
Abstract
Research within the autism spectrum disorder field has emphasized the role of socioeconomic status in shaping parents’ ability to access services for their child with autism spectrum disorder. However, research has yet to explore the possible mechanisms underlying this relationship. This study sought to address this research gap by examining the following questions: (1) Does parents’ service knowledge mediate the relationship between parent socioeconomic status and parents’ autism spectrum disorder service use? (2) What are parents’ reported service needs and service barriers, and do these needs vary across higher and lower socioeconomic status groups? Quantitative results from 244 parents of a child with autism spectrum disorder indicate that parents’ autism spectrum disorder service knowledge partially mediates the relationship between parent socioeconomic status and parents’ autism spectrum disorder service use. Qualitative findings helped to clarify this relationship by suggesting that both high and low socioeconomic status parents are aware of their child’s basic autism spectrum disorder needs. However, low socioeconomic status parents more often report needing more information about services and more in-home services and emphasize that a number of structural barriers impede their ability to meet their child’s autism spectrum disorder needs. On the other hand, high socioeconomic status parents more often report a need for “higher quality services,” possibly reflecting their better recognition of best practice guidelines. These results highlight the need for a multi-pronged approach to tackling unmet service needs within the autism spectrum disorder field.
Introduction
Intervention research over the past couple of decades has prompted advances in both the quality and the quantity of interventions that are available for children with autism spectrum disorder (ASD; Dawson, 2008; National Autism Center, 2009). This research has emphasized intervention as a means for children with ASD to see significant improvements in IQ, language, social skills, and educational placement (Dawson, 2008; Reichow and Volkmar, 2010; Rogers and Vismara, 2008). Despite these advances, studies examining service use have emphasized that many parents are dissatisfied or only somewhat satisfied with the services that they access for their child with ASD (Spann et al., 2003; Thomas et al., 2007b). When asked about areas in which ASD service use could be improved, parents generally report the need to improve the quality, quantity, and accessibility of services. For example, parents emphasize being dissatisfied with the information available about services, the insurance funding for service coverage, the lack of collaboration between parents and professionals, and the lack of professionals with specialized ASD training (Brookman-Frazee et al., 2012; Dymond et al., 2007). Although similar concerns are often reported by parents of children with other special health care needs (CSHCN; Chiri and Warfield, 2012; Kogan et al., 2008; Krauss et al., 2003), overall dissatisfaction with services is higher for parents of children with ASD (Bitterman et al., 2008; Montes et al., 2009) and likely reflects the substantial difficulty that parents of children with ASD experience when trying to access appropriate health and education services for their child.
Studies noting challenges in ASD service access have also noted that these challenges are not experienced to the same magnitude by all parents of a child with ASD. Rather, receiving an ASD diagnosis and accessing ASD services can be influenced by a number of factors, including a family’s socioeconomic status (SES; Durkin et al., 2010; Liptak et al., 2008; Patten et al., 2012). Specifically, low SES has been associated with a later age of ASD diagnosis (Durkin et al., 2010; Thomas et al., 2011) and decreased ASD service use (Liptak et al., 2008; Patten et al., 2012). Given the relationship between SES and service use, it is not surprising that lower SES families of CSHCN including ASD report a higher number of unmet service needs (Farmer et al., 2004; Larson and Halfon, 2010; Porterfield and McBride, 2007), greater difficulty accessing care, and a lower level of satisfaction with the services they are using than higher SES families (Farmer et al., 2004; Hare et al., 2004).
Although a number of studies have documented SES-based disparities in ASD service use, satisfaction, and unmet service needs (Farmer et al., 2004; Patten et al., 2012; Thomas et al., 2011), only a few studies have speculated about the potential mechanisms underlying this relationship, and existing evidence for these mechanisms has been indirect at best. For example, some researchers have suggested that lower SES families may experience a greater number of structural barriers that impede their service access (e.g. King and Bearman, 2011). In support of this hypothesis, research has found that lower SES parents are more likely to indicate that high service cost and transportation difficulties are barriers to service access (Patten et al., 2012; Porterfield and McBride, 2007; Thomas et al., 2011). This research is particularly important given the evidence that parents’ perceived barriers can impact their uptake and adherence of child mental health services more broadly (Kazdin et al., 1997). If lower SES families do experience a wider variety of barriers, as some research has hypothesized, it may be these differentially experienced barriers that play a role in their decreased service use. However, research has yet to examine which specific structural barriers differ across SES groups, and how these differences may explain the health gradients observed in ASD service use.
