
Abstract
High rates of anxiety and depression are reported among youth with autism spectrum disorders. These conditions are generally assessed using measures validated for typically developing youth. Few studies have investigated their validity for autism spectrum disorders, which is crucial for accurate assessment and the provision of proper treatment. The Revised Children’s Anxiety and Depression Scale was evaluated with 67 youth with autism spectrum disorders to examine its utility in measuring anxiety and depression in this population. Parents and children (aged 11–15 years) referred to a multisite intervention study completed the Pediatric Anxiety Rating Scale, Multidimensional Anxiety Scale for Children, Anxiety Disorders Interview Schedule, Child Behavior Checklist, and Revised Children’s Anxiety and Depression Scale. Results suggest acceptable internal consistency of the Revised Children’s Anxiety and Depression Scale. Modest convergent validity was found among the Revised Children’s Anxiety and Depression Scale and other standardized measures of anxiety and depression. There were stronger correlations between Revised Children’s Anxiety and Depression Scale Total scores and subscales of measures expected to correlate significantly than those not expected to correlate. One exception was a significant association between the Revised Children’s Anxiety and Depression Scale and Child Behavior Checklist Attention subscale, calling into question the divergent validity in separating anxiety from attention problems. Overall, results suggest preliminary support for the Revised Children’s Anxiety and Depression Scale in youth with high-functioning autism spectrum disorders.
Keywords
Introduction
In recent years, focus on coexisting psychiatric symptoms among individuals with autism spectrum disorders (ASD) has intensified. Approximately 74% of youth with ASD have at least one comorbid psychiatric disorder (e.g. Mattila et al., 2010).
Anxiety and depression are particularly prevalent among individuals with ASD. According to the Anxiety Disorders section of the Diagnostic Interview Schedule for Children (DISC; Muris et al., 2008), 84% of 44 children with ASD met criteria for an anxiety disorder. Using a modified version of the K-SADS, Leyfer et al. (2006) developed and piloted the Autism Comorbidity Interview–Present and Lifetime Version (ACI-PL), yielding depression rates of 10%–24% among children with autism (Leyfer et al., 2006). Other prevalence estimates have yielded rates as high as 70% in samples of adults with ASD (Lugnegård et al., 2011). Importantly, these rates are often derived using standardized assessments for typically developing individuals and must be interpreted with caution.
Given the potential negative impact of coexisting psychiatric symptoms, including increased functional impairment, timely and accurate identification of comorbid conditions is imperative. Moreover, there are promising interventions for associated symptoms in ASD; however, the lack of validated assessment tools has made it difficult to accurately assess magnitude of comorbid anxiety and depression and quantitatively assess response to treatment. Lack of validated measures of associated symptoms represents a gap in the field. As such, it remains unclear whether the measures currently used accurately identify depression and anxiety in this population.
The current study sought to address the gap in the literature by providing a preliminary assessment of the convergent and divergent validity of one promising measure of anxiety and depression for youth with ASD, the Revised Children’s Anxiety and Depression Scale (RCADS; Chorpita et al., 2005). The RCADS has yielded good convergent and discriminant validity with independent measures of anxiety and depression in clinical samples of youth, providing support for its use as a measure of depression and anxiety for children and adolescents. Given its strong psychometric properties, the RCADS holds promise for accurate assessment of these symptoms in youth with ASD.
Methods
Participants
Participants were 67 youth aged between 11 and 15 years (M =12.25 years, standard deviation (SD) = 1.15 years) with an ASD (autistic disorder: 68.3%, Asperger’s syndrome: 18.3%, pervasive developmental disorder—not otherwise specified: 13.3%) who also met criteria for an anxiety disorder. The sample consisted of 71.4% White, 9.5% Latino, 6.3% Asian American, 3.2% African American, and 9.5% other/mixed participants.
Procedure
Data were collected as part of a multisite (University of California, Los Angeles and University of South Florida) study examining the efficacy of cognitive behavioral therapy (CBT) to treat anxiety in adolescents with high-functioning ASD (see Ehrenreich-May et al., in press, for detailed description of CBT study procedures). Procedures were approved by the institutional review boards for human subject research at both study sites. Youth from Institution 1 were administered the Wechsler Intelligence Scale for Children, Fourth Edition (WISC-IV) at intake (full-scale M = 87.58, SD = 17.79, range = 57–138). For Institution 2, an intelligence quotient (IQ) assessment was administered within the past 3 years verifying a full-scale IQ of 85 or higher. Diagnosis of an ASD was confirmed using the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2002) and the Autism Diagnostic Interview–Revised (ADI-R; Lord et al., 1994). All participants met criteria for a principal anxiety disorder per the Anxiety Disorders Interview Schedule–Child/Parent (ADIS-C/P; Silverman and Albano, 1996).
