
Abstract
Anxiety and stress are everyday issues for many people with high-functioning autism, and while cognitive-behavioural therapy is the treatment of choice for the management of anxiety, there are challenges in using it with people with high-functioning autism. This study used modified experience sampling techniques to examine everyday anxiety and stress in adults with high-functioning autism and to explore the feasibility of delivering real-time stress management techniques using a mobile platform. High levels of anxiety were found to be characterised by worry, confusing thoughts and being alone but was not associated with internal focus, imagery or rumination. Participants reported improved mood and less worry and anxious thinking in the active phase of the study. These results support previous studies indicating that people with high-functioning autism differ in their experience of anxiety and provided preliminary data on the feasibility of real-time stress management. The limitations of this approach are discussed together with considerations for future work in the area of developing clinical interventions on mobile platforms.
Introduction
People with autism spectrum conditions (ASCs) have a life-long vulnerability to health difficulties, including anxiety, mood disorders and psychosis (Skokauskas and Gallagher, 2010), a tendency that increases in people with high-functioning autism 1 (HFA; White et al., 2009), possibly due to increased expressive abilities (Howlin, 1997) and/or social functioning and self-awareness (Sterling et al., 2008). Anxiety disorders are the most prevalent mental health problem in both children (Van Steensel et al., 2011) and adults (Skokauskas and Gallagher, 2010). Autobiographical accounts also provide support that anxiety and stress are common everyday experiences for individuals with HFA (e.g. Dubin, 2009).
Given the characteristics common to people with HFA and issues relating to coping with everyday issue in everyday contexts (Gaus, 2011), the use of technology-based interventions, ranging from virtual reality environments to mobile platforms (Grynszpan et al., 2014) to mobile technology such as the personal digital assistant (PDA), would appear to be worthy of consideration. PDAs are ideal in that they can readily accommodate suggested modifications for working therapeutically with individuals with autism spectrum (AS) (Moree and Davis, 2010), are primarily a visual medium and allow individuals to have control to work at their own pace. Moreover, the use of PDAs allows for repetition and provides the opportunity for individuals to build up coping skills within the everyday environment, which is particularly important when considering the consolidation of principles via computer-delivered interventions (Clough and Casey, 2011). Such mobile technology can function as a ‘coach’, providing prompts in real time (i.e. throughout the day and across environments), and such strategies have been suggested to aid the generalisation of skills (e.g. Cardaciotto and Herbert, 2004; Hare, 2013; Weiss and Lunsky, 2010). PDAs may be more suitable as they remove the social demands of therapeutic work and reduce reliance on memory, which may be problematic given the difficulties with autobiographical memory common among individuals with HFA. Furthermore, programmes can be designed in such a way that techniques can be reduced to step-by-step directions that are applicable across situations and provide a structured and consistent approach.
Experience Sampling Methodology (ESM) is an approach to assessment that captures moment-to-moment cognitive and behavioural events (Delespaul, 1995; Hektner et al., 2007). It is useful for exploring idiosyncratic experiences and for investigating individual differences (e.g. thoughts, feelings, behaviour) and phenomena that vary across individuals, time and context. It typically involves completing questionnaires in response to a signal (e.g. beep) at random or pre-determined intervals over time. ESM has been used extensively, in various forms (i.e. paper, computerised), to explore everyday experiences related to anxiety and mood disorders, bipolar disorder and psychosis (see Palmier-Claus et al., 2011 for review). However, only a handful of studies have used such approaches to explore the daily lives of individuals with ASCs (Chen et al., 2013; Hare et al., 2015; Hintzen et al., 2010; Hurlburt et al., 1994), and research has only recently begun to explore the use of ESM in the delivery of real-time intervention (e.g. Myin-Germeys et al., 2011).
The primary aim of this study was to act as a ‘Proof of Principle’ study with regard to the use of PDAs to deliver what was termed real-time stress management (RTSM) for everyday stress in people with HFA. The study had two formal hypotheses:
Hypothesis 1. There will be a reduction in the mean subjective rating of anxiety from the Baseline phase to the RTSM phase (i.e. 3 Baseline days vs 3 RTSM days).
Hypothesis 2. There will be a reduction in subjective ratings of anxiety after a stress management technique has been employed (i.e. pre- vs post-intervention ratings).
Method
The study was exploratory using an AB case series design with (a) a baseline phase of 3 days in which participants completed a PDA questionnaire (Hare et al., 2015) in response to random beeps (10 per day, between 10:00 a.m. and 4:00 p.m.) to examine thought content, form of thought, attentional style, length of rumination and level of subjective anxiety, and (b) the RTSM phase of 3 days in which participants also completed a RTSM programme via the PDA, delivered in the same way as the baseline phase. Stress management techniques were presented if and when participants indicated a high level of anxiety, as determined by the responses on the PDA questionnaire. Measures of anxiety and depressive symptoms were administered at the beginning and end of the 6 days.
This study received ethical approval from the University of Manchester School of Psychological Sciences Ethics Committee and the National Autistic Society.
