
Abstract
Autism is a lifelong neurodevelopmental disorder, with a known impact on quality of life. Yet the developmental trajectory of quality of life is not well understood. First, the effect of age on quality of life was studied with a meta-analysis. Our meta-analysis included 10 studies (published between 2004 and 2012) with a combined sample size of 486 people with autism and 17,776 controls. Second, as there were no studies on quality of life of the elderly with autism, we conducted an empirical study on quality of life of the elderly (age range 53–83) with autism (N = 24) and without autism (N = 24). The meta-analysis showed that quality of life is lower for people with autism compared to people without autism, and that the mean effect is large (Cohen’s d = −0.96). Age did not have an effect on quality of life. The study concerning the elderly with autism showed that the difference in quality of life is similar in the elderly. Age, IQ and symptom severity did not predict quality of life in this sample. Across the lifespan, people with autism experience a much lower quality of life compared to people without autism. Hence, the quality of life seemed to be independent of someone’s age.
Introduction
Autism 1 is a lifelong neurodevelopmental disorder, yet the developmental trajectory of people with autism is not well understood. A minority of adults with autism, although continuing to be affected by their autism, can find work, live independently and develop meaningful relationships with others. However, the majority have an overall poor outcome (Billstedt et al., 2005). They remain dependent on their parents or others, are either unemployed or underemployed and lead fairly isolated lives (Howlin et al., 2004, 2013). Moreover, a large number of adults with autism remain without appropriate services and effective interventions (Barnard et al., 2001; Gerhardt and Lainer, 2011). Consequently, many parents of children with autism do not know what to expect for the future of their children. They worry about what will happen to their children when they are not around to care for them anymore, and they fear that the adult services are not as good as those for children (Eaves and Ho, 2008). These factors combined highlight a growing need to describe the developmental trajectory of people with autism, so that the appropriate steps in provision of care can be taken.
The majority of research on outcomes in autism has focused on one or a few domains (e.g. work, friendships) or only on objective measures (e.g. employment status, but not employment satisfaction). Quality of life (QoL) is a more comprehensive, multidimensional concept that includes subjective well-being, and is well suited to assess people with autism (Burgess and Gutstein, 2007). The World Health Organization (WHO, 1995) defines QoL as the individual’s perception of his or her position in life in the context of the culture and value system, and in relation to one’s goals, expectations, standards and concerns. It incorporates the individual’s physical health, psychological state, level of independence, social relationships, personal beliefs and his or her relationship to salient features of the environment in a complex way. Therefore, the first goal of this study is to investigate the QoL of people with autism.
Previous research on unidimensional outcome measures suggests that one of the predictors contributing to better adult outcomes are less severe autism symptoms (Eaves and Ho, 2008; Kuhlthau et al., 2010). Autism symptoms seem to show modest improvement with age (Esbensen et al., 2009; Happé and Charlton, 2012). Age also has an effect on other aspects of autism, as older people have shown fewer sensory abnormalities (Kern et al., 2006) and less maladaptive behaviour (Shattuck et al., 2007) than younger people with autism. However, not all individuals improve. Some people reach a plateau in their development, and others decline (McGovern and Sigman, 2005). In addition, while some symptoms show modest improvements, this seldom leads to functioning in the normal range, which reinforces the notion that autism is a lifelong condition (Seltzer et al., 2004). Therefore, the second goal of this study is to assess the effect of age on QoL.
To our knowledge, there is currently no quantitative review of QoL in autism, but there are two qualitative reviews of QoL in autism by the same authors: Kamp-Becker et al. (2010) – 7 studies, and Kamp-Becker et al. (2011) – 9 studies, of which 5 studies overlap with those of the 2010 paper. The authors did not draw a general conclusion across studies, as between studies there was a wide variety in patient population, design, treatments and outcome measures. However, most studies show that QoL is relatively low in people with autism. Moreover, the effect of age was not studied, despite reports that in the general population QoL decreases with age (StatLine, 2010). Therefore, a direct comparison between the QoL of people with autism and people without autism is needed in order to control for the effects of aging on QoL found in the general population.
In this study, we investigate how the QoL of people with autism can be described over the entire lifespan. In Study 1, we will examine QoL quantitatively by performing a meta-analysis on QoL studies. We will describe the magnitude of the difference between QoL of people (i.e. children, adolescents and adults) with and without autism. As elderly people with autism are likely to be underrepresented in the existing studies (Mukaetova-Ladinska et al., 2012), we conducted Study 2, which will focus on QoL among the elderly with autism. In both studies, we explore the effect of age as well as other factors that influence QoL.
