
Abstract
Unintended pregnancies can cause stress, adversely affecting maternal and child health. This study examined the impact of negative feelings about pregnancy on child developmental delays and the mediating role of social support. Data from the Japan Environment and Children’s Study, involving 73,518 mother–infant pairs, were analyzed. Feelings about pregnancy were assessed during the first trimester, while developmental delays were evaluated at 3 years using the Ages and Stages Questionnaire and social support was measured at 2.5 years postpartum. Logistic regression analysis revealed that feelings other than “very happy” were associated with higher risks of developmental delays. Mothers reporting “no specific feelings” had the strongest association (adjusted odds ratio: 1.68; 95% confidence interval: 1.41–2.00). Social support significantly reduced delays, particularly for mothers reporting “other feelings” (45.0%; 95% confidence interval: 41.0–48.3). These findings underscore the importance of social support in mitigating developmental risks linked to negative pregnancy emotions.
Keywords
Introduction
Pregnancy is a major life event that transforms the daily lives of women. Maternal mental health conditions, including depression and anxiety disorders, are common complications during pregnancy and in the postpartum period (Fawcett et al., 2019; Gavin et al., 2005). About 33% of women develop symptoms of anxiety or depression during pregnancy and 40% develop symptoms postpartum (Wisner et al., 2013). Measures to maintain good mental health for pregnant women are gaining attention, and their importance is being recognized (Ghahremani et al., 2022).
When this life event is unwanted or unintended, it can place the mother in a highly stressful situation. Multiple studies have examined the relationship of pregnancy intendedness with maternal mental health (Gharaee and Baradaran, 2020; Tokuda et al., 2021), low birth weight (Shah et al., 2011), mother–infant (Shreffler et al., 2021; Tokuda et al., 2021) or mother–child (Beumer et al., 2024) bonding, and child development in both high-income countries (Delgado-Ron and Janus, 2023) and low-and-middle-income countries (Delgado-Ron and Andrade-Rivas, 2023). The results show that unwanted or unplanned pregnancies have a negative impact on these factors. Therefore, preventing or reducing unintended pregnancies is a key public health challenge (Santelli et al., 2003).
Pregnancy intention is commonly categorized as intended, unplanned, mistimed, or unwanted (Shreffler et al., 2021). The latter three categories are considered unintended (Shah et al., 2011). Typically, pregnancy intention is assessed by asking pregnant women to reflect on their perceptions before becoming pregnant, which raises concerns about the accuracy of these responses (Shreffler et al., 2021). Additionally, perceptions of pregnancy intention are not fixed and can change during pregnancy (Santelli et al., 2003).
Therefore, it is important to assess pregnancy intention immediately after pregnancy or in the early stage. Furthermore, there is a growing view that pregnancy intention encompasses various aspects, including emotional, cognitive, cultural, and contextual factors (Santelli et al., 2003). In a recent study, pregnancy intentions were measured as a multidimensional construct, based on self-reported data on the extent of pregnancy mistiming, unwantedness, and unhappiness (Beumer et al., 2024). The results showed that mistiming and unwantedness significantly predict psychosocial problems in children, unlike unhappiness, which is related to the emotional aspect of pregnancy intention. This is likely because the question (rating “I am happy to be pregnant” on a 4-point Likert scale) may have been insufficiently posed for assessing the emotional aspect and examining the relationship with children’s psychosocial problems. The Japan Environment and Children’s Study (JECS), a large-scale birth cohort study that includes questions on feelings about pregnancy during the early pregnancy stage, found that a negative feeling about pregnancy was significantly associated with worse mother–infant bonding (Tokuda et al., 2021). However, the impact of negative feelings about pregnancy on child development was unclear.
Social support for mothers affects not only their mental health but also their child’s development (Bedaso et al., 2021; Imanishi et al., 2024; Lähdepuro et al., 2024; Malik et al., 2023). Children born to mothers with high social support during pregnancy experience fewer developmental delays (Imanishi et al., 2024), and enhancing maternal social support during this time could promote better cognitive outcomes in children (Lähdepuro et al., 2024). When considering the relationship between pregnancy intention and social support, a higher percentage of pregnant women with negative attitudes toward their pregnancy had lower social support in the second/third trimester compared with those without such attitudes (Matsumura et al., 2022). This may be because unintended pregnancies can suppress behaviors related to the mental health of pregnant women, such as attending prenatal check-ups, resulting in a lack of access to support (Nagamine et al., 2023). However, while various positive effects of social support during pregnancy have been demonstrated, the impact of social support on child development during the postpartum childcare period has not been sufficiently examined.
Taken together, these findings highlight the need to clarify the theoretical mechanisms linking pregnancy-related feelings, social support, and child developmental outcomes. Negative emotional responses to pregnancy may influence child development through maternal stress and early caregiving processes, while social support is theorized to buffer such effects. According to the stress-buffering model (Cohen and Wills, 1985), support mitigates the adverse consequences of stress, and the optimal matching perspective (Cutrona and Russell, 1990) emphasized that these buffering benefits are most evident when the type of support provided corresponds to the recipient’s particular emotional or situational needs. In the context of pregnancy, a mother’s emotional state at the time the pregnancy is recognized may therefore serve as an important cue for identifying the form of support that is most appropriate and effective. Empirical research has shown that social support reduces maternal distress and enhances caregiving (Parkes and Sweeting, 2018). Additionally, longitudinal research suggests that the timing and variability of perceived support play a crucial role in shaping maternal mental health across the postpartum period (Matsumura et al., 2023). Overall, social support may function both as a protective factor and a mediator linking early pregnancy feelings to developmental outcomes.