Validity measures
RCADS
The RCADS (Chorpita et al., 2005) is a self-report measure of anxiety and depression for children aged 6–18 years, with sound psychometrics. It is composed of 47 items corresponding to 6 subscales: Major Depressive Disorder (MDD; 10 items), Panic Disorder (PD; 9 items), Social Phobia (SoP; 9 items), Separation Anxiety Disorder (SAD; 7 items), Generalized Anxiety Disorder (GAD; 6 items), and Obsessive–Compulsive Disorder (OCD; 6 items). Participants answer questions using a 4-point Likert scale from 0 (“never”) to 3 (“always”). The RCADS yields two summary scores: total anxiety (composed of the five anxiety subscales) and total internalizing (composed of all six subscales). For the current study, raw scores from the six subscales and two total scales were used.
ADIS-C/P
The ADIS-IV-C/P (Silverman and Albano, 1996) is a clinician-administered, semistructured interview assessing for the presence and severity of anxiety disorders. Clinical Severity Rating (CSR) scores ranging from 0 (“none”) to 8 (“very severely disturbing/impairing”) are generated for each anxiety disorder (SAD, SoP, GAD, OCD, and Specific Phobia (SP)), with a score of 4 or greater being clinically significant. The current study used each participant’s highest anxiety diagnosis CSR score, the number of clinically significant anxiety disorders, and CSR scores for each disorder.
Multidimensional Anxiety Scale for Children–Parent
The Multidimensional Anxiety Scale for Children–Parent (MASC-P; March, 1998) is a standardized 39-item parent-report index of anxiety in youth. The current study used the raw score and anxiety disorder totals, as well as the physical symptoms, harm avoidance, social anxiety, and separation/panic subscales.
Pediatric Anxiety Rating Scale
The Pediatric Anxiety Rating Scale (PARS; Research Units on Pediatric Psychopharmacology Anxiety Study Group (RUPP), 2002) is a clinician-rated scale assessing anxiety symptoms and the associated severity and impairment in children over the past week. It consists of 50 questions and 7 severity/impairment items. For the current study, scoring consisted of the clinician summary items and the 5-item score summary (composed of the clinician’s ratings of overall severity of anxiety feeling, overall severity of physical symptoms of anxiety, overall avoidance of anxiety-provoking situations, severity interference with family relationships, and severity interference with peer and adult relationships).
Child Behavior Checklist
The Child Behavior Checklist (CBCL; Achenbach, 2001) is a 118-item parent-report scale that assesses specific behavioral and emotional problems for youth aged 6–18 years. Raw CBCL subscale scores were reported in the current study.
ADOS
The ADOS (Lord et al., 2002) is a semistructured assessment conducted with the child and used to evaluate symptoms of autism. The ADOS severity score, derived from the social and communication domains, was utilized to evaluate divergent validity with the RCADS.
Results
Descriptive statistics
The mean score for the ADOS social and communication domains was 10.81 (SD = 3.7). Diagnosis of a principal anxiety disorder was made based on the ADIS-C/P. The most common type of anxiety was SoP (92.1%). The next most common was GAD (74.6%), followed by SP (44.4%) and OCD (44.4%), and SAD (36.5%).
Descriptive statistics for the main validity measure, the RCADS, are as follows: Total Anxiety Score M = 27.75, SD = 16.11; Total Internalizing Score M = 35.14, SD = 19.58; SoP M = 4.57, SD = 4.69; PD M = 7.92, SD = 5.06; MDD M = 3.49, SD = 2.99; GAD M = 5.17, SD = 3.32; OCD M = 6.22, SD = 3.95. The RCADS Total Anxiety and Total Internalizing Scores were significantly correlated (r = 0.979, p < 0.001). Cronbach’s alpha for the RCADS ranges from 0.72 to 0.93.
Validity
RCADS total scores: convergent validity
To measure concurrent validity of the RCADS Total Anxiety Score and Total Internalizing Score, correlations were conducted with total scores on the ADIS, MASC, PARS, and CBCL. Six of the 32 correlations of Total RCADS scores corresponded significantly with total scores on other measures (see Table 1 for r values).