We hypothesize that independent of age, QoL will be lower for people with autism than for people without autism. Although there will be individual differences in people’s life trajectory (Seltzer et al., 2004), we hypothesize that age plays a role in QoL, because autism symptoms often reduce with age. As people might learn to compensate, accept impairments and follow successful treatment (García-Villamisar et al., 2002), QoL could improve with age. However, a contrasting hypothesis would be that QoL will decrease with age. Age brings about increased responsibilities and decreased parental support, which may cause impairments to be perceived more intensively in adulthood than in childhood. There may even be an accumulative impact of autism impairments on finances, health and social life, as was found for attention deficit hyperactivity disorder (ADHD) impairments (Bernardi et al., 2012; Brod et al., 2012). For these reasons, we will explore the direction of the hypothesized age effect.
Methods study 1: quantitative review
Literature search
The databases PubMed, PsycINFO and Web of Knowledge were searched for studies (including theses and dissertations) that focus on QoL in autism (up to January 2013). Search terms relating to autism (e.g. autism, autism spectrum disorder (ASD), Asperger, pervasive developmental disorder–not otherwise specified (PDD-NOS) were combined with QoL and measures of QoL (e.g. quality of life, health-related QoL (HRQOL), World Health Organization Quality of Life-Brief (WHOQOL), PedsQL). We did not search unpublished work by authors, but cross-references of the obtained studies were checked for studies that might have been missed in the electronic search.
Inclusion criteria
The inclusion criteria were that a study: (a) concerned participants that were diagnosed with autism by clinical consensus (usually verified with standardized instruments); (b) included a self-report or proxy-report measure of QoL; (c) used a standardized, valid and reliable measure of QoL; and (d) addressed a comparison between groups with and without autism. Studies concerning people with autism and a co-morbid disorder were included, as this would increase generalizability.
Obtained studies
The literature search generated 3231 hits; based on titles and abstracts, 42 studies were selected. After full text screening, 28 out of the 42 studies did not meet inclusion criteria. Reasons for excluding studies were that the autism diagnosis was not validated (N = 3), the studies used a non-standardized QoL measure (N = 5), no control group was included (N = 17) or a different type of QoL (family QoL, communication QoL) was assessed (N = 3). Of the 14 studies that met inclusion criteria, 9 studies did not include all of the necessary information; authors were contacted and 5 provided the requested information. This resulted in 10 studies available for the meta-analysis, with 486 participants with autism and 17,776 participants without autism (Table 1). The large number of control participants is mainly due to the use of normative comparison groups. All the information in Table 1 was recorded by the first author and verified by the second author.
Main characteristics of the studies included in the meta-analysis.
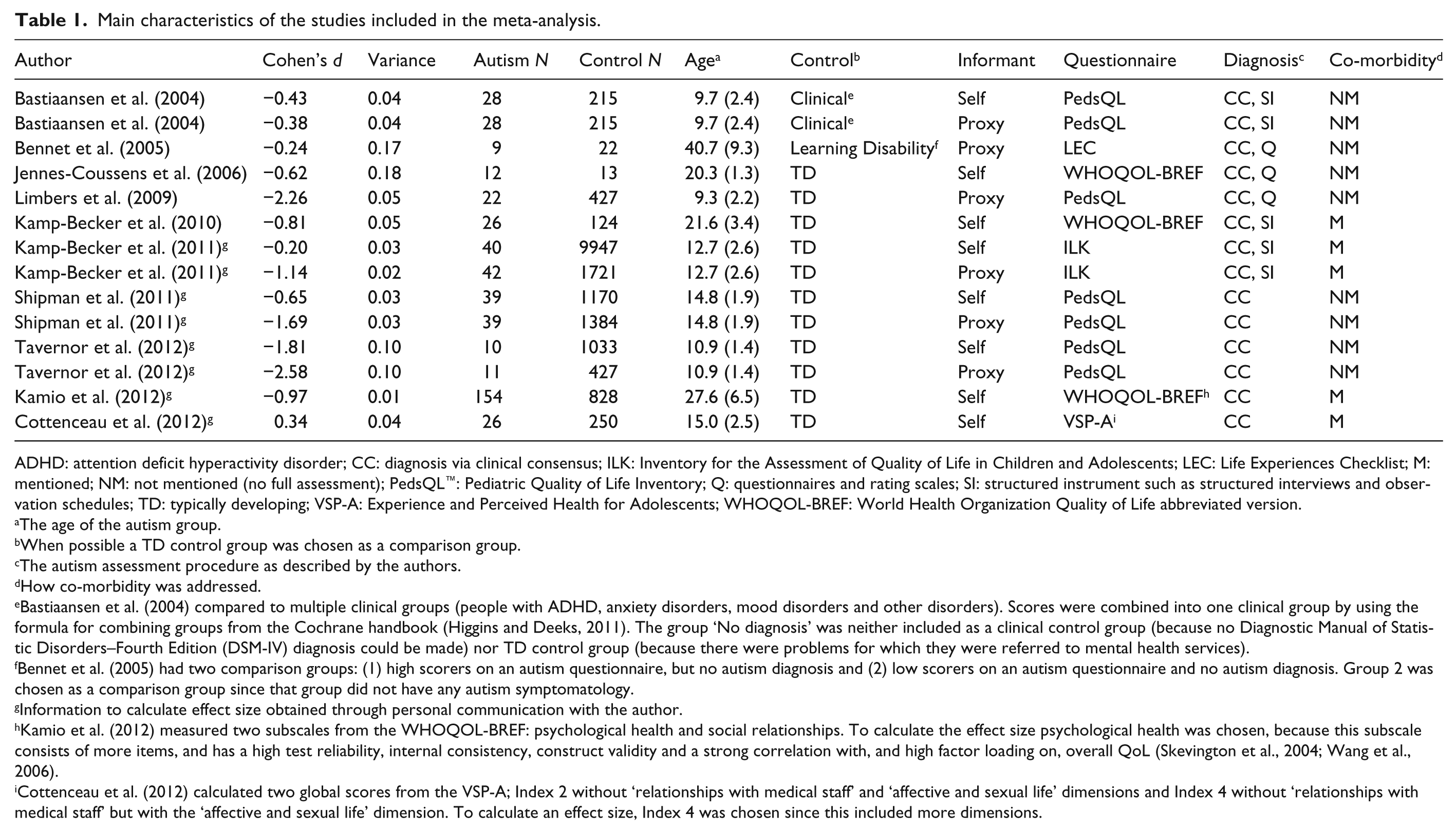