Alternatively, it has been proposed that lower SES families access fewer services because they are less aware of their child’s needs for specialty services or are less aware of available service options for their child (Porterfield and McBride, 2007). In support of this hypothesis, Porterfield and McBride (2007) showed that parents from lower SES backgrounds were less likely to indicate that their child needed specialty services than parents of higher SES backgrounds, despite the fact that they reported that their child experienced more severe health pathology. A related possibility is that higher SES parents may be more effective advocates for their child and may be better able to seek out and advocate for needed services when faced with barriers (King and Bearman, 2011).
To better understand the potential mechanisms underlying service access disparities in families of children with ASD, we conducted a mixed method study. In the first phase of the study, we used a quantitative approach to determine what services parents were currently accessing for their child with ASD. Consistent with previous health disparities research, we expected to find that higher SES parents would report accessing a greater number of services for their child with ASD. We also asked parents to indicate all of the services that they had heard of as treatment options for ASD. We hypothesized that if differences in parent knowledge about service availability played a role in health disparities (Porterfield and McBride, 2007), then parents from higher SES backgrounds would also report greater awareness of service options for ASD, and that this knowledge might mediate the relationship between parent SES and parent service use. In the second phase of the study, we used a qualitative approach to examine parents’ perceived service needs and barriers to service use. We hypothesized that many themes regarding perceived service needs and barriers to service access would be similar across SES levels. However, we also hypothesized that some unique themes would emerge based on parent SES, and that these differences might help explain the mechanisms underlying the relationship between SES and ASD service use.
Method
Participants
In total, 244 parents of a child with an ASD diagnosis (i.e. autistic disorder, Asperger’s syndrome, pervasive developmental disorder–not otherwise specified (PDD-NOS)) between the ages of 2 and 17 years (M = 6.41 years, SD = 2.57 years) participated in this Institutional Review Board–approved study. Recruitment for this study occurred in two ways. Of the sample, 73% (N = 177) was recruited through the Interactive Autism Network (IAN) Research Database. To increase the representativeness of the study sample, 27% (N = 65) of participants were non-IAN families who were recruited through ASD resource centers and ASD clinical centers across the United States. Informed consent was provided to all participants. Preliminary analyses indicated the two recruitment samples did not significantly differ on any collected demographic measures. As a result, the two samples were combined in all analyses.
