
Abstract
Weight bias internalisation (WBI) during preconception, pregnancy and postpartum undermines maternal health, yet factors promoting internalisation remain poorly understood. This cross-sectional study examined associations between WBI and weight stigma exposure, self-perceived weight and BMI among 511 women aged 18–45 years across reproductive stages in Western (Australia, UK, US) and non-Western (Singapore, Philippines) countries. Greater stigma exposure was consistently associated with higher WBI across all reproductive stages and countries. Higher self-perceived weight was associated with greater WBI during preconception and postpartum, but not during pregnancy. Self-perceived weight did not moderate the stigma-WBI relationship, and BMI was not independently related to WBI. Exploratory analyses revealed women in non-Western countries reported greater stigma exposure despite similar WBI levels. Findings suggest WBI is more strongly associated with stigmatisation and weight perceptions than BMI, challenging BMI-centric risk models and highlighting the need for multi-level strategies that reduce weight stigma while strengthening women’s resilience to internalisation.
Introduction
More than a physical attribute, weight is a visible marker onto which society projects ideals of health, morality and personal responsibility, especially for women (Puhl and Heuer, 2009; Ringel and Ditto, 2019). Across the globe, women are inundated with messages that pathologise larger bodies and equate thinness with worth (Abdoli et al., 2024; Rodgers et al., 2023). These ideals become especially pronounced during the reproductive periods of preconception, pregnancy and postpartum (PPP), when weight change, though essential for fertility, gestation, and infant development, is closely monitored and judged.
This societal scrutiny manifests through overlapping systems of surveillance. Healthcare providers enforce body mass index (BMI)-based weight targets that often disregard nuances in individual physiology (McAuliffe et al., 2020). Some openly shame patients or threaten to withhold preferred birth options based on weight (Basinger et al., 2023; Incollingo Rodriguez et al., 2020a). Family members make negative assumptions about health and lifestyle behaviours, often misattributing weight gain to overeating or inactivity (Nagpal et al., 2023). The media reinforce narrow ideals of ‘acceptable’ maternal bodies (Nippert et al., 2021), and strangers openly shame and police women’s appearance in public spaces, with some told they look ‘too fat to be pregnant’ (Incollingo Rodriguez et al., 2020b). The convergence of these sources creates conditions where weight stigma – the social devaluation, stereotyping and discriminatory treatment of individuals based on body size (Puhl et al., 2020) – is routine and unavoidable for many women. In fact, nearly two-thirds of women across all BMI categories report weight-based stigma during pregnancy and postpartum (Incollingo Rodriguez et al., 2020b).
Although weight stigma is well documented in pregnancy and postpartum, it also extends to preconception, defined here as the period leading up to pregnancy where women are actively trying to conceive with deliberate pregnancy planning intention (Hill et al., 2020). While this period may not involve the visible bodily changes of pregnancy or postpartum, it can involve anticipatory pressure to prepare, regulate or ‘optimise’ the body for reproduction (Hill et al., 2023). Women planning pregnancy are often encouraged to reach a ‘healthy’ weight to support fertility and future pregnancy outcomes (Harper et al., 2023), and many face BMI-based restrictions on access to fertility treatment despite limited evidence supporting such cut-offs (Caldwell et al., 2024; Koning et al., 2017). Recent evidence indicates that 62.5% of preconception women report experiencing weight stigma (Dever et al., 2026a). Across all three stages, then, weight stigma is a routine feature of women’s reproductive lives.
Such pervasive stigmatisation is consequential. Women exposed to weight stigma face greater risk of excess gestational weight gain and postpartum weight retention, as well as higher rates of depression, disordered eating and body dissatisfaction (Dever et al., 2025), factors that may cyclically influence each other. For instance, meta-analytic evidence confirms moderate associations between body dissatisfaction and depressive symptoms across pregnancy and postpartum (He et al., 2025). Importantly, these harms appear across the weight spectrum, indicating that vulnerability is driven not by body size alone but by the social meaning ascribed to weight (Incollingo Rodriguez and Nagpal, 2021). Yet despite mounting evidence of harm, weight stigma remains normalised and continues to be justified as a motivational strategy for behaviour change (Nutter et al., 2024).
Understanding that weight stigma harms women is essential to motivate reduction efforts, but insufficient to properly target societal interventions or to help women build resilience. We have limited understanding of how weight stigma engrains itself into the perinatal woman’s psyche, creating the phenomenon of weight bias internalisation (WBI), the process by which individuals accept and apply negative weight stereotypes to themselves (Durso and Latner, 2008). In particular, it remains unclear why some women are more vulnerable than others to internalisation during reproductive phases. Understanding risk factors for internalisation is important as WBI has been consistently linked to psychological and behavioural outcomes outside reproductive contexts (Bidstrup et al., 2022; Pearl and Puhl, 2018). In PPP groups, WBI has been observed among women with higher pre-pregnancy BMI and excessive gestational weight gain (Nagpal et al., 2022). It has, in turn, been associated with diminished trust in healthcare providers, and healthcare avoidance (Byrd et al., 2023), responses that may compromise both maternal and infant health. Weight bias internalisation has also been shown to mediate the relationship between postpartum weight retention and depression (Sharp et al., 2023), suggesting it acts as a psychological pathway through which weight-related experiences translate into mental health harm. However, not all women who experience weight stigma internalise it (Pearl and Puhl, 2018; Puhl et al., 2018). This variability underscores the importance of identifying factors that heighten susceptibility to WBI during PPP.
