
Abstract
Previous research has investigated caregiver attachment relationships in children with autism during early childhood, with few differences found from matched control groups. However, little is known of this relationship during middle childhood (ages 8–12 years). In this study, the aim was to establish whether there are differences in the security of attachment in children with high-functioning autism compared to typically developing children. A secondary aim was to establish whether caregivers’ perceptions of their child’s attachment to them accorded with the children’s own reports. Twenty-one children with high-functioning autism and 17 typically developing children were administered the Kerns Security Scale and the Inventory of Parent and Peer Attachment–Revised, and caregivers completed the same questionnaires from the viewpoint of their child. There were no differences between the groups in the children’s and parents’ reports of attachment security. Parents’ and children’s reports were moderately correlated on the Kerns Security Scale but were not correlated on the Inventory of Parent and Peer Attachment–Revised. The results indicate that levels of attachment security in children with high-functioning autism are not different from those in typically developing children.
The current study focused on the child-to-caregiver attachment relationship in children with high-functioning autistic disorder (HFA) during their middle childhood years. To date, the research on attachment in children with autism is largely limited to young preschool-aged children. Current evidence that the attachment relationship is important for other areas of psychosocial adjustment in middle childhood and beyond, such as emotional regulation, self-esteem, scholastic performance and social adjustment, calls for a better understanding of the attachments evidenced by school-aged children with autism.
The attachment relationship is a differential, affectional tie formed with the primary caregiver. In infancy and early childhood, the attachment figure is a ‘secure base’ for exploration and a ‘safe haven’ when the child is distressed (Ainsworth et al., 1978). Attachment in early development is expressed through marker behaviours that attract the caregiver’s attention, such as smiling and vocalising, and those that engage the caregiver in interaction, such as crying and clinging, which elicit care and protection by increasing proximity to the caregiver (Bowlby, 1969).
While all children develop caregiver attachments, these may differ in quality. The ‘Strange Situation’ laboratory procedure was developed to assess attachment security, using behavioural observations of young toddlers (12–20 months of age) upon separation and reunion with their caregiver (Ainsworth et al., 1978). Three attachment classifications were identified – ‘secure’ (B), ‘insecure-avoidant’ (A), and ‘insecure-ambivalent’ or ‘resistant’ (C). Main and Solomon (1990) identified a fourth classification, ‘disorganised’ or ‘disoriented’ attachment. In typical development, the majority of children (65%) display attachment security (Van IJzendoorn et al., 1992), which is theoretically and empirically linked to parental sensitivity (De Wolff and Van IJzendoorn, 1997).
As children develop, changes in cognitive abilities enable the attachment relationship to become internalised (Ammaniti et al., 2000). Bowlby (1969) referred to children’s cognitive or representational models of themselves in relation to their caregiver as ‘internal working models’ of attachment, which develop and become more elaborate from the second through the sixth year of life (Marvin and Britner, 2008). The internalisation of the attachment relationship reduces the requirement for physical proximity and contact (Marvin and Britner, 2008), and emotional availability takes over the focus from physical availability (Kerns et al., 2006).
Internal working models of attachment are schemas, which summarise prior attachment experiences (positive and negative) and inform future behaviour (Bretherton, 1985) and which guide the child’s perceptions of appropriate behaviour, his or her own self-worth and expectations of the caregiver’s and others’ behaviours (Thompson and Raikes, 2003). These internal working models also incorporate implicit decision rules about how to relate to others, which then influence the development of new relationships (Bretherton and Munholland, 1999). As Thompson and Raikes (2003) explain, ‘these models become interpretive filters through which children (and adults) reconstruct their understanding of new experiences and relationships in ways that are consistent with past experiences and expectations’ (p. 696). Thus, internal working models of attachment not only reflect the reality of the child’s relationships but also create the reality of future relationships (Bretherton, 2005).
At around 4 years of age, most children are able to correctly distinguish between their own and others’ mental perspectives and are able to consider these simultaneously. With the onset of this theory of mind ability, children become able to simultaneously consider their own goals and plans and their caregiver’s goals and plans, which facilitates a ‘goal-corrected partnership’ whereby the caregiver and child negotiate to reach a common goal (Bowlby, 1973). However, children with autism are characteristically impaired in theory of mind (Baron-Cohen et al., 1985). Attachments are further influenced by the developmental changes that occur during middle childhood (at age 7–12 years), such as, cognitive developments that include improvements in metacognition, memory and cognitive flexibility; social developments including the increased salience of peers, a shift from parental control to parent–child co-regulation and an enhanced understanding of others; and psychological developments, which include increased emotional regulation and self-awareness and a greater understanding of psychological traits (Kerns, 2008). These developments, most of which are problematic among those with autism, allow children’s internal working models to become both more elaborate and organised (Mayseless, 2005).