Recruitment
Participants were recruited via the National Autistic Society website and from local support groups in North West England. Inclusion criteria were a verifiable diagnosis of HFA from a psychologist or medical practitioner using Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV), Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) or International Statistical Classification of Diseases and Related Health Problems–10th Revision (ICD-10) criteria; aged between 18 and 65 years; a full-scale IQ (FSIQ) score within the non-intellectual disability range; fluency in English; and verbal comprehension equivalent to 9 years or above.
Measures
Autism Spectrum Quotient
Autism Spectrum Quotient (AQ) is a 50-item assessment of autism spectrum disorder (ASD) features in individuals without intellectual disability (Baron-Cohen et al., 2001). A cut-off score of 32 is taken as identifying adults with HFA within the general population (Baron-Cohen et al., 2001), although a more conservative threshold (26) has been suggested for use in ‘clinic referred populations’ (Woodbury-Smith et al., 2005).
Hospital Anxiety and Depression Scale
A 14-item measure of anxious and depressed feelings rated on a 4-point scale with a cut-off score of 8 for both sub-scales taken as indicating clinical anxiety or depression (Zigmond and Snaith, 1983), the Hospital Anxiety and Depression Scale (HADS) has been used previously in research with people with HFA (e.g. Abell and Hare, 2005).
Wechsler Abbreviated Scale of Intelligence
Wechsler Abbreviated Scale of Intelligence (WASI) (Wechsler, 1999) is a measure of general intellectual ability, comprising four subtests (Vocabulary, Similarities, Block Design and Matrix Reasoning), yielding Verbal IQ (VIQ), Performance IQ (PIQ) and FSIQ-4 scores. The British Picture Vocabulary Scale II (BPVS II, Dunn et al., 1997) was used to assess receptive verbal ability in Standard English.
The PDA Questionnaire was developed in a previous study (Hare et al., 2015) and involved 13 questions, with appropriate response formats (e.g. ‘open text’, ‘multiple choice’ and ‘analogue scale’) to explore the daily experience of anxiety in adults with HFA (Appendix 1). The RTSM approach was developed for this study, with participants being presented with various stress management strategies and explicit instructions when their reported subjective anxiety levels were high (i.e. ⩾3 on question 8) and included Relaxation, Attention Shifting, Deep Breathing, Positive Self-Talk and Positive and Distracting Imagery. Such strategies have been shown to be effective in technology-based management of anxiety (e.g. Newman et al., 1996, 1999; Riva et al., 2007) and have been recommended to improve coping among individuals with ASDs (e.g. Attwood, 2004; Gaus, 2007). There were no a priori grounds for prioritising one technique over another, and so participants were allowed to exercise their own preference in the RTSM phase. The content of the RTSM is shown in Appendix 2, and questionnaire and sampling design were in accordance with recommendations for ESM studies (Palmier-Claus et al., 2011).
Each participant was provided with a Palm Pilot (m500 Series) on which to record daily responses to the questionnaires running on iESP software (Intel Research Center, Seattle). Participants had 60 s to respond to a beep to complete a questionnaire and did not have access to previous questions or responses. Each question took approximately 2 min to complete, and the PDA was programmed to beep pseudo-randomly 10 times during the day (i.e. 10:00 a.m. to 4:00 p.m.). All participants were shown how to use the PDA and the RTSM programme, and all of the options were demonstrated and discussed in advance.
Results
Sample
In all, 14 participants started the study, with four dropping out within 3 days due to technical problems and one lost contact. The final sample (N = 9) comprised five men and four women with diagnoses of HFA with mean FSIQ score = 120 (standard deviation (SD) = 7.35, range = 110–131), mean reading ability age equivalent = 16.09 years (SD = 1.27 years, range = 13.5–17.0 years) and mean AQ score = 36.78 (SD = 7.48, range = 27–47). Baseline HADS scores indicated anxiety within the moderate to severe range (mean = 11.11; SD = 3.62; range = 7–17) and depression within the non-clinical range (mean = 3.89; SD = 2.85, range = 0–9). Most participants (N = 7) were taking psychotropic medication, primarily anti-depressants, for the management of anxiety and/or low mood symptoms for at least 6 months. Seven had previously engaged with mental health services, primarily for diagnostic assessment of HFA, and five had previously received cognitive-behavioural therapy.
Analyses
Data were transferred from the PDAs via a ‘Hot Sync’ function to a personal computer (PC) for analysis after each 3-day period. Data were included if participants completed a minimum of 20 reports (i.e. one-third of the total) within each 3-day phase, which constitutes the minimum recommended amount of valid ESM data over 6 days (Palmier-Claus et al., 2011).
Data were coded independently by a second rater to ensure inter-rater reliability and were initially analysed at a descriptive level to investigate the phenomenology of anxiety. Specific variables (i.e. ‘thought’, ‘doing’) were manually coded before inclusion in analyses. Thoughts were coded manually into focus, content and anxious (Hektner et al., 2007). Focus referred to whether a thought was internally (e.g. ‘I’m tired’) or externally (e.g. ‘I was thinking about a game on my Nintendo DS’) directed. Content referred to whether the thought involved another person and anxious referred to whether thoughts were coded as anxious, independent of the participant’s appraisal. Furthermore, responses regarding what the participants were doing when the PDA beeped were categorised as social (e.g. ‘Talking to my support worker’) or activity (e.g. ‘Doing housework’) (Hintzen et al., 2010). Work was not used as code as most participants were unemployed. Inconsistencies between raters were resolved and kappa values for inter-rater agreement were computed for focus (0.63; p < 0.0005), content variable (0.94; p < 0.0005), anxious (0.79; p < 0.0005), social (0.88; p < 0.0005) and activity (0.93; p < 0.0005).