ADHD: attention deficit hyperactivity disorder; CC: diagnosis via clinical consensus; ILK: Inventory for the Assessment of Quality of Life in Children and Adolescents; LEC: Life Experiences Checklist; M: mentioned; NM: not mentioned (no full assessment); PedsQL™: Pediatric Quality of Life Inventory; Q: questionnaires and rating scales; SI: structured instrument such as structured interviews and observation schedules; TD: typically developing; VSP-A: Experience and Perceived Health for Adolescents; WHOQOL-BREF: World Health Organization Quality of Life abbreviated version.
The age of the autism group.
When possible a TD control group was chosen as a comparison group.
The autism assessment procedure as described by the authors.
How co-morbidity was addressed.
Bastiaansen et al. (2004) compared to multiple clinical groups (people with ADHD, anxiety disorders, mood disorders and other disorders). Scores were combined into one clinical group by using the formula for combining groups from the Cochrane handbook (Higgins and Deeks, 2011). The group ‘No diagnosis’ was neither included as a clinical control group (because no Diagnostic Manual of Statistic Disorders–Fourth Edition (DSM-IV) diagnosis could be made) nor TD control group (because there were problems for which they were referred to mental health services).
Bennet et al. (2005) had two comparison groups: (1) high scorers on an autism questionnaire, but no autism diagnosis and (2) low scorers on an autism questionnaire and no autism diagnosis. Group 2 was chosen as a comparison group since that group did not have any autism symptomatology.
Information to calculate effect size obtained through personal communication with the author.
Kamio et al. (2012) measured two subscales from the WHOQOL-BREF: psychological health and social relationships. To calculate the effect size psychological health was chosen, because this subscale consists of more items, and has a high test reliability, internal consistency, construct validity and a strong correlation with, and high factor loading on, overall QoL (Skevington et al., 2004; Wang et al., 2006).
Cottenceau et al. (2012) calculated two global scores from the VSP-A; Index 2 without ‘relationships with medical staff’ and ‘affective and sexual life’ dimensions and Index 4 without ‘relationships with medical staff’ but with the ‘affective and sexual life’ dimension. To calculate an effect size, Index 4 was chosen since this included more dimensions.
Independent variables
For each study, the age of the autism participants was coded as a continuous variable. The following categorical variables were also coded: the respondent to the QoL questionnaire (self-report or proxy-report), the comparison group (typically developing (TD) or clinical control group) and the QoL questionnaire utilized (WHOQOL-BREF, Pediatric Quality of Life Inventory (PedsQL) or other). The study characteristics served as the independent variables in order to determine whether these characteristics moderated the effect size.
Dependent variable
The QoL questionnaires generated continuous outcomes, for which a standardized mean difference (Cohen’s d) was calculated. This effect size is widely used, is easily interpretable and can be calculated from t-test statistics (Thalheimer and Cook, 2002; Turner and Bernard, 2006).
