
Abstract
Osteogenesis Imperfecta (OI) is a rare disorder causing bone fragility, pain, and functional impairment that causes substantial psychosocial burden. This study examined how self-perceived burden (SPB), or distress from feelings of dependence on caregivers, relates to depression, anxiety, and suicidality in adults with OI. A total of 208 adults (M age = 42.9, predominately White and female) with OI were recruited to complete a cross-sectional survey assessing SPB, psychological symptoms, health, and sociodemographics. Results indicated that SPB was significantly higher among younger individuals, those not living with a partner, those living with adult family members, lower-income groups, and individuals unable to work due to health-related concerns. SPB was positively associated with pain, disability, and worse global health scores, and independently predicted depressive and anxiety symptoms, but not suicidality. Findings suggest SPB contributes to mental health burden in OI and that addressing it may improve psychological outcomes and quality of life.
Keywords
Introduction
Osteogenesis imperfecta (OI) is a rare genetic disorder typically caused by pathogenic variants in COL1A1 and COL1A2 (Tauer et al., 2019), which encode type 1 collagen, a key structural component of bone. These variants impair collagen production, resulting in bone fragility, recurrent fractures, skeletal deformities, and other systemic manifestations, including blue sclerae, dentinogenesis imperfecta, and hearing loss, among others (Schindeler et al., 2022; Subramanian et al., 2024; Tauer et al., 2019). Global prevalence is estimated between 1 in 15,000 to 1 in 20,000 (Deguchi et al., 2021), with substantial clinical heterogeneity across its subtypes (Rauch and Glorieux, 2004; Tauer et al., 2019; Westerheim et al., 2024). OI is classified into multiple subtypes based on clinical severity, radiographic features, and genetic etiology. The most widely used clinical classification system categorizes OI into Types I-IV based on severity and phenotypic presentation. Type I is the mildest and most common form; Type II is typically perinatally lethal; Type III is typically the most severe surviving form, characterized by numerous fractures, short stature, and progressive bone deformities; Type IV presents with intermediate severity (Tauer et al., 2019). Treatment includes bisphosphonate therapy to enhance bone density, orthopedic interventions for fractures and deformities, multidisciplinary pain management, and physical therapy to maintain mobility and muscle strength (MedlinePlus Medical Encyclopedia, n.d.; Subramanian et al., 2024).
OI profoundly affects health-related quality of life (HRQoL), with individuals frequently reporting chronic pain, reduced mobility, and fear of fractures, alongside psychosocial challenges such as social isolation, negative self-image, disease-related distress, and stigma (Cho et al., 2024; Rork et al., 2023; Wehrli et al., 2023). Individuals with OI often experience difficulties with daily activities, lower educational and employment opportunities, and impaired emotional well-being (Dahan-Oliel et al., 2016). Studies have found significantly lower HRQoL scores among both children and adults with OI when compared to healthy populations, particularly in physical and social domains (Dahan-Oliel et al., 2016; Wehrli et al., 2023). Depression and anxiety may also be more prevalent in this population, driven by limitations in independence, body image concerns, and uncertainty surrounding future health (Shepherd et al., 2024; Tosi et al., 2015; Wehrli et al., 2023). In individuals with varied physical disabilities, experiences of chronic dependence on caregivers, reduced autonomy, and social isolation may contribute to feelings of burdensomeness, a factor associated with increased risk of suicidal ideation (Chu et al., 2017). However, mental health comorbidities in OI remain largely understudied in the literature.
Self-perceived burden (SPB), defined as the emotional distress stemming from feelings of dependence on caregivers and a diminished sense of self-worth (Cousineau et al., 2003; Wilson et al., 2017), has been recognized as a significant risk factor for psychological distress in individuals with chronic pain conditions such as cancer, arthritis, and other debilitating illnesses (Kowal et al., 2012; Wilson et al., 2007a). The distress associated with SPB has been linked to increased rates of anxiety, depression, and suicidality (Ilgen et al., 2010; Wilson et al., 2007a), and may play a critical role in poor adjustment to chronic illness and caregiving relationships (Cousineau et al., 2003; Teismann et al., 2023). SPB also exacerbates the psychological challenges faced by both patients and caregivers, influencing treatment adherence, complicating caregiving dynamics, and affecting end-of-life decision-making (Fishbain et al., 2016; Wilson et al., 2000, 2007a, 2017). In conditions like cancer and chronic pain, where the psychological burden is well-documented (Kowal et al., 2012; Wilson et al., 2007b), SPB has been shown to elevate the risk of suicidal ideation and behaviors, highlighting its potential mental health impact for those living with serious, chronic conditions (Wilson et al., 2007a). Routine clinical assessment and early identification of SPB could enable timely and tailored clinical interventions, such as caregiver support or mental health referrals, that can reduce psychological burden and improve quality of life.
Depending on OI severity and clinical needs, individuals often require extensive caregiver support to manage daily living activities and complex medical regimens. One study found that over 80% of caregivers for individuals with OI reported high home care demands, including assisting with physical therapy, managing pain, and ensuring medication safety (Wang et al., 2024b). Unpredictable fractures and ongoing caregiver demands may foster stress, guilt, anxiety and helplessness in both caregivers and individuals with OI (Hill et al., 2019, 2022; Rapoport et al., 2023). These experiences may contribute to internalized feelings of burden and distress, suggesting a potential role of SPB in the psychological health of individuals with OI.
Despite its established relevance in other chronic health conditions, the association between SPB and suicidality in individuals with OI has not yet been examined. Addressing this gap is crucial for understanding the mental health needs of individuals with OI, as experiences of chronic pain, physical dependence, and limited autonomy may uniquely contribute to SPB and mental health consequences. This study aimed to investigate whether self-perceived burden (SPB) in adults with OI is associated with increased symptoms of suicidality, depression, and anxiety, as well as how SPB may vary by sociodemographic factors. Findings from this work may inform the development of targeted psychological and caregiver-support interventions for this population.
Materials and methods
Study design and participants
This cross-sectional study included English speaking adults (18–83 years) in the United States with a self-reported OI diagnosis. Recruitment drew from prior study participants who consented to future contact, as well as from external outreach through social media, regional OI support groups, and the Osteogenesis Imperfecta Foundation listserv. All participants provided informed consent. The study was approved by the Baylor College of Medicine Institutional Review Board in compliance with the Declaration of Helsinki (IRB # H-53652).