Looking across the literature, two factors represent promising points of departure for filling the gap in understanding vulnerability to WBI during PPP: the extent of weight stigma exposure and self-perceived body weight (SPBW). First, while much PPP research has honed in on a single source of stigma, such as healthcare interactions or family criticism, many women encounter weight stigma across multiple domains simultaneously (Incollingo Rodriguez et al., 2020b). The accumulation of negative messages from multiple sources may create an environment where stigmatising attitudes become increasingly difficult to dismiss, paving the way for internalisation. Indeed, Pearl et al. (2018) found that exposure to weight stigma from a greater number of interpersonal sources was associated with higher WBI among adults with obesity (N = 178; 87.6% female). Second, self-perceived body weight – that is, how women subjectively assess their body size irrespective of objective weight measures (Gardner, 2012) – may lower the threshold for self-directing negative messages about weight. Research outside the PPP context suggests that self-perceived weight is a stronger predictor of WBI than BMI (Puhl et al., 2018). Self-perceived weight also serves as the gatekeeper for other outcomes of the weight stigma sequelae. For instance, women who perceive themselves as heavier exhibit heightened cortisol responses to weight-related rejection (Himmelstein et al., 2015), stress-induced overeating (Robinson et al., 2015), and weight gain over time despite weight-loss efforts (Haynes et al., 2018).
Although the associations between weight stigma exposure, self-perceived weight and WBI are not unique to PPP, how the reproductive period shapes these relationships remains unclear. Preconception, pregnancy, and postpartum are each marked by distinct bodily expectations, social pressures and sources of weight-based scrutiny. Recent evidence suggests that dominant sources of weight stigma may differ across these stages, with media-related stigma most strongly linked to WBI during preconception, workplace stigma during pregnancy and family-based stigma during postpartum (Dever et al., 2026a). General-sample research is not designed to capture these stage-contingent patterns. Examining weight stigma exposure and self-perceived weight across PPP is therefore warranted, with direct implications for when, where and how to intervene across the reproductive timeline.
In the particular context of the PPP stages, self-perceived body weight may be especially salient as women compare their changing bodies to stage-specific body size expectations. For instance, during preconception, body optimisation messages may heighten the perceived significance of weight before pregnancy has even begun (McPhail et al., 2016). During pregnancy, women face contradictory imperatives: gain enough weight to support foetal development, but not so much as to be deemed ‘excessive’ or unhealthy (American College of Obstetricians and Gynecologists (ACOG), 2013). Postpartum, in turn, brings pressure to return to pre-pregnancy size even at the expense of recovering from childbirth (Hodgkinson et al., 2014). Women who compare their own, unique experience of PPP body transformations to these often unrealistic and unnuanced stage-specific benchmarks may perceive their bodies as larger, independent of actual weight. Having a higher SPBW may consequently heighten risk for internalising stigmatising messages. Yet whether SPBW moderates the stigma-WBI relationship during these transitions remains unknown, and clarifying this interaction is essential for targeted prevention.
Despite growing recognition that weight stigma threatens maternal health (Incollingo Rodriguez and Nagpal, 2021), important gaps in our understanding prevent us from protecting women most at risk for internalising that stigma and perhaps exacerbating the health threat. First, despite the distinct weight-related pressures that characterise preconception, most research has focused on pregnancy or postpartum, with preconception largely excluded, limiting upstream understanding of vulnerability to internalisation at the outset of the reproductive continuum. Second, existing studies have been conducted almost exclusively in Western contexts (Dever et al., 2025), precluding generalisations to maternal health in non-Western spaces. Early evidence from Asian and European populations suggests similar underlying WBI processes (Serap and Bilge, 2023; Sun et al., 2022), yet it is unknown whether associations among stigma exposure, self-perceived weight and WBI are consistent across differing societal contexts. These gaps represent missed opportunities to identify women at heightened risk during a period that shapes lifelong health trajectories.
The present study directly addressed these gaps by examining psychosocial risk factors associated with WBI across preconception, pregnancy and postpartum stages. Specifically, we investigated: (1) the association between weight stigma exposure and WBI across PPP stages; (2) whether self-perceived weight is associated with WBI and moderates the stigma-WBI relationship, controlling for BMI to isolate the unique contribution of subjective weight perceptions beyond objective weight status; and (3) whether these patterns differ between Western (Australia, US, UK) and non-Western (Singapore, Philippines) countries. This work overall aimed to elucidate whether cumulative stigma exposure and subjective weight perceptions are related to WBI during reproductive transitions across country contexts. The ultimate goal was to provide reliable guiding evidence for future research and prevention efforts targeting those most at risk.
Method
Study design and participants
An online cross-sectional study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (von Elm et al., 2008; see Supplemental Table S1). Participants were women aged 18–45 years in one of three reproductive stages: preconception (defined as actively trying to conceive; Hill et al., 2020), currently pregnant (at any gestational age), or postpartum (within 24 months of giving birth; Lipsky et al., 2012). The inclusion age range was selected to align with the typical reproductive period commonly used in maternal health research (Temmesen et al., 2023). Additional eligibility criteria included English literacy, internet access and residence in Australia, United Kingdom, United States, Singapore, or Philippines. For exploratory cross-regional comparison, countries were categorised as Western (Australia, United Kingdom, United States) and non-Western (Singapore, Philippines) contexts. This grouping enabled preliminary examination of potential regional differences in weight bias internalisation, given the extensive literature on thin-ideal promotion and weight stigma towards women during reproductive periods in Western contexts (Abdoli et al., 2024; Hailu et al., 2024) and the limited but emerging evidence from non-Western regions experiencing increasing obesity prevalence and documented weight-related discrimination (Mathialagan and Lau, 2024; Tee and Voon, 2024), which remain underrepresented in reproductive weight stigma research.
Procedure
Ethical approval was obtained from Monash University Human Research Ethics Committee (ID: 38307). Data were collected in August 2023 via an online survey administered through a Qualtrics research panel (Qualtrics, Provo, UT). Country selection was informed by panel availability. Eligible participants were recruited using quota-based convenience sampling to ensure representation across reproductive stages and countries. Upon accessing the survey, participants were presented with an explanatory statement outlining the study’s purpose and procedures. Written informed consent was obtained from all participants, indicated by their voluntary continuation into the survey after reading the explanatory statement. The anonymous online questionnaire took approximately 30 minutes to complete and was adapted with stage-appropriate terminology for each reproductive group. Data quality was ensured through IP address verification and embedded attention checks. Participants who completed the survey received compensation in accordance with Qualtrics’ standard panel rates.
Measures
Participants provided demographic information including age, reproductive history (gravidity and parity), marital status, country of residence, ethnicity and education level. Body mass index (BMI) was calculated from self-reported height and weight using the standard formula (weight in kg/height in m2). BMI was categorised according to World Health Organization (2025) guidelines as underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (⩾30.0 kg/m2).
