
Abstract
The goal of this stud was to examine whether a technological touch activated Collaborative Puzzle Game (CPG) increased positive social behaviors in children with high functioning autism spectrum disorder (HFASD). The CPG involved construction of a virtual puzzle by selecting and dragging pieces into the solution area on a touch screen table. The target picture was presented on the top of the screen. Six dyads of children with HFASD (aged 8-11 years) engaged in the CPG in a Free Play (FP) mode in which partners could independently move puzzle pieces versus in an Enforced Collaboration (EC) mode in which partners could only move puzzle pieces together. Videos of the dames were coded for the frequencies of positive and negative social interaction, affect, play, and autistic behaviors. Parents completed the Social Responsiveness Scale (SRS).
Wilcoxon Signed-ranks tests indicated that children with HFASD showed significantly higher frequencies of positive social interaction and collaborative play in the EC versus FP modes but there were no differences in negative social behaviors. Differences in social behaviors between partners during the puzzle games were not significant; however there were differences within pair in the severity of social deficits as assessed by the SRS questionnaire.
The CPG in an EC mode was effective in promoting positive social interaction by requiring children to work together towards a mutual goal. However, the increased challenge in this mode, particularly for children with lower social-communication skills, suggests the need for establishing selection criteria and mediation steps for such interventions.
Keywords
Introduction
Interventions for children with autism spectrum disorders (ASD) focus on the promotion of social and communication skills, which pose a core difficulty for individuals with this disorder (American Psychiatric Association, 2000). Although cognitively and verbally capable, children with a high functioning autism spectrum disorder (HFASD) face great challenges in learning the codes and maneuvering the social world. It is important to develop intervention strategies that facilitate collaborative capabilities and prepare the child for negotiating and working with peers. This pilot study sought to investigate the potential benefit of a technological touch activated Collaborative Puzzle Game (CPG) in increasing positive social behaviors in children with HFASD.
Children with HFASD show social deficits throughout life. Some of the specific social deficits that these children experience are inappropriate eye contact; lack of social reciprocity, shared enjoyment, and interests; and difficulty interpreting verbal and nonverbal social cues (American Psychiatric Association, 2000; Weiss and Harris, 2001). Aside from differences in intellectual abilities, children with HFASD show more social interaction skills and an ability to respond and initiate social interactions compared with children with ASD and an intellectual disability (Bauminger et al., 2003). Nonetheless children with HFASD encounter problems initiating and maintaining an interaction with peers during social activities or games. Maintaining interactions, in particular, requires the performance of complex and cooperative prosocial behaviors, such as sharing, collaborating, and negotiating, that pose difficulty for these children (Bauminger et al., 2008b; Sigman et al., 1999; Stone and Caro-Martinez, 1990). They also tend to show more parallel play rather than social or coordinated play when interacting with their friends, compared with typically developing peers (Bauminger et al., 2008a). Consequently, children with HFASD are prone to lower peer acceptance, loneliness, bullying, and difficulty negotiating their choices in social settings (Asher et al., 1990; Bauminger, et al., 2003; Scheeren et al., 2012). In addition, intact IQ often entails greater self-awareness to social difficulties, potentially leading to reduced self-confidence and well-being. A review of studies of social interventions for children with HFASD and Asperger’s syndrome shows scarcity of evidence for the efficacy of interventions tailored to their particular needs (Rao et al., 2008).
There is a growing recognition for the value of using innovative technologies to promote social skills in individuals with ASD (Dautenhahn and Werry, 2004; Gal and Weiss, 2011; Grynszpan et al., 2005; Nikopoulos and Keenan, 2004). Several studies have documented the benefits of virtual reality, robotics, and multimodal interfaces for increasing vocabulary, emotional expression, and social problem solving (Bernard-Opitz et al., 2001; Bosseler and Massaro, 2003, SikLányi and Tilinger 2004; Parsons et al., 2006; Dautenhahn, 1999; Gal et al., 2005; 2009). Such interventions are particularly suitable for persons with ASD as they (a) provide a controlled and predictable setting for social interaction that minimizes distractions and sensory stimuli; (b) enable to grade the amount, type, and level of social demands; and (c) are highly motivating for many individuals with ASD (Murray, 1997).