Data analyses
The data were analysed using the Metafor package for R (Viechtbauer, 2010). A random effects meta-analysis was performed to provide an average effect for the population of studies, as the included studies were assumed to be a random selection of the entire study population. We conducted a mixed effects meta-analysis to determine the moderating effects of the study characteristics. Effect sizes were regressed on the study characteristics in a restricted maximum likelihood meta-regression (Viechtbauer, 2010).
We tested the heterogeneity with conventional Q tests and with the I2 statistic. The I2 statistic estimates how much of the total variability in the effect size estimates (composed of heterogeneity and sampling variability) can be attributed to heterogeneity among the true effects. We checked for publication bias with funnel plots and the fail-safe analysis (Rosenthal, 1979).
Results study 1
Overall result
Based on our qualitative analysis, there were many differences in QoL between people with and without autism. The most affected domain of QoL seemed to be social functioning (Bastiaansen et al., 2004; Jennes-Coussens et al., 2006; Kamio et al., 2012; Kamp-Becker et al., 2010). Other relevant reported findings were that the autism group had fewer friends and more special education (Bastiaansen et al., 2004); lower physical health (Jennes-Coussens et al., 2006); lower QoL relating to relationships with friends, leisure, affective and sexual relationships; and placed less importance on activities with peers and more importance on activities with parents (Cottenceau et al., 2012).
Our quantitative analysis showed that the mean effect size is large, d = −0.96; 95% confidence interval = −1.39, −0.52; range = −2.58 to 0.34 (Figure 1). People with autism had a lower QoL than people without autism, z = −4.29, p < 0.001. There was significant heterogeneity between the effect sizes, τ2 = 0.63, Q(13) = 168.80, p < 0.001, I2 = 94.6%. Leave-one-out sensitivity analyses indicated that the effect remained significant regardless of which study was dropped (Cohen’s d ranged from −1.06 to −0.84, all p < 0.001). A QQ-plot confirms that there is a normal distribution of effect sizes.

Forest plot of the standardized mean difference (Cohen’s d) and 95% confidence interval of QoL. Negative effect sizes imply that the QoL is lower in people with autism as compared to controls while positive effect sizes suggest the opposite pattern.
Visual inspection and a regression test for funnel plot asymmetry indicated no asymmetry in the funnel plot (z = −0.40, p = 0.696; Figure 2). As the number of effect sizes is 14, the fail-safe N should be greater than 14 × 5 + 10 = 80, that is, the fail-safe N = 1544. Thus, there is no indication of publication bias.
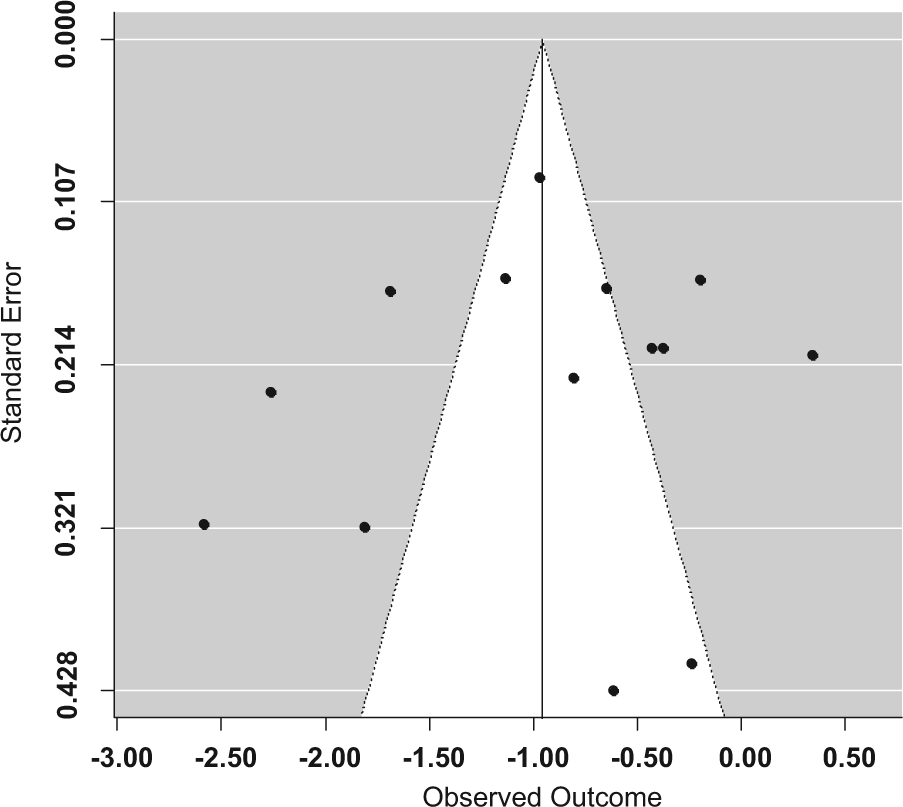
Funnel plot of effect sizes (Cohen’s d) against the standard errors. The dots represent the studies included in the analysis.
