
Abstract
Little is known about use of early interventions for autism spectrum disorder in Europe. Parents of children with autism spectrum disorder aged 7 years or younger (N = 1680) were recruited through parent organisations in 18 European countries and completed an online survey about the interventions their child received. There was considerable variation in use of interventions, and in some countries more than 20% of children received no intervention at all. The most frequently reported interventions were speech and language therapy (64%) and behavioural, developmental and relationship-based interventions (55%). In some parts of Europe, use of behavioural, developmental and relationship-based interventions was associated with higher parental educational level and time passed since diagnosis, rather than with child characteristics. These findings highlight the need to monitor use of intervention for children with autism spectrum disorder in Europe in order to contrast inequalities.
Introduction
Autism spectrum disorder (ASD), characterised by impaired social communication and interaction and by restrictive patterns of behaviours and interests, affects approximately 1% of children (Autism and Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators; Centers for Disease Control and Prevention (CDC), 2014; Baird et al., 2006). Cognitive impairment, psychiatric disorders and behavioural problems commonly co-occur with ASD (Lai et al., 2014). The complexity of the clinical presentation therefore requires early and appropriate intervention to promote positive outcomes for children and families.
There is a growing body of evidence from randomised controlled trials (RCTs), which best protect against bias, reporting promising results of the efficacy of early and intensive behavioural intervention (see reviews Narzisi et al., 2013; Warren et al., 2011) as well as of developmental or relationship-based interventions delivered by therapists or teachers (Dawson et al., 2010; Kaale et al., 2012; Landa et al., 2011; Pajareya and Nopmaneejumruslers, 2011) and parents (Green et al., 2010; Kasari et al., 2014; for a meta-analysis, see Oono et al., 2013). A number of countries in Europe have acknowledged these encouraging findings and recommend early intervention within national guidelines for autism (among others, France: Haute Autorité de Santé (HAS), 2012; United Kingdom: National Institute for Health and Care Excellence (NICE), 2013; The Netherlands: Health Council of the Netherlands (HCN), 2009). However, little is known about the actual use of ASD-related interventions in communities across Europe.
Several studies have reported on the use of intervention for young children in many countries, such as in the United Kingdom (Barrett et al., 2012; Cassidy et al., 2008), France (Rattaz et al., 2012), Israel (Raz et al., 2013) and the United States (Ruble and McGrew, 2007; Thomas et al., 2007b). However, because of the different focus of these studies (service costs, parental satisfaction, out-of-pocket expenditure) or the characteristics of the research site (e.g. a predominantly TEACCH-oriented State), comparison of intervention use across countries is difficult. This is due to several reasons: parents were sometimes asked about contacts with various professionals rather than about the use of different types of intervention; they were not systematically asked about all possible approaches or the samples are unlikely to be representative of the wider community. Three American groups conducted surveys of use of intervention that included respondents from other countries; however, the vast majority of participants were US residents (Bowker et al., 2011; Goin-Kochel et al., 2007; Green et al., 2006). The Green et al. (2006) study reached 552 families through the Autism Society of America chapter branches and found that families used on average seven different interventions, and while speech and language therapy was the most commonly reported intervention, the number of therapies used varied as a function of the child’s age and severity of disability within the autism spectrum. The Goin-Kochel et al. (2007) study replicated these findings on another sample (N = 479) recruited via similar routes. In the Bowker et al. (2011) study (n = 970), interventions based on ABA approaches were the most commonly reported interventions (37%), followed by ‘physiological interventions’ (including, for example, sensory integration and occupational therapy) and by speech and language therapy, music therapy and osteopathy, grouped by the authors in a ‘standard therapies’ category.
While these studies provide some information on the use of interventions for children with ASD in Northern America, a comprehensive description of use of intervention in Europe is lacking. Moreover, in all studies, except the two British studies and the Goin-Kochel et al. (2007) study, data for pre-schoolers were not separated out when children older than 7 years were included in the sample; this makes the interpretation of the findings difficult as the needs of children and young people with ASD change with development.
A separate but related issue is that of child and family factors associated with use of intervention, as we know that parents often report difficulties in identifying and accessing relevant services and professionals (Siklos and Kerns, 2006). Previous research in the United States has found that ethnicity and parental educational level were significant predictors of receiving an early diagnosis (Mandell et al., 2009; Shattuck et al., 2009) and accessing services (Liptak et al., 2008; Thomas et al., 2007a); however, differences in service use by ethnicity or parental education were not found in the United Kingdom (Barrett et al., 2012; Cassidy et al., 2008) and not analysed in the French study (Rattaz et al., 2012). Parents with a higher income and educational level may be better equipped to know about, advocate for and access interventions for ASD.
To promote strategies and mechanisms to collect and exchange information on ASD in Europe, the European Commission specifically included ASD in its 2003–2008 and subsequent public-health work plans (EU, 2007). With a similar aim, in 2010, the European Science Foundation funded the Cooperation in Science and Technology (COST) 1 Action ‘Enhancing the Scientific Study of Early Autism (ESSEA)’ network, composed of over 80 scientists from 23 European countries. The COST-ESSEA network had the objective to advance the pace of discovery about the earliest signs of autism (for example, studying infants at risk: Bölte et al., 2013), to combine techniques from cognitive neuroscience with those from the clinical sciences and to review the state of art of early identification (García-Primo et al., 2014) and intervention (McConachie et al., 2014) practices in Europe (Appendix 1).
Obtaining a detailed picture of amount and type of intervention received in Europe is important to inform the decisions of policy makers, both at a national and European level, in relation to funding of services and training of professionals. This study therefore used the ESSEA network to conduct a multi-country survey on use of early intervention for children with ASD across Europe. In order to enquire about a more homogeneous set of services, the age limit for inclusion in the study was set at 7 years, as by that age most children in Europe have started school.
Our aim was to describe the current use of behavioural, developmental and psychosocial intervention for children with ASD aged 7 or younger in 20 European countries. Specifically, our objectives were (a) to examine whether the type and amount of intervention received was a function of area of residency in Europe and (b) to examine whether child characteristics (age, gender, verbal ability), time since diagnosis and parental educational level were associated with use of intervention, both at a European and a regional level.
Methods
Ethical approval was given by the Research Ethics Committee of the Faculty of Children and Learning, Institute of Education, London, UK. Parents provided informed consent before completing the survey (IOE/FPS 385).