Although early observations suggested that children with autism may not develop attachments to their caregivers (e.g. Kanner, 1943; Rutter, 1978), there is now substantial empirical evidence that children with autism do develop these attachments (e.g. Dissanayake and Crossley, 1996; Sigman and Ungerer, 1984). In a review of attachment studies in children from 2 to 6 years, Buitelaar (1995) concluded that children with autism do form attachment relationships as evidenced by preferential proximity seeking and reunion behaviour after separation. Rutgers et al. (2004) conducted a meta-analysis on 10 studies focused on attachments in children with autism with age ranging from 2 to 5 years. The children with autism did develop caregiver attachments with 40%–63% being secure attachments, which was less than that achieved in various comparison groups (e.g. typically developing (TD) children, children with developmental language disorder and children with Down Syndrome). However, no differences in attachment security were found between the groups when only children with HFA (those with IQ within the normal range of intellectual functioning) were compared to the TD children. The authors concluded that it is not autism alone but the combination of autism and intellectual impairment that contributes to attachment insecurity. This conclusion was supported by Willemsen-Swinkels et al. (2000) and Naber et al. (2007) who found higher rates of disorganised attachment in children who had both autism and an intellectual impairment compared to control children. Similarly, Rogers et al. (1991, 1993) reported that developmental level, as measured by mental age (MA), predicted attachment security in children with autism more strongly than the severity of autism symptoms.
In recent years, attachment research in this area has extended into young children at risk of an autism spectrum disorder (ASD) as well as older, school-aged children with high-functioning ASD. Haltigan et al. (2011) reported that 15-month-old siblings of older children with an ASD (autism, Asperger’s disorder or pervasive developmental disorder–not otherwise specified) were no more or less likely than siblings of children without an ASD to form secure attachment relationships with their caregiver. In relation to older children, a study investigating the impact of social relationship variables (attachment security and mother–child relationship qualities) and social-cognitive abilities (theory of mind) on friendships in 8- to 12-year-old children with high-functioning ASD (autistic disorder or Asperger’s disorder) reported that 54.5% of these children reported secure attachments to their mothers, compared to 71% of TD children (Bauminger et al., 2010). However, this difference was not significant, which is consistent with research findings for younger children with autism. Further research is required to establish whether these results can be replicated in this age group.
Extending into adulthood, Taylor et al. (2008) reported on attachment in 20 adults aged 19–60 years with high-functioning ASD. Based on the Adult Attachment Interview (George et al., 1996), 3 of the 20 adults were classified as securely attached – markedly less than what would be expected based on studies of younger children (e.g. Rutgers et al., 2004). The authors note, however, that many of the participants had additional psychiatric diagnoses, and the rate of secure attachments found is in accordance with the rate expected in a general clinical sample.
Kraemer (1992) proposed two forms of attachment: first, an innate, psychobiological form, and second, a more cognitive form that incorporates internal working models of attachment (Dissanayake and Sigman, 2001). While previous research suggests that the psychobiological form of attachment might not differ in children with autism, Rogers et al. (1993) suggest that children with autism may experience difficulty in the development of the cognitive form.
The primary aim in this study was to establish whether there are differences in the security of the attachment relationship in school-aged children with HFA compared to TD children, both in terms of overall attachment security and individual components of this relationship. The secondary aim was to establish whether caregivers’ perceptions of their children’s attachment to them are consistent with their children’s own reports in an effort to validate the children’s reports. On the basis of previous findings on early childhood attachments in autism, one may hypothesise that the security of the attachment relationship in middle childhood will be similar to those of TD children. However, on the basis of their established impairments in social cognition and peer relationships, which are important in the further development of the internal working model, it may be expected that attachment security will be lower in those with HFA relative to TD children.
Method
Participants
Participants included 38 boys aged between 8 and 12 years, accompanied by either their mother or both parents, and in one case, a grandmother who had been the child’s legal guardian since he was 2 months of age. Girls were not recruited due to the higher incidence of autistic disorder in boys compared to girls (Fombonne, 2003). The HFA group comprised 21 children with a clinical diagnosis of autistic disorder (according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria, American Psychiatric Association (APA), 1994) without intellectual disability (full scale IQ, verbal IQ and performance IQ exceeding 70). The control group comprised 17 TD children.