In recent years, Shared Active Surface (SAS) have become available (Cappelletti et al., 2004). SAS are computer systems based on large interactive surfaces that can be placed horizontally (often known as tabletop devices). They can be operated by multiple people simultaneously, as the system interprets the gestures of more than one user as contributing to a single combined command. Therefore, SAS can be designed for collaborative interaction between two or more participants.
The DiamondTouch (DT) interface, which was used in this study, is a touch-sensitive SAS. It is capable not only of recognizing different users but can track who is touching where as well. Piper et al. (2006) used a four-player cooperative tabletop game to teach teamwork skills to children with Asperger’s Syndrome. Gal et al. (2009) tested a nine-session intervention with a Story Table collaborative interface and evaluated its effectiveness. They found that a multitouch tabletop intervention led to improvements in positive social skills for children with HFASD including a substantial increase in eye contact and sharing emotions as well as in demonstrating an interest toward the partner. A concomitant reduction of stereotypic and repetitive behaviors was observed while the children were interacting with the Story Table compared with the preintervention low-tech activities. Zancanaro et al. (2011a) developed the “Join-In Suite,” which is a three-user, touch-based application implemented via the DT. The application uses cognitive behavioral therapy (CBT) principles and is used to foster collaboration between pairs of children and to provide ways for a practitioner to control the pace and process of the interaction. In addition, they developed “NoProblem,” an application aimed at enhancing social communication skills for children with HFASD. Initial usability studies support the efficacy of these applications which embed collaboration in their structure in leveraging their engaging power (Weiss et al, 2011).
The application that was used in this study, the CPG, was designed to be completed by multiple players working at the same time on the DT table. The CPG is operated by players picking up, dragging, and releasing digital puzzle pieces on the screen. This application affords an interaction similar to other table play activities (Cappelleti et al., 2004). The CPG includes two modes: (a) Free Play (FP)—where the two players are free to move pieces independently, and (b) Enforced Collaboration (EC)—where the two players have to touch the digital piece together in order to drag and release it. This mode “forces” users to carry out joint actions while not allowing these actions to be completed by a single user. Using the CPG, two-user studies (Battocchi et al., 2009) with dyads of typically developing children and dyads of children with lower functioning autism attest to the high acceptability and usability of the different CPG modes. Findings from these studies show that in the EC mode, typically developing children negotiated their choices of puzzle pieces via verbal requests or by tapping a particular piece. Completion time was greater in the EC mode versus FP in both groups possibly due to the higher complexity and demand for collaboration. In both groups, the EC mode was associated with higher rates of simultaneous activity. It is unclear from these studies as to what specific changes occur in positive social and negative social behaviors between enforced and nonenforced modes of collaboration. In addition, the applicability of the CPG EC for children with HFASD and the role of within-dyad variability have not been investigated.
The described study sought to address the following research questions: (1) Does the EC relative to the FP mode elicit more positive social behaviors, less negative social behaviors, and less repetitive behaviors in children with HFASD? (2) Do differences in social skills within dyad change as a matter of the mode in which they play? (3) Does the severity of social impairments relate with social participation in the CPG? Our hypothesis was that operating the CPG in the EC mode will affect the extent of collaboration between participants relative to when they play in the FP mode.
Methods
Participants
The study included a sample of 12 boys with HFASD ages 8–11 years (M = 9.28, standard deviation (SD) = 0.94) from 2nd (n = 4), 3rd (n = 6), and 5th (n = 2) grades in a special classroom within a public school. Inclusion criteria were (a) meeting the criteria for autistic disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR; American Psychiatric Association, 2000), meeting criteria for ASD on the Autism Diagnostic Observation Schedule (ADOS: Lord et al., 2000), and receiving a diagnosis from a certified professional (i.e. developmental neurologist, psychiatrist, or clinical psychologist); (b) having a current nonverbal IQ of 80 or above to confirm that cognitive functioning was within the normative range. This was determined based on the Wechsler Intelligence Scale for Children–Revised (WISC-R) performance scale (Wechsler, 1974); and (c) being between the ages of 8 and 12 years. None of the children suffered from medical conditions (e.g. seizures, Fragile X syndrome) and had no uncorrected visual or hearing impairments. Five of the children were taking methylphenidate medication. The sample comprised of six Russian immigrant families; however, all participating children were born in Israel. Pairing of children was determined by their chronological age, communication and academic level of functioning, and previous successful partnerships based on the recommendation of the education and clinical team. The education and clinical teams at the school were asked to recommend pairs of children who could work together for the purpose of testing a collaborative intervention but were unaware of the nature of the experiment. Children who did not get along with each other were not paired. As the sessions took place during school hours, the child’s academic schedule also played a factor in pairing.
