
Abstract
Despite the well-documented success of cognitive restructuring techniques in the treatment of anxiety disorders, there is still little clarity on which cognitions underpin fear and anxiety in children with high-functioning autism spectrum disorder. This study examined whether certain cognitive appraisals, known to be associated with fear and anxiety in typically developing groups, may help explain these emotions in children with high-functioning autism spectrum disorder. It also investigated relations between these cognitive appraisals and theory of mind. Appraisals, fear and anxiety were assessed using a vignette approach in 22 children with high-functioning autism spectrum disorders and 22 typically developing children. The two groups differed significantly on all four appraisal types. Anxiety was negatively correlated with future expectancy and positively with problem-focused coping potential in the high-functioning autism spectrum disorder group but was not correlated with appraisals in the typically developing group. The two appraisals associated with fear were emotion-focused coping potential (in the high-functioning autism spectrum disorder group only) and self-accountability (in the typically developing group only). Linear regression analysis found that appraisals of emotion-focused coping potential, problem-focused coping potential and future expectancy were significant predictors of theory-of-mind ability in the high-functioning autism spectrum disorders group. These findings indicate that specific, problematic patterns of appraisal may characterise children with high-functioning autism spectrum disorders.
Unusual fears (Rapp et al., 2005; Witwer and Lecavalier, 2010) and exaggerated symptoms of anxiety are common across autism spectrum disorders (Gillott et al., 2001; Kim et al., 2000; Mazefsky et al., 2010) and are particularly marked in children with high-functioning autism spectrum disorder (HFASD) (Farrugia and Hudson, 2006). Fear in the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) (American Psychiatric Association (APA), 1994) is defined as the perception or anticipation of threat in the environment that is characterised by increased heart rate, tensed muscles and fight or flight reactions. Failure to resolve a fear despite attempts to do so on the part of an individual is thought to lead to the formation of anxiety disorders (Klein, 2009). Anxiety is classified as a clinical disorder and differs from fear in the degree of severity, frequency, persistence of symptoms and associated difficulties such as depression (Turner et al., 1992). Anxiety disorders are thought to occur in 2%–15% of the general population (APA, 1994), but estimates of the prevalence of anxiety problems in children with autism suggest that they are 49% greater than in the general population (Bellini, 2004).
DSM-IV (APA, 1994) identifies anxiety-like symptoms as commonly associated with autism, and empirical studies have shown a higher occurrence of anxiety in children with autism when compared to control groups of typically developing (TD) children (e.g. Evans et al., 2005; Kuusikko et al., 2008; Weisbrot et al., 2005). Autism and social anxiety may also overlap (Melfsen et al., 2006; Russell and Sofronoff, 2005). For example, symptoms of autism were found to co-occur in 45 children and adults who had a diagnosis of anxiety disorder (Towbin et al., 2005). Similarly, Sukhodolsky et al. (2008) report that in a sample of children diagnosed with autism (n = 151), Asperger’s syndrome (AS) (n = 6) or pervasive developmental disorders (n = 14), 43% also met the criteria for a DSM-IV diagnosis of social anxiety disorder.
Research aiming to clarify the aetiology, maintenance and treatment of anxiety disorders indicates that cognition may be a key internal process (Alfano et al., 2008; Miers et al., 2011; Rapee and Heimberg, 1997; Schultz and Heimberg, 2008). The current study therefore sought to address the extent to which specific stress-related cognitions are associated with anxiety among HFASD and TD populations.
Role of cognition in anxiety
The underlying principle of cognitive theories is that inaccurate or skewed interpretations of events lead to fear and anxiety in harmless situations (Clark and Beck, 1999; Clark and Wells, 1995). Specifically, a child’s belief about the nature of fear objects, their own ability to deal with them, their perceived responsibility and the anticipated outcomes all predict the development and maintenance of fears and symptoms of anxiety. These difficulties are referred to as cognitive errors (Beck and Emery, 1985), interpretation biases (Heinrichs and Hofmann, 2001) or impairment in cognitive appraisals (Lazarus and Folkman, 1987).
One influential model, proposed by Smith and Lazarus (1993), illustrates how the cognitive evaluation of a social situation determines emotional reactions. The authors elaborated on appraisal dimensions underpinning individual negative emotions, proposing that specific, unique appraisal dimensions are responsible for any emotional reaction. The model included four distinct appraisal dimensions: self-accountability, emotion-focused coping potential, problem-focused coping potential and future expectancy. Each situation is evaluated against each of these appraisal dimensions, and these then determine a person’s emotional reaction. Smith and Lazarus proposed that evaluation along appraisal dimensions is contingent upon one’s goals, abilities and motives. Thus, the same situation will be appraised differently by different individuals. Furthermore, Smith and Lazarus proposed that people engage in an assessment of their ability to change or influence incongruent situations and their ability to deal with them emotionally: These ‘secondary appraisal dimensions’ are problem-focused coping potential and emotion-focused coping potential, respectively. Emotion-focused coping potential underlies the emotional reaction of fear: for example, feeling uncertain about one’s own emotional reaction to a future situation, such as receiving poor examination results. An appraisal of low problem-focused coping potential may mean a person feels unable to formulate a proactive response when awarded low scores in an examination. Finally, future expectancy reflects how certain a person is about whether an outcome will be favourable or unfavourable. Evaluating whether examination results will lead to negative future outcomes is an example of appraisal of future expectancy. In the case of sadness, both future expectancy and problem-focused coping potential can account for variation. The self-accountability dimension involves an assessment of how much responsibility an individual takes for a confronting situation. It characterises guilt.