The Autism Diagnostic Observation Schedule (ADOS, Module 3; Lord et al., 2002) was administered to the children in the HFA group to confirm diagnosis. In all, 17 children met criteria for autistic disorder and four met criteria for ASD. The TD children were screened for symptoms of autism using the Social Communication Questionnaire (SCQ; Rutter et al., 2003), completed by parents. A score of 15 or greater on the SCQ indicates further assessment for autism is recommended, with the TD children receiving scores ranging from 0 to 9.
Sample characteristics
All children attended mainstream primary schools, enhancing comparability across the HFA and TD groups in terms of their academic and social learning opportunities. They were each administered the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999). Verbal MA was calculated as the mean MA of the vocabulary and similarities subtests; performance MA was calculated as the mean MA of the block design and matrix reasoning subtests. Overall MA was calculated as the mean MA of these four subtests.
Sample characteristics are presented in Table 1. The two groups were matched on chronological age (CA), t(28.63) = −.072, p = .943, and performance MA, t(36) = 1.73, p = .091, but the TD children had a significantly higher overall MA and verbal MA, t(36) = 2.54, p = .016 and t(36) = 3.12, p = .004, respectively. These variables were, therefore, considered as covariates in any analyses where they were correlated with the dependent variable of interest.
Sample characteristics for the HFA and TD groups.
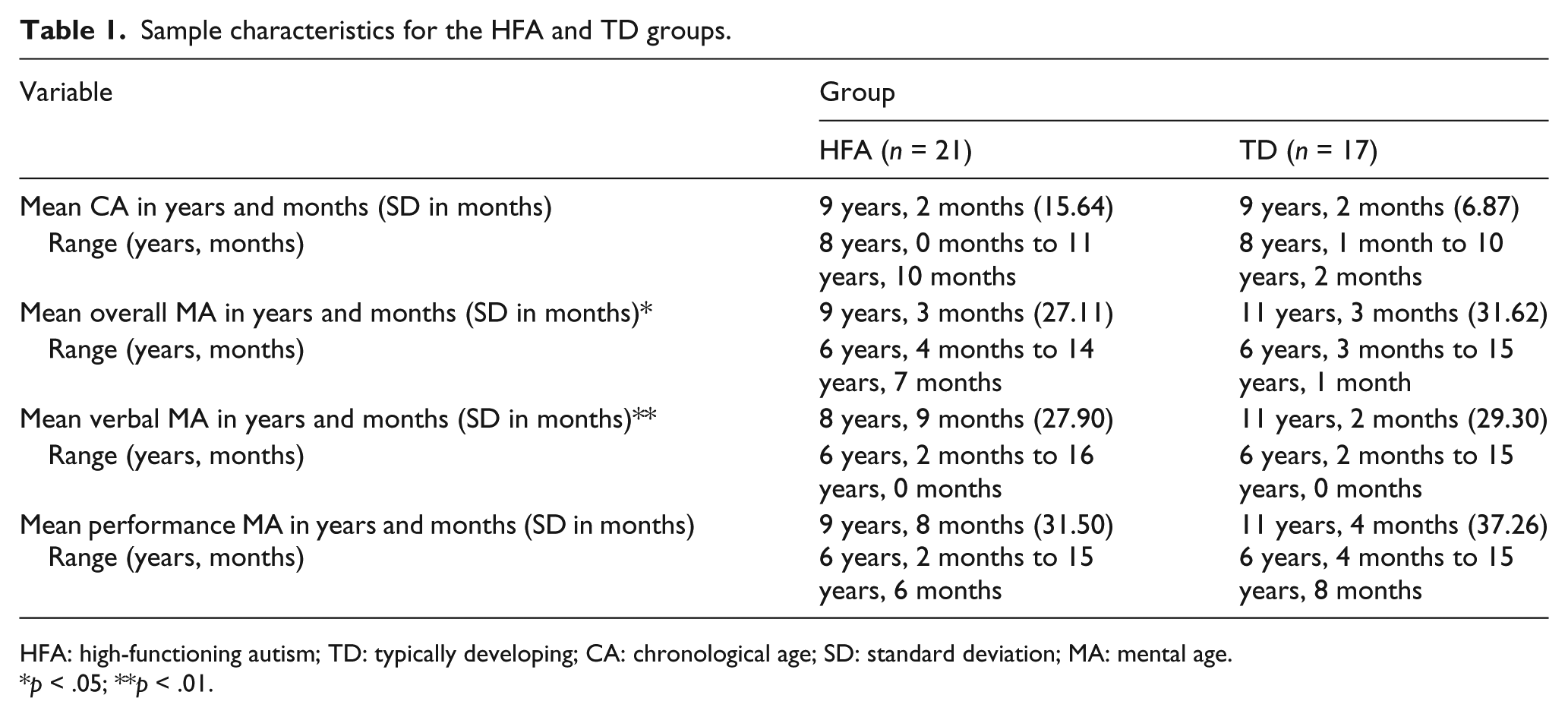
HFA: high-functioning autism; TD: typically developing; CA: chronological age; SD: standard deviation; MA: mental age.