Survey development
The survey, which asked about current use of intervention (type and number of hours per week) received at home, school and clinic, was developed over three phases each involving iterations within the COST-ESSEA international network. Initially, a list of interventions, therapy approaches and aids was drawn from previous literature (Green et al., 2006) and existing autism-related web resources (Research Autism: http://www.researchautism.net/autism-interventions/alphabetic-list-interventions). Subsequently, branded interventions not available in Europe (e.g. Giant Steps) were dropped. In this phase, it was acknowledged that therapy programmes with a very similar background are available with different names in different countries and also that parents are not always aware of the theoretical approach underlying a specific programme. Therefore, each question about a broader category of interventions (e.g. ‘Is your child currently receiving a behavioural intervention?’) was always accompanied by examples of specific programmes that could have been more familiar to the parent (e.g. ‘Applied Behaviour Analysis (ABA)’, ‘Pivotal Response Training (PRT)’). The examples were specific, when possible, to each country. Finally, a question about using ‘other interventions’ was included in the survey to ensure capturing other less-defined approaches not included in the other categories mentioned. Parents were then asked to specify the nature of the intervention by selecting one or more descriptions (‘other educational intervention’, ‘other psychological intervention’, ‘social skills training’, ‘other type’) or the option ‘I don’t know’. For each type of intervention in the survey, parents were asked to report the number of hours of intervention their child/they currently received per week. Parents were explicitly asked to consider all settings where the child received the treatment and to report on all sessions delivered at home, in clinics or in school. The total hours of school attendance were not collected. A section on use of medication and complementary and alternative medicine, not considered for this study, was also included in the questionnaire (see Salomone et al., in press).
To take part in the survey, parents had to answer ‘yes’ to the question ‘Has your child received any of the following diagnoses?’ followed by a listing of all diagnostic categories for ASD in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) and 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10), which were the diagnostic manuals in use in Europe at the time of the study. General background information on respondents was also gathered: relationship to child (mother/father/other) and educational level (below high-school diploma, high-school diploma, bachelor, master/post-graduate). The educational level was collapsed for analysis into the following two categories: low educational level (up to high-school diploma) and high educational level (bachelor and master/post-graduate). To comply with the relevant legislation on cross-national sharing of sensitive personal data in some of the participating countries, parents were asked to report on the country of residency but data on nationality and ethnicity were not collected. Respondents were asked to indicate the age of the child at the time of receiving an ASD diagnosis. Respondents were also asked to describe the child’s verbal ability by selecting one of five options (does not talk; uses single words; uses two- or three-word phrases; uses sentences with four or more words; uses complex sentences). Exemplars of each category were given to help respondents. For the purposes of analysis, the options were collapsed into the following two categories: low verbal ability (non-verbal or single words speech) and phrase speech (simple and complex phrases).
Before launching the survey, the questionnaire was piloted with parents approached through the main national parent support association in the United Kingdom (N = 8) and through personal contacts of clinicians in Italy (N = 2). Parents were asked to provide feedback on the survey’s content, format and accessibility. All parents reported that the survey was easily accessible and the questions clear and comprehensible. Based on the suggestion of some parents, the possibility to select a generic intervention if the nature of the approach was not known was further highlighted in the initial instructions. The final set of questions was then translated and adapted by one or two researchers for each of the countries involved in the project. The researchers in each of the countries were fluent in English and expert in the field of early autism. This process involved using the official translation of named programmes, where available in each country. Each translation was then uploaded onto a web platform and access to the survey was made available via nation-specific web links, each bound to an online dataset provided by the survey platform. A sample question of the English version of the survey is provided in Table 1.
Sample questions from the survey.
Recruitment
The survey was addressed to parents of children with ASD aged 7 or younger and living in 20 countries involved in the COST-ESSEA network: Austria, Belgium, Czech Republic, Denmark, Finland, France, Germany, Hungary, Iceland, Ireland, Italy, The Netherlands, Norway, Poland, Portugal, Romania, Spain, Sweden, the former Yugoslav Republic of Macedonia and the United Kingdom. Researchers and clinicians in the COST-ESSEA network promoted the recruitment of the participants through national parents’ associations who advertised the link to the web-based survey via posts on their official websites and social network pages, where available. If previous consent to receiving communications from the associations had been given, an email message was sent from the associations to their members’ mailing list. Parents were also recruited via autism-related websites and social networks and through the researchers’ professional contacts. In the former Yugoslav Republic of Macedonia, participants were recruited through the Paediatric Clinic of Skopje as parents’ associations did not exist and the survey was completed on paper for separate data entry. A decision was made to exclude Austria and Sweden from the study, as the number of participants recruited via all recruitment channels within the planned timeframe was too low (Austria: n = 1; Sweden: n = 5). For this reason, the final dataset included information on 18 countries. Two initial questions were designed to filter out participants who did not meet the inclusion criteria: to be a parent/caregiver of a child (a) with ASD and (b) aged 7 or younger. The survey was open for 45 days. When this period expired, the datasets were downloaded from the survey platform as SPSS files and merged into a single dataset for data analysis purposes.
Data analysis
The countries involved in the study were grouped in European regions, as defined by the official classification of the United Nations (UN, 2006): Western Europe (Belgium, France, Germany, The Netherlands), Northern Europe (Denmark, Finland, Iceland, Ireland, Norway, United Kingdom), Eastern Europe (Czech Republic, Hungary, Poland, Romania) and Southern Europe (Italy, the former Yugoslav Republic of Macedonia, Portugal, Spain). Descriptive statistics were used to report on type and amount of intervention used in the total sample, in the four European regions and in each country separately.
To explore the determinants of use of intervention and amount of intervention received in the total sample and in the four European regions, two specific categories of intervention (speech and language therapy, and a summary category including behavioural, developmental and relationship-based interventions) were selected as dependent variables. These two types of interventions were selected as they were the most frequently used in the total sample and in consideration of their conceptual relevance to ASD.
To compare the effect of European region of residence on amount of intervention received, three one-way between-subjects analyses of variance (ANOVAs) were conducted with the following dependent variables: (1) number of total hours per week of any intervention received; (2) number of hours per week of behavioural, developmental and relationship-based interventions and (3) number of hours per week of speech and language therapy received. Since the assumption of homogeneity of variance was not met for these data, we used the obtained Welch’s adjusted F ratio. Post hoc, pairwise, Bonferroni-corrected comparisons were conducted for each ANOVA.
To investigate the association of child and parental characteristics with use of intervention, we conducted logistic regressions for three primary outcomes (use of any intervention; use of behavioural, developmental and relationship-based interventions and use of speech and language therapy). The predictors in each model were child’s gender, verbal ability, age in months, time passed since diagnosis and parental educational level. The three logistic regression models were first run for the total sample and then for each of the four European regions separately.