Chi-square analyses and odds ratios (ORs) were used to determine which variables were associated with the subjective experience of elevated anxiety. To examine the impact of the RTSM intervention, subjective ratings of anxiety were aggregated by phase (i.e. Baseline, RTSM) and by day (i.e. Baseline: Day 1, Day 2, Day 3) and compared using repeated-measures Wilcoxon signed-rank test. Pre- and post-technique anxiety ratings in the RTSM phase were compared to assess whether there was a significant decrease in anxiety levels. All participants completed at least 33% of the questionnaires over the 6-day data collection period. However, an overall mean completion rate of 60.6% (range = 39.1%–88.7%) resulted in a sizeable amount of missing data being omitted from subsequent analyses.
Data derived from ESM approaches are nested within three levels (beeps, days and individuals), and therefore, hierarchical and statistical analyses must take into account the lack of independence within data points. Although multilevel modelling is considered the most appropriate approach for ESM data (see Schwartz and Stone, 1998; Scollon et al., 2003), the small sample meant this was not appropriate. Aggregation removes the impact of participant effects (i.e. dependence of repeated observations within subjects) and was thus deemed the most appropriate method of analysis for this data set. Data were analysed with SPSS Version 16 (SPSS Inc., 2007).
Phenomenology
Frequency and percentage of thought types in both phases are presented in Table 1. For these and all subsequent analyses, the phi coefficient was taken as indicative of the effect size, with a range from −1.0 (strong negative association) to +1.0 (strong positive association). A negative phi coefficient indicated that the variables were inversely associated. In the Baseline phase, thoughts were mostly appraised as worrying (25.71%), followed by practical (23.43%) and annoying (12.57%). In contrast, in the RTSM phase, most thoughts were appraised as practical (40.54%), worrying (13.51%) and neutral (10.81%), with significantly more practical (OR = 2.23; 95% confidence interval (CI) = 1.34–3.71) and fewer worrying (OR = 0.45; 95% CI = 0.24–0.84) thoughts in the RTSM phase. More thoughts were coded as involving another person in the Baseline phase (OR = 3.21; 95% CI = 1.61–6.08).