Parents came from 35 different US states, were 95% female, and were 38.10 years of age on average (Range: 23–64 years, SD: 6.68 years). Of the parents, 7% had a high school education or less, 33% had completed specialized training, and 60% had a 4-year college education or greater. Parents indicated that 66.5% of their children had an autism diagnosis, 11% had an Asperger’s syndrome diagnosis, and 21% had a PDD-NOS diagnosis. Of the children, 80% were male, and the average age of ASD diagnosis was 3.19 years (Range: 1–14 years; SD: 1.79 years). All participant characteristics are presented in Table 1.
Sample characteristics.
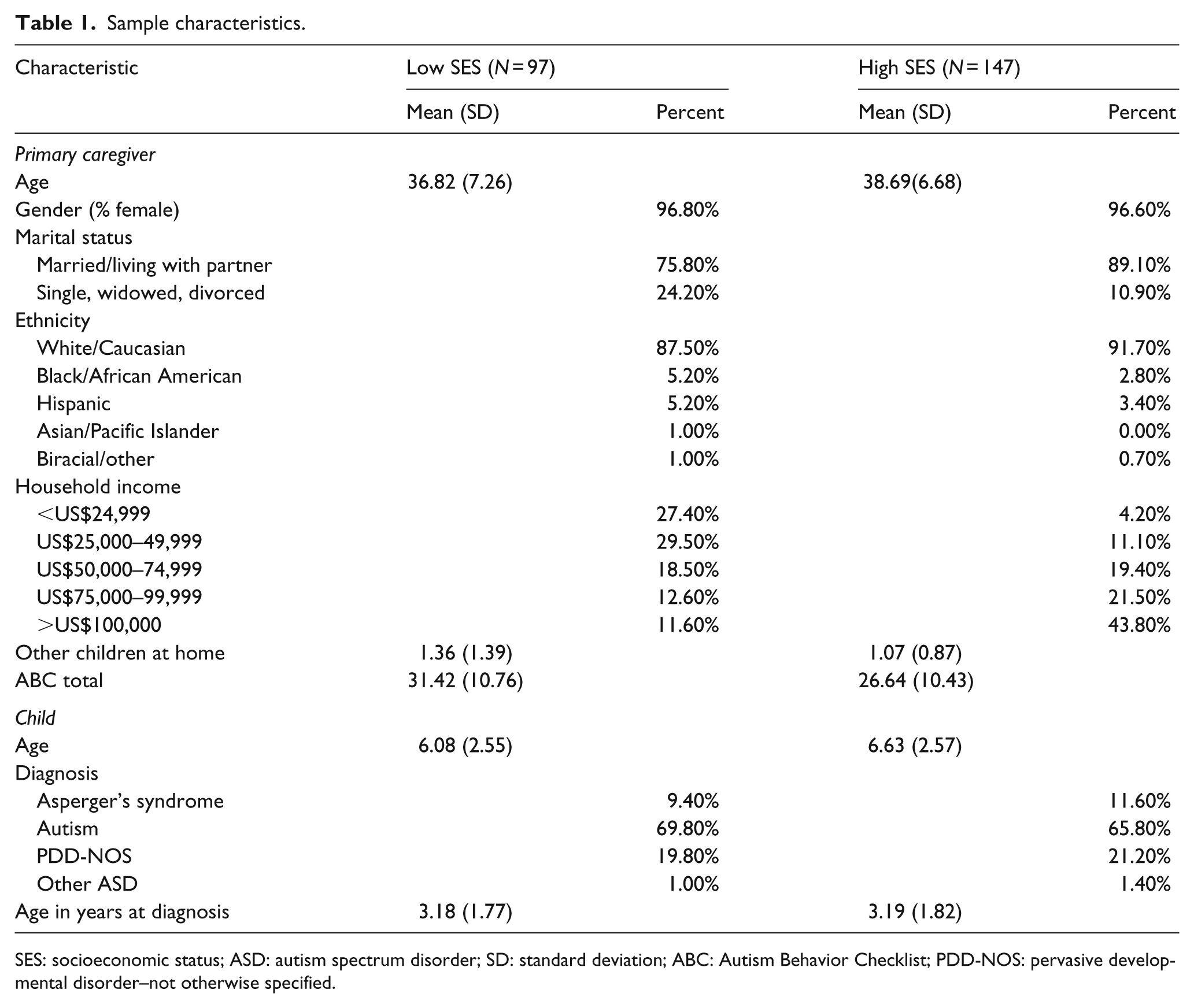
SES: socioeconomic status; ASD: autism spectrum disorder; SD: standard deviation; ABC: Autism Behavior Checklist; PDD-NOS: pervasive developmental disorder–not otherwise specified.
Measures
This study was administered over the Internet using Qualtrics software.
Socio-demographic information
Parents provided basic demographic information about themselves and their child. This included primary caregiver age, gender, education level, marital status, zip code (county of residence), as well as the age, gender, diagnosis, and age of diagnosis for their child with ASD.
Parent SES
For this study, parent education level was used as a proxy for SES. Parents reported their highest educational degree on a 5-point Likert-type scale with a 1 indicating the parent had not obtained a high school degree, a 2 indicating they had a high school degree, a 3 indicating they had a specialized training degree, a 4 indicating they had a 4-year college degree, and a 5 indicating that they had a graduate degree. Education level on this scale was used as the measure of Parent SES in the quantitative data analysis. For the qualitative analyses, parents with less than a 4-year college education were considered lower SES (N = 98, 40.30%), and those with a 4-year college education and higher were considered higher SES (N = 146, 59.70%). Prior to choosing our proxy for SES, we completed a review of how SES has typically been measured in other health disparities research. From this review, it appeared that there were many strategies to approximate SES, all with their unique set of advantages and disadvantages (Shavers, 2007). Although using maternal education as a proxy for SES is also associated with disadvantages, our review of prior research suggested that education is more stable than family income, less affected by parental age, and a better approximation of SES when it is measured as education credentials rather than years of education (Krieger et al., 1997; Shavers, 2007), which was how this variable was measured in this study.
ASD symptom severity
Parents completed the Autism Behavior Checklist (ABC) (Krug et al., 1980) as a measure of their child’s ASD symptom severity. The ABC consists of 57 questions that ask about behaviors that are specific to ASD, as well as other general behavior problems. Parents marked “yes” or “no” to indicate whether the particular behavior applied to their child. Items on the ABC are weighted so that a “yes” to a less severe behavior is scored as a 1, and a “yes” to a more severe behavior is scored as 4. Total scores were summed with higher total scores indicating more severe ASD symptoms. Cronbach’s alphas from this study indicated good inter-item correlations (r = 0.22) and good internal consistency (α = 0.94).