Convergent and divergent validity: correlations among RCADS total anxiety scores and scores from the ADIS, MASC-P, PARS, and CBCL.
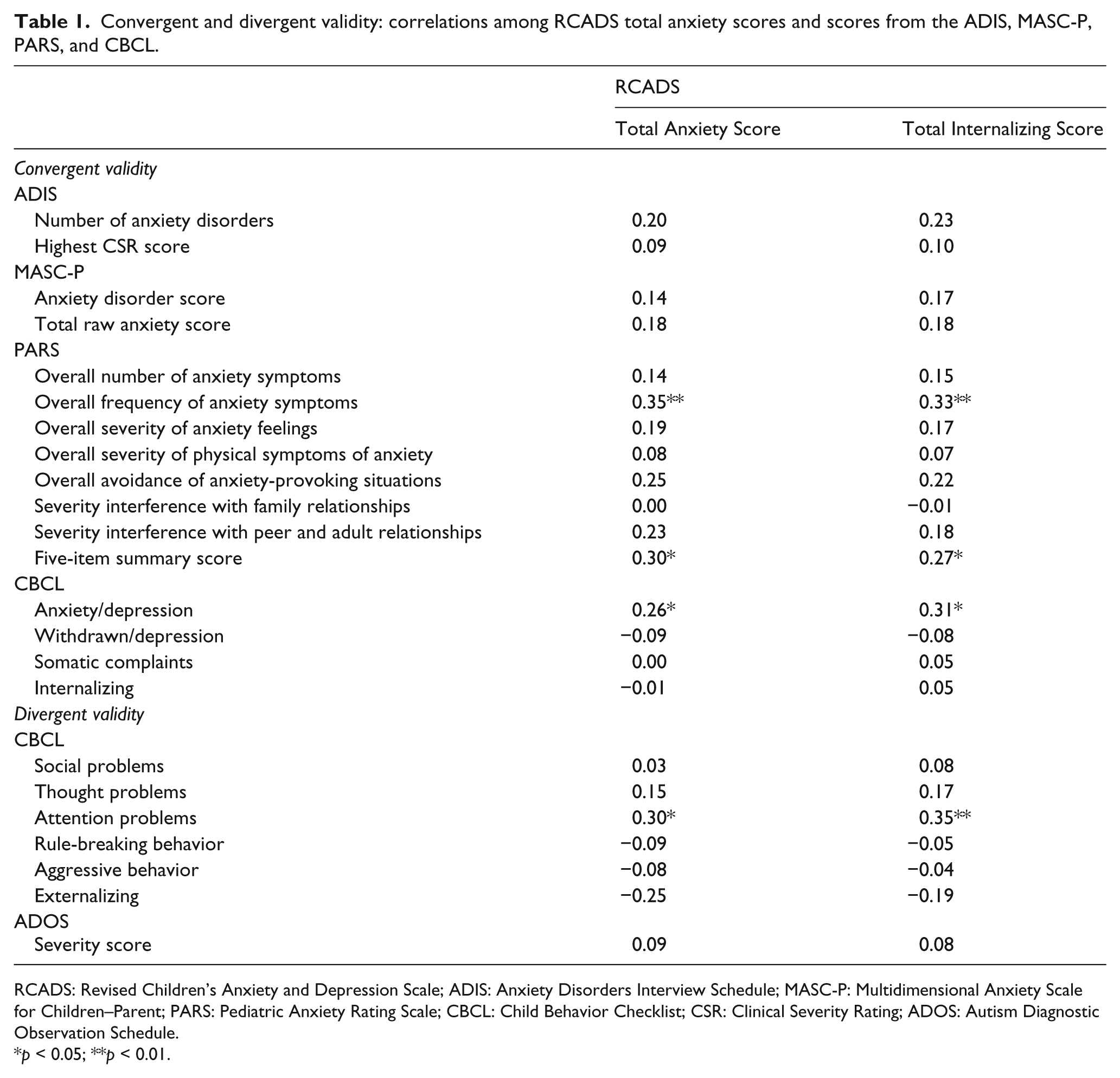
RCADS: Revised Children’s Anxiety and Depression Scale; ADIS: Anxiety Disorders Interview Schedule; MASC-P: Multidimensional Anxiety Scale for Children–Parent; PARS: Pediatric Anxiety Rating Scale; CBCL: Child Behavior Checklist; CSR: Clinical Severity Rating; ADOS: Autism Diagnostic Observation Schedule.
p < 0.05; **p < 0.01.