Measures
Independent measures
DT table
The CPG runs on a DT, a multiuser, touch-and-gesture-activated screen originally developed by the Mitsubishi Electric Research Laboratories (Dietz and Leigh, 2001) and now managed by CircleTwelve (www.circletwelve.com). Images are top-projected onto its 32-inch-wide touch-sensitive horizontal surface through any commercial video projector. The DT can determine, through a capacitive coupling system, which part of the surface is being touched and by whom it is touched (for up to four users simultaneously). The system allows users to interact directly through finger touch. This interface runs on a FP or EC mode.
Graphically, the CPG includes a variable number of rectangular puzzle pieces (up to 16) that, at the beginning of the game, are randomly spread out over the table. A target picture of the completed puzzle is displayed at the top of the screen. A solution area is positioned in the center of the screen and marked by a darker rectangular border. The players can drag the puzzle pieces to a new position inside or outside the solution area. The program provides animation options such as a drum sound when pieces spread out, different sounds when pieces are picked up or released, and visual and auditory feedback for correct and incorrect position of pieces in the solution area.
For the purpose of this study, 18 puzzle pictures were selected based on pilot data with typically developing children and children with autism that rated the level of difficulty and attraction of the puzzle. Completion times were also measured to ensure that all final puzzles require similar lengths of time to complete.
Dependent measures
Friendship Observation Scale (FOS, Bauminger et al. 2005)
For the purpose of video coding the puzzle tasks, the Social Interaction scale of the FOS was adapted. The FOS is an interactional coding system designed to assess manifestations of friendship including behaviors, verbalizations, and affects.
The five categories from this scale that were used in this study for video coding included: the Positive Social Interaction (PSI), Negative Social Interaction (NSI), Affect, Play, and Autistic Behaviors. The PSI includes Goal-Directed Behaviors (e.g. offering a goal-oriented action), Sharing Behaviors (e.g. showing and directing attention), Prosocial Behavior (e.g. encouraging), Conversation (e.g. negotiation), and Nonverbal Interaction (e.g. eye contact). The NSI includes items such as Teasing and Aggression. For the purpose of this study, the Affect scale was divided into a Positive Affect and Negative Affect score. The Play scale includes Parallel Play, Simple Social Play, Collaborative Play, and Unoccupied Play. The Autistic Behaviors scale includes items such as Repetitive Stereotypical Motor and Verbal Behaviors.
The FOS was originally developed to measure qualities of friendship in children on the autism spectrum. Previous research showed a mean interrater agreement level on the seven main categories of the FOS Positive Social Interaction scale of 93% (range: 84%–100%) (Bauminger et al., 2008a).
Video coding
Using Corel VideoStudio 12 software, every 30-s interval within one puzzle game was coded for the frequency of each of the FOS items, and puzzle completion time was recorded. The frequency of each of the five FOS categories was summed across all puzzles within mode. Thus, a higher score in a particular category indicated a higher quantity of behaviors in that category. The observer was trained to code the FOS items and achieved agreement levels of 80% and above across FOS items with the third author.
Social Responsiveness Scale (SRS: Constantino and Gruber, 2005)
This parent questionnaire consists of 65 items that assess the severity of social impairments as well as repetitive behaviors. The measure yields five scores: Total, Social Cognition, Social Awareness, Social Communication, Social Motivation, and Autistic Mannerisms, all of which can be converted into T-scores. SRS T-scores between 60 and 75 indicate a level of autistic social impairment that is “mild to moderate,” whereas scores above 75 indicate a “severe” level. The SRS has been extensively studied with evidence for high levels of internal reliability, α = 0.97; test–retest reliability, α = 0.85; and interrater reliability coefficients ranging from 0.75 to 0.91 across the different pairs of raters. In addition, receiver operating characteristic (ROC) analyses demonstrated the high sensitivity and specificity rates of the SRS in predicting an ASD diagnosis (Constantino and Gruber 2005). The structure validity of the SRS was also supported by several studies (Constantino et al., 2003, 2004). Since our sample was Hebrew speaking, the SRS was translated into Hebrew with the permission of the authors using a back-translation method.