Moderator analysis
At least part of the heterogeneity in the model may be due to the influence of moderators. First, age was added into the model but this did not have a moderating effect, p = 0.265. Second, we added control group, questionnaire and respondent to the model to explore whether these would moderate the effect size. The omnibus test was significant, QM (5) = 28.46, p < 0.001, and the three moderators were significant (control group, p = 0.002; questionnaire, p = 0.005; respondent, p = 0.004). The estimated amount of residual heterogeneity was equal to τ2 = 0.19, suggesting that (0.63-0.19)/0.63 = 69.8% of the total heterogeneity could be accounted for by the included moderators. There was still a significant amount of residual heterogeneity, QE(8) = 37.44, p < 0.001, indicating that study characteristics not considered in the model also moderate the effect size.
Further inspection of the moderators with univariate analyses revealed that there was no significant difference in effect size between studies that compared people with autism to a TD or clinical group (p = 0.153). There was no difference in effect size between studies that used the WHOQOL-BREF questionnaire and those that used the PedsQL, p = 0.446. Studies concerning a self-report (d = −0.63, p = 0.018) and studies concerning a proxy-report (d = −1.39, p < 0.001) both showed a difference in QoL between people with and without autism. The difference between these two estimates approached significance, z = −1.87, p = 0.062, indicating that a larger difference in effect size with a proxy informant as compared to self-reports made by people with autism. As five of the six studies that included a proxy informant had young participants (aged 9.3–14.8 years old), we tested for an interaction between age and respondent, but this was not significant. Hence, the moderator analyses suggest that when taken together, control group, questionnaire and respondent moderate the effect size, but only the respondent is a marginal moderator when other moderators are not considered.
Discussion study 1
The meta-analysis shows a large difference in QoL between people with and without autism. Age does not have a moderating effect, which might be due to the mean age (range 9.3–40.7) of the participants; the elderly with autism were underrepresented in the meta-analysis.
Studies that assess QoL with different types of questionnaires do not produce different results, which indicates a high comparability between the various QoL measures. Studies that compared to either a TD or a clinical control group do not produce different results; however, only three studies included a clinical control group.
The informant was found to be the only factor that may influence QoL. Parents rate the QoL of their children with autism lower than the children themselves do (Bastiaansen et al., 2004; Kamp-Becker et al., 2011). There may be several reasons for this discrepancy. First, parents of children with health concerns generally report a lower QoL than children themselves (Upton et al., 2008), and there is a greater agreement for observable (e.g. physical) functioning than for non-observable (e.g. emotional or social QoL) functioning (Eiser and Morse, 2001). Since social impairments form a substantial part of the autism symptomatology, this may explain the discrepancy between self- and proxy-report. Second, the discrepancy may be due to the difficulties that people with autism have when reporting on their own QoL. They may have a deficit in self-representation that affects the identification of emotional states in others as well as in themselves (Johnson et al., 2009; Lombardo et al., 2007). In addition, they may lack the emotional vocabulary, which could affect their ability to respond to items about their mood and feelings (Tavernor et al., 2012). However, this is debatable as it has been reported that self-reports of QoL from children with autism are valid and reliable (Shipman et al., 2011), and that children with autism have sufficient ability to rate their emotions appropriately (Hobson et al., 2006). Third, children may perceive their limited social and emotional functioning as a less severe problem, as compared to their parents. This is illustrated by a quote of a parent: ‘I answered the question producing negative scores, but upon reflection I think my child actually prefers being alone’ (Tavernor et al., 2012). Therefore, the discrepancy between parent- and self-report seems to be derived from a perceptual difference concerning children’s activities and appraisals, and not from a lack of parental knowledge. When parents are asked to respond as they think their child would, the correlation with self-report increases (Sheldrick et al., 2012). In conclusion, disagreement between parent’s and children’s reports of QoL is, in itself, unlikely to indicate that either is wrong or right, but rather is a consequence of each individual’s beliefs about the child’s health and well-being. Parent-reports, as an addition to self-reports, can provide another perspective, and thus, produce a greater understanding of QoL in autism.