However, not all empirical work has supported such a proposition. Nezlek et al. (2008) found that more than one appraisal was associated with negative emotions in a TD group of adults. Similarly, children with anxiety disorders appear to have appraisal biases that can be grouped into two broad categories: (1) overestimating the nature of threat and (2) underestimating one’s own ability to deal with it (Beck et al., 1985; Pilecki and McKay, 2011; Wright and Borden, 1991). Examples of the overestimation of threat include overgeneralisation (believing that a negative outcome will repeat itself in all future situations), catastrophising (holding very negative expectancies about the probable outcome of a situation) and personalising (holding oneself responsible for negative outcomes) (Creswell et al., 2006). More than one cognition could thus be associated with anxiety disorders. Indeed, studies of children with anxiety disorders have highlighted an association between anxiety difficulties and several cognitions including low future anticipation, high self-responsibility and high uncertainty about ways of dealing with the negative consequences of a social situation (Bögels and Zigterman, 2000; Creswell et al., 2011).
Different cognitions may underpin different forms of anxiety disorder. For example, cognitive theories of obsessive–compulsive disorder in children and adults have emphasised the importance of cognitions of inflated responsibility (Salkovskis, 1985, 1989), which is defined as holding oneself responsible for all negative events in a generalised fashion. Notably, inflated responsibility may be considered conceptually similar to the appraisal dimension of self-accountability again emphasising the link between appraisal dimensions and anxiety. Among a different group of anxiety sufferers, adolescents with social anxiety disorder, there is a significant association between cognitions related to likelihood and the cost of negative social and non-social events (Rheingold et al., 2003). ‘Likelihood’ here refers to expectancies about future and ‘cost’ meant personal relevance and coping potential to deal with the negative situation. The cognition of likelihood may be viewed as comparable to the appraisal dimension of future expectancy and cost to appraisals of motivational relevance and coping potential. Finally, people with specific phobias and those with generalised anxiety disorder present with high levels of future expectancies (Muris et al., 2007; Thorpe and Salkovskis, 1995; Tomarken et al., 1989; Wells, 2005), overestimating the occurrence of negative outcomes in fearful as well as non-fearful situations. Thus, across different anxiety disorders, the cognitive aetiology may differ.
These findings lead us to speculate that children with HFASD may exhibit specific cognitive errors since they too experience high levels of anxiety. Indeed, cognitive therapy intervention programmes for reducing the occurrence of fears and anxiety in children with autism (especially those with IQ > 70, that is, HFASD) already address maladaptive cognitions related to responsibility, relevance and belief in their ability to deal with negative social situations (Lang et al., 2010). Interventions based on these principles successfully reduce levels of anxiety among children with autism (e.g. Chalfant et al., 2007; Greig and Mckay, 2005; Wood et al., 2009). However, the focus of these studies has generally been on bringing about change rather than exploring the broader conceptual issues regarding which specific cognitions might contribute most to the raised levels of anxiety and fear in this population. This issue is the focus of the present study, which investigates the set of cognitions known as appraisals.
Ambiguity
Interpretation biases have been observed in ambiguous situations (e.g. Barrett and Healy, 2003; Daleiden and Vasey, 1997; Hadwin et al., 2006; Micco and Ehrenreich, 2008). Barrett et al. (1996) presented ambiguous situations representing some sort of physical or social threat to groups of children with anxiety disorders and then compared their responses to both control and non-anxious clinical groups. Anxious and non-anxious clinical groups interpreted ambiguous events as more threatening than the control group. In a similar study by Bögels and Zigterman (2000), children with anxiety disorders were exposed to ambiguous threatening situations, and more negative cognitions were reported by the anxious group compared to the control group. This finding in hypothetical ambiguous social situations has been widely replicated, and a statistically significant association has been shown between trait anxiety and threat interpretations (Chorpita et al., 1996; Creswell and O’Connor, 2010; Hadwin et al., 1997; Muris et al., 2000, 2003). It may be that when clear, relevant information in a situation is lacking, children instead have to rely on personality dispositions and past experiences when making judgements or inferring meaning (Crick and Dodge, 1994; Lazarus and Folkman, 1984). These judgements are likely to involve negative self-appraisals since these are more likely to be generated by individuals who experience a high degree of anxiety in socially ambiguous situations (Huppert et al., 2007). In this way, perceived situational ambiguity can influence social cognitive interpretation process (Constans et al., 1999).