Procedures
Children were recruited through a public school. Parents signed consent forms prior to their child’s participation in the study. Initial screening for eligibility was carried out looking at information from the child’s educational records from the past 3 years including their WISC-R scores administered by the psychological services. As part of this study, the ADOS Module 3 was administered to confirm diagnosis. Parents completed the SRS and a demographic questionnaire. The puzzle tasks were carried out in a quiet room within the school in the presence of an adult who is familiar to the child. Prior to the experimental session, an individual training session took place and had the twofold function of familiarizing the children with the interaction mode of the CPG and of ensuring that the game was suitable in difficulty level for the child. During the training phase, the experimenter demonstrated to the child how to interact with the digital objects displayed on the CPG until the child understood the touch, drag, and drop functions. The experimenter facilitated performance as needed during the training phase. For all children, the training started with a medium-sized picture divided into four pieces; if this level of difficulty was easily completed, subsequent puzzles had more pieces. Each child played three puzzles in the FP mode and three in the EC mode. One child was excluded from the sample at the training stage since he could not understand how to play the game. After training, the children took a 10-min break and then returned for the experimental phase.
Each dyad participated in two sessions that were a month apart. In each session, the children completed three puzzles in the FP mode and three in the EC mode. The three puzzles within mode for each session were randomly ordered; however, the same order was presented to all dyads. This led to a total of six puzzles per mode. At the beginning of the FP mode, the examiner explained to the children that they would have to work together to complete the puzzle and emphasized that the important thing was to “have fun playing together and helping each other.” During both modes, the experimenter only provided technical support related to the activation of the game (e.g. moving children further apart in case their seat mats were touching, because in such a case, the system could not identify each user separately).
Data analysis
There were categories/items on the FOS that had a very low frequency, and thus were not meaningful to compare within dyad and between modes. These included the Autistic Behaviors category for which most children (83.3%) had a “0” frequency, the Negative Affect score for which 83.3% of the children had a “0” frequency in the FP mode and 58.3% in the EC mode, and Parallel Play that was not observed for most children in the FP (83.3%) and EC (100%) modes.
Nonparametric tests were conducted as most dependent variables were not normally distributed. Significant levels for the Shapiro–Wilk’s test were as follows: PSI (p = 0.007), NSI (p = 0.25), Positive Affect (p = 0.06), Simple Social Play (p = 0.83), Collaborative Play (p = 0.05), and Unoccupied Play (p < 0.001). Although NSI and Simple Social Play were normally distributed due to the small sample size, a nonparametric approach was adopted throughout the study.
Initial analyses were conducted to examine whether frequencies across the two evaluation sessions could be summarized with one score. Clinically, the second evaluation may differ in scores from the first due to a potential decrease in novelty and challenge. Wilcoxon signed-rank tests demonstrated that there were no significant differences (p > 0.17) in PSI, NSI, Positive Affect, Simple Social Play, and Collaborative Play scores within each mode (i.e. EC, FP) between the first and second evaluations. Thus, frequency scores were summarized across the two evaluation sessions for each mode. Unoccupied Play was significantly more frequent in the second evaluation relative to the first within the EC mode, Z = −2.68 (p = 0.01). Given that all other comparisons were not significantly different between evaluations, frequencies across evaluations were aggregated for all scores.
Dyadic observations of social interaction must take into account the nonindependent nature of such data. In small samples, independence cannot be tested statistically and thus are assumed to be nonindependent by default (Kenny et al., 2006). Therefore, we first wanted to examine differences in frequency of FOS behaviors between partners within a dyad using Wilcoxon signed-rank tests. There were no significant differences between partners on the PSI, NSI, Positive Affect, and Play scores (p > 0.18).
Results
Completion times for each of the 12 puzzles were calculated for each dyad. There were puzzles that were not completed or not performed at all due to behavior problems that emerged and interfered with puzzle completion. The first dyad did not complete one out of the six EC puzzles. The second dyad did not do five out of the EC puzzles, did not complete the sixth EC puzzle, and did not complete one FP puzzle. The fifth dyad did not do one EC puzzle and did not complete three EC puzzles. Therefore, FOS frequency summary scores reported in this study are based on different durations of puzzle play which reflect the ability of the children to cope with the task demands. Although there were no significant differences in completion times between modes (Z = −0.11, p = 0.92), mean completion time for the FP mode was 2.56 min (1.22–7.65), while it was 3.76 min (0–10.33) in the EC mode.