Autism services
Parents were provided with a list of 52 services that have been identified as common services used by parents of a child with ASD (Hyman and Levy, 2010; Odom et al., 2010; Thomas et al., 2007b). From this list, parents selected (1) all of the services that they had used for their child over the past 6 months (Service Use) and (2) all the services that they had heard of as intervention options for ASD (Service Knowledge). Parents were also provided with blanks to indicate any services that they used that was not a part of the provided list.
Service needs and barriers to service use
Parents were asked to respond to two open-ended questions: (1) What services do you think your child could use that he/she currently does not have? and (2) What are some of the barriers that you have experienced in accessing services to meet your child’s needs?
Data analysis
Quantitative data
Initial bivariate correlations between the socio-demographic variables and service variables were examined. Parent SES and child symptom severity were both significantly associated with parent service knowledge and parent service use and thus were included in the path analysis. No other associations between demographic variables and autism service variables were significant.
SPSS AMOS software was used to run a path analysis as a means to analyze the quantitative data and to determine whether parent knowledge mediated the relationship between parent SES and parent service use. The path analysis included parent SES and child symptom severity as predictor variables, parent service knowledge as a mediator variable, and parent service use as the outcome variable. In this analysis, mediation would be indicated by statistically significant effects of the predictor variables on the mediator variable and of the mediator variable on the outcome variable (i.e. indirect effects), along with non-significant effects of the predictor variables on the outcome variables (i.e. direct effects); partial mediation would be indicated by indirect effects, but still significant direct effects.
Qualitative data
Given the open-ended nature of the qualitative questions, not all participating parents chose to respond to these questions. In total, 214 of the 244 participants responded to these questions. Those parents who did respond to the questions did not differ demographically from those that did (all d’s < 0.19). A ground theory approach, facilitated by the use of Dedoose software, was used to examine the qualitative data to understand service needs and barriers to service use (Corbin and Strauss, 1990; Strauss and Corbin, 1990). In the first phase of qualitative analysis (open coding), participant responses to each question were de-identified, compiled, and reviewed by the two investigators as a means to condense the data into analyzable codes (Corbin and Strauss, 1990; Strauss and Corbin, 1990). These initial codes were collaboratively determined at the transcript’s manifest level and were created based on constant comparative analysis, in which segments of the transcript were thoroughly compared for similarities and differences. Reliability was assessed after each investigator independently coded the transcripts and was calculated as percent agreement on 30% of each transcript (Boyatzis, 1998). Analysis indicated good reliability, with agreement on 89.70% of codes. In the second phase, investigators used axial coding to relate the specific codes from the first phase into broader “subcategories” (Corbin and Strauss, 1990; Strauss and Corbin, 1990). During the third phase, selective coding was used to integrate all of the relationships between categories and subcategories into one, overarching phenomenon. Critically, all coders were blind to child and family characteristics during the coding process.
Finally, relational and variational sampling was used to compare patterns of parent-reported service needs and barriers across higher and lower levels of SES (Strauss and Corbin, 1990). Additionally, parent-reported service need and barriers to service use codes were tallied across participants and compared across SES groups as a means to quantify and compare the percentage of parents who were spontaneously reporting specific needs and barriers. The method of transforming qualitative codes into quantitative themes is frequently used in qualitative research as a means to compliment qualitative research (Boyatzis, 1998).
Results
Path analysis
Figure 1 presents the paths with significant standardized beta values. As can be seen in the model, parent SES was a positive predictor of parent service knowledge (0.17), which was a positive predictor of parent service use (0.24). Higher parent SES was associated with greater knowledge of autism services, and greater knowledge of autism services was associated with a higher number of services used. Parent SES also had a direct effect on service use (0.16). In contrast, child symptom severity was not a significant predictor of parent service knowledge (−0.12) or parent service use (0.07).