Weight stigma exposure
Weight stigma exposure (WSE) was assessed via a 10-item checklist capturing whether participants had experienced stigma related to their weight across a range of interpersonal and societal contexts. Adapted from previous studies in pregnancy and postpartum samples (Incollingo Rodriguez et al., 2020a; Nagpal et al., 2023), the measure was further expanded for preconception and piloted (n = 10) to ensure clarity and relevance. Participants indicated whether or not they had experienced weight stigma from each source (e.g. immediate or extended family, friends, partners, healthcare providers, workplace (employers or co-workers), strangers, the media, other pregnant or postpartum women and the wider community). The number of sources selected was summed to create a continuous score (range: 0–10), reflecting exposure across multiple sources. The measure showed acceptable internal consistency (Cronbach’s α = 0.74; see Supplemental Table S2 for stage-specific values).
Self-perceived body weight
Self-perceived body weight (SPBW) was assessed using a single item: ‘How do you perceive your body weight right now?’ Response options included seven categories: Very Thin, Somewhat Thin, Slightly Thin, Average, Slightly Heavy, Moderately Heavy and Very Heavy. Due to small cell sizes at both extremes of the distribution, we first collapsed the seven categories into four groups (see Table 1): Thin, Average, Slightly Heavy and Moderate/Very Heavy. For analysis, we further dichotomised these into two theoretically meaningful groups of roughly equal size: participants who selected Thin or Average in one group (n = 294, 58%) and those who responded Slightly Heavy or Moderate/Very Heavy in another group (n = 217, 42%). This classification distinguishes between individuals who perceive themselves as having excess body weight versus those who do not–a threshold that prior work has found to be psychologically useful for identifying vulnerability to weight stigma (Himmelstein et al., 2015).
Characteristics of the study sample.
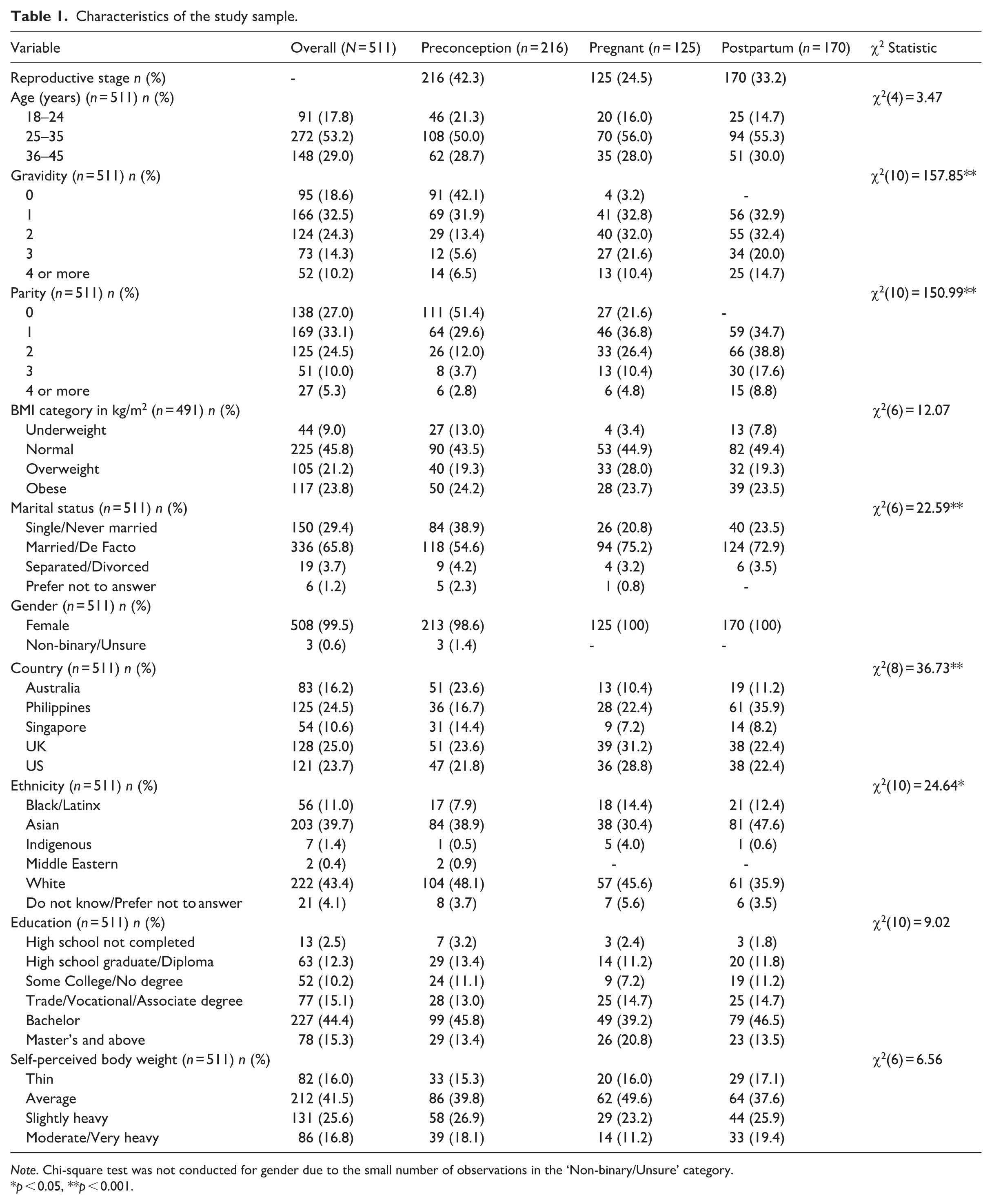
Note. Chi-square test was not conducted for gender due to the small number of observations in the ‘Non-binary/Unsure’ category.
p < 0.05, **p < 0.001.