Study 2: new data on QoL in the elderly with autism
One shortcoming observed in the meta-analysis was the lack of studies that assessed QoL in elderly with autism. Therefore, in Study 2 we conducted an empirical study in order to focus on QoL in the elderly with autism. Moreover, there was a large amount of unexplained heterogeneity in the meta-analysis even after including several potentially important moderators (control group, questionnaire and informant). Unfortunately, information regarding the participants’ symptom severity (Eaves and Ho, 2008; Kuhlthau et al., 2010), IQ (Howlin et al., 2004; McGovern and Sigman, 2005) and early language development (Billstedt et al., 2005; Szatmari et al., 2003) were too sparse to include in the meta-analysis, while these participant characteristics are relevant predictors of adult outcome. Hence, in Study 2 we assessed symptom severity and intelligence in relation to QoL. Moreover, two more moderators of QoL were explored. First, we know that QoL is affected in early stages of cognitive decline (Bárrios et al., 2013); therefore, we investigated whether regular cognitive mistakes influence QoL in the elderly with autism. Second, we explored whether psychological problems related to psychopathology also influence QoL of the elderly with autism because psychological health is an important part of QoL (WHO, 1995) and co-morbid psychopathology is common among people with autism (Geurts and Jansen, 2012).
Methods Study 2
Participants
The autism group consists of intellectually able elderly with autism (N = 24), who were diagnosed with autism in their adult life. Individuals were included if they had received a diagnosis of autism via clinical consensus, had a high score (≥60) on the Social Responsiveness Scale Adult version (SRS-A; Noens et al., 2012) or if they met both criteria. Most of the participants were included in a previously published study on cognitive functioning in the elderly with autism (Geurts and Vissers, 2012). We included one additional participant who filled out the QoL questionnaire but who was not tested for the original study.
TD controls (N = 24) were included if they did not have autism (based on self-report and SRS-A scores < 60) or any other psychiatric disorder, and did not have any relatives diagnosed with autism. For more details about the participants, see Table 2.
Group means and standard deviations for age, gender, estimated IQ and Social Responsiveness Scale Adult version score.
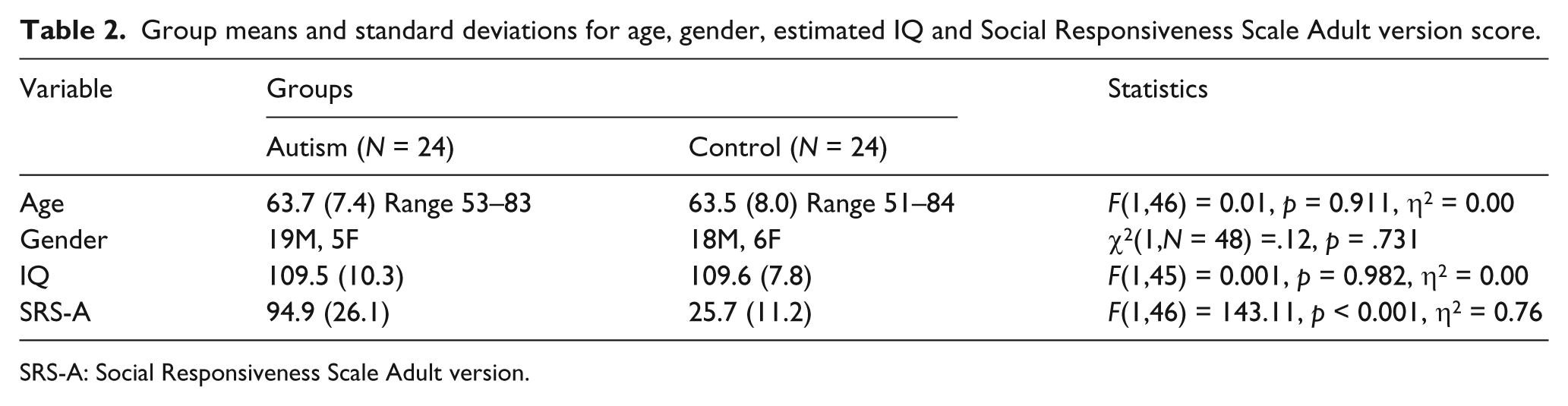
SRS-A: Social Responsiveness Scale Adult version.
Materials
Quality of life
There is currently no instrument available to measure QoL specifically in people with autism. A benefit of a generic measure of QoL, such as the RAND-36 (Van der Zee and Sanderman, 1993), is that it is easier to compare across groups of people. The RAND-36 (also known as SF-36) is a brief and comprehensive 36-item self-report health-related QoL questionnaire. It includes eight of the most frequently measured health concepts: physical functioning, role limitations caused by physical health problems, role limitations caused by emotional problems, social functioning, emotional well-being, energy/fatigue, pain and general health perceptions (Ware, 2000). The Dutch manual of the RAND-36 (Van der Zee and Sanderman, 1993) was used to calculate the total scores. The total score is the mean of the aforementioned eight scale scores. A higher score indicates a better QoL. Van der Zee and Sanderman (1993) conclude that the RAND-36 is a valid, reliable and sensitive measurement of QoL. Internal consistency for each of the scale scores range between α = 0.71 and 0.92 (mean is 0.84).