RCADS total scores: divergent validity
Correlations were examined between RCADS Total scores and subscales of the CBCL and ADOS that were not expected to be related (e.g. CBCL Social Problems, Thought Problems, Attention Problems, Rule-Breaking Behavior, Aggressive Behavior, and Externalizing) to determine divergent validity. None of the relationships were significant, with the exception of the Attention Problems subscale of the CBCL correlating significantly with RCADS Total Anxiety Score and RCADS Total Internalizing Score (see Table 1).
RCADS subscale scores: convergent validity
Pearson correlations were also used to examine concurrent validity of the RCADS subscales with CSRs from the ADIS and subscales of the MASC-P. Of 24 relationships examined, 5 subscales of the RCADS correlated significantly with diagnostic severity scores from the ADIS; one correlation was significant between subscales of the RCADS and MASC-P. These results are presented in Table 2.
Correlations among RCADS subscales and ADIS/MASC subscales.
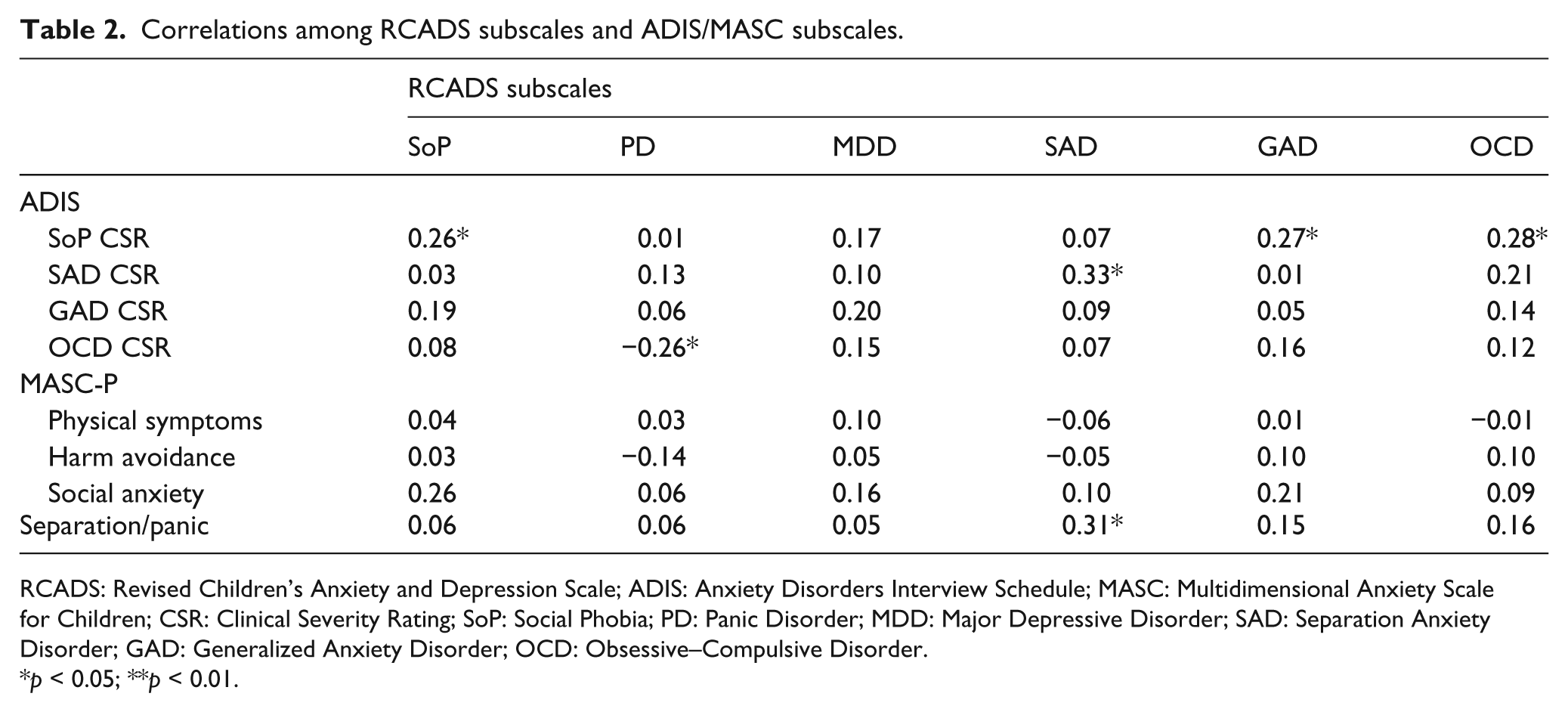
RCADS: Revised Children’s Anxiety and Depression Scale; ADIS: Anxiety Disorders Interview Schedule; MASC: Multidimensional Anxiety Scale for Children; CSR: Clinical Severity Rating; SoP: Social Phobia; PD: Panic Disorder; MDD: Major Depressive Disorder; SAD: Separation Anxiety Disorder; GAD: Generalized Anxiety Disorder; OCD: Obsessive–Compulsive Disorder.
p < 0.05; **p < 0.01.