Weight bias internalisation
Weight bias internalisation (WBI) was measured using the 18-item Weight Bias Internalisation Scale-Modified (WBIS-M; Pearl and Puhl, 2014) which was previously adapted for pregnancy and postpartum populations (Nagpal et al., 2022) and further expanded for use with preconception women in this study. The scale measures the extent to which individuals internalise negative societal attitudes about weight and apply these judgements to themselves. Participants responded to statements such as ‘I would be ashamed for people to know what I really weigh’. All items were rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores indicating greater internalisation. The scale demonstrated excellent internal consistency (Cronbach’s α = 0.94; see Supplemental Table S2 for PPP-specific values).
Data analysis
All analyses were conducted using IBM SPSS Statistics version 29 (IBM Corp., Armonk, NY, USA). A priori power analysis indicated the sample (N = 511) was adequately powered (80%) to detect small effects (f = 0.10) at α = 0.05, with up to 20 predictor variables (Incollingo Rodriguez et al., 2020a). The study was powered to detect effects across PPP stages; comparisons between Western and non-Western countries were exploratory and not included in the original power analysis. Following data quality screening, 20 cases with implausible BMI values were excluded. Missing data were minimal (<0.1% of total responses), with 11 participants each missing a single survey item. Mean substitution was applied for these missing values.
Descriptive statistics were calculated for the total sample, by reproductive stage (PPP) and by country-context (Western vs non-Western). Weight stigma exposure was calculated by summing the total number of sources endorsed by each participant (range: 0–10) and was treated as a continuous variable in all analyses. For descriptive purposes only, we also present the distribution of participants across four exposure categories: 0 (no exposure), 1–3 sources, 4–6 sources, and 7–9 sources. Categorical variables (self-perceived weight, BMI category) were compared across reproductive stages and country contexts using chi-square tests. Continuous outcomes (weight stigma exposure, WBI) were analysed with one-way ANOVAs and post-hoc Bonferroni corrections to examine differences by reproductive stage and country context. Pearson correlations examined bivariate associations among key variables.
Multiple regression models were conducted using the PROCESS macro (Model 1; Hayes, 2013) to examine main and moderating effects. Weight stigma exposure was entered as the continuous predictor variable, and WBI as the continuous outcome. Self-perceived body weight was examined as both a main effect and moderator of the stigma-WBI relationship. All models controlled for BMI as a continuous variable. Separate models were run for the full sample, and stratified by reproductive stage (PPP) and country context (Western vs non-Western). Moderation was assessed through the significance of the interaction term (weight stigma exposure × self-perceived body weight), with model variance (R2) and unstandardised regression coefficients (b) reported to quantify the strength of associations.