Frequency of thought type throughout Baseline and RTSM phases.
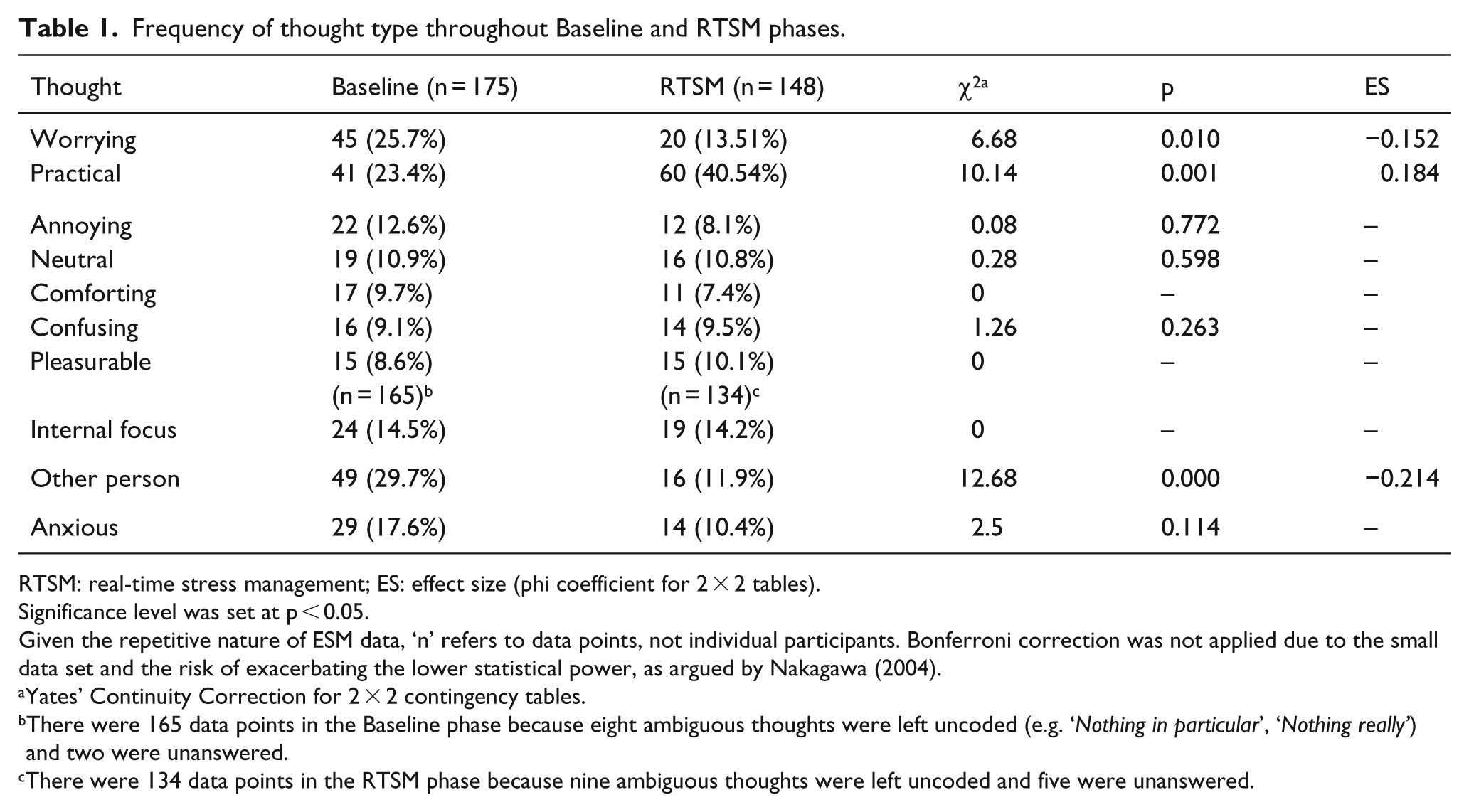
RTSM: real-time stress management; ES: effect size (phi coefficient for 2 × 2 tables).
Significance level was set at p < 0.05.
Given the repetitive nature of ESM data, ‘n’ refers to data points, not individual participants. Bonferroni correction was not applied due to the small data set and the risk of exacerbating the lower statistical power, as argued by Nakagawa (2004).
Yates’ Continuity Correction for 2 × 2 contingency tables.
There were 165 data points in the Baseline phase because eight ambiguous thoughts were left uncoded (e.g. ‘Nothing in particular’, ‘Nothing really’) and two were unanswered.
There were 134 data points in the RTSM phase because nine ambiguous thoughts were left uncoded and five were unanswered.
The frequencies of thought form for both phases are shown in Table 2, with a similar distribution across both, with most thoughts being described as ‘talking to myself’ followed by ‘like an image’. There were no significant differences between phases.
Frequency of form of thought over baseline and RTSM phases.

RTSM: real-time stress management; ES: effect size.
Frequencies of duration, regularity and novelty of thought, as well as mood and anxiety ratings, are shown in Table 3. The greatest proportion of thoughts in the Baseline and RTSM phases was rated as lasting between 1 and 5 min and was reported as frequent and typical. Participants rated mood as ‘happy’ the majority of time in both phases (Baseline: 68.1% vs RTSM: 85.8%), although this was significantly more often in the RTSM phase. Participants also more often reported elevated subjective anxiety in the Baseline phase (66.3% vs 34.5%). ORs revealed that participants were 3.24 times (95% CI = 1.79–5.87) more likely to rate mood as ‘happy’ and were only 0.27 times (95% CI = 0.16–0.44) as likely to experience elevated anxiety in the RTSM phase.
Frequency of thought duration, regularity of thought, mood, anxiety and novelty of thought.
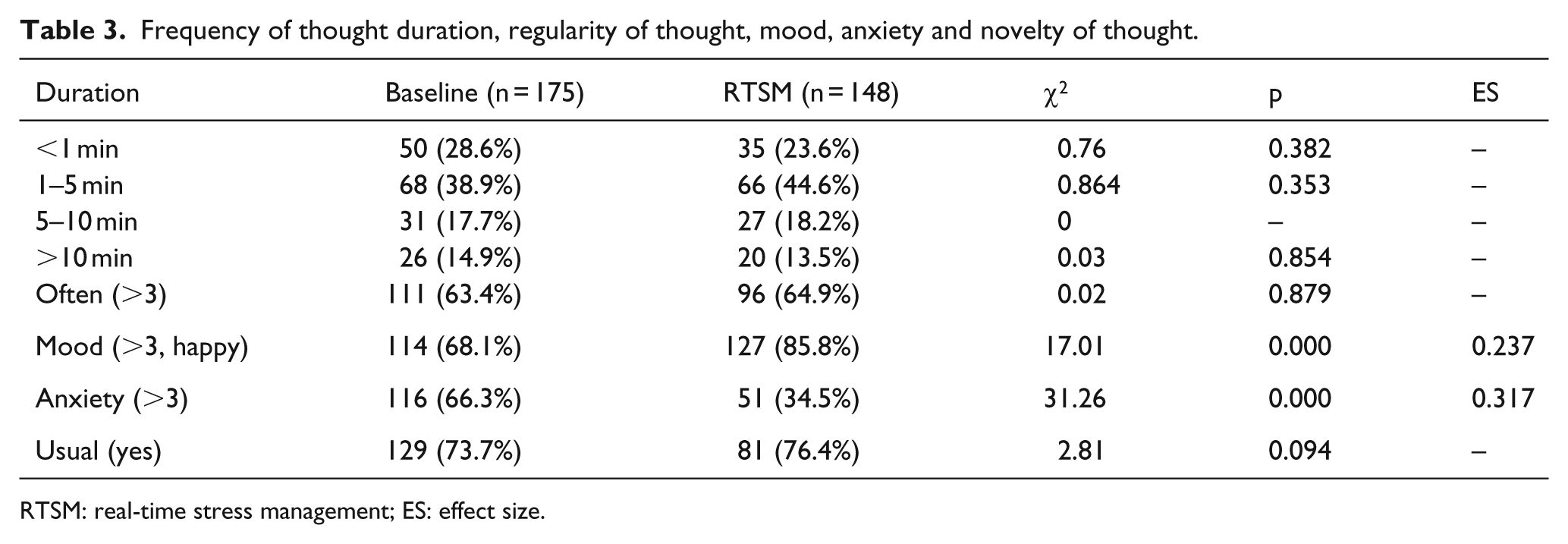
RTSM: real-time stress management; ES: effect size.