Procedures
Interested persons completed an eligibility survey administered via REDCap, and eligible individuals were then contacted by the study team and scheduled for a video call using a HIPAA-compliant online meeting platform (i.e. Zoom). Following consent procedures, demographic information, including social and medical history, was collected along with a cross-sectional survey on their mental wellbeing, experiences with OI, medical care and treatment, and overall quality of life. After completing the study, participants were encouraged to share the study flier with others who might qualify.
Participants who scored above the cutoff grade for clinically significant depressive symptoms on the Patient Health Questionnaire 8-item (PHQ-8 ⩾ 10) were administered the following additional screening question for suicidality: “Sometimes when people experience depression, they have thoughts about no longer wanting to be here, or ending their life in some way. Is that something you have experienced?” Those who answered “yes” to the screener were administered the Ask Suicide-Screening Questions (ASQ) to assess their level of suicide risk. All assessors were trained in ASQ administration by a licensed clinical psychologist, and all elevated PHQ-8 scores, suicide screener responses, and ASQ-positive results were reviewed in real time with a clinical psychologist to confirm proper protocol was followed and to conduct a thorough safety risk assessment.
Measures
Self-perceived Burden Scale (SPBS)
The SPBS measures the degree of emotional distress individuals experience due to the perceived burden their instrumental, emotional, or financial support places on their caregivers, and it is frequently used as an outcome measure in interventional studies (Cousineau et al., 2003; Wilson et al., 2017). The SPBS conceptualizes self-perceived burden as a psychological perception of burden, and participants are asked to reflect on their feelings toward anyone providing unpaid assistance with day-to-day activities, including friends, neighbors, or family, regardless of the frequency or intensity of support. Originally developed as a 25-item questionnaire, the SPBS was later condensed into a validated 10-item short form, which demonstrates high correlation with the full version and strong internal consistency (Cousineau et al., 2003; Oeki et al., 2012; Wilson et al., 2017). In the present study, participants completed the 10-item short form, rating each item on a five-point Likert scale ranging from 1 (none of the time) to 5 (all of the time). Higher total scores reflect greater perceived burden related to the impact of their care needs on others. Internal consistency for the SPBS was excellent (α = 0.92).
Generalized Anxiety Disorder 7-item (GAD-7)
The GAD-7 is a self-reported, seven-item scale used to assess symptoms of generalized anxiety disorder. Each item asks how often, over the last 2 weeks, the respondent has been bothered by specific problems related to anxiety (e.g. “feeling nervous, anxious, or on edge”). Items are rated on a 4-point Likert scale ranging from 0 (“not at all”) to 3 (“nearly every day”), with total scores ranging from 0 to 21. Higher scores reflect more severe anxiety symptoms, with established cutoffs of 5, 10, and 15 indicating mild, moderate, and severe anxiety (National HIV Curriculum, n.d.). The GAD-7 is well-validated with demonstrated sensitivity of 89% and specificity of 82% for identifying clinically significant anxiety (Spitzer et al., 2006). In the present study, internal consistency for the GAD-7 was good (α = 0.89).
Patient Health Questionnaire 8-item (PHQ-8)
The PHQ-8 is an eight-item self-report measure designed to assess the presence and severity of depressive symptoms based on the diagnostic criteria for major depressive disorder. Respondents rate how often they have been bothered by each symptom over the past 2 weeks using a 4-point Likert scale from 0 (“not at all”) to 3 (“nearly every day”), resulting in total scores from 0 to 24 where higher scores indicate more severe depression (Kroenke et al., 2001). Severity cutoffs commonly used are 5 (mild), 10 (moderate), 15 (moderately severe), and 20 (severe depression) (Dhingra et al., 2011). In the present study, internal consistency for the PHQ-8 was good (α = 0.86).
Ask Suicide-Screening Questions (ASQ)
The ASQ is a brief, validated suicide risk screening tool developed to identify individuals who are at an increased risk for suicide. It is comprised of four yes or no questions that assess recent suicidal ideation and lifetime suicide attempt history. It asks whether, in the past few weeks, the respondent has (1) felt that they would be better off dead, (2) wished they were dead, (3) felt they wanted to kill themselves, and (4) had ever attempted suicide (National Institute of Mental Health (NIMH), n.d.). The ASQ has been validated among individuals aged 8 and older, demonstrating strong sensitivity (97%) and specificity (88%) for identifying suicide risk (Horowitz et al., 2012).
Health Assessment Questionnaire (HAQ)
The HAQ, a short form of the full Stanford Health Assessment Questionnaire, includes the HAQ Disability Index (HAQ-DI), the HAQ Patient Global Scale, and the HAQ Pain Visual Analog Scale (VAS). This tool assesses health-related quality of life in individuals with chronic illness from the individual’s perspective and has been widely used across diverse settings (Bruce and Fries, 2003). The HAQ-DI consists of 20 questions assessing perceived ability to perform daily activities, like dressing, eating, hygiene, and walking, rated from 0 (no difficulty) to 3 (unable to do). The pain VAS evaluates usual pain over the past week on a 0–100 scale, with 0 indicating no pain and 100 indicating severe pain. The HAQ Patient Global Scale measures overall health on a similar 0–100 scale, where 0 indicates feeling very well and 100 very poor.
Analytic Plan
Participants who responded “prefer not to answer/does not apply to me” on all or most items of the SPBS were excluded from analytic models because these responses precluded calculation of a meaningful SPBS total score. Differences between included and excluded participants were compared using independent samples t-tests and chi-squared tests of independence. Cohen’s d was calculated to estimate effect sizes for mean differences (0.2 = small, 0.5 = medium, 0.8 = large), and Cramer’s V was calculated to estimate effect sizes for proportion differences (0.1 = small, 0.3 = medium, 0.5 = large). Missing data patterns were assessed among those included, and multiple imputation using fully conditional specification was conducted to impute missing continuous variables, with all available data utilized as predictors in the imputation model. In alignment with guidance from Graham et al. (2007) and White et al. (2011), 25 imputed data sets were generated, and pooled estimates are reported where applicable. Descriptive statistics summarized levels of SPB as well as health and psychological symptomatology. Analyses of variance (ANOVA), independent samples t-tests, and bivariate correlations were conducted to evaluate how SPB varied across sociodemographic and clinical factors. Two multiple linear regressions evaluated whether SPB predicted depressive and anxiety symptomatology independently of health status and age. All predictors were entered simultaneously into the models, with predictors and outcomes standardized within each imputation before analysis to allow estimation of pooled standardized regression coefficients. We examined model assumptions for both regressions and found no significant multicollinearity or violations of residual normality, homoscedasticity, linearity of relationships, or influential cases. Regression predictor effect sizes were interpreted using standardized β coefficients (0.1 = small, 0.3 = medium, 0.5 = large). All data analyses were conducted using SPSS Version 30.