p < .05; **p < .01.
The groups did not differ in relation to maternal age (HFA: M = 39.24 years, TD: M = 41.47 years) or paternal age (HFA: M = 41.30 years, TD: M = 43.13 years), parental employment (HFA: 19% of mothers and 86% of fathers employed full time, TD: 6% of mothers and 77% of fathers employed full time), parental education (HFA: 62% of mothers and 57% of fathers with a tertiary degree, TD: 65% of mothers and 59% of fathers with a tertiary degree) or household income (both groups had average income range from AU$60,000 to AU$70,000 per annum).
As the focus of the current study was on children’s attachment to their caregiver, the child’s primary caregiver was of interest. The majority of parents of TD children (71%) shared the care between mother and father, whereas more children with HFA (52%) were primarily cared for by their mothers. Although more mothers were the primary caregivers in the HFA group, the Chi-square test for independence (with Yates Continuity Correction) indicated no significant differences between the groups (p > .05).
Measures
The Kerns Security Scale (KSS; Kerns et al., 1996, 2001) is a 15-item child report questionnaire designed to measure children’s perceptions of attachment security in the caregiver relationship during middle childhood. Items are grouped into the subscales of ‘dependency’ (e.g. whether a child finds it easy to trust his or her parent) and ‘availability’ (e.g. whether a child worries that a parent will not be there when needed) (Lieberman et al., 1999).
The scale presents pairs of statements based on the Harter scale (1982) in which children are presented with two possible response types (e.g. ‘Some kids wish they were closer to their Mum’ but ‘Other kids are happy with how close they are to their Mum’) and are asked to indicate which group of kids they are most like. This method of identifying with either one or the other groups of kids decreases the child’s likelihood of responding in a sociably desirable manner (Harter, 1982). Items on the KSS are scored between 1 and 4 (range: 15 to 60), with a higher score indicative of a more secure attachment. Internal consistency has been demonstrated with Cronbach’s alphas around .80 or higher (Kerns et al., 2005), and 2-week test–retest reliability is also adequate (r = .75; Kerns et al., 1996). Positive correlation with a secure attachment prototype based on the Doll Story Completion Task, (r = .38, p <.001), and negative correlation with an avoidant attachment prototype, (r = −.30, p <.001), are given as evidence of construct validity (Granot and Mayseless, 2001).
The Inventory of Parent and Peer Attachment–Revised (IPPA-R; Armsden and Greenberg, 1987; Gullone and Robinson, 2005) is a 28-item child report questionnaire measuring the quality of attachment to parents (and peers) and how well they serve as a source of psychological security. Only the parent–child scale was used in the current study. The original IPPA (Armsden and Greenberg, 1987) was designed to assess attachment in 16- to 20-year-olds and was later adapted by Gullone and Robinson (2005) to measure attachment in 9- to 15-year-old children. While the content of the 28 items remained the same, the wording of some items was simplified for the younger age group (e.g. ‘I feel my parents are successful as parents’ was modified to read ‘My parents are good parents’). This measure has also been used successfully with 8-year-old children (e.g. Bauminger et al., 2010).
While the IPPA-R uses a more simplistic 3-point response scale (‘never true’, ‘sometimes true’ and ‘always true’) for the younger age group, a 5-point response scale was employed in the current study (‘almost never or never true’, ‘rarely’, ‘sometimes’, ‘often’, ‘almost always or always true’), as is used in the original IPPA (Armsden and Greenberg, 1987). The decision to use the original 5-point scale was to ensure variability in the data, as the extreme options of ‘never’ and ‘always’ could potentially lead to over-reporting of the only other response: ‘sometimes’. The use of Likert scales has been recommended for children aged 6 to 18 years, and 5-point scales have been used successfully with this age group (Van Laerhoven et al., 2004). Possible total scores ranged from 28 to 140 on this measure.