Verbal intelligence
The Dutch Adult Reading Test (DART; Schmand et al., 1992) is a list of 50 words with irregular spelling that are to be read aloud. The number of correctly pronounced words was used to calculate a DART-IQ score. It is relatively insensitive to cognitive impairment caused by neurological disorders and is a strong predictor of intelligence (Schmand et al., 1998). The psychometric properties are excellent as the interrater reliability is 0.96 and the internal consistency is 0.91 (Schmand et al., 1992).
Symptom severity
The SRS-A (Noens et al., 2012) is a 64-item self-report rating scale that serves as an index of severity of deficits in the autism spectrum. Five domains were assessed: social awareness, social information processing, capacity for reciprocal social communication, social anxiety/avoidance and autistic preoccupations and mannerisms. This scale has excellent internal consistency, α = 0.94–0.95 (Constantino and Todd, 2005).
Psychological problems
The symptom checklist (SCL-90; Arrindell and Ettema, 1986) is a widely used multidimensional 90-item self-report symptom inventory that screens for a broad range of psychological problems. Subscales are anxiety, agoraphobia, depression, somatisation, insufficiency of thought and behaviour, distrust and interpersonal sensitivity, hostility and sleeping problems. The SCL-90 has good test–retest reliability, internal consistency and concurrent and discriminant validity (Derogatis, 1977).
Cognitive problems
The Cognitive Failures Questionnaire (CFQ; Broadbent et al., 1982; Ponds et al., 1997) is a 25-item self-report questionnaire that assesses common types of cognitive mistakes in perception, memory and motor function (e.g. misplacing one’s keys or forgetting appointments). Internal consistency is 0.91, and test–retest reliability over a 2-month period is 0.82 (Vom Hofe et al., 1998).
Of the aforementioned materials, the SRS-A was specifically designed for an autism population, and the SCL-90 (Spek et al., 2013) has been used in an autism population before. The RAND-36, DART and CFQ have not previously been used in an autism population.
Data analyses
First, a univariate analysis of variance was conducted to determine the difference in QoL between people with and without autism. Next, we combined the autism and TD groups in order to conduct a linear regression analysis. Age, IQ and symptom severity were tested as potential predictors of QoL. Exploratory regression analyses on the combined group were performed to test interaction effects of age, IQ and symptom severity with group, as well as the predictive powers of psychological and cognitive problems on QoL.
A boxplot revealed three outliers in the TD control group that had low scores on the RAND-36 (more than 1.5× the interquartile range (IQR)). All analyses were performed with and without these outliers. When there was no difference in the pattern of findings, we reported the results based on the full sample. When a difference was found, we reported the results of both analyses.
Results Study 2
Main outcome
The autism group reported a lower QoL (M = 66.7, SD = 16.6) compared to the TD group (M = 82.0, SD = 13.2), F(1,46) = 12.5, p = 0.001, η2 = 0.21. To test whether age, IQ and symptom severity were predictors of QoL, a regression analysis was conducted. Results showed that the model was significant, F(3,43) = 4.06, p = 0.013, η2 = 0.17. Age and IQ were not significant, but symptom severity did significantly predict QoL, β = −0.44, p = 0.002, with more symptoms relating to a lower QoL. However, all the individuals in the autism group had more severe autism symptoms than the TD control group, and so this seems to be an effect of group. An additional regression analysis was run on only the autism group; this showed that for people with autism, symptom severity did not predict QoL, F(1,22) = 0.044, p = 0.836.
Exploratory regression analyses
Exploratory regression analyses were performed to determine whether age, IQ and symptom severity had a different impact on QoL within the two groups. There were neither interaction effects nor main effects of age, IQ or symptom severity. The effect of group was present in most models (results can be obtained from the first author).
Furthermore, we explored whether cognitive problems and psychological problems were potential predictors of QoL. The direct group comparison showed that the autism group reported more cognitive problems (M = 45.1, SD = 13.8) than the TD group (M = 30.9, SD = 11.5), F(1,46) = 15.1, p < 0.001, η2 = 0.25. Moreover, the autism group reported more psychological problems (M = 166.3, SD = 36.7) than the TD group (M = 120.2, SD = 42.5), F(1,46) = 16.2, p < 0.001, η2 = 0.26. The regression analysis showed that there were main effects for cognitive problems and psychological problems, but these effects disappeared when outliers where removed. This suggests that these effects were due to influential outlying data points.
Inclusion of Study 2 in the meta-analysis
As this study provides unique information about QoL in the elderly with autism (Cohen’s d = −1.02, variance 0.10), it was also included in the meta-analysis; this did not significantly change any of the findings reported in Study 1.