Results
Participants
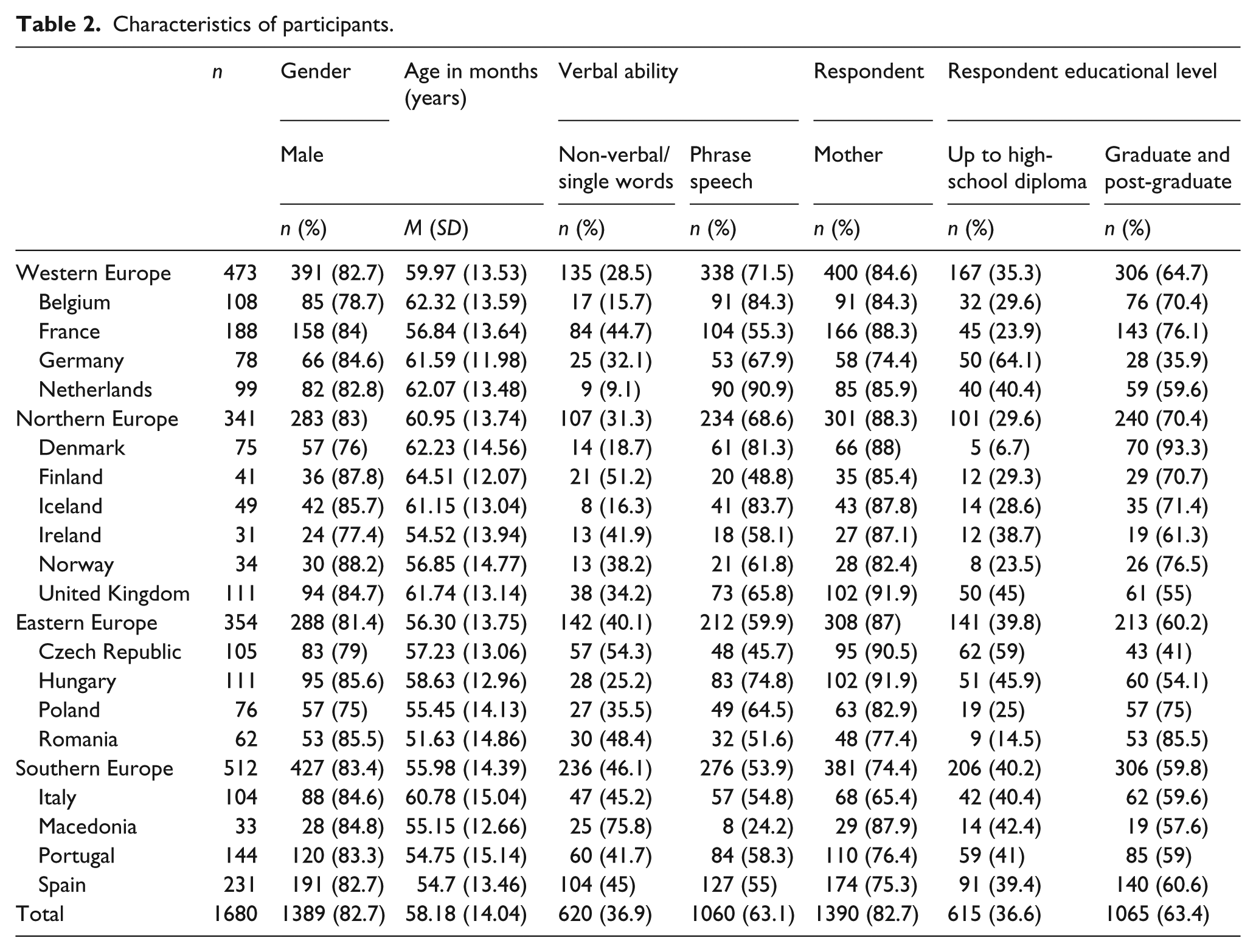
A total of 1680 families from 18 European countries participated in the study. Participation by European regions was balanced (Western Europe: n = 473; Northern Europe: n = 341; Eastern Europe: n = 354; Southern Europe: n = 512). In 83% of cases, mothers completed the survey. Overall, the educational level of respondents was high, although it varied across countries (63% of total sample had a degree or a post-graduate qualification; range: 36%–93%). In total, 83% of children with ASD were male, and the mean age was 58.18 months (SD = 14.04, range 21–83). Children’s reported ability to use at least phrase speech was 63% in the total sample and ranged from 24% to 91% across countries (Table 2).
Characteristics of participants.
Use of interventions
The majority of parents (n = 1529, 91%) reported using at least one type of intervention (M = 9.44 hours/week, SD = 11.95; Median = 5; interquartile range (IQR) = 2 to 11). However, 9% (n = 151) reported no use of intervention. The number of parents reporting using any intervention in Northern Europe (82.1%) was significantly lower than in Western Europe, Eastern Europe and Southern Europe (see Tables 3 and 4). The percentage in Western and Eastern Europe was significantly lower than in Southern Europe. The number of parents reporting not currently using any intervention ranged from 1.3% (Poland) to 29% (Ireland); in six countries, this proportion was >10% (The Netherlands, Denmark, Ireland, United Kingdom, Czech Republic, the former Yugoslav Republic of Macedonia). In the total sample, children who did not use any type of intervention did not differ by age (t(1689) = −0.591, p = 0.554), gender (χ2(1) = 0.068, p = 0.449) or verbal ability (χ2(1) = 1.025, p = 0.178.) from children using some sort of intervention. However, there were significantly more parents with a lower educational level in the group of those not using intervention (χ2(1) = 20.457, p < 0.001), as well as more children who had been diagnosed less than a year prior to survey completion (χ2(1) = 20.457, p =< 0.001).
Use and intensity of interventions.