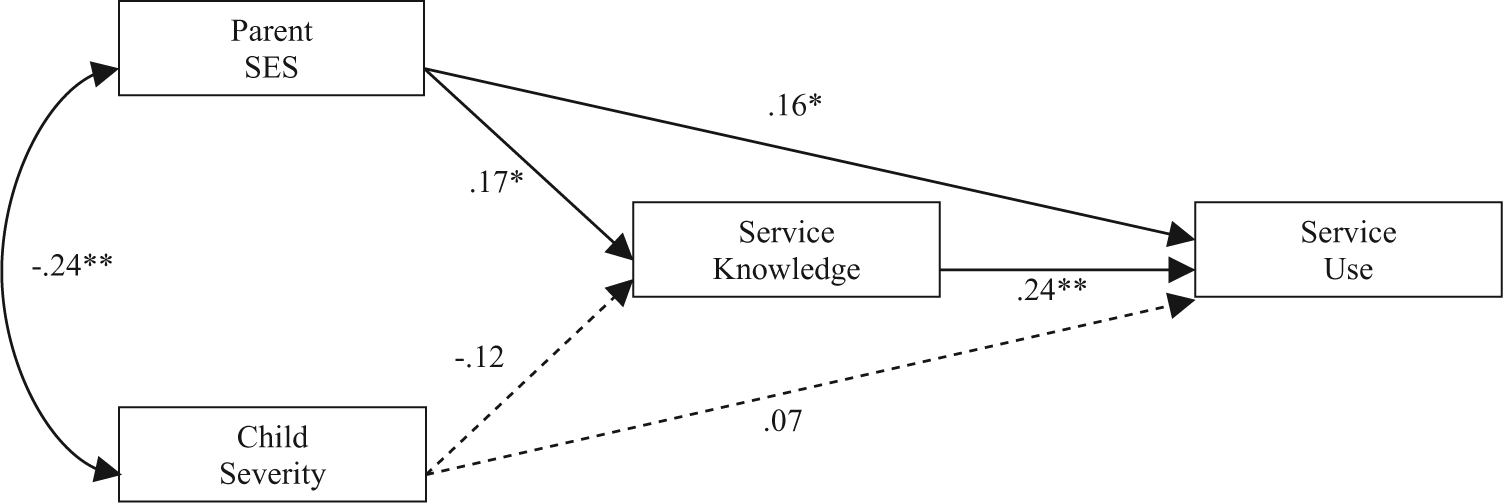
Path analysis of the relationship between study variables.
These findings suggest the relationship between parent SES and service use may be partially explained by parent knowledge about service options available. However, the significant direct effects of parent SES on service use indicates other factors also contribute to disparities in service use seen among lower SES families.
Reported service needs
Parents were asked, “What services do you think your child could use that he/she currently does not have?”; 85.71% (n = 84) of lower SES group and 89.04% (n = 130) of the higher SES group responded to this item. Spontaneously reported service needs, grouped by SES, are displayed in Table 2. As can be seen, primary themes included the need for applied behavior analysis (ABA) services, in-home services, parent training, and speech therapy, in addition to higher quality and larger quantities of services:
I need a place where the therapist will work with me and him to teach me how to help his progress at home. I can’t find good therapists and doctors. Most have been a waste of my time. There is a dearth of high quality social skills training in schools and in private groups.
Percentage of parents within each SES group that spontaneously reported each service need and barrier to service use.
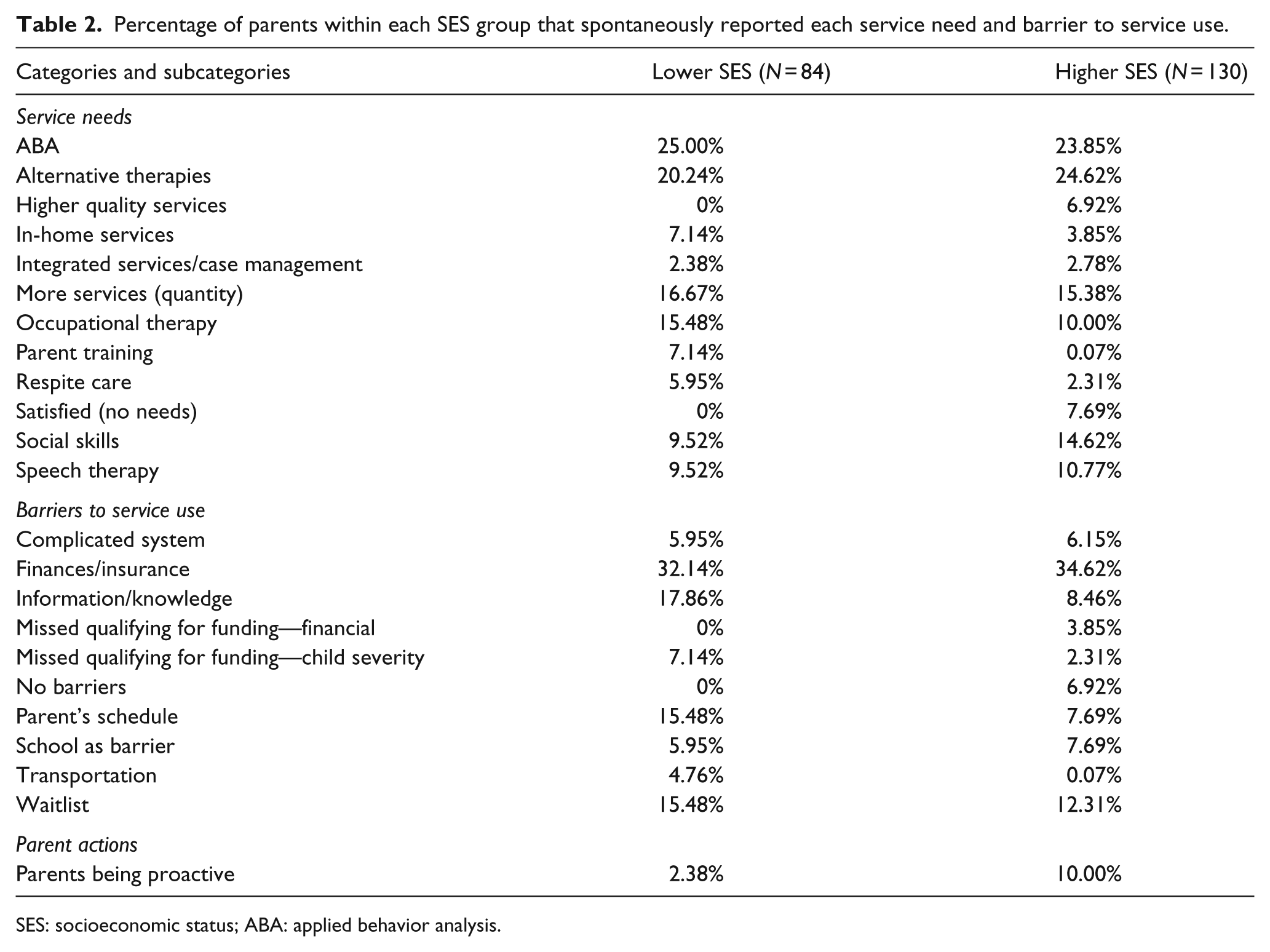
SES: socioeconomic status; ABA: applied behavior analysis.
As can also be seen in Table 2, service needs varied by the SES group. Lower SES parents were more likely to endorse needing respite care, in-home services, and parent training services. On the other hand, only higher SES parents reported needing access to social skills groups and higher quality services, and these parents more frequently endorsed being satisfied with their service needs. Finally, both lower and higher SES parents indicated that they needed a larger quantity of services. This included needing both more hours of the services they were currently using, as well as needing a wider variety of services that they were not currently receiving:
I like the services he is getting but wish he could get more each week. She needs any and all. She needs more speech and OT. But I would also like to try out herbal supplements and chelation therapy. Maybe social and group therapies too.
Barriers to service use
Parents were asked, “What barriers do you experience when attempting to access services for your child?” Responses to this portion of the survey fell into themes that are displayed in Table 2. Generally, parents emphasized the difficulty in navigating a complex system to find services and emphasized that finances, insurance, transportation, wait lists, scheduling, and their own knowledge served as barriers to their service use. Moreover, like parent-reported service needs, many parent-reported barriers to service use varied by the SES group.
Parents in both higher and lower SES groups reported frustration with the lack of appropriate insurance coverage for services and the high out-of-pocket cost of services. However, higher SES families were more likely to indicate that their income precluded them from receiving additional funding for services:
Financial barriers are number one—my husband and I are over income and we have to come out of our pockets to provide services to our son and we can’t afford it. Insurance covers limited services and we are at a deficiency in giving our son what he needs.
On the other hand, lower SES parents more often indicated their child’s symptom severity or age was a barrier to meeting the cutoff to receive public funding for services:
When he turned three years of age his services ended which means I am responsible to pay out of pocket for his therapies. It is very expensive. It is aggravating that insurance companies don’t help.
Additionally, lower SES families were more likely to indicate that transportation and their own busy work schedule prevented them from accessing services. Parents reported that many services were offered within typical work hours and that few were accessible to them after the work day:
I work full time and have another child and most appointments are during the day. I cannot take time off or rearrange my already full schedule to work in therapy.