Situational context data (Table 4) showed participants were mostly alone (62.3%) and engaged in an activity almost half of the time (48.0%). Participants were significantly more often in social contexts when in the Baseline phase and only 0.36 (95% CI = 0.15–0.81) times as likely to be engaged in a similar situation in the RTSM phase.
Frequencies of situational context.
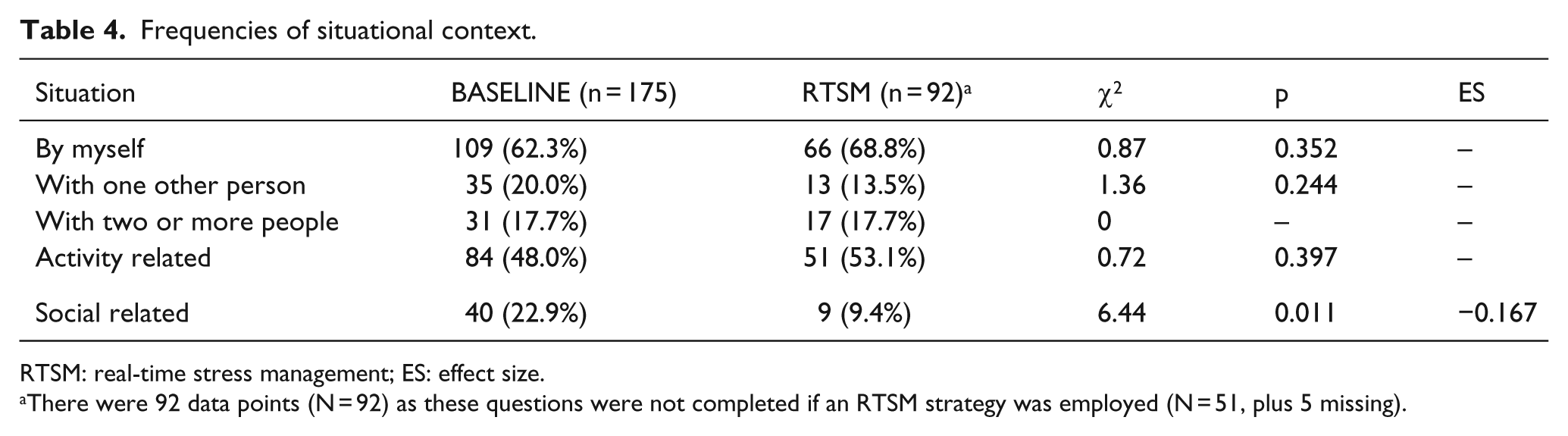
RTSM: real-time stress management; ES: effect size.
There were 92 data points (N = 92) as these questions were not completed if an RTSM strategy was employed (N = 51, plus 5 missing).
Participants were generally not disturbed by the beep, with only 34 occasions (19.4%) when it was reported as ‘annoying’, causing a ‘loss in train of thought’ or making them ‘nervous’. There were no significant differences between phases, and none of these variables were associated with elevated levels of anxiety in the Baseline phase.
Anxiety
The frequency and types of thoughts when participants indicated elevated levels of anxiety (i.e. ⩾ 3) are shown in Table 5. Worrying thoughts were significantly associated with heightened anxiety in both Baseline (OR = 16.79; 95% CI = 3.73–104.73) and RTSM (OR = 15.67; 95% CI = 3.97–72.15) phases, and all instances of confusing thoughts were significantly associated with elevated anxiety in the Baseline phase. In the Baseline phase, anxiety was negatively associated with the neutral (OR = 0.25; 95% CI = 0.08–0.74), comforting (OR = 0.18; 95% CI = 0.05–0.58) and pleasurable (OR = 0.16; 95% CI = 0.04–0.57) thoughts. In the RTSM phase, anxiety was negatively associated with pleasurable thoughts and internally focussed thoughts (OR = 0.33; 95% CI = 0.11–0.99) and positively associated with anxious thoughts (OR = 3.88; 95% CI = 1.09–14.46).
Frequency of thought type when reporting elevated anxiety (i.e. ⩾3).