Therefore, we aimed, first, to clarify the impact of negative feelings about pregnancy on child development and, second, to examine the mediating effect of social support in reducing developmental delays in children using data obtained from a nationwide birth cohort study, the JECS. For the first objective, we investigated the relationship between feelings when pregnancy was identified, which were obtained from a questionnaire completed during the first trimester of pregnancy, and developmental delays using the Ages and Stages Questionnaire, Third Edition (ASQ-3). For the second objective, a mediation analysis was conducted to examine whether maternal social support when the child is 2.5 years old helps to mitigate developmental delays in children.
Methods
Study design
The JECS is an ongoing nationwide government-funded birth cohort study investigating the association of various environmental factors with children’s health and development. The design and baseline characteristics of the JECS are detailed elsewhere (Kawamoto et al., 2014; Michikawa et al., 2018). Briefly, recruitment took place between January 2011 and March 2014 at cooperating health care providers, such as obstetrics and gynecology departments and health centers, across 15 regional centers throughout Japan, including rural and urban locations. Follow-up occurred in mid/late pregnancy, at childbirth, at 1 month postpartum, and at 0.5, 1.0, 2.0, 2.5, and 3.0 years postpartum. Data were collected using self-administered questionnaires distributed to the participants or from the medical record transcriptions by physicians, midwives/nurses, and/or research coordinators.
The study protocol was reviewed and approved by the Japanese Ministry of the Environment’s Institutional Review Board on Epidemiological Studies (100910001) and the ethics committees of all participating institutions. Written informed consent was obtained from all participants. The present study was also approved by the Ethics Committees of the University of Toyama (R2024116) and the Institute of Science Tokyo (2024215). All procedures contributing to this work complied with the ethical standards of the relevant national and institutional committees on human experimentation and with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.
Study data
This study used the jecs-qa-20210401 (jecs-ta-20190930) dataset, which was first released in April 2021 and completed in February 2022 and contains data on 103,057 pregnancies. We excluded 5647, 948, and 3521 pregnancies due to multiple registrations (second or third registration of the same mother in the JECS), multiple births (twins or more), and miscarriages or stillbirths, respectively. Among the remaining 92,941 unique mother–infant pairs with singleton live births, we excluded an additional 1667 due to no response or missing data on the exposure, 13,906 due to no response to the questionnaire at 2.5 years postpartum, which included the mediator, and 3850 due to no response to the questionnaire at 3.0 years postpartum, which included the outcome, leaving 73,518 unique mother–infant pairs with singleton live births for the final analysis (Supplemental Figure 1).
Measures
Exposure
“Feelings when pregnancy was identified” were assessed during early pregnancy using the following six response options: 1 = Very happy, 2 = Unexpected but happy, 3 = Unexpected and confused, 4 = Upset, 5 = Did not have any specific feelings, and 6 = Other feelings. This single-item question is part of the standardized questionnaire used nationwide at pregnancy registration and has also been employed in previous JECS studies (e.g. Tokuda et al., 2021), supporting its relevance for epidemiological research.
Outcome
Child developmental delays at 3.0 years of age were assessed using the ASQ-3, an age-specific, structured, parent-completed, child monitoring system (Squires and Bricker, 2009). The ASQ-3 comprises a set of well-validated questionnaires that have been recommended by the United Nations Children’s Fund to verify whether children have normal neurological development (Korfmacher and Chawla, 2013). The Japanese version of the ASQ-3 has also been validated (Mezawa et al., 2019) and has already been used in several studies (Inoue et al., 2024; Matsumura et al., 2025).
The ASQ-3 assesses the following five areas of development: (a) communication: language skills, such as babbling, vocalizing, listening, and understanding; (b) gross motor: arm, body, and leg movements during movement and play; (c) fine motor: hand and finger movements; (d) problem solving: problem-solving skills, learning, and playing with toys; and (e) personal-social: self-help skills, solitary social play, and play with toys and others. Screen-positive cases for each area are defined as those with scores on or below the cut-off values (Mezawa et al., 2019). If a parent’s completion dates at 3.0 years were not within ± 1 month of the estimated delivery date, accounting for early delivery, the data were treated as missing values in accordance with the scoring guidelines.
The total number of screen-positive cases over the five developmental areas of the ASQ-3 (i.e. communication, gross motor, fine motor, problem solving, and social/interpersonal) was further calculated (thus, ranging from 0 to 5 points), and this total score was used as the outcome. For a detailed examination, each of the five developmental domains of the ASQ-3 was also examined as outcomes.