Overall, parents in both higher and lower SES groups reported frustration and confusion when attempting to navigate service access and emphasized the need for case management to help integrate their child’s wide-ranging service needs. Interestingly, it was the lower SES families that more often indicated the need for information regarding available services, which services would most benefit their child, and how insurance coverage fits into the picture:
The problem is that it can be extremely overwhelming trying to figure out what to try, what will work, what is covered by insurance, and where to start. No one seems to know what services we should be getting. Pediatricians say to call psychiatrist. Psychiatrist says we don’t need anything. I wish we had a set person that I could ask questions to about ASD and that could advise us at to which services we could and should be receiving.
Parents in both higher and lower SES groups also indicated that even when they were able to locate appropriate services for their child, the wait lists for these services were long and limited valuable intervention time:
Everyone says the earlier you start services the better off you are and that intervention is everything, especially in the first 5 years, yet that’s about how long you have to wait before you ever see any real services manifest.
When discussing services received through the public school system, both lower and higher SES parents reported frustration with the ways in which services were being implemented in the school setting. For example, parents emphasized that services were not effectively implemented in the school and that teachers were not trained to provide services to children with ASD specifically:
He is mainstreamed at school with some extra support but he is really struggling to learn reading and math. The school sometimes feels like a waste of time as far as him learning things. Not because he is unteachable but because it is the wrong environment for him.
Parent actions
Parents had varied responses to the complicated and frustrating systems that they were navigating. Some parents reported feeling that they were overwhelmed by the system and discouraged about their ability to access services for their child:
I think he (my son) is eligible for ABA therapy, covered by insurance, but I’m intimidated by all the hoops I’d have to jump through to get it started. As a parent, I am frustrated, sad, and disappointed regularly and have reached out to other parents of ASD children for guidance, only to find out that they have already gone through the same things and not much has improved.
Other parents, nearly all from higher SES backgrounds, indicated that they were proactive in order to gain access to the services that they were looking for. This included fighting the system, changing or quitting their job to accommodate therapy, moving to areas with better service options, or creating new services for their child and others in their community. These parents emphasized that services were indeed hard to access, but that they felt capable of actively seeking out and finding the services that their child needed:
My child needs speech therapy, has a language delay, but our insurance doesn’t cover it. I’ve fought and fought. Even thrown out Stevens law but we are exempt from that. Case managers do not give information on what’s available, you have to uncover it yourself and then it’s a fight to even get the services. We had very limited access to services in our small community. We have now moved into a major metro area and are doing intensive intervention in order to make up for lost time.
Discussion
The results of this study expanded prior health disparities research within the ASD field by examining the nature of the relationship between parent SES and parent service use. Our quantitative findings demonstrated that while parent SES was associated with greater ASD service use, this relationship was partially mediated by parents’ knowledge of ASD service options. This finding supports the hypothesis that lower SES parents are less likely to be aware of service options for their child, which may contribute to their use of fewer services for their child.
While quantitative results clarified the role of SES on the services parents had heard of and those they were using, the qualitative results helped to provide a more nuanced picture of how SES might be influencing parent service knowledge and use by examining parent-reported service needs and barriers to service use. What became most apparent was the quantity versus quality split in parent-reported service needs. Both lower and higher SES families reported needing more frequently recommended services such as ABA, speech-language therapy, and occupational therapy. These similarities in reported needs across groups suggest that both high and lower SES parents are aware of their child’s ASD needs. However, lower SES families in particular were less likely to report being satisfied with their service use and reported needing more information about services, more in-home services, more respite care, and more parent training. The spontaneously reported dissatisfaction, lack of knowledge, and need for more of these specific services are consistent with the quantitative results that demonstrated that lower SES parents reported having heard of fewer service options and having accessed fewer services for their child with ASD. Taken together, these findings suggest that many lower SES parents are aware of their child’s broader service needs, but are less aware of the multitude of other services available, and how to go about accessing enough services to meet those needs.
Lower SES parents more often reported that their work schedule and transportation prevented them from accessing services. This is consistent with the hypothesis that lower SES parents experience a greater number of structural barriers that negatively influence their ability to access services. Their expressed desire to implement intervention themselves or to have services delivered within their home environment may reflect the belief that these specific services will help them overcome service access barriers. Interestingly, a similar percentage of higher and lower SES parents reported financial and insurance barriers when attempting to access services for their child. It has been proposed that service costs may be a particularly salient structural barrier to service access that might explain disparities in service use for lower SES families. The fact that higher education parents were equally likely to report financial and insurance barriers as lower education parents may indicate that public insurance, which one must qualify for based on low income or high child need, provides better coverage of ASD services than private insurance (Krauss et al., 2003; Thomas et al., 2007a). Although we did not collect information on the families’ type of insurance, this interpretation is consistent with the finding that higher SES parents were more likely to report difficulty qualifying for insurance funding based on their income.