Theory-of-mind ability
For children with autism, social situations might appear ambiguous because of a theory-of-mind (TOM) deficit (Baron-Cohen et al., 1997). TOM deficits imply a state of uncertainty with regard to other person’s thoughts in a social situation (Frith and Happè, 1994), which is likely to reduce clarity and increase ambiguity. It is proposed that a TOM deficit is a contributing factor for anxiety and social difficulties in children with autism spectrum disorders (Blackshaw et al., 2001; Brent et al., 2004). It may therefore be the case that TOM deficits in children with autism are an important factor when considering appraisals relating to social situations. To our knowledge, only Farrugia and Hudson (2006) have investigated cognitions in relation to anxiety in children with HFASD. They recruited 29 adolescents with AS, 30 with anxiety disorder and 30 TD controls and found higher scores for anxiety and negative thoughts in the AS group than the anxiety-disordered and TD groups. Significant associations were also found between anxiety symptoms and negative cognitions such as ‘I will never overcome my problems’, ‘Something awful is going to happen’ and ‘There is something very wrong with me’. So, children’s beliefs about the nature of fear objects, their perception of their ability to deal with them, their level of perceived responsibility and their anticipated outcomes appear to be associated with symptoms of anxiety.
Despite widespread evidence of the success of cognitive restructuring techniques in the treatment of anxieties and fears in children with autism (Reaven et al., 2009; White et al., 2010), surprisingly little systematic work has been undertaken to study which specific cognitions might contribute to anxiety in this group. There is however a strong rationale for predicting that anxieties and fears in children and young people with HFASD are underpinned by specific cognitions.
The specific hypotheses and objectives of the current study are as follows:
Replication of previous findings
1. The HFASD group will have significantly higher scores for fear and anxiety compared to TD group.
2. The HFASD group will have significantly lower scores for TOM ability than TD group.
Novel hypotheses
3. The HFASD group will have significantly higher scores for the appraisal dimension of self-accountability and significantly lower scores for problem-focused coping potential, emotion-focused coping potential and future expectancy than the TD group.
4. The four appraisal dimensions will be significantly associated with fear and anxiety in both the HFASD and TD groups.
Exploratory research question
Are the four appraisals dimensions significantly associated with each other?
Is TOM ability significantly associated with all four appraisal dimensions in the HFASD and TD groups?
Method
Participants and selection procedure
Sources of recruitment were the National Autistic Society (NAS), Scottish schools with special units and voluntary parent support groups in England and Scotland. Ethical approval was obtained from the University Ethics Committee, NAS ethics and local Education councils in which participating schools were located. Inclusion criteria were that children in both groups should be aged 8–12 years. Children in the HFASD group had to already have a diagnosis of high-functioning autism or AS (as reported by parents) and children in the TD group had to attend a mainstream school and have no diagnosis of developmental delay (as reported by parents). Data were collected from community samples of children: 22 in the HFASD group (18 boys and 4 girls) and 22 in the TD group (15 boys and 7 girls). Parents and children were informed that they would be asked to ‘give a description of a past emotional experience’ and ‘imagine being in a story about a frustrating situation and answer some questions about any feelings of anxiety’. Study objectives and procedures were explained to parents and children, and all were advised that their participation was voluntary, that they could withdraw at any time of the study and that information obtained from them would be treated in confidence.
Measures
Appraisals and fear
Scenarios which children would perceive to be frustrating were developed by asking 12 TD children and 14 children with HFASD to recount an experience from the preceding 2 weeks where they felt frustrated (based on Losh and Capps, 2003). The word ‘frustrated’ was explained to ensure that there was uniformity in children’s understanding of this term. Thematic analysis (Braun and Clarke, 2006) was used to identify which situations were frustrating to children in both the HFASD and TD groups. Four common themes were extracted: argument with siblings, bullying in school, rejection from peers and emphasis by teachers on over-compliant behaviour. Four scenarios were written based on these themes, each of which described a frustrating situation. An inter-rater reliability check was carried out on these hypothetical frustrating situations for how well they illustrated a frustrating story on a 0–3 scale. Out of 10 non-psychologist raters, eight gave a score of 3 for each story and two gave a score of 2. These four scenarios were thus considered reliable and randomly distributed across participants, resulting in only one scenario administered to each participant.
For each of the four scenarios, children were asked to imagine that they were in the described situation and to write a few sentences describing their reactions. Next, they completed an appraisal questionnaire to measure perceived self-accountability, problem-focused coping potential, emotion-focused coping potential and future expectancy relating to the vignette. Finally, participants completed a fear questionnaire to assess the extent to which they would feel fearful if they were in the vignette situation. The appraisal and fear questionnaires were adapted from Smith and Lazarus (1993), with language altered to be more age appropriate. Children were also asked to rate the extent to which each of three emotional adjectives for fear (‘frightened’, ‘scared’ and ‘afraid’) characterised their perceived emotional state. Each questionnaire used a 0–11 rating scale, and all questionnaires were completed four times (once for each scenario). The questionnaires were presented in the same order to all the participants in both the HFASD and TD groups: appraisal questionnaire being the first and fear questionnaire the second.