Discussion
Results indicated acceptable internal consistency for the RCADS in youth with high-functioning ASD, with modest convergence between RCADS total scores and the PARS total scores as well as the CBCL Anxious/Depressed subscale; and a specific relation between RCADS SAD subscale and ADIS SAD severity scores. Moreover, there were mostly stronger correlations between domains expected to correlate than those that were not expected to correlate. However, the correlation between RCADS total and the CBCL Attention subscale calls into question divergent validity in separating anxiety from attention problems on the RCADS. Taken together, results suggest that the RCADS could have utility in this population, but more convincing evidence is needed.
In this early adolescent sample of youth with ASD, the RCADS exhibited good internal consistency, suggesting that response patterns to items measuring similar constructs within the RCADS were similar. This is an encouraging finding and may reflect the ability of older youth to reliably interpret and answer items pertaining to their emotional state.
Findings from the total score comparisons suggest modest potential. Total scores on the RCADS correlate with PARS total scores and with the CBCL Anxiety/Depression Scale, albeit to a modest degree. In the context of research on the youth–parent agreement on the CBCL and other symptom measures showing an average level of correlation of around 0.25 (Achenbach et al., 1987), these findings are comparable and suggest that parent–child convergence is no worse at the total score level than it is in general clinical child and adolescent samples. At the subscale level, there was less adequate convergence; only ratings of separation anxiety showed statistically significant convergence among raters.
Some evidence of divergent validity emerged, with a key exception: correlations with the CBCL Attention subscale of the same magnitude as all of the convergent validity correlations. This was an unexpected finding; however, less ability to focus attention has previously been associated with higher levels of anxiety in children and adults (e.g. Reinholdt et al., 2012), perhaps because attention, a key aspect of executive functioning, helps regulate emotional impulses.
The low-to-moderate agreement between informants is an inherent limitation of the current study, rendering interpretation of associations between the RCADS and clinician-reported (e.g. ADIS) or parent-reported (e.g. CBCL) measures challenging. The low concordance between child- and parent-report may be driven by youth underreporting their own symptoms, despite being part of a treatment-referred group and clearly exhibiting symptoms based on parent interview (see Ehrenreich-May et al., in press).
Given its modest evidence for validity, the RCADS could potentially be a useful tool for self-report of anxiety and possibly depression among youth with ASD. However, a major challenge in the development and validation of self-report measures of internalizing symptoms in ASD is the respondent’s potential limitation in self-awareness and emotion recognition. Although caregivers may not have access to the internal emotional distress of their children, they often seek appropriate treatment to target these symptoms, suggesting they have a fair amount of insight into their child’s challenges. Alternatively, depression and anxiety may manifest differently in youth with ASD than in typically developing youth, making it more challenging for clinicians and parents to accurately interpret manifest behavior and detect coexisting psychopathology.
In sum, results suggest that the RCADS may be useful in detecting anxiety and depression in youth with ASD, although further investigation is required, perhaps with larger samples. The good internal consistency of the RCADS is encouraging and suggests youth with ASD reliably answer questions probing their experiences related to anxiety and depression. However, results should be considered preliminary given that only a subset of correlations are significant, with rs ranging from 0.26 to 0.33. Although these correlations appear somewhat low, they are within the range typically reported within the child psychopathology literature (Achenbach et al., 1987). Nonetheless, we acknowledge that the low values commonly reported in the literature reflect a concern regarding the validity of existing measures of child psychopathology. The modest correlations presented in this study suggest measures like the RCADS may be used to provide preliminary estimates of depression and anxiety among youth with ASD. However, clearly, there is also a need for ASD-specific measures of psychopathology.
Footnotes
Funding
1/3 CBT for Anxiety Disorders in Autism: Adapting Treatment for Adolescents Study P.I. / Site P.I.: Jeffrey Wood Agency: National Institute of Child Health and Human Development Type: R34 (HD65270-01, Year 01).