Results
Data preparation and participant exclusion
Of 300 individuals who completed the larger study battery, 92 were excluded from data analyses due to responding “prefer not to answer/does not apply to me” on all or most SPBS items. Notably, these excluded individuals had significantly lower depression scores [t(291) = −2.30, p = 0.011, d = −0.29], less pain [t(292) = −5.18, p < 0.001, d = 0.65], less disability [t(298) = −5.40, p < 0.001, d = −0.68], and better self-rated global health [t(287) = −3.42, p < 0.001, d = −0.44] than those retained in the final analytic sample (n = 208). Those excluded were also more likely to report living alone [χ2(1) = 27.71, p < 0.001, V = 0.30], less likely to live with a partner or spouse [χ2(1) = 4.42, p = 0.036, V = −0.12] or an unrelated adult [χ2(1) = 4.47, p = 0.035, V = −0.12], were more likely to be working and less likely to be retired or receiving/waiting for disability [χ2(9) = 29.26, p < 0.001, V = 0.31], and were more likely to report type I OI [χ2(8) = 17.20, p = 0.028, V = 0.24]. No other significant differences emerged between those included and excluded from analyses. Among the remaining 208 participants, missing data for HAQ, PHQ-8, GAD-7, and SPBS individual scale items was less than 1%, with 3.2% of total scores missing, and 14.4% of cases with at least one missing score. Little’s Missing Completely at Random test was non-significant, χ2 (52) = 51.66, p = 0.487, suggesting insufficient evidence to reject the assumption that data was missing completely at random.
Sample characteristics
Participant demographics are reported in Table 1. The average age was 42.9 years old (SD = 15.4; range 18–83). Most participants identified as White, female, heterosexual, college educated, non-Hispanic/Latino, and living with a spouse/partner. The most common self-reported OI classification was type I. Mean anxiety (GAD-7: M = 7.83, SD = 5.48), and depression (PHQ-8: M = 7.10, SD = 5.11) scores fell within the mild range. Participants reported moderate global health (M = 64.63, SD = 22.05; 0–100 scale), moderate pain over the last week (M = 50.56, SD = 26.58; 0–100 scale) and low-to-moderate functional disability (M = 1.01, SD = 0.73; 0–3 scale). Mean self-perceived burden was 24.47 (SD = 8.89; 10–50 scale), indicating moderate perceived burden. Table 2 presents means and standard deviations for individual SPBS items using raw (i.e. non-imputed) data.
Sample characteristics (N = 208).
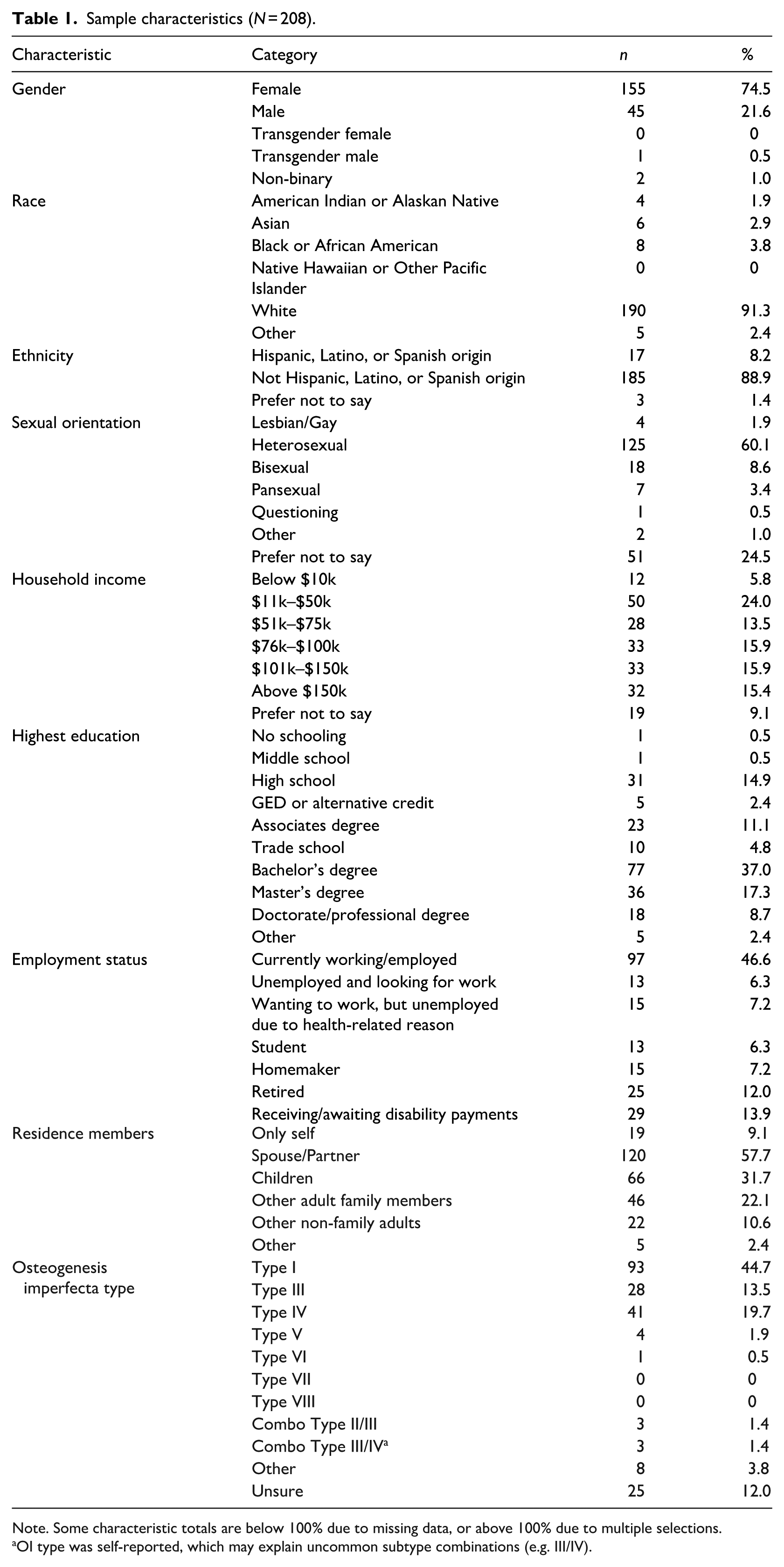
Note. Some characteristic totals are below 100% due to missing data, or above 100% due to multiple selections.