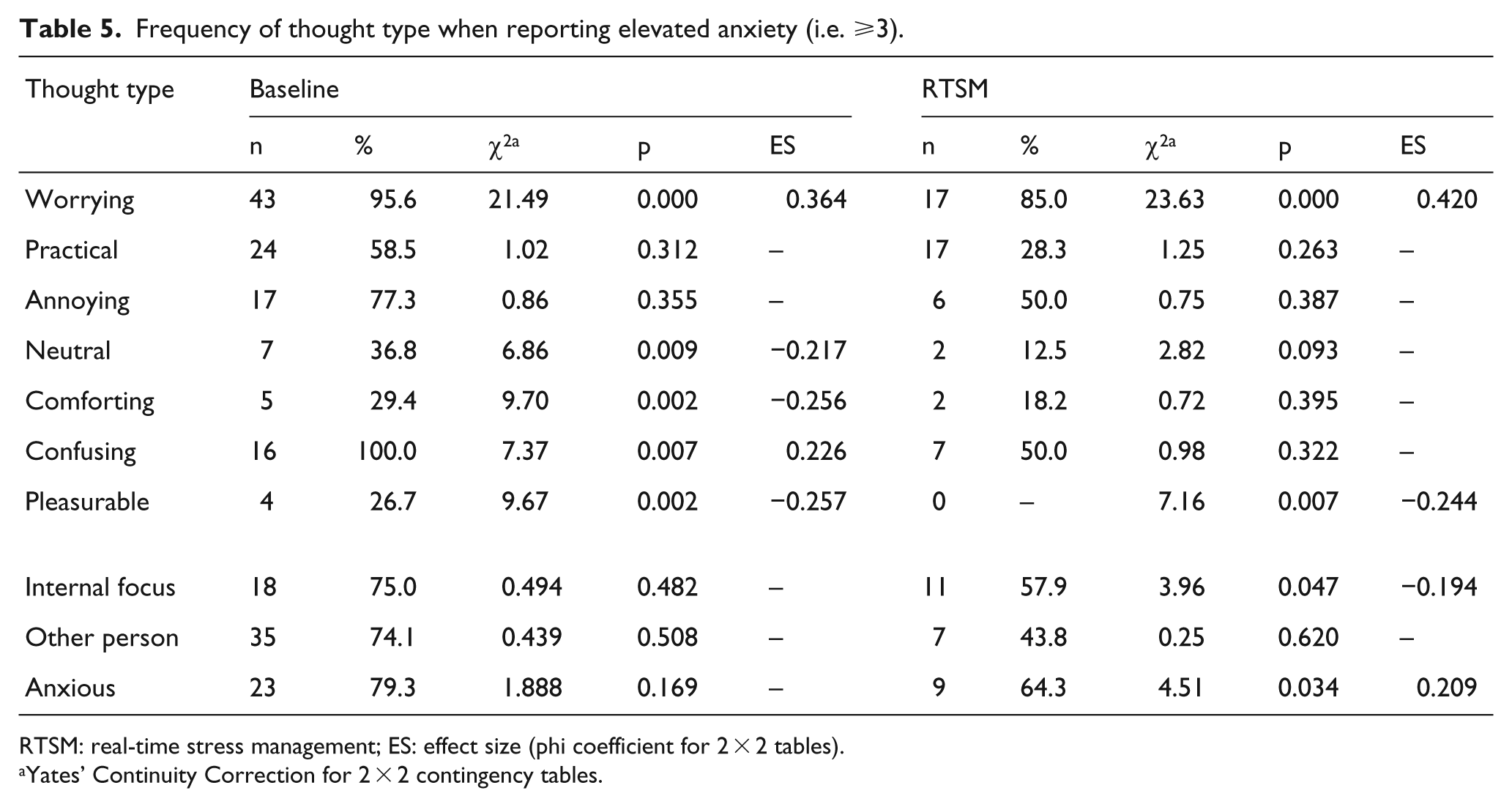
RTSM: real-time stress management; ES: effect size (phi coefficient for 2 × 2 tables).
Yates’ Continuity Correction for 2 × 2 contingency tables.
Table 6 presents the duration, novelty and regularity of thoughts, as well as mood rating when experiencing elevated anxiety. Although most thoughts lasting over 10 min occurred alongside heightened anxiety, this association was not significant. Anxiety was negatively associated with ‘happy’ mood (i.e. when rated as ‘sad’) in both phases (Baseline OR = 0.02; 95% CI = 0.00–0.11; RTSM OR = 0.16; 95% CI = 0.05–0.48), with the likelihood of rating mood as ‘happy’ decreasing by factors of 0.02 and 0.16, respectively, when experiencing anxiety.
Frequency of thought duration, regularity of thought, mood and novelty of thought when reporting elevated anxiety.
RTSM: real-time stress management; ES: effect size (phi coefficient for 2 × 2 tables).
Yates’ Continuity Correction for 2 × 2 contingency tables.
There was a significant association between anxiety and whether an individual was alone or in the company of one other person. Individuals were 2.56 (95% CI = 1.28–5.16) times more likely to report heightened anxiety when alone, but only 0.29 (95% CI = 0.13–0.66) times as likely when with someone else.