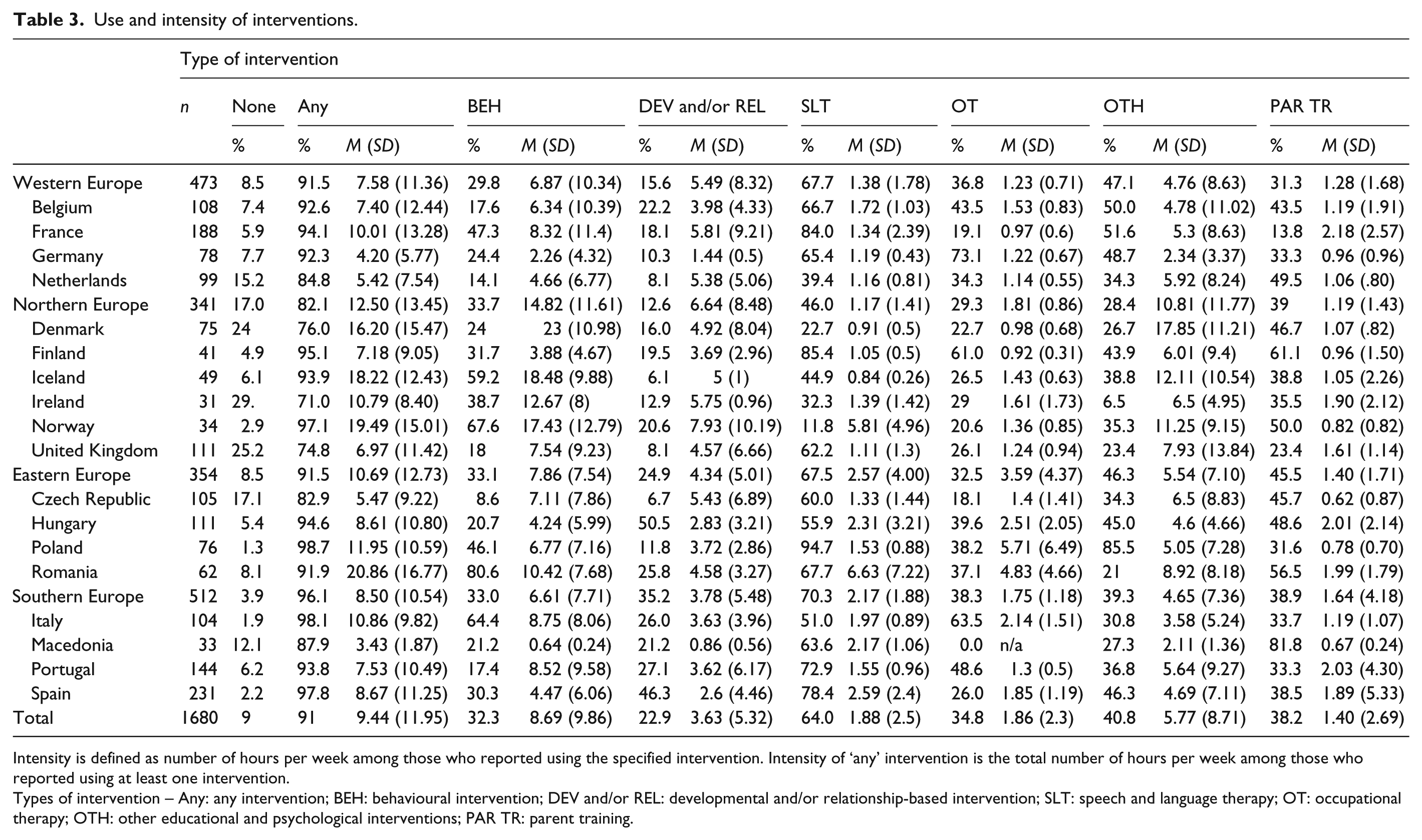
Intensity is defined as number of hours per week among those who reported using the specified intervention. Intensity of ‘any’ intervention is the total number of hours per week among those who reported using at least one intervention.
Types of intervention – Any: any intervention; BEH: behavioural intervention; DEV and/or REL: developmental and/or relationship-based intervention; SLT: speech and language therapy; OT: occupational therapy; OTH: other educational and psychological interventions; PAR TR: parent training.
Use of intervention by European regions.
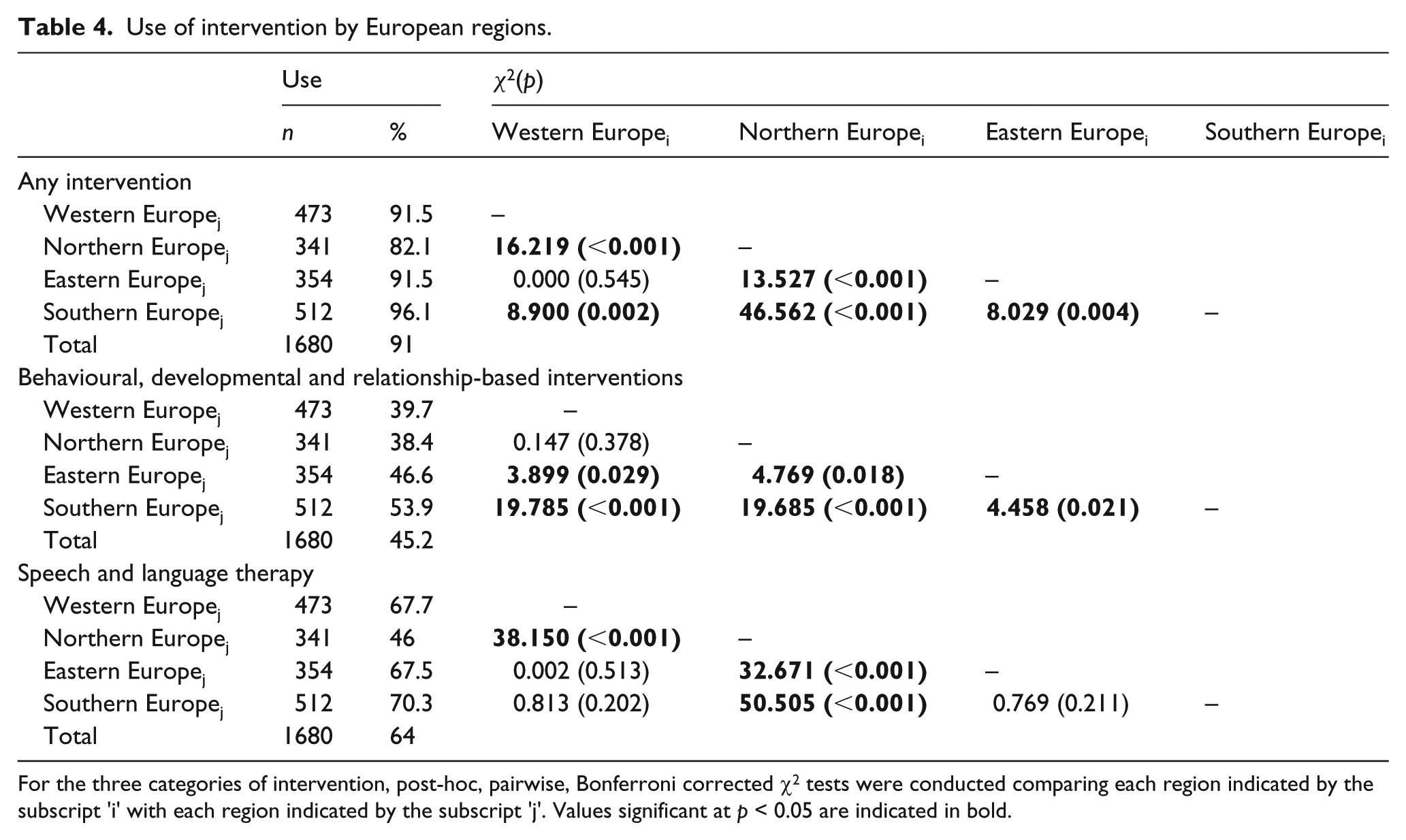
For the three categories of intervention, post-hoc, pairwise, Bonferroni corrected χ2 tests were conducted comparing each region indicated by the subscript ‘i’ with each region indicated by the subscript ‘j’. Values significant at p < 0.05 are indicated in bold.
Speech and language therapy was the most widely used intervention (64% of total sample) with a uniform pattern of use by European regions, with the exception of Northern Europe (46%) where reported use was significantly lower than in Western (68%), Eastern (68%) and Southern Europe (70%). Behavioural, developmental and relationship-based interventions were used in 45% of the sample. The proportion of parents reporting using such treatments was significantly higher in Southern Europe (54%) than in Western (40%), Northern (38%) and Eastern Europe (47%). Reported use in Western and Northern Europe was significantly lower than use in Eastern Europe (see Table 4).