Differences between FP and EC modes
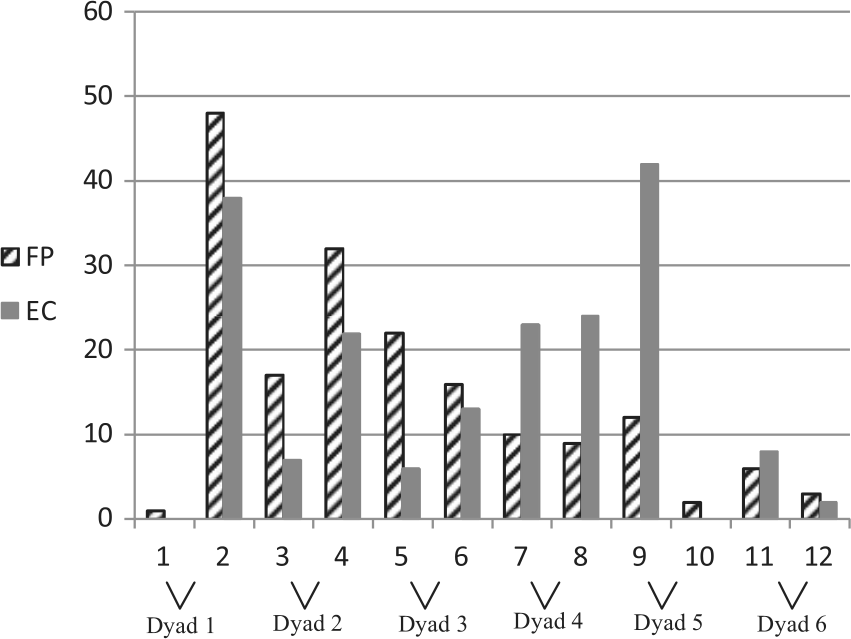
Our primary research question related to the behavioral differences between modes. Wilcoxon signed-rank tests indicated that there was a significant difference between the EC versus the FP mode in the PSI (Mdn = 45.5, Mdn = 38.0, respectively; Z = −2.28, p = 0.02, r = –.66). As can be seen in Figure 1 and Table 1, the partners of dyad 2 were the only ones who did not show higher frequencies of PSI in the EC mode. Partners in dyad 3 showed the greatest difference between modes; however, note that they also started off high in the FP mode. Investigation of the PSI categories that contributed to the difference between modes showed that there were marginally higher scores in the EC versus FP mode for most categories: Goal Directed Behaviors (Mdn = 38.0, Mdn = 29.5 respectively; Z = −1.88, p = .06, r = −.54), Sharing (Mdn = 2.0, Mdn = 1.0 respectively; Z = −1,71, p = .09, r = −.49), Pro-social behavior (Mdn = 2.0, Mdn = 0.50 respectively; Z = −1.73, p = .08, r = −.50), and Conversation (Mdn = 4.0, Mdn = 2.50 respectively; Z = −1.85, p = .06, r = −.53). There were also significantly more children who had lower frequencies of Positive Affect in the EC versus FP mode (Mdn = 5.0, Mdn = 7.50 respectively; Z = −2.10, p = .04, r = −.61, see Table 1).

Comparison of PSI frequencies between modes.
Wilcoxon Ranks Tests Comparing Behaviors between Modes.

Note. For all individual PSI items the EC>FP group was the greatest.
p<.05.
Wilcoxon Signed-ranks tests comparing scores on Play items between modes, showed that there were significantly higher rank scores in the EC versus FP mode for Collaborative Play (Mdn = 10, Mdn = 0 respectively; Z = −2.25, p = .02, r = −.65) but also higher rates of Unoccupied Play (Mdn = 2.5, Mdn = 0 respectively; Z = −2.53, p = .01, r = −.73, see Table 1).
There was no significant difference between modes in NSI (Z = −0.35, p = 0.72). Figure 2 and Table 1 show that for NSI, there was no consistent pattern of scores between modes with some children who showed clearly less NSI in the EC mode (n = 5), while for others, more NSI was presented in the EC mode (n = 4). There were three more children with very low (0–3) NSI scores in both conditions (Wilcoxon classified them as having more NSI in the FP relative to EC mode).
Comparison of NSI frequencies between modes.
Tests were repeated excluding the second and fifth dyads with incomplete puzzle and generated similar findings.