Results
The final sample comprised 511 women across preconception (n = 216), pregnancy (n = 125), and postpartum (n = 170) stages. Participants resided in both Western (65%) and non-Western (35%) countries. The majority of participants were aged 25–35 years (53%). BMIs were represented across standard categories: 44% normal weight, 20% overweight, and 23% obese. The sample was ethnically diverse with the largest proportions identifying as White (43%) and Asian (40%). See Table 1 for characteristics of the overall sample and by PPP status.
Weight stigma exposure and weight bias internalisation
Participants reported exposure to an average of 1.67 sources of weight stigma (SD = 1.87), with no significant differences across reproductive stages. Exploratory analysis revealed a regional difference in stigma exposure, with women in non-Western countries reporting slightly greater exposure (M = 1.97, SD = 2.08) than those in Western countries (M = 1.51, SD = 1.72; F(1,509) = 6.95, p = 0.01). Scores on WBI averaged 74.05 (SD = 22.37), indicating moderate levels of internalisation, with no significant differences across reproductive stages or country contexts (see Table 2). Overall, 63% of participants reported experiencing weight stigma from at least one source. Specifically, 37% of participants reported no stigma exposure, 46% reported 1–3 sources, 14% reported 4–6 sources, and 3% reported 7–9 sources (see Supplemental Table S3 for detailed comparisons).
Means and standard deviations for weight stigma exposure and weight bias internalisation by reproductive stage and country context.
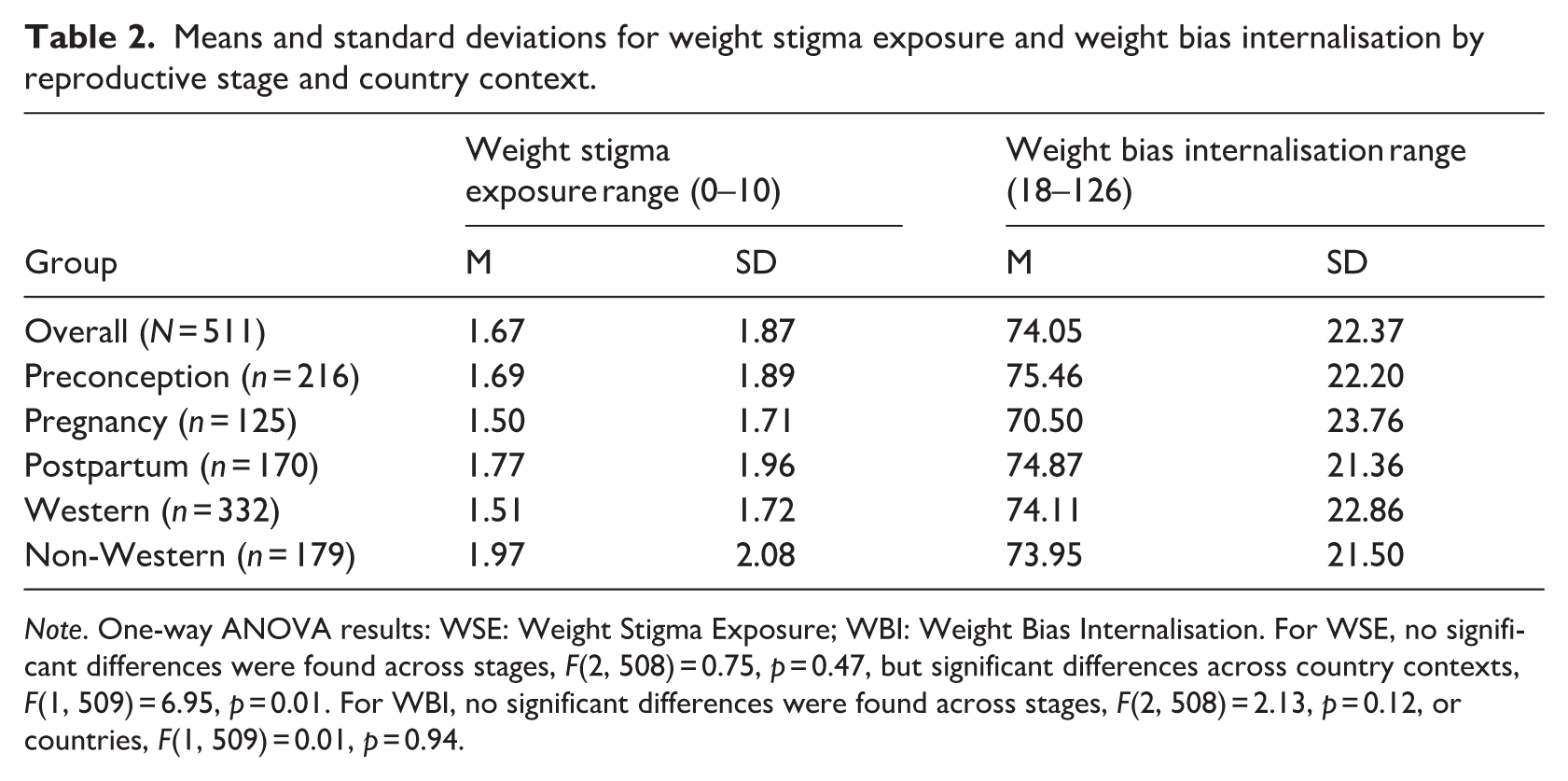
Note. One-way ANOVA results: WSE: Weight Stigma Exposure; WBI: Weight Bias Internalisation. For WSE, no significant differences were found across stages, F(2, 508) = 0.75, p = 0.47, but significant differences across country contexts, F(1, 509) = 6.95, p = 0.01. For WBI, no significant differences were found across stages, F(2, 508) = 2.13, p = 0.12, or countries, F(1, 509) = 0.01, p = 0.94.
Self-perceived body weight
Self-perceived body weight across reproductive stages and country contexts is summarised in Table 3. Overall, 58% of women perceived themselves as having a lower body weight, while 42% perceived themselves as having a higher body weight. No significant differences in self-perceived body weight were observed across reproductive stages or between Western and non-Western countries.
Self-perceived body weight [n (%)] by reproductive stage and country context.
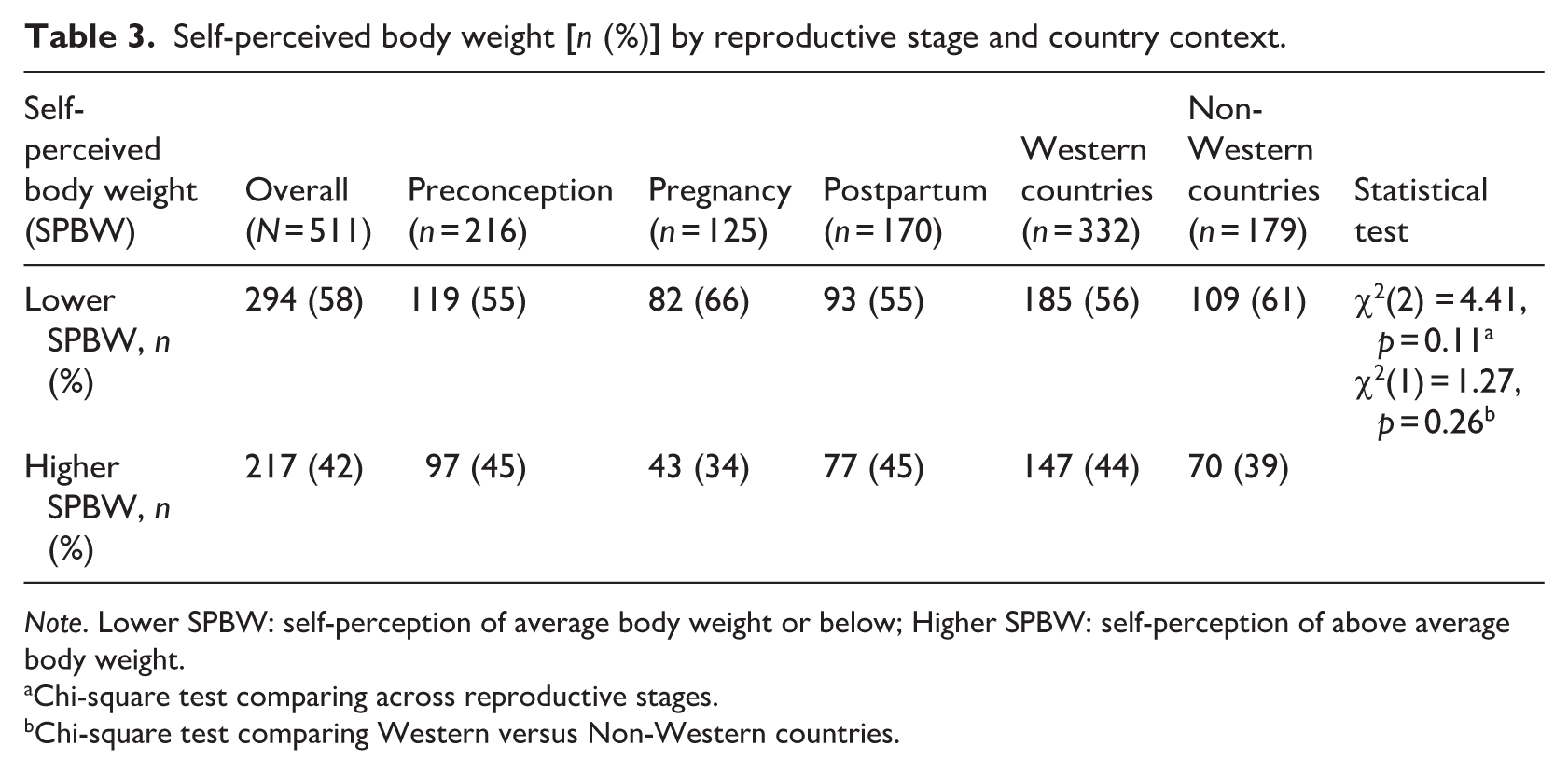
Note. Lower SPBW: self-perception of average body weight or below; Higher SPBW: self-perception of above average body weight.