TOM
To measure TOM ability in children, Happé’s (1994) Strange Stories was used. This consisted of 24 short vignettes with questions. One question checked comprehension, and a second question asked for justification of the character’s actions (two justification questions in some vignettes). The stories were presented in the same order to all participants. Children were asked to imagine being the central character in the story and then to answer the questions. Good internal reliability scores of between .80 and .86 in both the HFASD and TD groups were found.
Anxiety
The Spence Children’s Anxiety Scale (SCAS: Spence, 1998) is a 45-item self-report questionnaire that assesses overall anxiety as well as six sub-types of anxiety: Panic attack and agoraphobia, separation anxiety, physical injury fears, social phobia, obsessive–compulsive and generalised anxiety. The scale has parent and child versions on which respondents rate each item using a 4-point scale (Never, Sometimes, Often and Always). Spence (1997, 1998) reports excellent psychometric properties for the SCAS scale: internal reliability coefficient = .93, Guttman split-half reliability = .92 and test–retest reliability across 6 months = .60. The current study also found good internal reliability (from .84 to .92) on all the sub-scales.
Cognitive ability
This was estimated using the Vocabulary test from the Wechsler Intelligence Scale for Children–Fourth UK Edition (WISC-IV, Wechsler, 2003). This test assesses understanding of word knowledge and verbal concept formation in children aged 6 years–16 years and 11 months. The Vocabulary sub-test is considered ‘to be the best single indicator of general intelligence’ (Groth-Marnat, 2009: 151), correlating .72 with the full-scale IQ on the WISC-IV scale. It was thus used as a proxy measure of cognitive ability in children in the current study, and it showed good reliability in both the HFASD (α = .82) and TD (α = .84) groups.
HFASD
The Childhood Autism Syndrome Test (CAST: Scott et al. (2002) was designed and standardised for the screening of children aged 4–12 years at risk for autism-related symptoms. It was used to provide independent confirmation of the presence of autism symptoms in the HFASD group and their absence in the TD group. It consists of 37 statements about the child’s current level of functioning in social, cognitive and communication domains. Parents are asked to mark either ‘yes’ or ‘no’ for each statement on the scale. Scores of 15 and over generally reflect clinical levels of difficulties associated with autism (Scott et al., 2002). The CAST scale showed high reliability for both the HFASD (α = .80) and TD (α = .79) groups.
Procedure
Personal accounts of past frustrating, emotional experiences were elicited from both TD and HFASD participants (see section ‘Measures’). These same children participated in the main study which took place 2 months later. For all self-report scales, children were asked whether they would prefer questions to be read aloud or whether they preferred to read them on their own. All children preferred the questions to be read aloud.
Difficulties with self-awareness and self-expression have been documented across the autism spectrum disorder; however, this ability is known to be well developed for high-functioning individuals with autism (Braverman et al., 1989; Ozonoff et al., 1989). To account for any difficulties understanding or completing self-report questionnaires, pictorial aids were presented, each question was repeated twice, and children were always asked whether they fully understood the questions. Parents were also present in the same room to provide assistance if necessary. The content of all measure was clearly outlined to both parents and children in advance to avoid any anxieties resulting from unpredictability or exposure to novel stimuli; these strategies have been shown to be successful with children with autism (Ozonoff, 1997; Ozonoff and Jensen, 1999). All 44 children in both the HFASD and TD groups had the questions read out to them. Two children in the TD group initially chose to read the materials themselves but subsequently stopped and asked the researcher to read for them. Scales were presented in the same order to all children: Strange Stories, hypothetical frustrating scenarios, the appraisal and fear questionnaires, the SCAS (child version) and finally the Vocabulary sub-test. The CAST scale was completed by parents separately, after testing with their child was completed. All children were given a break of 8–10 min after administration of the appraisal and fear questionnaires before continuing with the remaining measures.
Analysis strategy
Initial data cleaning procedures consisted of missing and out-of-range value analysis and double entry of a randomly selected 10% of responses. Assessment of skewness and kurtosis was also carried out, but all data were found to be normally distributed. Between-group differences for background characteristics (age, gender, CAST scores and Vocabulary sub-test of WISC-IV scale), fear, anxiety (Hypothesis 1), TOM ability (Hypothesis 2) and appraisal dimensions (Hypothesis 3) will be investigated through independent t-tests. The correlation results will be reported for assessing association of appraisals with fear and anxiety (Hypothesis 4), and linear regression analysis will be carried out to assess the strength of association between appraisals and TOM ability (Research Question 1).
Results
Sample characteristics
There was no difference in age or gender between the HFASD and TD groups (see Table 1). On the CAST scale, the HFASD group had a significantly higher mean than the TD group with a large effect size (see Table 1). Scores for all children in the HFASD group ranged from 15 to 27, indicating the presence of symptoms of autism in this group (Williams et al., 2005), while the TD group’s scores ranged from 1 to 12, that is, below the cut-off value of 15. For the WISC-IV Vocabulary sub-test, children in the HFASD group did not significantly differ from those in the TD group, and both groups scored within the average range. These two results together provided independent supporting evidence that the children were correctly classified into HFASD and TD groups.