Mediator
Social support was assessed using a 3-item social support scale derived, with minor modifications, from the short (5-item) version of the ENRICHD Social Support Inventory (ESSI; Mitchell et al., 2003), which was included in the questionnaire at 2.5 years postpartum (Matsumura et al., 2023). The 5-item ESSI demonstrates good concurrent validity, as indicated by strong correlations with other established measures of social support, such as the Perceived Social Support Scale and the Inventory of Socially Supportive Behaviors (Mitchell et al., 2003). Although we used the 3-item version, because a scale can be used reliably if approximately half the items are present (Hawthorne and Elliott, 2005), both the 5-item version, characterized by a one-factor structure and high internal consistency (Cronbach’s α), and the three-item version are considered to measure the same construct. Supporting this view, confirmatory factor analysis in our sample demonstrated that the three items loaded onto a single latent factor and yielded a high Cronbach’s α value, indicating that the 3-item questionnaire functions as a unidimensional scale (Supplemental Figure 2). This characteristic aligns with the findings of our previous study (Matsumura et al., 2022). Based on this research, we divided the total score (ranging from 3 to 15) into quartiles and defined the social support received by the women as high (15, full score), upper-middle (13–14), lower-middle (10–12), and low (3–9).
Covariates
Background factors that may influence feelings when the pregnancy was identified and/or child neurodevelopment were selected as covariates. However, variables that could affect child development, such as birth weight, were not included as covariates. The covariates selected using these criteria were maternal age; pre-pregnancy BMI; parity (0, 1, and ⩾2); marital status (married or unmarried); highest educational level (⩽12, >12– < 16, or ⩾16 years); annual household income (<4, 4– < 6, or ⩾6 million JPY); employment status (yes or no); smoking status (never, quit before learning of pregnancy, quit after learning of pregnancy, current); alcohol intake (never, former, current), as assessed by the Food Frequency Questionnaire (Yokoyama et al., 2016); living with mother’s parent(s; yes or no); living with partner’s parent(s; yes or no); tertile of physical activity level (low, mid, high), as measured using the International Physical Activity Questionnaire (IPAQ; Craig et al., 2003; Murase et al., 2002); history of major psychiatric disease such as depression, anxiety, and schizophrenia (yes or no); folic acid supplementation (Gao et al., 2016); and 15 regional centers where the participants were recruited. The variables were categorized according to standard medical or common practice in Japan and/or the results of previous studies (Matsumura et al., 2024). All covariates were obtained from the self-administered questionnaire distributed during pregnancy, as mentioned above, except for parity, which was obtained from medical record transcription.
Statistical analysis
Mothers’ characteristics are summarized as frequencies (percentages) or means ± standard deviations (SDs).
To examine the association between feelings when the pregnancy was identified and child neurodevelopmental delays, crude and adjusted odds ratios (CORs and AORs) and the corresponding 95% confidence intervals (CIs) were calculated using a generalized linear regression model, with logit set as a link function. The feeling “1 = Very happy” was used as the reference. Covariates were entered into the multivariable analysis model using the forced entry method.
Missing data were treated using multiple imputations. To make this more efficient, auxiliary variables that were related to the variables being imputed were also imputed at the same time. Missing response rates were 6.73% for annual household income, 3.51%–4.27% for each ASQ-3 developmental domain, 3.11% for working status, 2.55% for parity, 1.47% for physical activity, and ⩽1.0% for all other variables. We created 10 imputed datasets using chained equations (van Buuren, 2007), and the results were combined using Rubin’s rule (Rubin, 2004).
To examine the extent to which this association was mediated by the social support level (high, upper-middle, lower-middle, and low), we calculated ORs with and without the mediator included in the model. Then, the magnitude of the mediating effect was assessed by the percentage reduction in the two models calculated using the following equation (Laaksonen et al., 2008):
The CIs for %Diff were calculated using a nonparametric bootstrap method with 400 replicates. To account for variability introduced by imputation, we adopted single imputation nested in the bootstrap percentile method, adding noise to reflect imputation uncertainty. This approach, recommended by previous studies (Brand et al., 2019; Schomaker and Heumann, 2018), provides the best statistical properties when combining multiple imputation with bootstrapping. Finally, %Diff was reported as the median along with the 95% confidence interval obtained from the bootstrap percentile method.
All data were analyzed using SAS (ver. 9.4; SAS Institute Inc., Cary, NC) and R (ver. 4.5.1; R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of
Table 1 shows the participants’ characteristics. The distribution of mothers’ feelings on identifying their pregnancy was as follows: “very happy” (49,395; 67.2%), “unexpected but happy” (17,899; 24.3%), “unexpected and confused” (4704; 6.4%), “upset” (358; 0.5%), “did not have any specific feelings” (344; 0.5%), and “other feelings” (818; 1.1%). Mothers who reported feelings other than “very happy” tended to have lower levels of social support.
Characteristics of participants according to feelings when pregnancy was identified.