RTSM
Participants completed an average of 19.4 (SD = 5.83) questionnaires in the Baseline phase and 16.33 (SD = 5.10) in the RTSM phase. During the RTSM, elevated anxiety levels (i.e. >3) were reported on 51 (33.8%) occasions, with participants employing various techniques of which 58.8% (n = 30) were successful. Most (N = 33, 66.0%) post-technique anxiety ratings (
The subjective anxiety ratings were aggregated by phase (i.e. Baseline and RTSM) and by day for each participant, to give a single mean anxiety rating for each phase and each day for each participant:
Aggregated mean anxiety (Day) – Comparison of mean scores from the first and last days of Baseline and RTSM phases did not indicate any significant differences for either phase (Baseline first day
Aggregated mean anxiety (Phase) – There was a significant decrease (z = −2.52, p = 0.012, ES = 0.59) in subjective ratings of anxiety in the RTSM (
Participants commented that responding to questions was straightforward and similar to a mobile phone and caused little if any disruption. There was some frustration when a trial interrupted an activity, suggesting that participant-initiated trials may be more acceptable and practical. Upon completion of the study, most participants reported some degree of interference with their daily lives. The most significant limitations of the intervention was the unreliability of the PDAs, which added to the frustration and anxiety reported by some of the participants and contributed to the majority of drop-outs during the baseline phase. Another issue related to reactivity (Heron and Smyth, 2010; Palmier-Claus et al., 2011), with some participants reporting frustration due to the unpredictability of the PDA beeps and/or waiting for beeps, thus potentially preparing responses in advance and reporting elevated anxiety due to increasing awareness of the ‘erratic nature’ of their thoughts. Thus, it is possible that a participant contingent schedule may provide an alternative solution.
In this regard, there is emerging evidence that the subjective experience of people with HFA may be qualitatively different from the neurotypical population (e.g. Dubin, 2009; Hare et al., 2015; Hurlburt et al., 1994; Schleismann and Gillis, 2011). One participant expressed difficulty distinguishing between thoughts and overall experiences and provided descriptions suggestive of synaesthesia (Simner, 2011). Recording thoughts via the PDA in verbal form was thus problematic, and she reported that merely writing a thought failed to capture the experience.
Discussion
This study was essentially a preliminary ‘Proof of Principle’ study to examine the feasibility of using a PDA to deliver basic RTSM to people with HFA. In order to do this, the study tested two hypotheses, namely, that the subjective reports of anxiety would decrease from both the pre-treatment baseline level to the RTSM phase and after a stress management technique has been employed. Data were collected from nine participants and there was some support for both hypotheses. Regarding Hypothesis 1 (There will be a reduction in overall subjective ratings of anxiety from the Baseline phase to the RTSM phase (i.e. 3 Baseline days vs 3 RTSM days)), there was a significant decrease in participants’ subjective ratings between the Baseline and RTSM phases, suggesting that individuals reported less anxiety in the intervention phase. This could be related to the techniques employed as part of the RTSM or could be related to the decrease in thoughts appraised as worrying and reports of improved mood. Overall, the current findings lend some support to Hypothesis 1 over the corresponding null hypothesis. In the case of Hypothesis 2 (There will be a reduction in subjective ratings of anxiety after a stress management technique has been employed (i.e. pre- vs post-intervention ratings)), comparisons between participant ratings of anxiety provided before and after a technique in the RTSM phase revealed a significant difference. There was a decrease in anxiety ratings after a technique was employed, suggesting an impact of the RTSM on the experience of anxiety in this sample. Again, these findings can be taken as supporting Hypothesis 2 over the corresponding null hypothesis.
The ancillary aim of the study to examine the feasibility of RTSM was addressed through consideration of various factors (e.g. practicality, adherence, credibility, effectiveness, participant satisfaction). Participants completed more than half of the questionnaires during baseline and RTSM (64.7% and 54.3%, respectively), with missing data being primarily due to missing trials and situations in which PDA use was inappropriate (e.g. college lecture, driving, phone calls). Brief response times also suggested that participants may have been completing questions, but were practising techniques for a limited period of time. Compliance is an issue in ESM studies (Broderick and Stone, 2006; Heron and Smyth, 2010), and Newman et al. (2011) suggest that although computerised interventions are most effective with motivated individuals seeking support for psychological difficulties, compliance declines when interventions are employed with minimal therapist contact.
Ranfelt et al. (2009) highlight the importance of participants’ belief that a given approach is ‘effective and reliable’. Participants reported regarding the techniques as helpful in reducing subjective anxiety in situ 60% of the time and that they would continue to use elements of the intervention. Although RTSM was used less often as a result of decreased subjective anxiety, participants appeared to spend very little time practising the techniques. However, both subjective ratings from the baseline and from the RTSM phase, the latter rating being provided before and after a given technique, decreased, which could indicate that RTSM had some impact on the experience of anxiety. It is not clear whether this was related to using the techniques per se or distraction resulting from using the PDA. However, there was no associated decrease in subjective anxiety at the end of baseline, suggesting that merely using the PDA for several days did not have a significant effect. The mean HADS anxiety score for the participants indicated clinically significant levels of anxiety, and it is also possible that although participants were motivated to take part, the simple self-help techniques may not have been appropriate given these high levels of anxiety.