Sample characterisation: age, gender, CAST scores and Vocabulary sub-test of WISC-IV scale.

HFASD: high-functioning autism spectrum disorder; TD: typically developing; SD: standard deviation; CAST: Childhood Autism Syndrome Test; WISC-IV: Wechsler Intelligence Scale for Children–Fourth UK Edition.
p < .001.
Differences between HFASD and TD groups on fear and anxiety (Hypothesis 1)
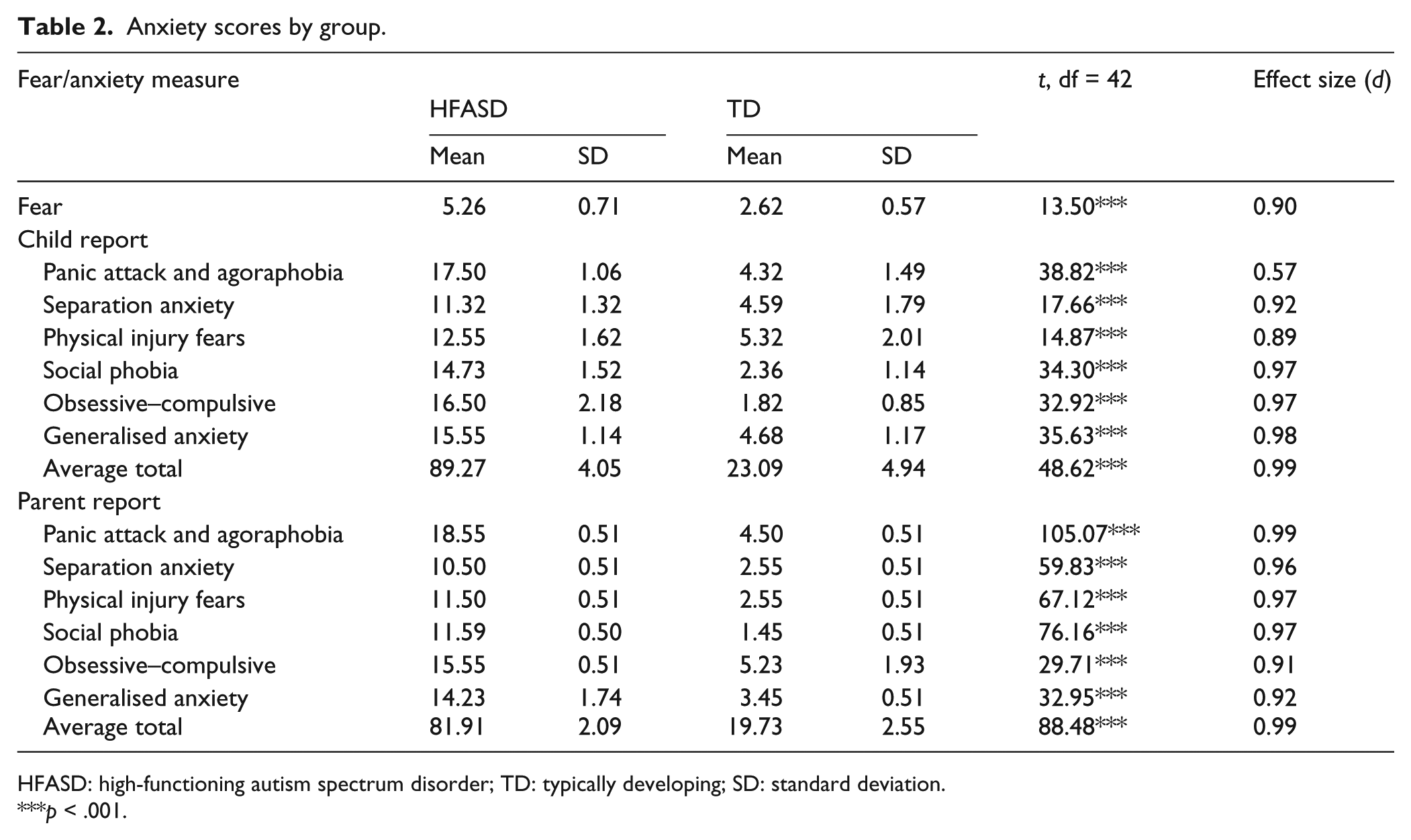
The HFASD group had significantly higher fear scores and significantly higher anxiety scores than the TD group on all six sub-scales of both the child-report and the parent-report versions of the SCAS with large effect sizes (see Table 2).
Anxiety scores by group.
HFASD: high-functioning autism spectrum disorder; TD: typically developing; SD: standard deviation.
p < .001.
