social influence, and broader contextual factors. As such, while the following implications are tailored to university settings, the findings suggest that vaccine-related communication in clinical and community settings should adopt trust-building, context-sensitive approaches that engage vaccine perceptions and decision-making with nuance rather than treating hesitancy as fixed opposition.
First, health communication should move beyond binary ‘pro/anti’ vaccine messaging. Instead, messages should acknowledge uncertainty, build trust, and validate student concerns, especially surrounding long-term safety and institutional motives. Communication surrounding scientific methods which deviate from the norm, should further be encouraged among this critically engaged and well-educated group. Second, universities can support students by teaching critical media literacy, reducing reliance on overloaded, and often misinformed, social media sources. Third, while mandates are major drivers for uptake, institutions should accompany these with incentives, transparency and dialogue to preserve students’ sense of autonomy and inclusion. Fourth, attention should be given to structural and academic considerations, including academic calendars, staged rollouts, and socio-cultural and political concerns. Tailoring timing and delivery strategies can improve accessibility and reduce passive delays among students in LMIC settings. Fifth, campaigns that frame vaccination as relational and community-oriented may more effectively appeal to student values than those based on individual risk. Finally, institutions should help students navigate social tensions that arise around vaccination within friendships, families, and communities.
Strengths and limitations
This study offers a context-specific contribution to the literature on vaccine hesitancy in South African university settings. By drawing on qualitative narratives across diverse student identities and disciplines, our study offers insight into the psychosocial nuances of vaccine perceptions among students in higher education. That said, findings should be interpreted in light of certain limitations. First, it is likely that vaccine perceptions among students have shifted with time, such as between the beginning, height and official end of the pandemic (Xiao et al., 2022). Second, as a self-report study, responses may have been shaped by social desirability bias. Third, while the sample included students in fields beyond the health sciences, future work should explore inter-faculty comparisons given known disciplinary variation in vaccine attitudes (Min Htike et al., 2025). Finally, as a qualitative study conducted within a single institutional context, the findings are not statistically generalisable but instead provide contextually situated insights that may be transferable to similar higher education and LMIC settings.
Conclusion
Although the World Health Organisation officially declared an end to the COVID-19 pandemic (WHO, 2023), vaccine hesitancy continues to pose a significant challenge to public health, with implications that extend well beyond the COVID-19 context. Our findings emphasise the importance of trust, context, and social dynamics in shaping health behaviour among university students. As higher education institutions plan for future health emergencies and vaccination efforts, engaging students as informed, complex, and socially embedded role players will be essential for building health-literate and resilient academic communities.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261457429 – Supplemental material for Exploring the perceptions of the COVID-19 vaccine among university students in South Africa: A qualitative inquiry into vaccine hesitancy and uptake
Supplemental material, sj-docx-1-hpq-10.1177_13591053261457429 for Exploring the perceptions of the COVID-19 vaccine among university students in South Africa: A qualitative inquiry into vaccine hesitancy and uptake by Phillipa Haine, Bronwyne Coetzee and Ashraf Kagee in Journal of Health Psychology
Footnotes
Acknowledgements
We would like to thank all our participants for their involvement in the study.
Ethical considerations
Ethical approval for the study was granted by the Health Research Ethics Committee of Stellenbosch University (Ref: N21/05/012-COVID-19). Participation was entirely voluntary and anonymous. Informed consent was obtained from all individuals prior to their involvement. To ensure the wellbeing of participants, contact details for free counselling services were provided should any psychological discomfort or distress arise as a result of participation in the study. No participants accessed the free counselling services. Anonymity and confidentiality were maintained through the use of participant codes and the exclusion of any personally identifiable information. All data were securely stored in password-protected digital files and backed up on OneDrive.
Consent to participate
Before commencing the interviews, participants were required to provide written informed consent to participate.
Consent for publication
Before commencing the interviews, participants were required to provide written informed consent for publication.
Author contributions
Prof. Ashraf Kagee and Prof. Bronwyne Coetzee designed and executed this project. They also oversaw conceptual planning and data collection at all stages. Dr Phillipa Haine conducted the data analysis and wrote the first draft of this manuscript. Ms Chantal Streicher, Ms Lindokuhle Shongwe and Mr Marnus Janse Van Vuuren contributed to data collection and data cleaning.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was obtained from the National Research Foundation (Grant No: 137992) and the SA Medical Research Council.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available on request via the corresponding author.
Supplemental material
Supplemental material for this article is available online.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy of any affiliated agency of the authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.