ANOVA models were performed for three dependent variables: total hours per week of any intervention, hours per week of behavioural, developmental or relationship-based interventions and hours per week of speech and language therapy (Table 5). There was a significant effect of European region of residency on total number of hours of intervention used; however, the effect size was small. Post hoc comparisons using the Bonferroni test indicated that the mean hours of intervention used by children living in Western Europe (M = 6.94, SD = 11.07) was significantly lower than the mean hours used by children living in Northern Europe (M = 10.26, SD = 13.09) and Eastern Europe (M = 9.79, SD = 12.54).
Amount of intervention by European regions.
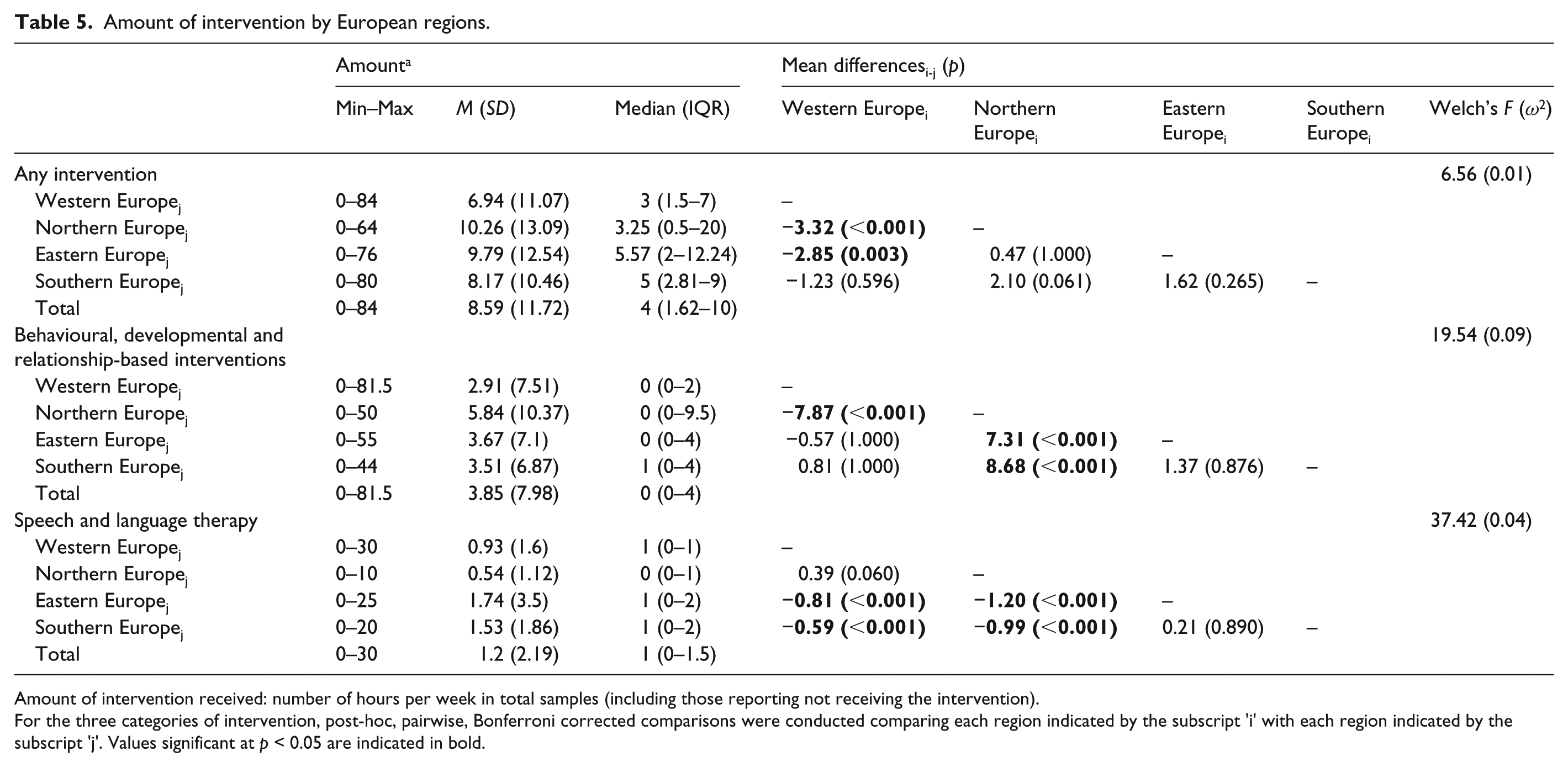
Amount of intervention received: number of hours per week in total samples (including those reporting not receiving the intervention).
For the three categories of intervention, post-hoc, pairwise, Bonferroni corrected comparisons were conducted comparing each region indicated by the subscript ‘i’ with each region indicated by the subscript ‘j’. Values significant at p < 0.05 are indicated in bold.
A significant effect of region was also found on number of hours of behavioural, developmental or relationship-based interventions with a medium effect size as well as on number of hours of speech and language therapy, where the effect size was small. For the behavioural, developmental or relationship-based interventions, post hoc comparisons indicated that the mean hours used by children living in Northern Europe (M = 5.84, SD = 10.37) was significantly higher than the mean hours used by children living in Western Europe (M = 2.91, SD = 7.51), Eastern Europe (M = 3.67, SD = 7.1) and Southern Europe (M = 3.51, SD = 6.87). For speech and language therapy, post hoc comparisons indicated that the mean hours used by children living in Western Europe (M = 0.93, SD = 1.60) and Northern Europe (M = 0.54, SD = 1.12) were significantly lower than the mean hours used by children living in Eastern Europe (M = 1.74, SD = 3.50) and in Southern Europe (M = 1.53, SD = 1.86).
Predictors of use of intervention
Logistic regression models were performed for three outcomes: use of any intervention, use of behavioural, developmental or relationship-based interventions and use of speech and language therapy (Table 6). The models were run first in the total sample and were then repeated on four subsamples based on the European regions. All models’ χ2 statistics were significant (ps ranged < 0.001 to 0.048), except for the model predicting use of any intervention in Northern Europe (p = 0.187), which was therefore rejected. The Hosmer and Lemeshow goodness-of-fit test was not significant (hence indicating well-fitting models) for all remaining logistic regressions except for the model predicting use of any intervention in the whole sample (p = 0.041), and this model was rejected too. Nagelkerke’s R2 for the remaining models ranged from 0.04 to 0.13, which is an indication that several other relevant variables had not been included in the models. Table 5 reports the odds ratios and 95% confidence intervals (CIs) for the predictors and the models’ statistics.
Predictors of use of interventions.