Chi-square test comparing across reproductive stages.
Chi-square test comparing Western versus Non-Western countries.
Correlation analyses
Bivariate correlations between key study variables are presented in Table 4. Weight stigma exposure was significantly associated with WBI across all reproductive stages, with the strongest relationship observed during pregnancy (r = 0.52, p < 0.001) compared to preconception (r = 0.43, p < 0.001) and postpartum (r = 0.40, p < 0.001). Self-perceived body weight showed moderate correlations with BMI across all groups (r = 0.51 −0.57, p < 0.001). Weight stigma exposure was significantly associated with BMI only in the postpartum group (r = 0.17, p < 0.05).
Correlations between study variables.
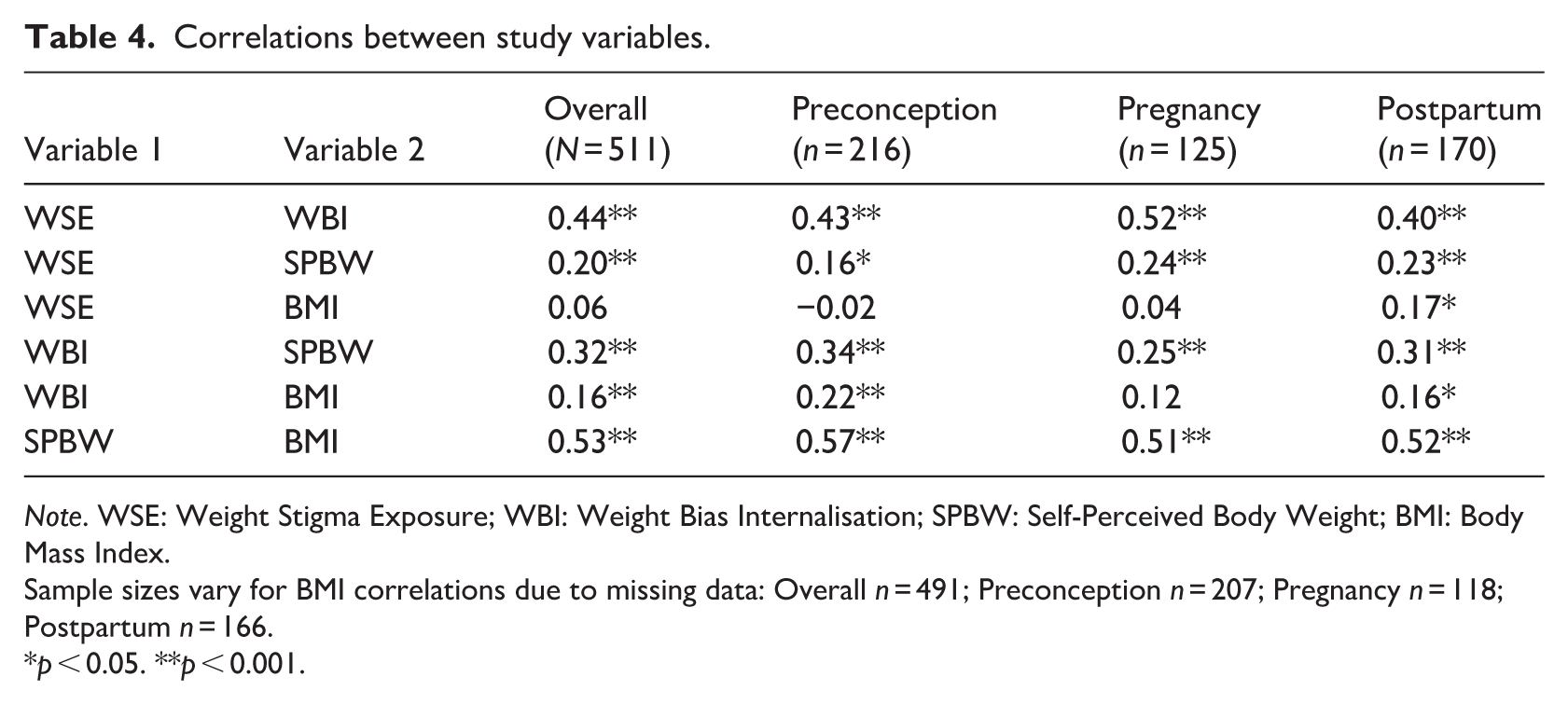
Note. WSE: Weight Stigma Exposure; WBI: Weight Bias Internalisation; SPBW: Self-Perceived Body Weight; BMI: Body Mass Index.
Sample sizes vary for BMI correlations due to missing data: Overall n = 491; Preconception n = 207; Pregnancy n = 118; Postpartum n = 166.
p < 0.05. **p < 0.001.
Factors associated with weight bias internalisation
Multiple regression examined factors associated with WBI and tested whether self-perceived body weight moderated the relationship between weight stigma exposure and WBI.
Main effects
Greater weight stigma exposure was consistently associated with higher WBI across all multivariate models. In the overall sample, greater stigma exposure was positively associated with higher WBI (b = 6.13, p < 0.001), a pattern that was evident across reproductive stages: preconception (b = 6.32, p = 0.003), pregnancy (b = 7.49, p = 0.03), and postpartum (b = 4.57, p = 0.02), as well as in both Western (b = 6.30, p < 0.001) and non-Western countries (b = 5.16, p = 0.008). Self-perceived body weight was significantly associated with WBI in the overall sample (b = 7.59, p < 0.001) controlling for BMI. Here, regardless of objective weight, individuals with higher self-perceived weight reported greater internalisation. This association was also significant among preconception (b = 7.10, p = 0.008) and postpartum participants (b = 7.92, p = 0.007), as well as in both Western (b = 8.83, p < 0.001) and non-Western countries (b = 6.09, p = 0.02). However, the association was not significant during pregnancy (b = 5.66, p = 0.09). Although BMI was positively correlated with WBI in bivariate analyses (Table 4), this relationship was no longer significant once weight stigma exposure and self-perceived weight were included in the models (preconception p = 0.31; pregnancy p = 0.10; postpartum p = 0.19; see Supplemental Table S4).