Only higher SES families reported a need for “higher quality services.” This need may reflect the fact that higher SES parents reported being more proactive when faced with barriers to service access. This finding is consistent with past research studies demonstrating the role of social class on diagnostic and service-seeking behavior (Wing, 1980). It may be the case that this proactive search for services leads higher SES parents to have a better recognition of best practice guidelines and “high quality” services. It may also be the case that higher SES parents create more services by being stronger advocates for their child and fighting the system when faced with barriers to service use. This advocacy may lead parents to perceive that more services are available to them and may help explain why they endorse using significantly more services than lower SES parents.
Our study findings call for the need to address service dissemination issues at distinct levels. At the first level, the findings underscore the importance of addressing the role of SES on the amount of knowledge that parents have about ASD services. This lack of knowledge could be addressed by more explicitly helping parents navigate service options for their child. Providing parents with basic psychoeducation, social support, and strategies to access services should be a critical portion of any diagnostic process, and may serve to reduce parent stress while enhancing their service knowledge.
At the second level, our study findings suggest that some parents may be aware of their child’s service needs, but are simply unable to address these needs within their community. For higher SES families, there was notable concern about the quality of available services. Training providers to specifically work with children with ASD and using more effective models in order to disseminate best practice service guidelines to community providers may be one such method to address these concerns (Dingfelder and Mandell, 2011). On the other hand, both higher and lower SES parents emphasized concern about the quantity of services they were receiving and expressed a desire to learn intervention strategies themselves as a means to provide intervention to their child within the home setting. This expressed interest is crucial to consider given that parent-mediated intervention has been shown to be an evidence-based service that can directly target the core social communication deficits of ASD, while also reducing parent stress (Ingersoll and Wainer, 2013; Tonge et al., 2006). Taken together, these “second level” barriers suggest a stronger emphasis on establishing models of provider and parent training as a means to enhance the quantity and quality of available services for families at all SES levels.
At the final level, our study findings highlight the need to help parents navigate a complex system. Although there were notable individual-level disparities in service availability, parents unanimously indicated barriers in being able to integrate their child’s many service needs. The request for integrated service care as a means to decrease parent stress and frustration is by no means new to the ASD field (Brookman-Frazee et al., 2012; Dymond et al., 2007). One solution to this problem is to implement a medical home-based model of care to help guide parents through their service needs by providing family-centered and culturally competent services that are overseen by one primary care provider. Such models of care are often used for children with special health care needs as a means to coordinate and enhance services, while also decreasing parent stress (Ghandour et al., 2011). Research has noted that despite their complex health needs, children with ASD are less likely than other children with special health care needs to receive a medical home model of health care (Brachlow et al., 2007). However, more widespread use of such a model will be critical in order to address the unanimous stress that parents indicate when attempting to access and navigate their child’s service needs across multiple settings.
In summary, our study findings give a more nuanced picture of the role of SES on parents’ ability to access services for their child with ASD. Specifically, notable disparities emerged in the services that parents had heard of as intervention options for their child, parent-reported service needs, and parent-reported barriers to service use. Given these findings, it will be crucial to address service access issues using a multi-pronged approach in order to increase the quality and quantity of services available to families of a child with ASD.
Limitations
There are several limitations to consider with this study. First, because the study survey was completed online, the sample demographics may not be representative of all primary caregivers of a child with ASD, and the sample was limited in its number of parents who had received less than a high school education. Additionally, this study did not measure participating parents’ health insurance status. This is an important limitation to consider in our quantitative analysis given that Medicaid insurance status has been associated with greater access to services than privately based insurance plans and that qualification for Medicaid is based on both income and child ASD symptom severity (Liptak et al., 2008). Future research should examine how insurance status may influence the relationship between service knowledge and service use. Another limitation to consider is the fact that the two open-ended survey questions were worded so that they asked about parents’ negative experiences in accessing services for their child. Therefore, the responses that parents provided may have been biased in that they were less likely to report positive experiences when navigating the health system. Finally, as noted, the manner in which demographic information was asked of parents limited our definition of SES. Given this limitation, future research should use other measures of SES in order to determine the mechanisms underlying the relationship between SES, service barriers, service needs, and service use.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.