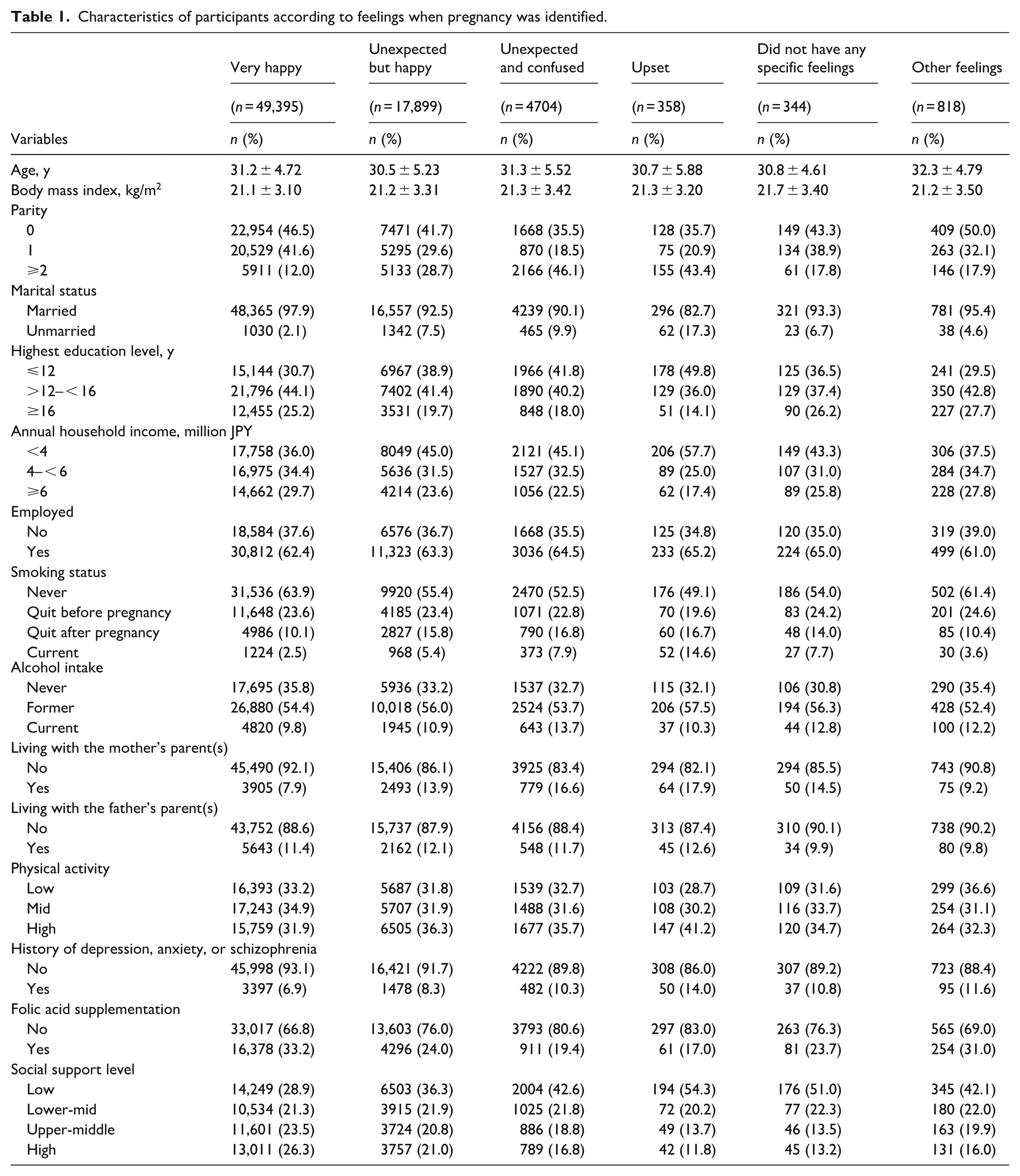
Table 2 shows the total number of screen-positive cases, CORs and AORs according to feelings when the pregnancy was identified, and the mediating effect of social support on the relationship between feelings when the pregnancy was identified and child neurodevelopmental delays. Overall, feelings other than “very happy” were associated with an increased likelihood of child neurodevelopmental delays. The strongest association was found for mothers who “did not have any specific feelings” (AOR: 1.68; 95% CI: 1.41–2.00).
Total number of screen-positive cases, crude and adjusted ORs according to feelings when pregnancy was identified, and the mediating effects of social support.