OI type was self-reported, which may explain uncommon subtype combinations (e.g. III/IV).
Self-perceived burden descriptives by scale item.
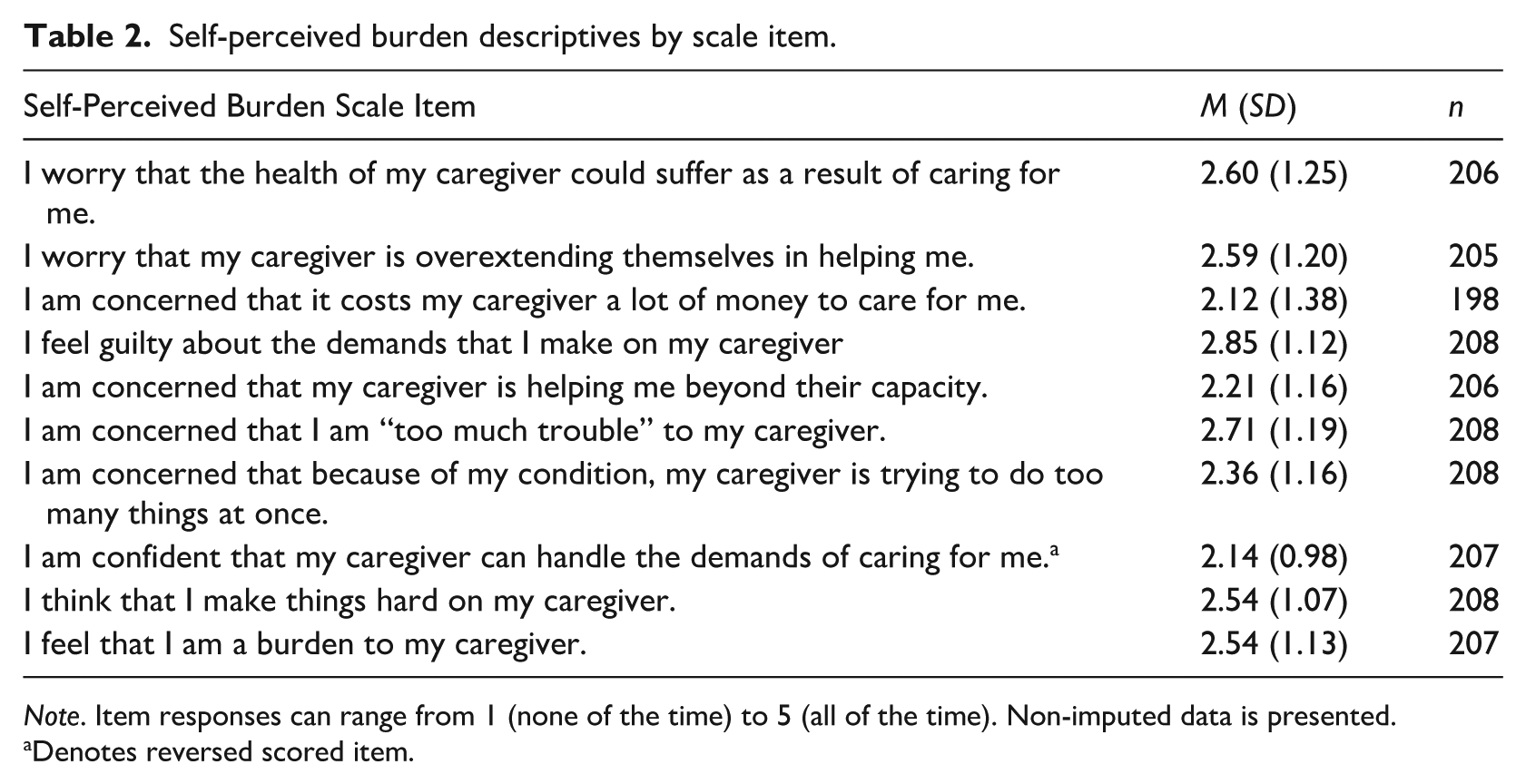
Note. Item responses can range from 1 (none of the time) to 5 (all of the time). Non-imputed data is presented.
Denotes reversed scored item.
Self-perceived burden and sample characteristics
Pooled bivariate correlations revealed that SPB was negatively associated with older age (rpooled = −0.24, p < 0.001). Participants living with a spouse/partner reported lower SPB than those who did not [tpooled (206) = −3.14, p = 0.002, d = −0.44]. In contrast, those who reported living with “other” adult family members, including parents, grandparents, and siblings, reported higher SPB than those who did not [tpooled (206) = 2.99, p = 0.003, d = 0.50]. White participants also reported lower levels of SPB [tpooled (206) = −2.07, p = 0.044, d = −0.48]. Self-perceived burden differed by annual household income [F (5,166) range 2.70 to 2.93, p range 0.014–0.022], with Bonferroni-adjusted pairwise comparisons (i.e. significance set to <0.0033) indicating higher self-perceived burden among individuals earning $11k to $50k compared with those earning over $150k (dpooled = 0.80). Additionally, SPB varied across employment status [F (6, 206) range 4.07 to 4.26, all p < 0.001]. Pairwise comparisons using Bonferroni adjustments (i.e. significance set to <0.0023 to account for 21 possible comparisons) found that those reporting they were unable to work due to a health-related reason reported higher SPB than those currently employed (dpooled = 0.84), those identifying as a homemaker (dpooled = 0.94), and those who are retired (dpooled = 1.21). Further, those identifying as a student reported higher SPB than those who are retired (dpooled = 1.04). Self-perceived burden did not differ by gender, ethnicity, having children in the house, living with other non-family member adults, having at least a 4-year college degree, or self-reported OI classification (see Supplemental Table 1). Notably, 31% of participants rejected most SPBS items, suggesting substantial heterogeneity in how SPB is experienced or conceptualized in OI.