Differences between HFASD and TD groups on appraisals (Hypothesis 2)
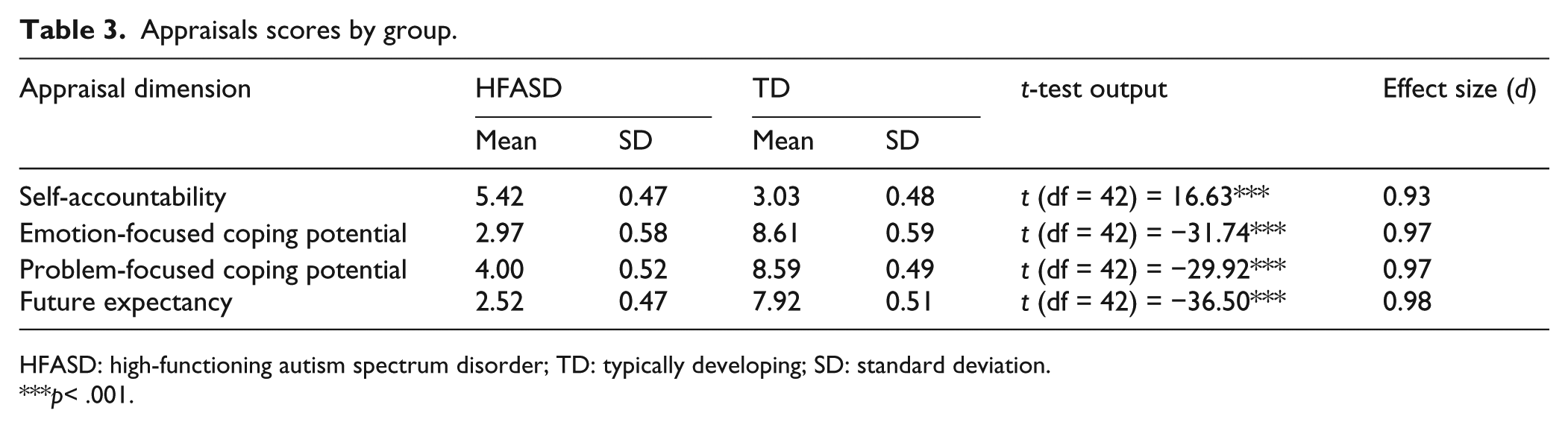
Table 3 shows that the HFASD group had significantly lower emotion-focused coping potential, problem-focused coping potential and future expectancy than the TD group, but significantly higher self-accountability. These findings indicate that in hypothetical frustrating situations, children in the HFASD group held negative expectancies about the outcome, had low confidence in their ability to deal with the adverse consequences of that situation and took greater responsibility for negative outcomes.
Appraisals scores by group.
HFASD: high-functioning autism spectrum disorder; TD: typically developing; SD: standard deviation.
p< .001.
Differences between the HFASD and TD groups on TOM (Hypothesis 3)
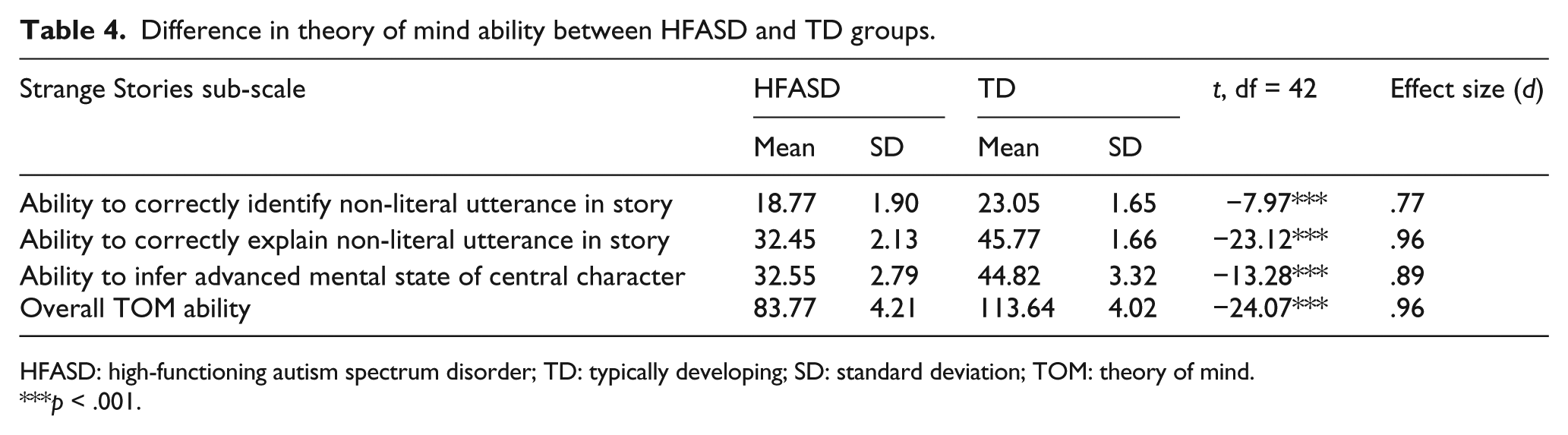
As hypothesised, the HFASD group scored significantly lower than the TD group on TOM ability. This was true for TOM overall and also for all three sub-scales (see Table 4).
Difference in theory of mind ability between HFASD and TD groups.