Comparison of differences within dyads by mode
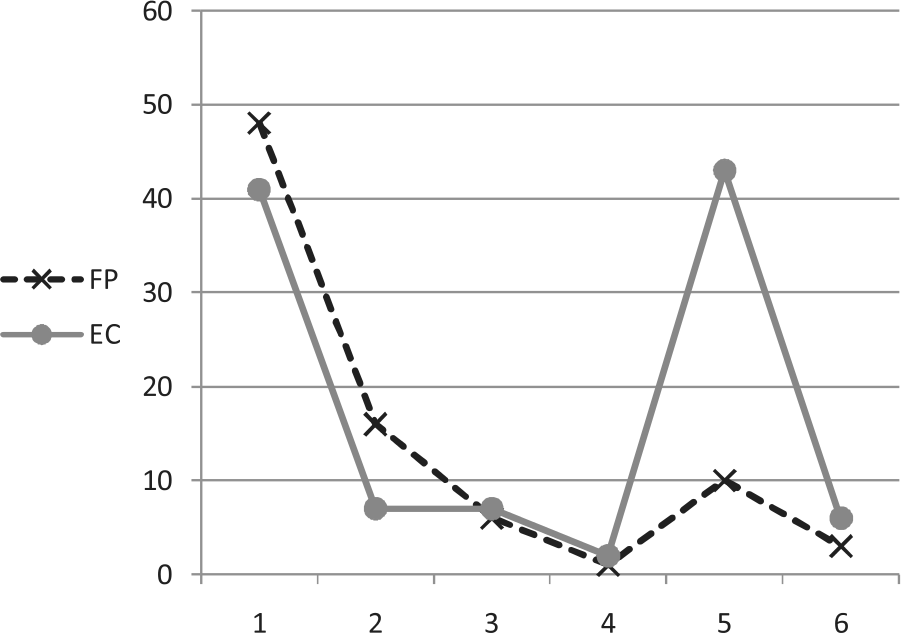
We examined whether the difference between partners of a dyad changed between modes to indicate whether the observed differences between modes were accounted for by differences within a dyad. This analysis also aimed to investigate whether the CPG mode influenced dyadic behavior. For this purpose, we created an absolute difference score by subtracting partner 2’s score from that of partner 1’s for each dependent variable within mode (see Figures 3 and 4). Wilcoxon signed-rank tests showed that there were no significant differences between modes for the dyad difference scores in PSI, NSI, Positive Affect, and Play (p > 0.05), indicating that the differences between dyads were not a result of differences between modes.

Dyad absolute difference in PSI between partners by mode.
Dyad absolute difference in NSI between partners by mode.
Association with social deficits
To examine the degree to which the severity of social deficits as reported by parents on the SRS are associated with the child’s gain from the CPG, a Spearman’s Rho correlation was conducted between the SRS domain t-scores and PSI and NSI scores within each mode. The PSI score in the EC mode had a significant correlation with the SRS Social Awareness (r = −0.59, p = 0.04) and marginally significant with the Social Communication scores (r = −0.53, p = 0.08). In other words, greater severity of deficits in these areas was associated with lower frequencies of PSI, particularly in the EC mode. No significant correlations were identified for PSI in the FP mode and none for NSI. Follow-up analyses using Wilcoxon signed-rank tests showed that there were significant differences between dyad partners in SRS Expressive Communication t-scores (Mdnp1 = 59, Mdnp2 = 49, respectively; Z = −2.02, p = 0.04) and marginally significant differences in SRS Social Awareness t-scores (Mdnp1 = 61, Mdnp2 = 48, respectively; Z = −1.83, p = 0.07). Therefore, although all children met criteria for HFASD, there were differences within dyad in the baseline severity of social deficits.
Discussion
This study provides evidence for the advantages and disadvantages of using an EC interface with dyads of children with HFASD. As a group, children with HFASD showed significantly higher frequencies of positive social behaviors and collaborative play and lower rates of positive affect in the EC versus FP mode. This was achieved while playing in a familiar setting (i.e. school, educator/therapist, and classmate) using a familiar task on a table surface with the built-in constraints to work collaboratively. Although there was great variability in the engagement of individual children in the CPG, differences between modes were not explained by statistical differences within dyad. Children with lower severity of social communication impairments based on the SRS presented higher frequencies of positive social behaviors in the EC mode.