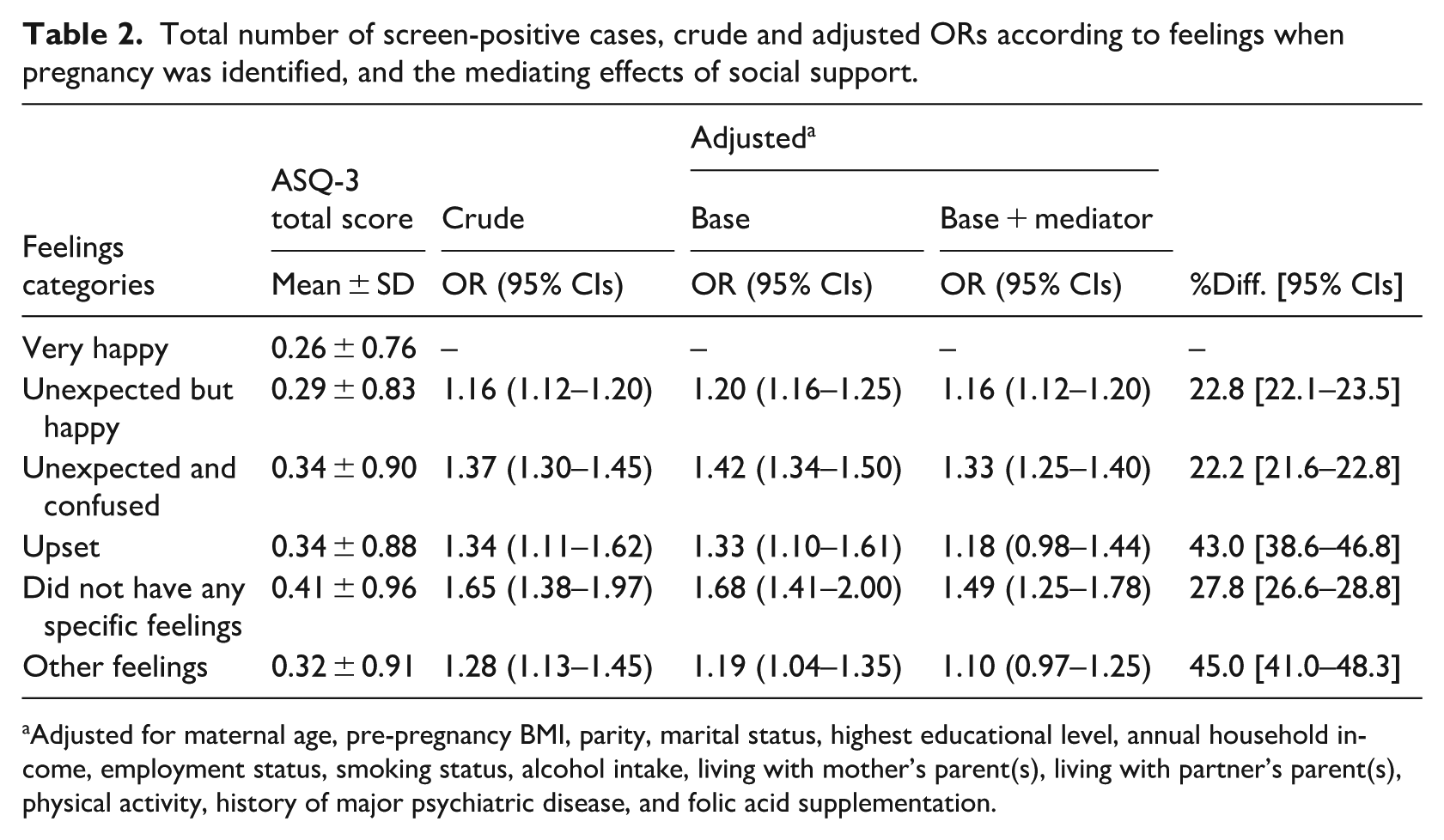
Adjusted for maternal age, pre-pregnancy BMI, parity, marital status, highest educational level, annual household income, employment status, smoking status, alcohol intake, living with mother’s parent(s), living with partner’s parent(s), physical activity, history of major psychiatric disease, and folic acid supplementation.
Regarding the mediating effect of social support, the overall effect was evident. The highest percentage of the mediating effect was observed in the “other feelings” group (%Diff: 45.0; 95% CI: 41.0–48.3), followed by the “upset” (%Diff: 43.0; 95% CI: 38.6–46.8) and “did not have any specific feelings” (%Diff: 27.8; 95% CI: 26.6–28.8) groups. Mediation was also observed in the “unexpected but happy” group (%Diff: 22.8; 95% CI: 22.1–23.5) and “unexpected and confused” group (%Diff: 22.2; 95% CI: 21.6–22.8).
Table 3 shows the results of the analysis for each of the five developmental domains of the ASQ-3. Overall, a similar trend was noted as with the total score. However, for the problem-solving domain, the strongest association was identified for mothers who reported feeling “upset” (AOR: 1.53; 95% CI: 1.08–2.17).
Prevalence, crude and adjusted ORs according to feelings when pregnancy was identified, and the mediating effects of social support.