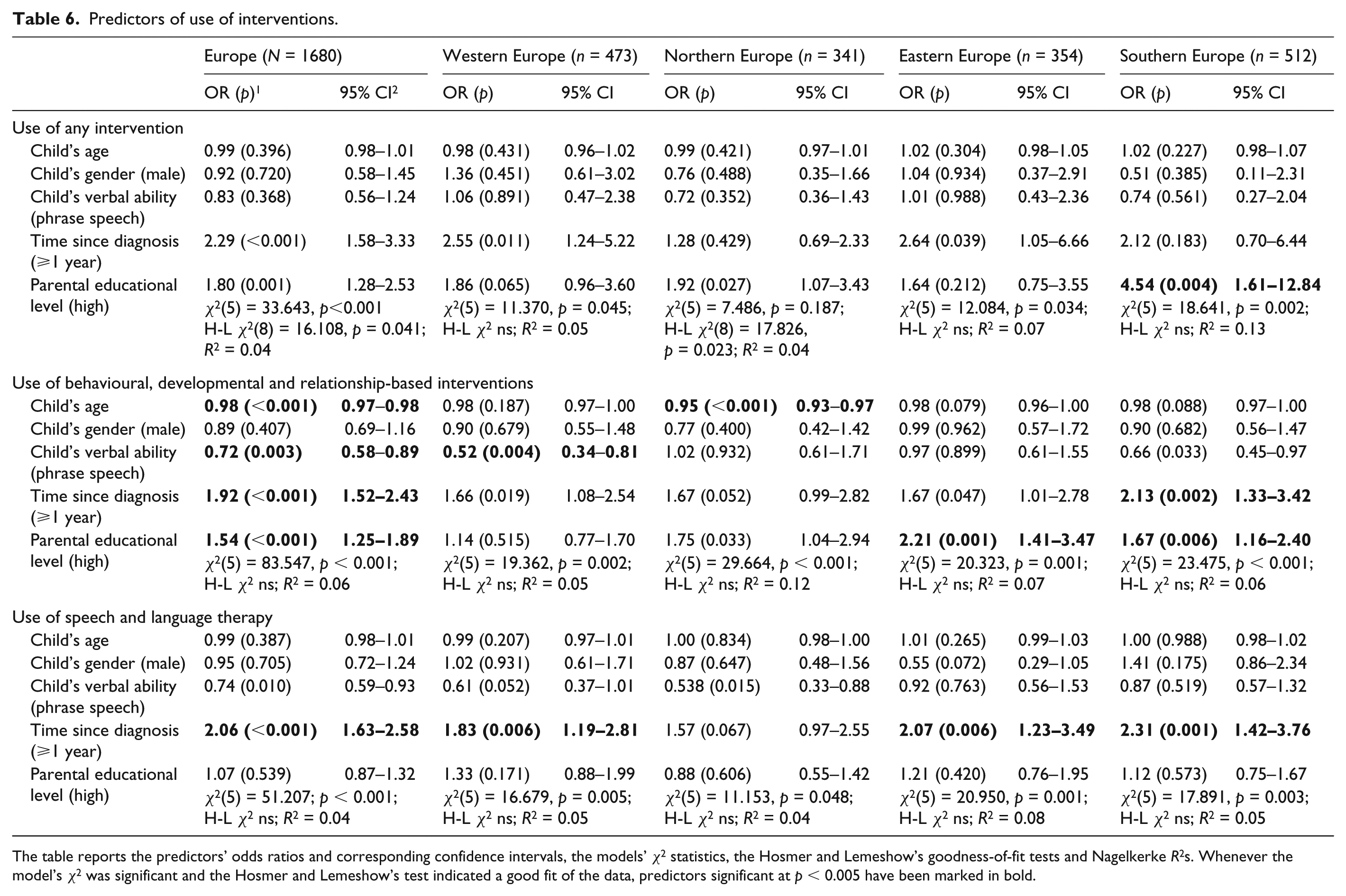
The table reports the predictors’ odds ratios and corresponding confidence intervals, the models’ χ2 statistics, the Hosmer and Lemeshow’s goodness-of-fit tests and Nagelkerke R2s. Whenever the model’s χ2 was significant and the Hosmer and Lemeshow’s test indicated a good fit of the data, predictors significant at p < 0.005 have been marked in bold.
Use of any intervention
In Southern Europe, controlling for child age, gender and verbal ability and for time passed since diagnosis, a high parental education level significantly increased the odds for the child to use at least one type of intervention (OR = 4.54, p = 0.004; 95% CI = [1.61, 12.84]). No associations between the predictors and use of at least one type of intervention were found for the other European regions. Time passed since diagnosis and parental educational level were found to be significantly associated with use of any intervention in the total sample; however, the Hosmer and Lemeshow’s goodness-of-fit test of the model indicated that the model’s estimates did not fit the data at an acceptable level.
Use of behavioural, developmental or relationship-based interventions
In the total sample, controlling for child age, gender, verbal ability and time passed since diagnosis, a high parental educational level significantly increased the odds for the child to use behavioural, developmental or relationship-based interventions (OR = 1.54, p < 0.001; 95% CI = [1.25, 1.89]). The same effect was found for Eastern (OR = 2.21, p < 0.001; 95% CI = [1.41, 3.47]) and Southern Europe (OR = 1.67, p = 0.006; 95% CI = [1.16, 2.40]), but not for Western and Northern Europe. A longer time passed since diagnosis (⩾1 year) was also associated with a significant prediction for use of behavioural, developmental or relationship-based interventions in the total sample, but when examining the regional subsamples, the prediction was significant in Southern Europe only (OR = 2.13, p = 0.002; 95% CI = [1.33, 3.42]).
Among child characteristics, verbal ability was a significant predictor in the total sample (OR = 0.72, p = 0.003; 95% CI = [0.58, 0.89]) and in Western Europe only (OR = 0.52, p = 0.004; 95% CI = [0.34, 0.81]), with non-verbal children and children with single words at an increased likelihood to use behavioural, developmental or relationship-based interventions compared with those with phrase speech. Child age was a significant predictor for use of such interventions in the total sample (OR = 0.98, p < 0.001; 95% CI = [0.97, 0.98]) and in Northern Europe (OR = 0.95, p < 0.001; 95% CI = [0.93, 0.97]), with younger children more likely to use these interventions.
Use of speech and language therapy
Time passed after receiving the diagnosis was the only significant independent factor for use of speech and language therapy in the total sample, with children diagnosed more than 1 year before the survey more likely to use it (OR = 2.06, p < 0.001; 95% CI = [1.63, 2.58]). The same effect was found in Western (OR = 1.83, p = 0.006; 95% CI = [1.19, 2.81]), Eastern (OR = 2.07, p = 0.006; 95% CI = [1.23, 3.49]) and Southern Europe (OR = 2.31, p < 0.001; 95% CI = [1.42, 3.76]), but not in Northern Europe.
Discussion
The aim of this study was to obtain an overview of use of intervention per week among parents of young children with ASD across 18 European countries. The survey, the largest conducted worldwide (N = 1680), is the first to report data on a European sample. The recruitment method, an online survey distributed via national parents associations, was selected to reach the largest possible number of families in a systematic fashion across Europe and therefore maximise the representativeness of the sample. A number of steps were undertaken to minimise the potential bias associated with the translation and adaptation of the survey in 18 different languages, including using local terminology to describe treatments, where available, and the employment of consensus methods in the group of expert clinicians and researchers involved in the development of the questionnaire.