Discussion Study 2
This study shows a large difference in QoL between people with and without autism. Factors that are likely to have an effect on QoL – intelligence, symptom severity and language development – could not be studied in the meta-analysis due to the lack of information in the included studies. Fortunately, some insight into these factors could be gained from Study 2. Intelligence – as estimated by the DART-IQ – was not found to have an effect on QoL. It should be noted that all participants were intellectually able (IQ range 81–130), and the effect of intelligence may be more pronounced in the lower ranges (Howlin et al., 2004; McGovern and Sigman, 2005). Severity of symptoms did not influence QoL, which is contradictory to previous reports (Eaves and Ho, 2008; Kuhlthau et al., 2010). This might be due to the small sample size that resulted in insufficient power to detect such an effect. However, an alternative interpretation could be that among the elderly, symptom severity may no longer be a relevant factor. Unfortunately, there was no information on language development in Study 2. For the elderly, it is often not feasible to recover information about language development in childhood. However, this is still a factor that, when feasible, should be studied. The exploratory analysis showed that psychological problems or cognitive problems did not contribute to QoL over and above the effect of group.
General discussion
Our main aim was to test if there was a difference in QoL between people with and without autism and to explore the factors that influence QoL. The meta-analysis shows that there is a large difference in QoL between people with and without autism. This effect was observed in children, adolescents, adults and the elderly.
The hypothesis that age affects QoL is not supported by the present results. This indicates that individual differences seem to be more prominent than an overall trend. This is in line with previous research that also found no associations between QoL and age (Kamio et al., 2012; Kamp-Becker et al., 2011). To the contrary, Bennet et al. (2005) reported that increasing age was associated with decreasing QoL. However, they did not include a subjective QoL assessment, and their results could reflect deteriorating circumstances, and not necessarily life satisfaction. When focussing solely on relationships with friends (one aspect of QoL), QoL did seem to improve with age in a sample aged 10 to 19 years old (Cottenceau et al., 2012). This coincides with the finding that adolescents improve in the reciprocal social interaction domain (Seltzer et al., 2003). However, overall there is no substantial evidence of QoL improving or deteriorating over the lifespan. This lack of an age effect should be interpreted with caution; the number of included studies in the meta-analysis is relatively small, and the distribution of ages is skewed towards young people. While Study 2 was a good addition to the meta-analysis, the number of studies concerning adults and the elderly remained small, and thus the effect of age could not be studied optimally.
Several limitations might complicate the interpretation of our findings. The participants in Study 2 had an estimated IQ in the normal range and received the autism diagnosis in their adult life. Therefore, they may not be representative of the whole autism population. Another caveat is the small amount of studies in the meta-analysis. There was a sufficient amount of studies to conduct a meta-analysis, but unfortunately, another 17 studies with valuable information about QoL in autism could not be included because they did include a control group. These studies describe QoL, or they use QoL to measure treatment efficacy. Including a control group in these types of studies would generate a wealth of relevant information regarding QoL in people with autism. We also recommend including measurements that assess variables that might influence QoL because in the current meta-analysis much heterogeneity was left unexplained. As IQ, symptom severity and language development are thought to be important factors in adult outcome, it is recommended that future studies on QoL at least take these into account, so it can be determined whether these factors indeed explain some of the heterogeneity. Moreover, a longitudinal study to examine the age factor would be ideal, but a well-balanced cross-sectional study could already improve our understanding of the developmental trajectory of QoL in people with autism.
The large difference in QoL between people with and without autism warrants that much work needs to be done to help people with autism reach a higher level of QoL. Environmental factors and treatment can contribute to this. A higher QoL is related to early diagnosis (Kamio et al., 2012) and a larger amount of perceived support (Renty and Roeyers, 2006). QoL improves with supported employment (García-Villamisar et al., 2002), residential (Gerber et al., 2011) and leisure programmes (García-Villamisar and Dattilo, 2010). Hence, it is important that organizations that care for people with autism take all of the above into account so that the QoL of people with autism can be improved.
The meta-analysis also shows that the focus of research is on young people (see also Mukaetova-Ladinska et al., 2012). For a comprehensive picture of autism, more attention should be paid to adults and the elderly. In return, this can also lead to valuable information for young people with autism. A better understanding of the developmental trajectory of autism means that interventions can be adjusted to the specific needs of people with autism across the lifespan.
Footnotes
Acknowledgements
We would like to thank Anika Bexkens and Laura Ruzzano for their statistical advice regarding the meta-analysis. Moreover, we also thank Laura Ruzzano for her helpful grammar-related comments.
Funding
This work is part of the research program “Autism and Aging: A Double Jeopardy”, which is financed (VIDI grant number 452-10-003) by the Netherlands Organization for Scientific Research (NWO).