Self-perceived burden and mental health variables
Self-perceived burden (SPB) was positively associated with anxiety and depressive symptomatology. Additionally, greater SPB was associated with worse self-rated global health and positively associated with pain and functional disability. A full correlation matrix is provided in Table 3. The regression predicting depressive symptomatology was significant [F (5, 202) range 33.55 to 38.29, all p < 0.001, R2 range 0.45–0.49] with SPB emerging as an independent, positive predictor of depressive symptomatology, with a small effect size. Additionally, the regression predicting anxiety symptomatology was also significant [F (5, 202) range 17.85 to 19.41, all p < 0.001, R2 range 0.29–0.31], with SPB also emerging as an independent, positive predictor of anxiety symptomatology, with a small effect size. Pooled regression coefficients are presented in Table 4.
Pooled bivariate correlations among variables of interest.
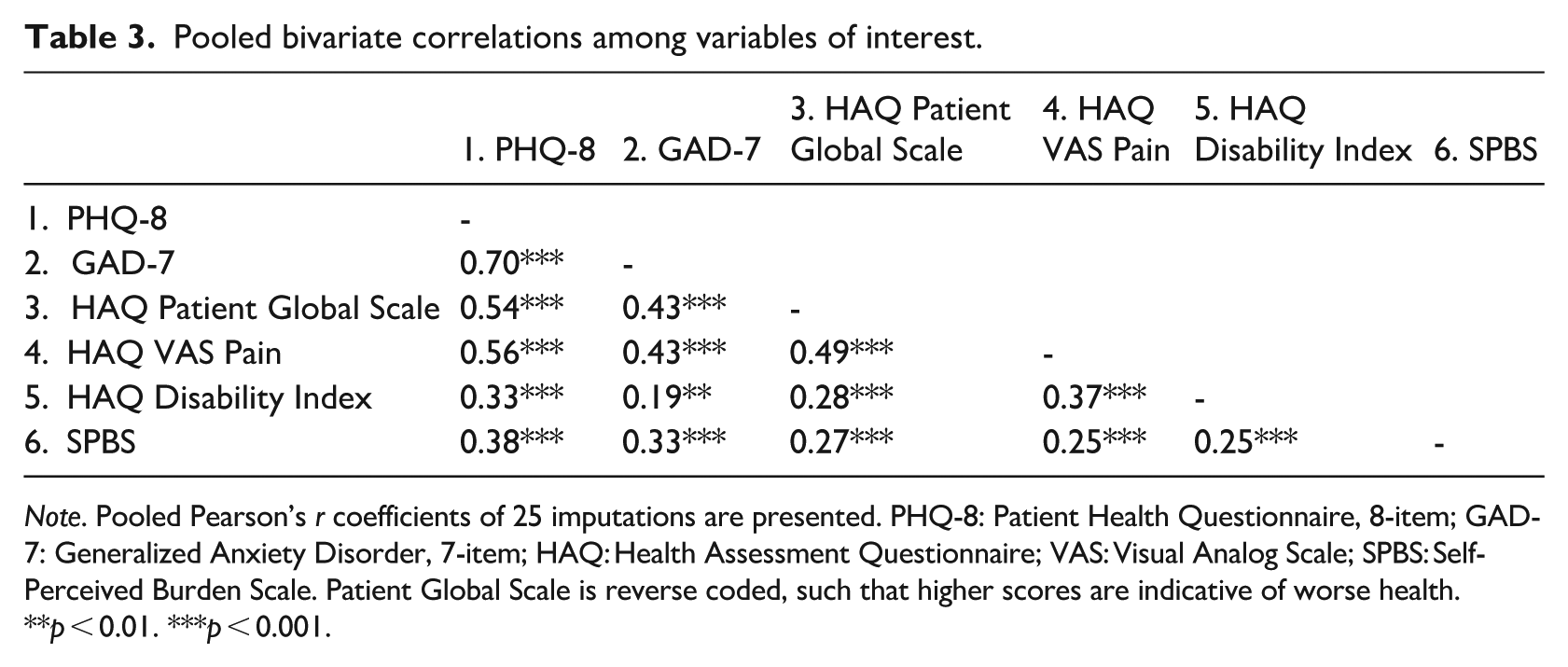
Note. Pooled Pearson’s r coefficients of 25 imputations are presented. PHQ-8: Patient Health Questionnaire, 8-item; GAD-7: Generalized Anxiety Disorder, 7-item; HAQ: Health Assessment Questionnaire; VAS: Visual Analog Scale; SPBS: Self-Perceived Burden Scale. Patient Global Scale is reverse coded, such that higher scores are indicative of worse health.
**p < 0.01. ***p < 0.001.
Pooled regression coefficients for prediction of PHQ-8 and GAD-7 scores.