The study has identified a diverse pattern of use of intervention across Europe both in terms of type and amount of intervention received. It has also demonstrated that use of intervention is associated with parental educational level as well as child characteristics. Moreover, this study identified for the first time differential patterns of therapy utilisation in the West, North, East and South areas of Europe. These regional groupings, codified as such in the United Nations geoscheme, are not simply defined by geographical proximity, but are also characterised by similar economic and cultural background. Our approach allowed us to identify patterns of intervention use for children with autism that can potentially inform health and economic policies, now increasingly applied at a supranational level such as in programmes promoted within the European Union (EU, 2013).
A number of relevant findings emerged. First, almost 1 in 10 parents who took part in the survey reported that their child was not currently receiving any type of intervention. At a country level, there was large variation in the overall use of intervention. The proportion of children not receiving any intervention was more than 20% in Denmark, Ireland and the United Kingdom, between 10% and 20% in The Netherlands, Czech Republic and the former Yugoslav Republic of Macedonia, and less than 10% in the rest of the countries. This figure is much lower than the rate reported by Bowker et al. (2011), the only study reporting on use of any type of intervention (23% in North America and 43% in a smaller sample, n = 63, from Europe and other background). This and other differences in our results might be due to sampling bias and the different recruitment methods employed in our and other studies, as well as availability of different interventions. However, it should also be noted that we enquired about a greater range of interventions (for example, parent training was not included in the Bowker et al. survey) in a much larger sample.
Children not receiving any type of intervention did not differ by age, gender or verbal ability, but in this group there were significantly more children whose parent had a lower educational level and more children who had been diagnosed less than a year before survey completion. Nonetheless, the overall estimated probability of not using any type of intervention based on child and parental characteristics considered together did not accurately fit the data at a European level. Notably though, when examining the estimates by European regions, we identified a strong association of parental educational level with use of intervention in Southern Europe only, where children whose parent had a lower educational level were four times less likely to use any intervention. This finding is particularly striking considering that the parents who took part in our survey had, on average, a significantly higher educational level than the general population. This suggests that in the general population, an even wider proportion of children with ASD might not be using any intervention.
In terms of crude amount of total hours of intervention received, children in Western Europe received overall significantly less hours of intervention than children in Northern Europe and Eastern Europe. In line with previous findings in the United States (Goin-Kochel et al., 2007; Green et al., 2006), in our sample speech and language therapy stood out as the most common intervention for the majority of children in all Europe (range 68%–70%), with the exception of Northern Europe (46%). While speech and language therapy was used by a smaller number of children in Northern Europe, the overall amount received in that region was comparable to the amount received in Western Europe and only slightly less than in Eastern and Southern Europe (between 1 and 2 hours less). No association between child or parental characteristics and use of speech and language therapy was found in Northern Europe; however, in the rest of Europe, children who had been diagnosed at least 1 year prior to survey completion were twice more likely to use this intervention. These results are not surprising given that speech and language therapists are usually part of paediatric or psychiatric services within the national health systems in some countries and/or part of school and education system in others. We did not collect information on the providers of intervention, but it is reasonable to presume that in most cases, speech and language therapy had been provided by the respective national health or educational systems. This may explain why speech and language therapy is consistently reported as the most frequently used intervention in different studies (Barrett et al., 2012; Goin-Kochel et al., 2007; Green et al., 2006). Alternatively, this might reflect parents’ choices or professional advice as language difficulties often are among the first concerns and therefore may be identified as priority targets for intervention following diagnosis. The association of time passed since the diagnosis with use of speech and language therapy might represent waiting lists or other systemic factors, such as bureaucracy, that delay use of intervention. In some countries, speech and language therapy is also provided in schools or other day care settings. Therefore, although parents were instructed to include all settings where the child might have received intervention while completing the survey, we cannot exclude the possibility that in some countries parents may not have reported their child receiving speech and language therapy because they considered it as an integral part of the school curriculum. This might have influenced our results, particularly the finding that speech and language therapy was less used in Northern Europe.
A different pattern emerged when considering the use of behavioural, developmental and relationship-based interventions. Behavioural interventions were used by a third of the sample overall, with equal distribution by European region but much wider range by country. Developmental and relationship-based approaches were more commonly used in Southern and Eastern Europe. All these treatments, combined together, represented the second most used type of intervention (55% in the total sample). The proportion of children receiving these interventions was fairly similar across Europe (Southern 54%, Eastern 47%, Western Europe 40%, Northern Europe 38%) but on average children in Northern Europe received between 8 and 9 more hours per week than the children in the rest of Europe (for those using the intervention, the mean reported hours were 15 in Northern Europe and between 6 and 8 for the rest of Europe).
Moreover, we identified some differences by region of residence in the factors predicting use of these interventions. Child characteristics predicted use of behavioural, developmental and relationship-based interventions in Northern and Western Europe: younger children and children who had not developed phrase speech were, respectively, more likely to be using such interventions in those regions of Europe. However, a higher parental educational level predicted increased likelihood of using such interventions in Eastern Europe and in Southern Europe; in the latter, time passed since the diagnosis was also an independent predictor of use of intervention. The available data cannot tease out the nature of the associations between child characteristics and use of intervention in Western and Northern Europe; for example, this might be due to services prioritising younger or more impaired children, or parents of such children might be more motivated to use specific interventions. As far as Southern and Eastern Europe are concerned instead, the association of parental educational level with use of behavioural, developmental and relationship-based interventions (but not with speech and language therapy) regardless of children’s needs might be an indication that these interventions are not provided by public national health systems and have to be found and paid directly by the families. Educational level of adults is in fact a common proxy for socioeconomic status (SES) in the literature and its relation with occupational status and income is well established (Bradley and Corwyn, 2002). In a US sample of 70 parents of children with ASD aged 6 years or younger enrolled in a parent advocacy group, parental educational attainment predicted higher service utilisation (Siller et al., 2014). Our study replicates this finding of a significant association of parental educational level with use of intervention on a non-US large-scale sample; additionally, our study suggests that, at least in Europe, this effect might vary by area of residence.
In the absence of systematic information on differences and similarities in national health and educational policies across Europe, it is not possible to speculate on which might be the most influential factors driving the differences in service use we found. However, our finding that in Southern and Eastern Europe children of individuals with a lower educational level had considerably fewer chances of using interventions suggests per se that there are health inequalities in Europe in respect to intervention for ASD. This is something that policy makers in Europe, both at a national and a union level, need to be made aware of. Furthermore, finding such an effect in this highly educated sample raises the possibility that the gap in terms of use of intervention between richer and poorer sectors of society in Eastern and Southern Europe might be even wider in the general population.