Moderation effects
Moderation analyses tested whether self-perceived body weight moderated the relationship between weight stigma exposure and WBI, controlling for BMI. The interaction term was non-significant across all models, indicating that self-perceived weight did not moderate the association between weight stigma exposure and WBI. This finding was consistent across the overall sample (b = −0.59, p = 0.21), reproductive stages [preconception (b = −0.70, p = 0.36), pregnancy (b = −0.21, p = 0.87), postpartum (b = −0.42, p = 0.53)], and both country contexts [Western (b = −0.55, p = 0.39), non-Western (b = −0.35, p = 0.61)]. Sensitivity analyses modelling SPBW as an ordinal variable (1–4) in the overall and stage-specific models yielded comparable non-significant results (b = −0.59, p = 0.21; all stage-specific p > 0.36), confirming the robustness of findings. Models explained substantial variance in WBI: Overall R2 = 0.25, Preconception R2 = 0.27, Pregnancy R2 = 0.32, Postpartum R2 = 0.22, Western countries R2 = 0.30, non-Western countries R2 = 0.21 (all p < 0.001). Full results are presented in Supplemental Tables S4 (by reproductive stage) and S5 (by country).
Discussion
This study is the first to investigate factors that may signal vulnerability for weight bias internalisation across all three reproductive stages, including the previously understudied preconception period. This work is further novel in its comparison of these associations between Western and non-Western countries. Within this framework we found that greater exposure to weight stigma from multiple sources and higher self-perceived body weight emerged as independent psychosocial risk factors for higher WBI even after controlling for BMI. These associations were generally consistent across all reproductive stages and country contexts, highlighting that the cumulative experience of stigma across sources as well as the subjective appraisals of one’s body are more closely linked to WBI than objective body size.
Indeed, women who reported experiencing weight stigma from more sources showed greater internalisation regardless of BMI. This reflects the cumulative nature of weight-based mistreatment across multiple contexts and that weight stigmatisation itself confers risk. Self-perceived body weight also emerged as a consistent independent risk factor for higher WBI across most analyses, wherein women who perceived themselves as having higher body weight tended to report greater WBI. Moreover, it is not merely the case that women with larger bodies also have higher self-perceived weight. Instead, how a woman perceives her body uniquely contributes to her internalisation of weight stigma, independent of BMI. This aligns with previous studies indicating that self-perception may be more influential than actual weight status for understanding stigma-related outcomes (Himmelstein et al., 2015; Puhl et al., 2018).
However, the association between self-perceived body weight and WBI was not observed during pregnancy, suggesting that pregnancy may temporarily attenuate the link between weight perception and internalisation. It may be that, as weight and body changes are normative to pregnancy, self-perceived weight is less engrained and trait-like during this time. In other words, a woman may notice fluctuations in her weight, but attribute this to her pregnancy rather than an enduring self-perception which drives resultant self-stigma. The temporary state nature of self-perceived weight during pregnancy may therefore be less related to more enduring levels of internalisation. It is also possible that WBI is well-established prior to pregnancy, and so fluctuating self-perceived body weight during pregnancy is less influential. Another explanation is that pregnant women may experience ‘functional appreciation’, valuing their body for what it can do (e.g. supporting foetal growth) rather than how it looks (Bień et al., 2025; Papini et al., 2022), which may relatively lessen the link between one’s perceived weight and WBI.
While stigma exposure and self-perceived weight each influenced WBI, these associations did not appear to be interactive. Self-perceived weight did not moderate the relationship between weight stigma exposure and WBI. That is, experiencing stigma from more sources was related to greater internalisation, regardless of how women viewed their own weight. Similarly, BMI was unrelated to WBI once psychosocial factors were considered. Although BMI remains relevant for assessing certain medical risks (ACOG, 2013; Institute of Medicine, 2009), it was not associated with psychological risk for weight bias internalisation. In our study, women’s subjective weight perceptions and their exposure to stigma – rather than objective weight status – emerged as key factors linked to WBI.
Exploratory cross-national comparisons revealed regional differences in stigma exposure but not in WBI levels. Women from non-Western countries reported slightly higher weight stigma exposure than their Western counterparts, despite similar levels of WBI across groups. Differences in sociocultural norms around weight-related commentary may partially explain this pattern. In collectivist societies, remarks about women’s appearance or weight are often socially sanctioned and intended as expressions of care or advice rather than criticism (Kawamura, 2012; Mathialagan and Lau, 2024), normalising frequent body commentary and potentially contributing to differences in what constitutes stigmatising behaviour. The similarity we identified in WBI across countries, despite differing exposure levels, may reflect globalisation and widespread exposure to Western media, which has been associated with the spread of similar thin ideals internationally (Al Riyami et al., 2024; Lang and Ye, 2024; Pradeilles et al., 2022; Thompson et al., 2020).
Taken together, these findings highlight that WBI during reproductive periods is more strongly associated with psychosocial risk factors than with objective indicators of body size such as BMI. The consistency of the patterns demonstrates the pervasiveness of this association, and the limitations of BMI-centric approaches to maternal health.
Clinical and policy implications
Recognising that internalisation reflects psychosocial rather than physical processes underscores the need for multi-level action that addresses both individual experiences and the systems and environments that legitimise weight stigma. Weight-inclusive healthcare policies, clinician training that moves beyond BMI-centric risk assessment and public health messaging that normalises body diversity are essential first steps to reducing the social acceptability of weight stigma. At the community level, culturally responsive education is needed to reframe body-related communication, particularly in contexts where weight commentary is intended as care or advice. Such initiatives may shift social norms and create conditions that minimise both exposure to stigma and its internalisation by increasing awareness of the psychological impact of appearance-related comments.