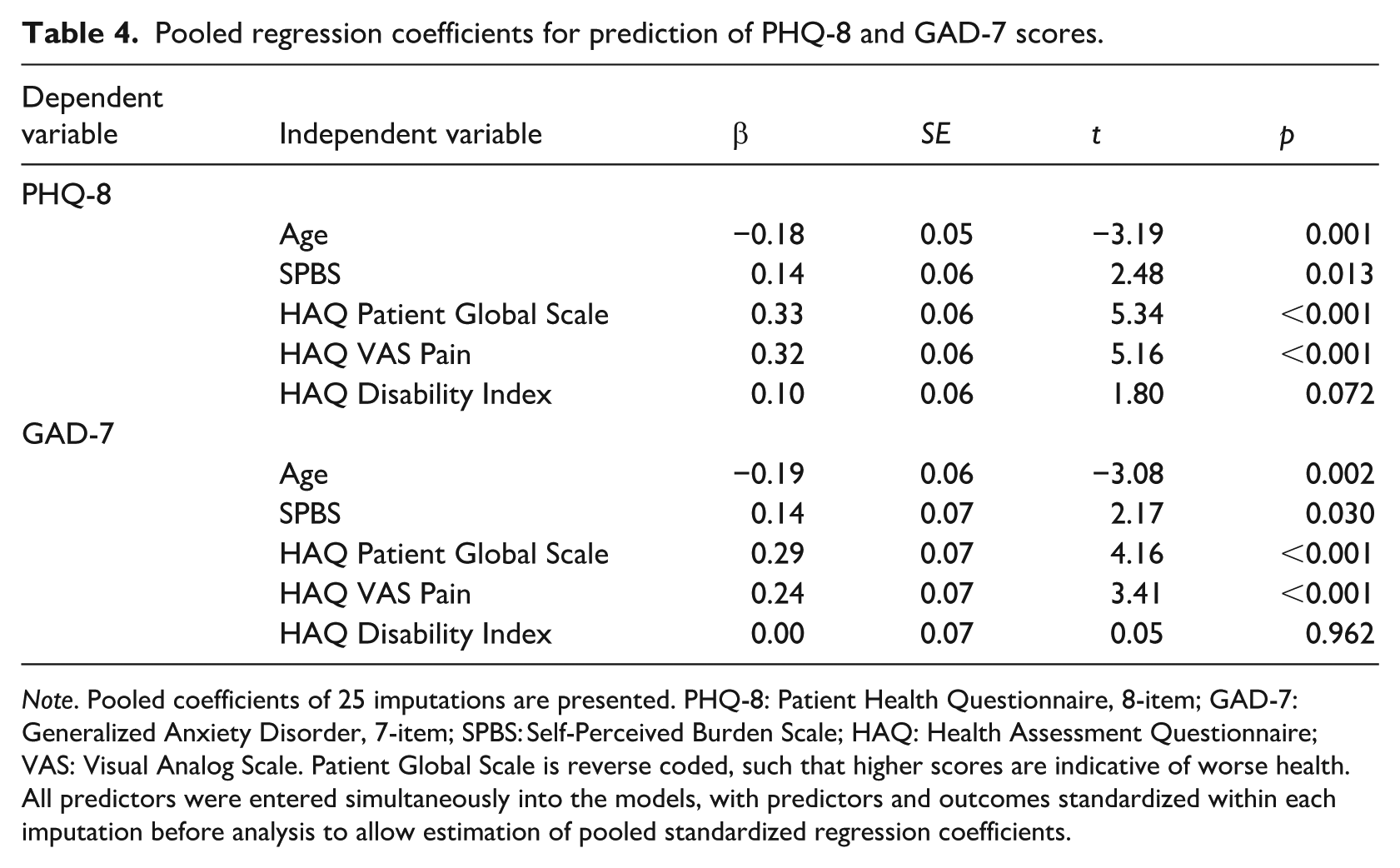
Note. Pooled coefficients of 25 imputations are presented. PHQ-8: Patient Health Questionnaire, 8-item; GAD-7: Generalized Anxiety Disorder, 7-item; SPBS: Self-Perceived Burden Scale; HAQ: Health Assessment Questionnaire; VAS: Visual Analog Scale. Patient Global Scale is reverse coded, such that higher scores are indicative of worse health. All predictors were entered simultaneously into the models, with predictors and outcomes standardized within each imputation before analysis to allow estimation of pooled standardized regression coefficients.
Of our 208 participants, 60 scored >10 on the PHQ-8 and completed subsequent suicide screening. Of these 60 participants, 26 (12.5% of the whole sample) endorsed “yes” to the lifetime suicide screener and were subsequently administered the ASQ. An independent samples t-test revealed that SPB did not significantly differ between those who did and did not endorse this screening item among the 60 assessed [tpooled (58) = 0.53, p = 0.594, d = 0.14]. At ASQ item level, one participant endorsed wishing to be dead over the past few weeks, two participants endorsed feeling they or their family would be better off if they were dead, one endorsed having suicidal ideations in the past week, and eight reported a past suicide attempt. No participant endorsed having current thoughts of suicide at the time of the survey. In total, 11 of 26 participants endorsed yes to at least one item of the ASQ, with no SPB differences between those who did and did not [tpooled (24) = −0.01, p = 0.991, d = −0.01].
Discussion
As the first study to examine SPB in adults with OI, these findings offer new insights into how self-perceived burden may relate to the sociodemographic backgrounds and psychological well-being in adults with OI. Understanding SPB in this population is especially critical given the chronic and multifaceted nature of OI, which often imposes physical, financial, and emotional demands on individuals and their caregivers (Hart et al., 2024; Tsimicalis et al., 2016; Westerheim et al., 2024).
Findings align with research in other chronic health conditions, including cancer, where SPB is associated with sociodemographic factors including financial toxicity, lower income, occupational disruption, and caregiver psychological status (Chen et al., 2023; Liu et al., 2022; Ting et al., 2020). Adults with OI in the present study showed similar patterns. Lower income and reduced autonomy (e.g. student status, inability to work due to health, younger age) were linked to greater SPB. These findings may reflect the financial burden of OI, including extensive healthcare resource use, significant out-of-pocket expenses, and frequent hospitalizations (Hart et al., 2024; Shih et al., 2024; Storoni et al., 2022). Importantly, individuals with disabilities in the United States may be forced to remain below strict income thresholds to maintain access to public insurance benefits such as Medicaid, which cover essential services including mobility devices, medications, and specialist care. Exceeding asset limits, often as low as $2000, can result in loss of coverage, forcing a choice between employment and healthcare access (Center on Budget and Policy Priorities, 2011). Limited income, reduced work experience, and decreased financial independence may amplify these pressures, contributing to increased perceived burden among affected individuals. Additionally, SPB was directly correlated with functional disability, suggesting that increased physical limitations may intensify perceptions of burden through greater caregiver reliance. Notably, prior research in the general older adult population has found that impairment in activities of daily living (ADLs) is more strongly associated with perceived burden than other domains of impairment, such as cognition and social participation, which are not significantly correlated with SPB (Mournet et al., 2020).