HFASD: high-functioning autism spectrum disorder; TD: typically developing; SD: standard deviation; TOM: theory of mind.
p < .001.
Association of appraisals with fear and anxiety (Hypothesis 4)
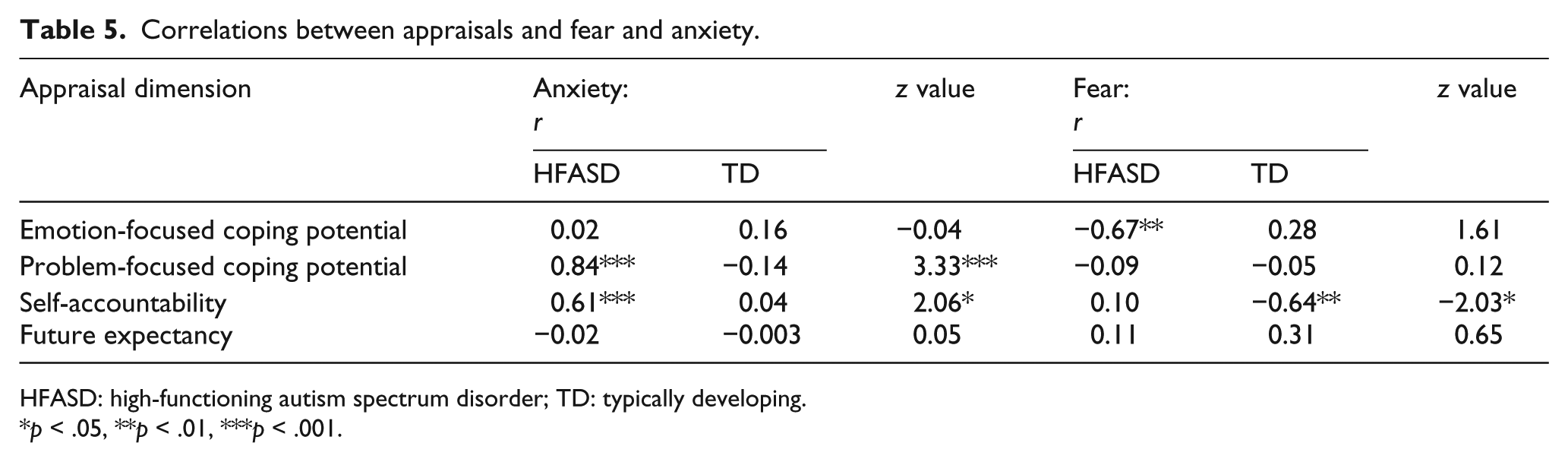
Anxiety was significantly correlated with problem-focused coping potential and self-accountability appraisals for the HFASD group. There were no significant appraisal accountability correlations for the TD group (see Table 5). These findings indicate that in hypothetical frustrating social situations, low expectations about the outcome and low confidence in one’s own ability to deal with the adverse consequences of a situation were associated with higher anxiety in the HFASD group. For fear, only the negative correlation with emotion-focused coping potential was significant for the HFASD group, and only the positive correlation with self-accountability was significant for the TD group.
Correlations between appraisals and fear and anxiety.
HFASD: high-functioning autism spectrum disorder; TD: typically developing.
p < .05, **p < .01, ***p < .001.
Correlation coefficients for the HFASD and TD groups were compared to see whether they were significantly different using Fisher’s r–z transformation (Howell, 2007). There were significant between-group differences for the correlation of anxiety with appraisal of problem-focused coping potential, anxiety with self-accountability and fear with self-accountability (see Table 5). However, there were no significant differences between the HFASD groups in correlations between anxiety and emotion-focused potential and fear and emotion-focused coping potential.
Associations between appraisal dimensions (Research Question 1)
Bivariate correlation analysis showed that in the HFASD group, emotion-focused coping potential was significantly associated with future expectancy and self-accountability with problem-focused coping potential (see Table 6). There were no significant correlations in the TD group.
Associations between appraisal dimensions.

HFASD: high-functioning autism spectrum disorder; TD: typically developing.
p < .05.
Association of appraisals with TOM ability (Research Question 2)
Two linear regressions, each using the Enter method, were carried out with the four appraisal dimensions of self-accountability, emotion-focused coping potential, problem-focused coping potential and future expectancy as the predictor variables and TOM ability as the outcome variable. The first regression, with the HFASD participants, resulted in a significant model, F(4, 17) = 14.72, p < .001, and explained 77.6% of the variance (Adjusted R2 = .78). Emotion-focused coping potential (β = .41, p = .007), problem-focused coping potential (β = −.54, p = .001) and future expectancy (β = .43, p = .005) were all significant and unique predictors of TOM ability; however, self-accountability (β = .23, p = .10) was not significant. The second regression, with the TD participants, was not significant, F(4, 17) = 1.70, p = .19, Adjusted R2 = .29.