Items in the IPPA are grouped into the subscales of ‘trust’ (i.e. the degree of mutual understanding and respect in the attachment relationship), ‘communication’ (i.e. the extent and quality of spoken communication) and ‘alienation’ (i.e. feelings of anger and interpersonal alienation). A total score is obtained by calculating the sum of these three subscales (Armsden and Greenberg, 1987; Gullone and Robinson, 2005) with higher total scores indicating greater attachment security.
Internal consistency of the three subscales of the IPPA-R is reported to range from .76 to .83 (Gullone and Robinson, 2005), and the average test–retest reliability over a 3-week period for the original IPPA is reported as .93 (Armsden and Greenberg, 1987). Positive correlations with children’s scores on the Self-Esteem Inventory (r = .51, p < .001) and the Care subscale of the Parental Bonding Instrument (PBI) (r = .73, p < .001) and a negative correlation with the Overprotection subscale of the PBI (r = −.51, p < .01) are given as evidence of construct validity (Gullone and Robinson, 2005).
Procedure
Children and at least one caregiver, usually the child’s mother, attended the Olga Tennison Autism Research Centre at La Trobe University. Caregivers completed a demographic and background information questionnaire, and the KSS and IPPA-R to ascertain whether their perception of the child’s attachment to them matched their children’s reports. At the same time, the children were administered the WASI, KSS and IPPA-R by one of the two female experimenters. The caregivers of TD children also completed the SCQ, and children with HFA were administered the ADOS.
Results
Child-to-caregiver attachment
KSS
Descriptive statistics for children’s total score, dependency and availability attachment ratings on the KSS are presented in Table 2, and as is evident from this table, there were no differences between the children with HFA and TD children. A one-way analysis of covariance (ANCOVA) on the total score confirmed this, F(1, 35) = 0.10, p = .75,
Adjusted mean (standard deviation (SD)) child and parent ratings on the KSS.

KSS: Kerns Security Scale; HFA: high-functioning autism; TD: typically developing.
Descriptive statistics for parents’ total score, dependency and availability ratings on the KSS are also presented in Table 2. An ANCOVA indicated no difference between parental reports of the groups on total attachment ratings, F(1, 35) = 0.47, p = .50,
IPPA-R
Descriptive statistics for children’s total score and trust, alienation and communication ratings on the IPPA-R are presented in Table 3. In keeping with the findings on the KSS, the ANCOVA on the total attachment security score indicated no difference between the groups, F(1, 35) = 0.22, p = .64,
Adjusted mean (standard deviation (SD)) child and parent ratings on the IPPA-R.

IPPA-R: Inventory of Parent and Peer Attachment–Revised; HFA: high-functioning autism; TD: typically developing.
Descriptive statistics for parents’ scores on the IPPA-R are also presented in Table 3. The independent-samples t-test conducted to compare the parents’ total scores showed no significant difference between the groups, t(36) = 1.90, p = .065. The magnitude of the differences in the means (mean difference = 9.00, 95% confidence interval (CI): −0.60 to 18.60) was moderate (
Parent–child agreement
KSS
The correlations between children’s and parents’ ratings of attachment security on the KSS were investigated using Pearson’s product–moment correlation coefficients. For children with HFA, parent and child total scores were moderately positively correlated, r = .39, p = .08, as were the dependency scores, r = .49, p = .03. However, parent and child availability scores were not correlated, r = .07, p = .77. For TD children, the relationships between children’s and parents’ ratings of attachment on the KSS were investigated using partial correlations, as overall MA was related to both parent and child ratings. Moderate, positive correlations were present between child and parent total scores, partial r = .46, p = .08, and dependency scores, partial r = .46, p = .07. Once again, there was no relationship between parent and child availability scores, r = .11, p = .70.
IPPA-R
The correlations between children’s and parents’ ratings of attachment security on the IPPA-R indicated that the agreement between children and their parents in each group was negligible. For the HFA group, parents’ and children’s total scores were not correlated, r = .02, p = .92, nor were their trust scores, r = .05, p = .84, communication scores, r = .02, p = .94, or alienation scores, r = .11, p = .62. The findings for the TD group were similar: total scores: r = −.01, p = .99; trust: r = −.09, p = .75; alienation: r = .17, p = .51; and communication: r = .14, p = .60.