These results also align with previous research identifying protective sociodemographic factors associated with lower SPB, including greater social support and higher socioeconomic status (Jung et al., 2024; Nikbakht Nasrabadi et al., 2022; Wang et al., 2025). Notably, adults with OI who live with a spouse or partner reported lower SPB than those living alone or with other, non-spousal family members. Similar patterns have been observed in patients with Alzheimer’s disease (Conde-Sala et al., 2010), another condition involving caregiver dependence. This observation underscores the importance of understanding individuals’ broader social contexts, as perceptions of caregiver expectations and dependency may vary by relationship type.
White participants reported lower SPB than participants from other racial backgrounds. Although the sample lacked sufficient diversity to examine these differences in depth, this pattern may reflect broader structural and sociocultural factors shaping experiences of disability and caregiving. Differential access to healthcare resources, financial supports, and disability services may influence caregiver reliance and perceptions of dependence. Structural inequities and culturally informed norms surrounding family responsibility and interdependence may also influence experiences of burden.
Relational context also appears important. Living with a spouse or partner was associated with lower SPB, whereas living with other adult family members (e.g. parents or siblings) was associated with higher SPB. Partner relationships may involve more reciprocal caregiving and interdependence, while family-of-origin caregiving may reinforce dependency roles that heighten concerns about autonomy or role expectations. However, these associations may also reflect underlying differences in other factors, such as age, socioeconomic status, or disability severity, which may influence both living arrangements and perceptions of burden. Younger individuals also reported higher SPB, possibly reflecting developmental factors such as emerging independence. Taken together, these findings suggest that living arrangements may interact with broader social and functional factors that shape experiences of perceived burden.
Beyond individual and interpersonal factors, broader social determinants of health also influence SPB. Financial insecurity, ableism, limited paid leave or caregiver benefits, and healthcare inequities are all structural forces that can contribute to perceptions of burden (Brown and Ciciurkaite, 2022; Stoddard-Dare et al., 2018; Wang et al., 2024a). Sociodemographic factors such as age, race, ethnicity, language proficiency, and educational level may shape adjustment to chronic illness, influencing both perceived burden and mental health outcomes. For example, White, English-speaking patients often report better psychological adjustment and healthcare outcomes than minoritized patients or those for whom English is a second language (Zhang et al., 2012). Drawing on the social model of disability, which distinguishes between impairment and societal barriers that limit participation, SPB may also reflect structural constraints on independence and social inclusion, such as inaccessible workplaces or inadequate caregiver leave. Understanding SPB in OI therefore requires considering both personal experience and broader sociopolitical contexts.
Higher SPB has been associated with anxiety and depression among stroke survivors (Ren et al., 2016), individuals with movement disorders (Dempsey et al., 2012), and patients with cancer (Chen et al., 2023; Xiaodan et al., 2022). The present study suggests that this pattern extends to the OI population, with higher SPB significantly associated with greater anxiety and depression symptoms. Notably, these associations remained significant even when accounting for the effects of physical health, suggesting that SPB may contribute to psychological distress beyond functional impairment alone. Clinically, this highlights the importance of screening for mental health concerns in patients endorsing feelings of burden, regardless of their pain or disability severity. Importantly, caution is warranted in attributing psychological distress as an inevitable consequence of OI without considering the broader social and structural factors that shape one’s experience. It is important to understand burden and mental health conditions as arising from interactions between health status and environmental and social conditions including ableism and inadequate access to necessary supports.
However, there was no relationship between SPB and suicidality in this sample, contrasting with previous research identifying positive correlations between SPB and suicidality in individuals with chronic pain (Fishbain et al., 2016; Wilson et al., 2017) or other mental health conditions (Teismann et al., 2023). Importantly, only a portion of our sample was screened for suicide, and of that only a small number of participants endorsed suicidal ideation (n = 11), thus limiting our ability to adequately assess relationships between SPB and suicidality in this sample. Still, unique protective factors observed within the OI community may buffer against suicidality and psychological distress, including acceptance, self-efficacy, and cognitive reframing (Cho et al., 2024), which overlap with protective factors observed in those with anxiety and depression (Lin et al., 2020; Yu et al., 2021). Further, evidence suggests individuals born with disabilities may demonstrate stronger disability identity, self-efficacy, and life satisfaction than those with acquired disabilities (Bogart, 2014; Kim and Park, 2024; Shindi, 1983). However, additional research is needed to clarify the relationship between SPB and suicidality in individuals with OI; this relationship should be examined in future studies designed specifically to assess suicidal ideation in OI populations.
Notably, nearly one-third of participants preferred not to answer or felt that the majority of SPBS items did not apply to them. These individuals, who were excluded from analyses, reported better mental and physical health, and were more likely to be living alone and working. Although interpretation is constrained by the absence of a direct measure assessing whether participants identified as having a caregiver, these findings suggest that many individuals with OI may rely less on caregiving support or may not identify with burden narratives. Accordingly, the analytic sample reflects individuals who endorse experiences of SPB, while also highlighting meaningful variability in how caregiver dependence is perceived. Future research should examine why some individuals do not endorse burden and how this relates to psychological and health outcomes.
Overall, these insights position SPB as a meaningful clinical target that can inform screening practices, therapeutic conversations, and the delivery of more holistic, patient-centered care to the OI population. Incorporating screening tools, such as the SPBS, may help clinicians assess emotional distress while providing language for individuals to articulate their unique struggles and potential needs, which may include in-home assistance, health insurance, or mobility devices (Simmons, 2007). This may enhance communication, support shared decision-making and facilitate tailored interventions by connecting individuals to relevant resources. Recognizing SPB as a contributor to individuals’ mental health may also guide context-specific care, including structured conversations about care needs and boundaries, referrals to evidence-based psychotherapy, and efforts to address systemic barriers through workplace accommodations and asking patients directly about unmet support needs, which may help mitigate feelings of burden.