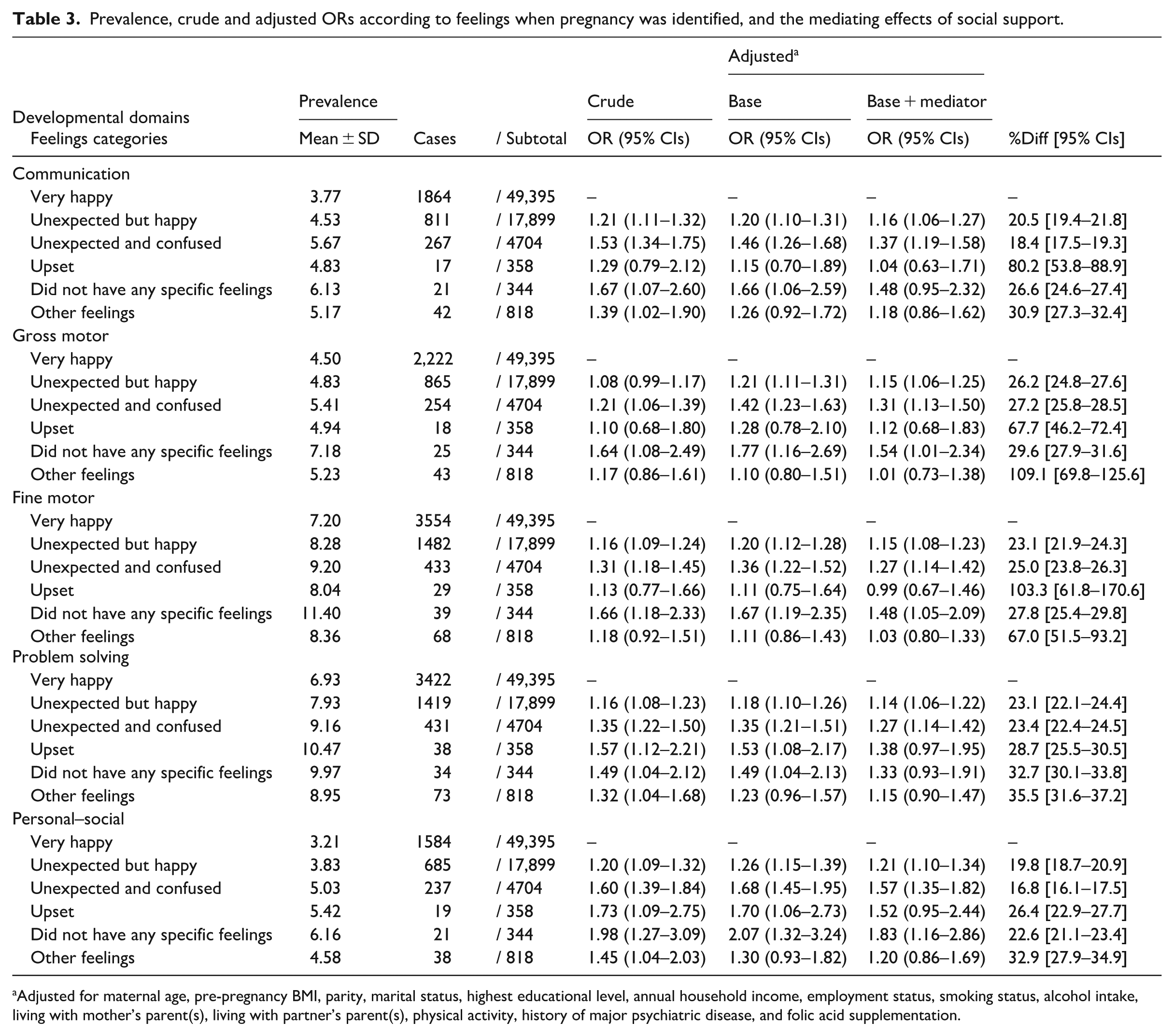
Adjusted for maternal age, pre-pregnancy BMI, parity, marital status, highest educational level, annual household income, employment status, smoking status, alcohol intake, living with mother’s parent(s), living with partner’s parent(s), physical activity, history of major psychiatric disease, and folic acid supplementation.
Regarding the mediating effect of social support, effects tended to be evident across the developmental domains, with the percentages ranging from 16.8% to 109.1%. The highest percentage of the mediating effect was observed in the “upset” group for the communication and fine motor domains and in the “other feelings” group for the gross motor, problem-solving, and personal-social domains.
Discussion
In this study, our analysis of a large dataset from the JECS national birth cohort study revealed the impact of negative feelings about pregnancy on child development up to the age of 3 years. Mothers who did not feel very happy when they found out that they were pregnant showed a higher risk of their children experiencing developmental delays compared with those who felt very happy. In particular, “unexpected and confused,” “upset,” and “did not have any specific feelings” exhibited higher risk factors. The first two responses clearly indicate negative feelings. The significant association between negative feelings about pregnancy and developmental delays can be seen as consistent with previous research that has indicated a link between pregnancy intention and developmental delays (Delgado-Ron and Andrade-Rivas, 2023; Delgado-Ron and Janus, 2023). However, the fact that those who answered “did not have any specific feelings” showed the highest risk of developmental delays is a very important finding, as it highlights the characteristics of those who may need support in the future. Furthermore, the finding that those who did not expect their pregnancy but were happy also have a risk of developmental delays supports the importance of efforts to prevent unintended pregnancies and improve the health of women and their children, as pointed out by Santelli et al. (2003).
Next, we found a mediating effect of social support on the relationship between negative feelings about pregnancy and child developmental delays. Maternal social support when the child was 2.5 years old effectively reduced developmental delays. In particular, in those who felt “upset” or “did not have any specific feelings” when they found out about their pregnancy, social support had a significant positive impact on child development. Those who felt “upset” or “did not have any specific feelings” were likely to have had unplanned pregnancies or had never considered pregnancy, indicating a lack of pregnancy intention. Among those with unintended pregnancy, there were different emotional experiences, and the effectiveness of social support was also greater for those who “did not have any specific feelings,” highlighting the need to examine the feelings of pregnant women when they find out about their pregnancy. Furthermore, although the risk of developmental delays in the group of women who answered “other feelings” was lower compared with mothers who answered “upset” and “did not have any specific feelings,” the mediating effect of social support was most pronounced in this group, a noteworthy finding in terms of the effectiveness of social support.