Discussion
Overall, the security of attachment between children with HFA and TD children were largely similar, as reported by themselves and their parents. Despite their well-known difficulties in the social realm, including their social cognition and peer relationships, the middle-school-aged children and their parents from both groups reported similar levels of total attachment security and perceptions of dependency and availability on the KSS. Likewise, children from both groups reported similar levels of total attachment security and perceptions of trust, alienation and communication on the IPPA-R, and parents from both groups also reported similar levels of total attachment security on this measure.
The findings from this study are in accordance with those from previous research on attachments in younger children with autism as well as children of a similar age group. Consistent with the findings of Rutgers et al. (2004) and Bauminger et al. (2010), there were no differences between these children and TD children in the security of their attachments to their caregivers.
Correlations between parents’ and children’s reports of attachment
Correlations between parents’ and children’s reports on the attachment measures also revealed comparable patterns across the two groups. Parents’ and children’s total scores on the KSS were moderately, positively correlated, for both the HFA and TD groups. The dependency ratings showed the highest correlations for both groups, with no correlation between availability scores, indicating that children and parents from both groups may either have interpreted the meaning of ‘availability’ differently or that the children simply disagreed with their parent’s reports of their availability for their child. In contrast to the KSS, there were no correlations between parents’ and children’s total scores on the IPPA-R for either group. Thus, parents and children from both groups did not agree at all on attachment security as measured by the IPPA-R, whereas moderate agreement was achieved on the KSS. As a result, findings on the IPPA-R must be interpreted with caution as the questions on this measure may be differentially interpreted by parents and middle-school-aged children with and without ASD.
Possible explanations for the discrepancy between parents’ and children’s ratings on the IPPA-R include social desirability and normalising relating to the response formats of the attachment measures. The KSS presents pairs of statements based on the Harter scale (1982), ‘some kids/other kids’ format, in which children are presented with two possible response types and are asked to indicate which group of kids they are most like. This response format decreases the child’s likelihood of responding in a sociably desirable manner (Harter, 1982) and also serves to normalise both response options. In contrast, the IPPA-R requests that children respond to statements such as ‘my parents are good parents’ with a frequency (‘never or almost never’ through to ‘always or almost always’). There is potential, using this response format, for children to answer these questions in a more socially desirable manner as they are more personalised, which may have resulted in the low levels of agreement between parent and child reports on this measure.
Study limitations
The inclusion of only boys in the current study limits the generalisability of the results to the female population. Due to the much higher incidence of autism in boys than girls, there is comparatively little research specifically addressing the presentation of autism in girls. However, gender differences in autism have been noted in developmental functioning, autism symptoms and severity and behavioural problems (see Hartley and Sikora, 2009, for a review). Given the disagreement in the field regarding gender differences in attachment during middle childhood in the typical population, even less is known about the effect of gender on attachment in children with HFA (Bakermans-Kranenburg and Van IJzendoorn, 2009a, 2009b; Del Giudice and Belsky, 2010; Kerns et al., 2007; Van IJzendoorn and Bakermans-Kranenburg, 2010).
Clinical implications: facilitating attachment security
Facilitating the development of attachment security is clinically important given the established relationship between the security of attachment and psychosocial outcomes throughout development. A secure attachment has been associated with higher positive mood, increased constructive coping, emotional and behavioural regulation, increased global self-worth and perceived competencies, improved friendship quality and social competence (Granot and Mayseless, 2001; Kerns et al., 2006, 2007). In contrast, an insecure-ambivalent attachment has been associated with social anxiety, and insecure-avoidant and insecure-ambivalent attachments have been associated with internalising and externalising behaviour problems (Brumariu and Kerns, 2008; Granot and Mayseless, 2001). While a diagnosis of autism may increase a child’s risk of developing emotional, social and behavioural problems, a secure attachment relationship may represent a protective factor for these children, and its development should be fostered.
Future directions
To date, no research has investigated the outcomes of developing a secure attachment in ASD, and this empirical gap needs to be addressed in order to argue that the child–caregiver attachment relationship in ASD functions in the same way as in children without an ASD. Given the assumed clinical implications of developing a secure attachment relationship and the deficits in social-emotional and social-cognitive skills that often characterise ASDs, it is important that future research investigate the role that these skills play in the development of attachment in this population. Social-emotional and social-cognitive skills that may impact this development include self-perception, empathy, theory of mind and memory. Understanding which of these skills contribute uniquely to the development of a secure attachment may allow for specific interventions to target these areas to facilitate positive outcomes.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.