Increases in positive social behaviors of children with HFASD in the EC versus FP CPG mode were specifically notable in goal-related, sharing, prosocial, and conversational behaviors, with goal-related behaviors being the most commonly observed type of positive social behavior. However, there were no differences in nonverbal positive interaction (i.e. eye contact) between modes. This is in contrast to findings of children with HFASD showing higher rates of eye contact in the Collaborative Story Table interface relative to collaborative low-tech activities (Gal et al., 2009). Discrepancies in findings may relate to the puzzle task affording more intense visual skills on account of looking at the partner.
One can parallel the rationale for applying the CPG in the EC mode to that of Constraint-Induced Movement Therapy (CIMT), a controversial intervention implemented with adults following stroke or children with neuromuscular disorders. In this intervention, the unaffected limb is immobilized physically for a certain timeframe, while intensive training of the affected limb takes place, with various studies supporting its efficacy (Charles and Gordon, 2005). Similarly, the underlying hypothesis of EC is that by creating circumstances that inevitably demand collaboration in order to complete a desired goal, the child’s brain will be required to generate and practice social skills. Support for the need for enforcing collaboration derives from evidence showing that when left free to play, pairs of children with ASD engage in parallel rather than collaborative play while this was not the case for typically developing children (Bauminger et al., 2008a). Results from the current study highlight the positive behavioral effects of “forcing” children with HFASD to collaborate. In practice, such a strategy when incorporated as part of an intervention can provide a supportive framework for practicing a weak area.
Nonetheless, the idea of “forcing” clients to practice skills can lead to negative outcomes. The lack of a significant consistent decrease in NSI (e.g. controlling, aggression, teasing) in the EC versus FP mode may reflect the price of the EC mode for some children. This contrasts previous research that shows a decrease in NSI in children with ASD during play with the Collaborative Story Table (Gal et al., 2009). There were individual children in our sample for whom NSI increased in the EC mode. Interestingly, their increase in NSI did not necessarily correspond with a decrease in PSI in the EC mode. For example, both partners of the fourth dyad showed a large increase in PSI in the EC mode but also more NSI in the EC mode. The second, seventh, and ninth participants who showed the highest frequency of NSI were also highly verbal and dominant children. It is also possible that while trying to negotiate and foster goal-directed social behaviors, some children express a greater need for control over their partner. For other children, the EC mode may have increased their frustration and antagonism (e.g. domineering partner leading to the other partner’s avoidance), variables that should be quantified in future research.
Similar to the NSI, the lower rank of positive affect in the EC mode did not correspond with higher negative affect in the EC mode as negative affect was rarely displayed across modes. Lower positive affect may relate to the elevated stress and lack of freedom to choose whether to collaborate or not in the EC mode. Aside from corresponding to the challenges of the EC demand, lower positive affect may reflect difficulties of individuals with ASD in cross-modal integration of social behaviors such as facial expression and speech (Dawson et al., 1990).
Surprisingly, completion times were not significantly different between modes, inconsistent with previous studies using this interface with dyads of typically developing children and dyads of older children with low functioning autism (Battocchi et al., 2009). However, our study is the first to compare EC and FP modes using a within-subject design. Nevertheless, the mean completion time was close to 1½-min longer in the EC versus FP mode and may not have reached significance due to the small sample size. Clinically, completion times reflected the emergence of more problem behaviors for some children, while for other children, longer durations reflected the negotiation and interaction that was going on in the EC mode. Thus, shorter durations do not necessarily correspond with fewer difficulties in the EC mode, and thus cannot serve as outcome measures for such an intervention. In order to define for whom this interface is appropriate in increasing positive social behaviors, there is a need for understanding individual partner’s features. There was great variability in the performance and engagement in the puzzle game between dyads as apparent in the differences in the number of puzzles completed and in the individual patterns of differences between modes (see Figures 1 and 2). Some of the features that emerged as influential of the dyad’s gain from the EC mode were the child’s age/developmental level and social interaction style. With respect to age, the second dyad, comprising children who were the youngest in sample, and consequently, also the lowest developmentally (within study criteria), appeared to benefit the least from the EC mode as they were not able to complete several puzzles, and showed more positive social behaviors and play in the FP mode. In contrast, the third dyad, comprising the oldest, achieved the most from the EC mode. In terms of social interaction style, SRS findings suggest that children with greater difficulties in social awareness (e.g. knows when he is too close to someone) and expressive communication (e.g. has difficulty talking around a topic) benefit less from the EC mode. This can be explained by the