Participants who selected “other feelings” were asked to freely describe their feelings. Out of 818 women who chose “other feelings,” 635 provided open-ended responses. The responses suggested the complex interrelationship among various feelings, based on individual past experiences. At 40%, the most frequently mentioned topic was happiness, accompanied by anxiety or worry due to various past experiences, such as stillbirths, miscarriages, earthquakes, and infertility treatments. This suggests that these participants experienced complex and multifaceted feelings and emotions. When respondents are unable to select their feelings from the provided options and choose “other feelings,” it is crucial to listen attentively and offer support to alleviate their anxiety. Currently, in Japan, a Maternal and Child Health Handbook is provided at public health centers when pregnancy is identified. Assessment of feelings about pregnancy at this time could be useful for screening those who need social support. Previous studies have shown that those without pregnancy intention or with a negative attitude toward pregnancy are less likely to attend prenatal check-ups (Nagamine et al., 2023) or engage in maternal health behaviors (Chatterjee and Sennott, 2020), making it difficult for them to connect with the available support during pregnancy. However, childbirth is an opportunity to connect with medical institutions, and healthcare providers need to ensure that they do not overlook those who need support and engage with them accordingly.
Although social support significantly reduces developmental delays for those who “did not have any feelings” about their pregnancy, the risk remains considerably high compared with other groups. Examination of the nature of these developmental delays revealed particularly prominent delays in the personal-social domain. Personal-social factors include items such as asking the child to identify whether the child in the mirror is a boy or a girl and ensuring that the child takes turns properly, whether with other children or adults. These questions assess both the child’s self-awareness and their ability to adhere to social rules and norms. Imagining the interactions between a mother who did not feel any feelings about her pregnancy and her child, it can be anticipated that the mother’s engagement might be superficial, suggesting an environment where the child has fewer opportunities to establish self-identity and interact with others. Alongside maternal social support, improving the child’s surrounding environment by increasing interactions with adults could help to deepen the child’s understanding of themselves.
Interestingly, while the group that did not have any specific feelings about their pregnancy had the highest risk in most domains, the group that felt “upset” had the highest risk in the problem-solving domain. The feeling of being “upset” reflects a state of not knowing what to do or how to act about the pregnancy, which may be related to the pregnant woman’s low problem-solving ability. The finding that the pregnant woman’s problem-solving ability is a risk factor for developmental delays in the child’s problem-solving domain suggests that children develop problem-solving skills by observing their close caregivers. Furthermore, in this “upset” group, this risk is mitigated by social support, particularly in reducing developmental delays in the communication domain, highlighting the importance of interactions with others.
One possible mechanism by which social support when the child is 2.5 years old reduces child developmental delays is as follows. Although studies have not shown a relationship between social support during the childcare period and child development, the relationship with social support during pregnancy has been clarified, which can be useful when interpreting the effects of social support during the childcare period. Reviews of previous studies have shown that social support during pregnancy reduces anxiety and depression during pregnancy (Bedaso et al., 2021) and mitigates the relationship between depression and fear of childbirth (Zhou et al., 2021). Additionally, children born to mothers with high social support during pregnancy experience fewer developmental delays (Imanishi et al., 2024), and it is suggested that enhancing maternal social support during this time could promote better cognitive outcomes in children (Lähdepuro et al., 2024). Therefore, it is plausible to infer that the effectiveness of social support during the childcare period identified in this study improves maternal mental health by reducing anxiety and depression during this period, leading to better child development. Furthermore, because the timing and onset of anxiety and depression are higher after birth than during pregnancy (Wisner et al., 2013), the importance of social support during the childcare period, in addition to during pregnancy, can be emphasized.
This study has some limitations. First, pregnancy-related feelings were measured using a single-item question without established psychometric validation. Categories such as “no specific feelings” and “other feelings” may not fully capture the complexity of maternal emotional responses during early pregnancy, which could lead to some degree of misclassification. Although this item is widely used in routine municipal maternal health assessments in Japan and has been applied in previous JECS studies, future research would benefit from validated multi-item scales to more comprehensively assess maternal emotional states.
Second, the assessment of child development was based on the mother’s self-reports. Mothers who “did not have any feelings” about their pregnancy showed a significantly higher risk of developmental delays, and differences in attentional engagement or reporting tendencies may have influenced their evaluations. In addition, emotionally vulnerable mothers may be more prone to perceptual or reporting biases. As a result, the risk may be overestimated. It may be necessary to have individuals other than the mother evaluate the child’s development.
Third, as is common in many long-term cohort studies, the potential for selection bias should be considered. As previously described, mothers who were excluded from the current analysis were current smokers, younger, less educated, had more births, and consumed fewer folic acid supplements. This suggests that these mothers were likely to have less social support. Therefore, it is reasonable to assume that excluded mothers were inherently more likely to benefit from social support, which may have led to an underestimation of the effect. Furthermore, although no quantitative data exist, it cannot be ruled out that the individuals who agreed to participate in the survey were biased. In addition, we recruited women early in their pregnancies, meaning that those who first visited the hospital later in their pregnancies were excluded from the analysis by design. Those who start prenatal check-ups late are often those who did not intend to become pregnant (Altfeld et al., 1997), and it is possible that individuals at high risk of developmental delays are not included in this study.
In conclusion, we found that negative feelings about pregnancy contribute to child developmental delays and demonstrated that social support mitigates this relationship. Our findings highlight the importance of implementing measures to reduce unintended pregnancies and provide continuous social support to those who have negative feelings about pregnancy, especially for those who did not have any feelings about their pregnancy.