Within this broader framework, targeted support across the reproductive timeline can help prevent internalisation and build resilience to stigma. The preconception period – marked by heightened pressure to ‘optimise’ weight for fertility, may benefit from body-positive counselling integrated into fertility care. Pregnancy appears to offer a key opportunity: self-perceived weight was not associated with WBI during this stage, suggesting this may be a favourable period for intervention. Psychoeducational antenatal programmes that normalise bodily changes and address internalisation may capitalise on this window to build lasting resilience. Self-compassion and body acceptance interventions have demonstrated effectiveness in reducing internalised weight bias during pregnancy and postpartum (Papini et al., 2022), and broader evidence also shows that self-compassion reduces body shame among women (Haley et al., 2025; Nightingale and Cassin, 2023). Such approaches may help sustain body acceptance and prepare women for the renewed societal pressures and risk of internalisation that re-emerge postpartum.
Circumventing internalisation is a key upstream endeavour for preventing its associated psychological consequences. Our finding that self-perceived body weight was associated with WBI independently of BMI underscores the importance of subjective cognitive appraisals over objective weight measures in understanding stigma-related harm. Therapeutic approaches that help women recognise weight stigma as a form of social injustice, rather than personal inadequacy, may offer psychological support while broader systemic changes are pursued. However, such individual-level strategies should be viewed as complementary harm reduction, not primary prevention, implemented alongside broader efforts to reduce weight stigma at its source. These strategies are synergistic with emerging models for promoting body image resilience in the face of stigma, such as the Promoting Resilience in Women’s Weight Stigma Management (PRISM) model (Dever et al., 2026b), which addresses weight bias internalisation across intrapersonal, interpersonal and systemic levels. PRISM positions resilience-building not solely as an individual responsibility, but as requiring concurrent efforts to strengthen coping resources, build inclusive support systems and dismantle the structural drivers of weight stigma.
Strengths, limitations and future directions
A key strength of this study is the large, geographically diverse sample spanning all three PPP stages, which provides insights into WBI across a range of contexts, many unexplored in prior research. Additionally, assessing cumulative weight stigma exposure across multiple sources allowed us to capture a comprehensive account of women’s lived experiences with stigma, moving beyond single-source perspectives. Another strength is the incorporation of both objective (BMI) and subjective (self-perceived body weight) measures of body size, allowing us to examine their independent associations with WBI. Importantly, we tested whether self-perceived weight moderates the stigma-WBI relationship, to understand factors that heighten risk for internalisation.
Despite these strengths, the cross-sectional design precludes inference both about how WBI develops over time and about the direction of the relationships observed here. Although we have framed weight stigma exposure as a predictor of WBI consistent with prevailing conceptualisations in the literature (Pearl and Puhl, 2018), reverse pathways are plausible: women with higher WBI may be more attuned to weight-related commentary, more likely to interpret ambiguous comments as stigmatising, and therefore more likely to report exposure across multiple sources. Longitudinal designs with repeated measurement of both constructs are needed to disentangle these directional pathways and identify periods when intervention may be most needed.
Additionally, while our study included participants from multiple countries, the sample was recruited through convenience sampling and is not nationally representative. Our Western versus non-Western country groupings, while useful for exploratory comparisons, represent broad classifications that do not capture heterogeneity within groups. In this vein, although the study was adequately powered for reproductive stage comparisons, statistical power was more limited for these exploratory analyses. Accordingly, the exploratory results reported here should be used in hypothesis generation for future research seeking to expand upon these cross-context insights and pursue more definitive cultural comparisons. Future cross-national research should also include more diverse countries within each region and examine specific cultural mechanisms that contribute to stigma exposure differences.
Conclusion
Our findings demonstrate that risk for WBI is not conferred by body size alone. Rather, it is more strongly associated with how women perceive their weight and the extent of weight stigma they experience. Weight stigma exposure consistently predicted internalisation across all reproductive stages and country contexts, regardless of how women viewed their own bodies. Self-perceived body weight also independently predicted internalisation in most analyses, however, this association was not observed during pregnancy. This period therefore may be unique and warrants further inquiry to comprehensively understand how physical changes during pregnancy interact with the internalisation shuttle. The consistency of these patterns across country contexts underscores the pervasive influence of weight stigma on women’s psychological health during reproductive periods. Collectively, these findings highlight the importance of social exposure and psychological perception over objective weight measures in understanding WBI during reproductive periods. This further underscores that addressing WBI requires coordinated action across multiple levels, from systemic reform to delegitimise weight stigma in the long-term to individual resilience in the meantime. Reducing WBI necessitates transforming the social contexts that produce and sustain weight stigma, positioning this work within broader efforts to challenge weight-based discrimination as a pressing public health and social justice concern.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053261462432 – Supplemental material for Weight stigma exposure, self-perceived weight and weight bias internalisation across preconception, pregnancy and postpartum
Supplemental material, sj-docx-1-hpq-10.1177_13591053261462432 for Weight stigma exposure, self-perceived weight and weight bias internalisation across preconception, pregnancy and postpartum by Michelle Dever, Briony Hill, Helen Skouteris and Angela C. Incollingo Rodriguez in Journal of Health Psychology
Footnotes
Ethical considerations
The study was approved by the Monash University Human Research Ethics Committee (Project ID: 38307) on 23 August 2023 and conducted in accordance with the Declaration of Helsinki.
Consent to participate
An explanatory statement containing participant and consent information was provided at the beginning of the survey. Consent was obtained when participants indicated their agreement and proceeded to the survey.
Consent for publication
Consent for publication is not applicable to this article as it does not contain any identifiable data.
Author contributions
MD: Methodology, formal analysis, Writing original draft, BH: writing – review & editing, supervision. HS: Writing – review & editing, supervision. ACIR: Conceptualisation, methodology, formal analysis, writing – review & editing, supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MD is funded by a Monash Graduate scholarship supported by an Australian Research Council (ARC) Discovery Project (DP220101107) and RTP scholarship. BH is funded by an Australian Research Council (ARC) Discovery Early Career Researcher Award (DE230100704).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data are available in the manuscript and Supplementary Materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.