built-in demand of this mode to notice the other partner’s social cues in order to act together or negotiate an alternative. The partners in the second and fifth dyads with the greatest number of incomplete puzzles were also those with lower rates of goal-directed behaviors and positive affect in the EC versus FP mode. In addition, anecdotally, when one partner had a passive interaction style and the other was dominant (such as in the first and fifth dyads), the FP mode enabled the passive partner to avoid acting, while in the EC mode active involvement was required. In turn, this led to increased tension and frustration of the dominant/controlling partner who could no longer act independently. These two extreme patterns of social interaction (i.e. passive versus active) have been applied to subclassify children with ASD (Wing and Gould, 1979), both of which challenge peer play (Wolfberg, 2004). The FOS NSI items of control and aggression toward others did not capture these dynamics nor did they differentiate the dyads with fewer completed puzzles. While not directly measured, anecdotally, it appeared that for some children, problem behaviors were exacerbated by the demand to collaborate. Evaluating passive and off-task behaviors may provide insight into the factors that account for engagement in this intervention. Although the differences in FOS social behaviors within dyad partners were not significant, the figures show large gaps in frequencies within some of the dyads supporting the above discussion of the role of partner’s features. The relative stability between modes may have reflected the fact that whoever started high/low relative to the other partner maintained that gap irrespective of mode. Further investigation of matching partners based on their social skills and interaction style for maximizing the gain from such an interface is warranted. Applying a three-user co-located interface allows a facilitator to intervene in the dyadic interaction in a manner that reduces negative social behaviors and moderates the role of a passive partner (Zancanaro et al., 2011b). Another strategy which can increase the efficacy of such an intervention is to conduct EC training sessions in which the examiner role models a potential partner.
In conclusion, on one hand, the EC led to more interaction and negotiation, while on the other hand, the increased challenge in the EC versus FP mode was evident in its higher number of uncompleted trials, lower positive affect, and for individual children a pattern of more negative social behaviors and/or less positive behaviors. There were children for whom the level of challenge in the EC mode was overwhelming and did not enable them to intuitively gain from this interface. It is possible that applying this mode over time coupled with direct facilitation of social strategies could lead to higher rates of benefit.
Limitations
The small sample size in this study requires replication of the experimental design with more dyads to provide a better understanding of the selection criteria suitable for this intervention strategy eventually leading to the “just-right challenge.” This sample size may also explain the marginal level of significance in some of the FOS comparisons. In addition, the FOS was not sensitive in capturing autistic behaviors as noted by their very low frequency in this study. These behaviors may have also been more subtle due to the short activity-based context examined relative to previous findings of fewer repetitive behaviors when children with HFASD engaged in the Collaborative Story Table (Gal et al., 2009).
Future research is important for testing the carryover of gains in positive social behaviors to other life settings. The difficulties in social dynamics within some of the dyads call for testing the advantage of working in mixed dyads (i.e. with a typically developing partner) as shown by Bauminger et al. (2008a). At the same time, unmixed dyads have the advantage of facilitating nonhierarchical dynamics. Follow-up analyses indicated differences in SRS t-scores within dyad, a gap which may have influenced their participation. There is a need to gain a better understanding of the ideal dyad match for promoting social interaction in children with HFASD considering age, temperament, social capacities of both partners, on-task behaviors, and overall level of functioning.
Conclusion
EC interfaces show a great potential in guiding children with HFASD to interact with one another to complete a mutual goal. The structured task provides a self-explanatory paradigm in which children can physically and mentally practice negotiation, collaboration, and teamwork. Negative social behaviors were not influenced by mode. At the same time, like in many interventions such as the CIMT, this intervention does not fit all, with some children showing an opposite effect of elevated frustration and off-task behaviors when “forced” by technology to collaborate. Features that may play a role in a child with HFASD’s benefit from the EC mode are being older and stronger in expressive communication and social awareness, as well as playing with a peer who shares a similar level of severity of social deficits. Further research is needed to determine for whom this strategy is efficacious and under what type of human and technology facilitation. Implementing innovative collaborative platforms for promoting social skills in children with HFASD is an important step in providing the means for repeated practice of an area of weakness within a motivating, structured, and predictable context.
Footnotes
Acknowledgements
We thank the Mitsubishi Electric Research laboratory for their donation of the equipment used in this research.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The first author’s work was supported by a European International Reintegration Grant (# 203715).