While there is scientific consensus over the fact that children with ASD should receive individualised, multi-dimensional and multi-disciplinary interventions, the reality is that in our survey significant parts of the population report no or limited use of therapy. Whether this is because some parents have few opportunities to know how to access behavioural, developmental and relationship-based interventions, or whether such interventions are generally not publicly funded and hence available to families only via their own funds, considerable policy and service development is required across Europe to ensure that communities are consistent with the rights of children with disabilities to access health and education (UN, 2007). More research is needed to further explore the role of socioeconomic factors in use of interventions, and whether a similar pattern is found in other parts of the world.
Limitations and future directions
Several limitations of the study need to be acknowledged, many shared by previous research conducted on this subject. The recruitment method chosen (online survey distributed by parent associations) might have been prone to selection bias, as research has shown that parents of children with autism involved in support groups are likely to have a relatively high income and educational level (Mandell and Salzer, 2007) and that access to Internet in Europe is still a function of socio-demographic characteristics (Vicente and López, 2011). Our sample was in fact characterised by an unusually high educational level: 63% of respondents of our survey (for the vast majority women) reported having a graduate or post-graduate educational level. Data from the European Commission on tertiary education attainment in females for the year when the survey was completed (2012) show that only 40% of European women in the age range 30–34 years have an education level above secondary schooling (Eurostat, the Statistical Office of the European Union, 2014). While this is a limitation shared by previous studies (for example, in the V. Green et al. study, 88% of the sample had an educational level beyond high school), this may limit the generalisability of our results to the European population. Moreover, since recruitment was conducted locally by each national association, differences in the outreach of each organisation might have influenced sampling and, although relatively uniform at a regional level, sample sizes at a country level varied considerably. Critically, we do not know how representative the parents who responded to our survey were of service utilisation more generally within each community, and whether in some countries certain sectors of the population were particularly underrepresented. It is likely that parents enrolled in parents’ associations are more active and successful in seeking and accessing intervention. However, while this recruitment strategy was potentially bound to bias, it allowed us to reach a large number of families in a wide range of countries, making this study the largest conducted to date on the topic and the first providing systematic data for Europe.
Our study was also limited by the use of cross-sectional data, which do not facilitate exploration of whether our results represent an age or cohort effect influenced by economic contingencies in Europe. Furthermore, although educational level is a common proxy for SES, future studies need to examine whether the present results hold also for other indicators, such as household income or parental occupation. The interpretation of our finding has also been limited by the lack of information on the type and amount of services available publicly via the national health systems in each country, as opposed to privately accessed interventions. In addition, it was not possible to separate out the contexts where intervention was provided, particularly in respect to intervention provided in school or day care settings, and this may have limited the interpretation of our findings. While there is some evidence of lack of uniformity in the public provision of services for children with disabilities across Europe (Ballesteros et al., 2013), more detailed cross-national comparisons of health and educational systems, which would have allowed us to better interpret our findings, are not available. Data from existing and future international cooperation programmes are needed to better understand and address possible inequalities in use of intervention for autism. Further EU initiatives to strengthen the scientific cooperation among European countries are needed in order to conduct trans-European studies that can employ more resource-intensive recruitment methods that are likely less prone to selection bias and can contribute to overcome the limitations of the present study and previous research on the topic.
Finally, reliance on parent report in the absence of direct assessments places a limitation on these findings in relation to severity of symptoms and behavioural characteristics. Furthermore, no attempt was made to collect information on additional determinants of service use. For example, the presence of comorbid disorders in children with ASD is likely to influence intervention usage, but we did not enquire about comorbidities. Future prospective studies are needed to understand the patterns of intervention use in childhood taking into account the educational as well as the clinical settings where intervention is provided. To keep the survey to a minimum and maximise completion rate, we chose not to directly enquire about the accessibility of various interventions and why parents did or did not use certain interventions. In retrospect, the availability of such direct information would have been very valuable to interpret the variability found across regions in intervention usage. In future studies, parents should be explicitly asked for the reasons underlying not using (certain) interventions. This is necessary in order to be able to distinguish personal choices (e.g. not agreeing with the philosophy of the intervention), from lack of availability (interventions not being distributed in the area), barriers to access (e.g. waiting lists or costly interventions solely provided privately) or knowledge barriers (parents not knowing of the existence of certain interventions). Future work may also include further exploring the regional variations by analysing the results per country, taking into account the respective national health systems and exploring the different patterns of public versus private provision of services in each country that might have affected our findings.
Conclusion
In conclusion, our study showed that in the Eastern and Southern regions of Europe, more educated parents are more successful than parents with lower educational level in obtaining use of specialist interventions that could improve the outcomes of children with autism. This finding is particularly notable since, as outlined above, our sample had a higher education level than the general European population. Moreover, it appeared that even relatively low-cost and commonly publicly funded interventions such as speech and language therapy are not immediately available for the majority of families, as in all Europe (except for Northern Europe), children recently diagnosed were only half as likely to use intervention as children diagnosed at least 1 year prior to survey completion.
Our data also showed a considerable variability in the amount of intervention used across countries with the overall mean of the whole sample being 9 hours per week. While there is little scientific evidence on what constitutes the appropriate number of hours per week necessary to obtain long-lasting positive outcomes, some guidelines give explicit recommendations (at least 25 hours per week: Myers and Johnson, 2007). Other guidelines, such as the Practice Parameters released by the American Academy of Child and Adolescent Psychiatry (Volkmar et al., 2014), do not include a specification of the amount of the ‘appropriate, evidence-based, and structured educational and behavioral interventions’ (p. 244) recommended, and low-intensity (and therefore more sustainable in the real settings) versions of well-established models (Dawson et al., 2010) are just beginning to be tested (Vismara et al., 2009).
At a societal and political level, our study highlights the pressing need to address inequalities in access to healthcare. Training professionals in the community, particularly those employed in national health and educational systems, to early diagnose and treat ASD is crucial to ensure that families are not left alone in dealing with their child’s difficulties. Parent support strategies should be implemented, involving the civil society in an inclusive model of awareness. Public services need to be empowered in terms of funds and resources in order to guarantee timeliness and continuity in the provision of intervention and education. In the economic uncertainty that characterises these times, it is vital to ensure that sound and scalable interventions are tested in international collaborative efforts and then implemented in the communities across Europe. The implementation of methodologically rigorous RCTs of interventions that are realistically implementable within the constraints of school and clinic services in Europe will provide evidence on the ‘minimum critical amount’ needed to make long-lasting improvements in outcome. Research findings should, in turn, inform future policy and practice guidelines for treatment provision for all young children with autism across Europe.
Footnotes
Appendix 1
Acknowledgements
We are grateful to all the parents who participated in the study and to the parent associations that were involved in recruiting the participants.
Funding
This research was supported by COST Action BM1004 funded by the European Science Foundation. TC and JG also received support from the Innovative Medicines Initiative Joint Undertaking under grant agreement no. 115300, resources of which are composed of financial contribution from the European Union’s Seventh Framework Programme (FP7/2007–2013) and EFPIA companies’ in-kind contribution.