Discussion
The HFASD group scored significantly higher than the TD group on fear and on all six categories of anxiety disorders. This robust evidence, from both child and parent reports, strengthens previous findings based on parent report only (e.g. Kim et al., 2000; Mazefsky et al., 2010; Muris et al., 2000; Witwer and Lecavalier, 2010). Our results also indicate that the HFASD group’s appraisals reflected higher self-accountability, lower emotion-focused and problem-focused coping potential and lower future expectancy than was the case for the TD group. The finding that appraisals are associated with fear and anxiety for children in the HFASD group is novel. Furthermore, associations between appraisals and feelings of both fear and anxiety were significantly different for the HFASD and TD groups. These findings are discussed in detail in the following.
The significant association between self-accountability and anxiety in the HFASD group supports previous studies of children with anxiety disorders where inflated self-blame was indicated as a problematic cognition underpinning anxiety (Freeston et al., 1996; Rassin et al., 2000; Rheaume et al., 1995). The current findings support previous research associating anxiety with negative expectancies and perceptions about ability to cope among non-autistic individuals with anxiety (Creswell et al., 2005; Thorpe and Salkovskis, 1995) and non-anxious adolescents (Smari et al., 2001). As far as we are aware, there is no published evidence on cognitive appraisals in an HFASD sample.
The finding that only one appraisal dimension is associated with fear in both the HFASD and TD groups is consistent with Smith and Lazarus’s (1993) model. They report an association between emotion-focused coping potential and fear in TD individuals; in contrast, we found that this association only among the HFASD group and not in the TD group. For the TD group, we found self-accountability was associated with fear. It could be that in TD children, appraisal–emotion relationships are different from adult appraisal–emotion relationships, and also that such relationships are different in TD and autism groups. It is also possible that the current study was under-powered: regression models with sample sizes smaller than 109 combined with the number of predictors may be unable to detect smaller effects relating to individual predictor variables, even though they are adequate when testing the significance of the overall regression model (Green, 1991).
As with previous research findings, the HFASD group also scored significantly lower than the TD group on all three sub-scales of the Strange Stories task. Further analysis showed that three of the four appraisal types were uniquely associated with TOM ability in the HFASD group but not in the TD group. This suggests that appraisals may be associated in some way with the deficit in TOM ability observed in children with autism spectrum disorders. Previously, TOM ability has been shown to be associated with emotional difficulties (Brent et al., 2004), and our results suggest that there is merit in testing the proposal that appraisals mediate this relationship. Specifically, lower levels of TOM may reduce children’s perceived ability to deal with frustrating situations and may increase the anticipation of poor outcomes, possibly as a result of the contextual ambiguity introduced by poor TOM ability. Future research should test this hypothesis.
The findings from the current study suggest that cognitive appraisals might be crucial in understanding fear and anxiety, and that these appraisals might form the focus of cognitive restructuring techniques employed to counter anxiety in this group. There are already cognitive-based treatment programmes aimed at improving TOM ability and reducing the occurrence of anxiety in children with autism (Sofronoff et al., 2005; White et al., 2010). Our findings provide a new direction for research into which specific cognitions could be targeted in cognitive therapy programmes designed to treat of fear and anxiety in children with HFASD. Based on the current findings, cognitions related to negative expectancies about the outcome of a situation and low belief in one’s ability to deal with the adverse consequences of a situation are significantly associated with anxiety. Such cognitions could be targeted in a cognitive intervention programme to improve expectancies and belief in one’s own ability.
One limitation of the present study was its use of scenarios describing frustrating events. This technique relies upon the ability of children with HFASD to both understand a story and correctly report how they would think and feel if they were in a similar situation. However, as children with autism are known to experience difficulty understanding social contexts (Ropar et al., 2003; Sobel et al., 2005), this may limit the effectiveness of their engagement with the task. Furthermore, while this experimental method increases our ability to control extraneous variables, it also places constraints upon the ecological validity of the results. Nonetheless, this was the first study of the relationship of appraisals with TOM ability, fear and anxiety in children with HFASD, and as such provided a useful starting point for further research.
A second limitation of the study is that parents were relied upon to accurately report diagnoses of high-functioning autism. We were able to independently assess the likely accuracy of these reports using the CAST scores of both groups, though we acknowledge that the CAST only identifies children at risk of autism and is not a diagnostic instrument. A final limitation of the study is the use of the WISC-IV Vocabulary sub-test as a proxy measure of IQ. It should be noted that while this correlates well with the full-scale WISC-IV IQ for TD individuals (Groth-Marnat, 2009), this relationship has not been verified for children with autism spectrum disorders.
In conclusion, the present study was the first to investigate the relationships between anxiety and the appraisals of social situations among children with and without HFASD. Children in the HFASD group appraised social situations in specific and potentially maladaptive ways characterised by higher self-accountability, lower coping potential and lower future expectancy when compared to a TD group. Appraisal styles similar to these have previously been associated with anxiety and negative emotions in groups of children without autism. The present study reports that a significant association between TOM ability and appraisal dimensions was present only for children with HFASD. Future investigation of these issues is important for both developing theory relating to our understanding of fear and anxiety in children with HFASD and developing interventions directed toward more positive cognitions.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.