Supplemental Material
sj-docx-3-hpq-10.1177_13591053261460707 – Supplemental material for The mediating effect of social support on the relationship between negative feelings about pregnancy and child developmental delays: A nationwide birth cohort – the Japan Environment and Children’s Study
Supplemental material, sj-docx-3-hpq-10.1177_13591053261460707 for The mediating effect of social support on the relationship between negative feelings about pregnancy and child developmental delays: A nationwide birth cohort – the Japan Environment and Children’s Study by Mitsue Nagamine, Kenta Matsumura, Junko Sakai, Akiko Tsuchida and Hidekuni Inadera in Journal of Health Psychology
Supplemental Material
sj-jpg-1-hpq-10.1177_13591053261460707 – Supplemental material for The mediating effect of social support on the relationship between negative feelings about pregnancy and child developmental delays: A nationwide birth cohort – the Japan Environment and Children’s Study
Supplemental material, sj-jpg-1-hpq-10.1177_13591053261460707 for The mediating effect of social support on the relationship between negative feelings about pregnancy and child developmental delays: A nationwide birth cohort – the Japan Environment and Children’s Study by Mitsue Nagamine, Kenta Matsumura, Junko Sakai, Akiko Tsuchida and Hidekuni Inadera in Journal of Health Psychology
Supplemental Material
sj-jpg-2-hpq-10.1177_13591053261460707 – Supplemental material for The mediating effect of social support on the relationship between negative feelings about pregnancy and child developmental delays: A nationwide birth cohort – the Japan Environment and Children’s Study
Supplemental material, sj-jpg-2-hpq-10.1177_13591053261460707 for The mediating effect of social support on the relationship between negative feelings about pregnancy and child developmental delays: A nationwide birth cohort – the Japan Environment and Children’s Study by Mitsue Nagamine, Kenta Matsumura, Junko Sakai, Akiko Tsuchida and Hidekuni Inadera in Journal of Health Psychology
Footnotes
Acknowledgements
We are grateful to the participants of the JECS and to all individuals involved in the data collection process. Members of the JECS Group as of 2024: Michihiro Kamijima (Principal Investigator, Nagoya City University, Nagoya, Japan), Shin Yamazaki (National Institute for Environmental Studies, Tsukuba, Japan), Maki Fukami (National Center for Child Health and Development, Tokyo, Japan), Reiko Kishi (Hokkaido University, Sapporo, Japan), Chiharu Ota (Tohoku University, Sendai, Japan), Koichi Hashimoto (Fukushima Medical University, Fukushima, Japan), Chisato Mori (Chiba University, Chiba, Japan), Shuichi Ito (Yokohama City University, Yokohama, Japan), Ryoji Shinohara (University of Yamanashi, Chuo, Japan), Hidekuni Inadera (University of Toyama, Toyama, Japan), Takeo Nakayama (Kyoto University, Kyoto, Japan), Ryo Kawasaki (Osaka University, Suita, Japan), Yasuhiro Takeshima (Hyogo Medical University, Nishinomiya, Japan), Seiji Kageyama (Tottori University, Yonago, Japan), Narufumi Suganuma (Kochi University, Nankoku, Japan), Shoichi Ohga (Kyusyu University, Fukuoka, Japan), and Takahiko Katoh (Kumamoto University, Kumamoto, Japan).
Ethical considerations
The study protocol was reviewed and approved by the Japanese Ministry of the Environment’s Institutional Review Board on Epidemiological Studies (100910001) and the ethics committees of all participating institutions. The present study was also approved by the Ethics Committees of the University of Toyama (R2024116) and the Institute of Science Tokyo (2024215).
Consent to participate
Written informed consent was obtained from all participants. All procedures contributing to this work complied with the ethical standards of the relevant national and institutional committees on human experimentation and with the Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.
Consent for publication
Not applicable as there was no identifying data contained in this article.
Author contributions
Mitsue Nagamine: Conceptualization, Methodology, Formal analysis, Writing–Original Draft. Kenta Matsumura: Conceptualization, Methodology, Formal analysis, Writing–Original Draft, Visualization. Junko Sakai: Writing–Review & Editing. Akiko Tsuchida: Investigation, Writing–Review & Editing. Hidekuni Inadera: Writing–Review & Editing, Supervision, Project administration. The JECS group: Investigation, Resources, Data Curation, Review & Editing, Supervision, Project administration, Funding acquisition. All authors approved the submission of the manuscript in its current form.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The JECS was funded by the Ministry of the Environment, Japan. The funding source played no role in the study’s design, collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit this paper for publication. The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the above government.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are unsuitable for public deposition due to the ethical restrictions and legal framework of Japan. It is prohibited by the Act on the Protection of Personal Information (Act No. 57 of 30 May 2003, amendment on 9 September 2015) to publicly deposit data containing personal information. Ethical Guidelines for Medical and Health Research Involving Human Subjects enforced by the Japanese Ministry of Education, Culture, Sports, Science and Technology and the Ministry of Health, Labor and Welfare also restrict the open sharing of epidemiologic data. All inquiries about access to data should be sent to
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.