Key strengths of this study include a relatively large sample size for a rare condition, the use of validated instruments, and its status as the first to examine associations between SPB and suicidality in adults with OI. Nonetheless, limitations should be considered. The cross-sectional design precludes a casual inference between SPB and mental health outcomes. The sample was relatively homogenous with predominately White, highly educated, and female participants, which may limit generalizability. Recruitment through the OI Foundation listserv and prior research participant pools may have preferentially reached individuals more engaged in advocacy or research, potentially underrepresenting those with lower health literacy, lower educational attainment, or less engagement with OI support networks. Experiences of SPB may also vary across intersecting identities, including race, ethnicity, socioeconomic status, and disease characteristics, which can influence the internalization of burden and stigma (Bowleg, 2012; Ghosh et al., 2020). Because the study included only adults and required active online participation, findings may not generalize to children, individuals with limited digital access, or those with more severe, physically limiting disease. Additionally, SPB and mental health measures relied on self-report, which may introduce response bias, especially with sensitive topics such as suicidality. Only participants with PHQ-8 scores ⩾10 were screened for suicidality, potentially excluding individuals experiencing suicidal thoughts without meeting the depressive threshold. Because the PHQ-8 does not include a suicidality item and the ASQ is validated as a universal rather than depression-triggered screener, suicidal ideation was likely underestimated in this sample. OI diagnosis was also self-reported, without clinical and genetic confirmation. Missing SPB data further suggests possible response bias, and findings may not generalize to individuals with OI who do not identify with burden narratives or who have less severe health impacts.
Future research should examine these associations longitudinally and explore whether interventions targeting SPB improve mental health outcomes in individuals with OI. Additional efforts could help clarify the mechanisms linking SPB with psychological distress, such as perceived social support, self-worth, or treatment adherence, which could inform the development of more precise, mechanism-driven interventions. Moreover, it may be valuable to investigate how the congenital nature of OI shapes psychological adjustment and SPB compared with acquired disabilities. Finally, given that SPB is influenced by social determinants of health, future studies should include more diverse populations to examine how intersectionality shapes the experience and internalization of burden.
Conclusion
This study evaluated relationships between sociodemographic factors, self-perceived caregiver burden, and the mental health outcomes in adults with OI. Younger age, lower income, and living with non-spousal adult family members were associated with greater SPB, potentially reflecting the effects of the financial strain and reduced autonomy. Higher levels of SPB were significantly linked to greater anxiety and depression symptoms independent of age, physical disability, pain, and overall health status. However, SPB was not associated with suicidality in this sample, a finding that should be interpreted cautiously given methodological limitations. Findings also suggest a meaningful proportion of adults with OI may altogether not align with burden narratives. Collectively, these findings highlight SPB as a clinically relevant correlate of psychological well-being in adults with OI, particularly among those who identify with burden narratives. Assessing SPB in clinical care may help identify at-risk individuals and guide targeted, patient-centered interventions aimed at improving autonomy, coping, and caregiver dynamics in this rare disease population.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261460738 – Supplemental material for Self-perceived burden and mental health outcomes in adults with osteogenesis imperfecta
Supplemental material, sj-docx-1-hpq-10.1177_13591053261460738 for Self-perceived burden and mental health outcomes in adults with osteogenesis imperfecta by Emily R. Strouphauer, Camille Villar, Ryan J. McCarty, Danqi Li, Gianna M. Colombo, Brendan Lee, Chaya N. Murali, Dianne Nguyen, Sarah Sadek, Marie-Eve Robinson, Jocelyn Gomez, Michelle Fynan, V. Reid Sutton, Andrew D. Wiese and Eric A. Storch in Journal of Health Psychology
Footnotes
Ethical consideration
The study was approved by the Baylor College of Medicine Institutional Review Board in compliance with the Declaration of Helsinki (IRB # H-53652).
Consent to participate
All participants provided written informed consent prior to participation.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
ERS, CV RJM, DL, GMC, VRS, ADW, EAS, BL, members of the BBDC, CNM, DN, SS, MER, JG, and MF contributed to the conceptualization of the study. Data curation was performed by DL, GMC, and RJM. RJM conducted the formal analyses. EAS and ADW provided study supervision. ERS, CV, RJM, DL, GMC, VRS, CM, ADW, and EAS contributed to drafting the manuscript. All authors reviewed, edited, and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) and National Institute of Mental Health under Award Number U54AR068069-S1, and by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number P50HD103555 for use of the Clinical and Translational Core facilities. The Brittle Bone Disorders Consortium (1U54AR068069-0) is a part of the National Center for Advancing Translational Sciences (NCATS) Rare Diseases Clinical Research Network (RDCRN), and is funded through a collaboration between the Office of Rare Diseases Research (ORDR), NCATS, the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), the National Institute of Dental and Craniofacial Research (NIDCR), the Eunice Kennedy Shriver National Institutes of Child Health and Development (NICHD), and the National Institute of Mental Health (NIMH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Lee discloses the following relationships: research support from Safoni and Kyowa-Kirin. Dr. Murali discloses the following relationships: research support from Biomarin Pharmaceuticals. Dr. Storch reports receiving research funding to his institution from the Ream Foundation, International OCD Foundation, and NIH. He receives direct funding from the International OCD Foundation as well as MHNTI for providing trainings on treating obsessive-compulsive disorder with psychotherapy. He was a consultant for Brainsway and Biohaven Pharmaceuticals in the past 36 months. He owns stock less than $5000 in NView (for distribution of the Y-BOCS and CY-BOCS) and receives royalties from OCD Scales LLC (for distribution of the Y-BOCS and CY-BOCS). He receives book royalties from Elsevier, Wiley, Oxford, American Psychological Association, Guildford, Springer, Routledge, and Jessica Kingsley. Dr. Sutton discloses the following relationships: research funding from Ultragenyx; Osteogenesis Imperfecta Foundation Board of Directors member. Dr. Fynan discloses the following relationships: consultant for Ultragenyx; Osteogenesis Imperfecta Foundation Board of Directors member. Dr. Robinson discloses the following relationships: Ascendis Biopharma, Ipsen Biopharmaceuticals, QED therapeutics: Study grant to institution; Ultragenyx and Ipsen Biopharmaceuticals: Consultancy fees to institution.
Data availability statement
The data that support the findings of this study may be available upon request to the corresponding author. Data is not publicly available due to privacy and ethical restrictions. All persons participating in this research provided informed consent.*
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.