Generalising skills beyond therapy sessions has been highlighted as a particular issue for individuals with ASD engaged in psychotherapeutic interventions (e.g. Anderson and Morris, 2006; Hare, 2013). Studies of children have suggested the use of parent involvement (e.g. Reaven and Hepburn, 2003; White et al., 2010), and studies involving adults have suggested using others as ‘coaches’ as potential solutions (e.g. Cardaciotto and Herbert, 2004; Weiss and Lunsky, 2010). The use of the PDA platform aimed to perform a similar function, in that it would act as a prompting system when individuals experienced anxiety. Frequency of use and response times indicated that although participants were using the techniques, practice times were very brief. Newman et al. (2003, 2011) discuss the impact of varying levels of contact (i.e. self-help only, minimal contact) in research involving computerised interventions. The RTSM programme was intended as a minimal contact intervention, in that individuals could use the PDA as a portable ‘coach’ throughout their day-to-day lives. However, researcher contact (non-therapeutic) with participants could involve up to three meetings and multiple emails (as reminders of meetings, charging the PDA) over the 6-day study period. This process seemed somewhat problematic for some participants who struggled to work within the boundaries of the research relationship. These individuals reported living quite socially isolated lives and expressed frustration over past experiences with mental health services, often in terms of difficulties with access or inconsistent support over time, and appeared to be seeking more rather than less contact with psychologists. Other computerised interventions have incorporated regular (i.e. ‘check-in’) sessions to review the process (e.g. Morris et al., 2010), although this level of contact may be a particular difficulty for some individuals with AS and should be considered further in future studies.
Other research has investigated computerised interventions using real-time feedback in real-world contexts to aid insight, facilitate the monitoring of treatment, identify individual triggers and ultimately increase an individual’s awareness into adaptive and potentially maladaptive responses to various situations (Kaliouby and Robinson, 2005; Newman et al., 2011; Ranfelt et al., 2009; Wichers et al., 2011). Groden et al. (2002) and Tantam (2000) stress the importance of an idiosyncratic approach in order to identify stressors, needs and coping skills specific to each person with HFA, and the techniques described in both Hare et al. (2015) and this study may have more potential as assessment sessions to support a multi-component intervention (cf. Morris et al., 2010). Such an idiosyncratic approach would have implications for the potential clinical utility of an RTSM intervention. Ideally, such programmes could be tailored initially to the individual and their particular circumstances and then be adapted on an ongoing basis, developing in conjunction with individuals as they gain insight and skills through the course of treatment. Ranfelt et al. (2009) discuss the development of a real-time psycho-behavioural mobile device to support the social functioning of adolescents with HFA (HANDS Project).
There are several issues with this study that could be addressed in future work. In particular, there was no consideration of whether the participants had any prior experience of cognitive-behavioural or other form of psychotherapy nor of their possible motivation for taking part in an experimental study, for example, whether they were actively seeking some of psychotherapy and/or whether they were currently very anxious as was indicated by the HADS scores. Similarly, there was no consideration of whether the participants would have any prior preference for which of the RTSM techniques they would rather use. This could be readily addressed in future studies that could use RTSM in the context of ongoing therapeutic work. There is also the possibility that participants may have actively avoided identifying themselves as ‘worried’ during the RTSM phase in order to minimise the effort of engaging with the resulting intervention options. Finally, the wording of both the questions and responses in the RTSM package, which were based on the previous study by Hare et al. (2015), could be revised in the light of the current studies to ensure a better match between the forms of the questions and possible answers and to remove any potentially leading questions (e.g. ‘how nervous were you feeling?’).
Despite the weaknesses and limitations, this study has provided preliminary data for the feasibility of a momentary (i.e. ESM based) intervention in HFA. The difficulties with the dedicated PDA platform itself limited the feasibility of this particular intervention, suggesting that another ambulatory device that was more familiar and required less attention from the user, such as mobile phones, may be more suitable (Clough and Casey, 2011; Ekberg et al., 2011). The results and participant feedback have also provided useful guidance for future modifications. The findings of this study have added to the snapshot of what is known about the experience of anxiety in this population. Mapping out this experience from moment to moment has allowed examination of the phenomenology of anxiety, highlighting both its variable and idiosyncratic nature, which have implications for psychotherapeutic work. This study has highlighted a need for ongoing person-to-person support and input into the delivery of RTSM beyond what was anticipated. This suggests that such approaches may be more appropriate and beneficial as an adjunct to face-to-face interventions rather than as a stand-alone treatment.
Footnotes
Appendix
| Hello. |
| What were you thinking about just before the alarm sounded? |
| How would you describe the thought you were having just before the alarm sounded? |
| Confusing |
| Annoying |
| Worrying |
| Practical |
| Pleasurable |
| Comforting |
| Neutral |
| What was the form of the thought you were having? |
| Like written symbols |
| Like written text |
| Like someone was talking to me |
| Like I was talking to myself |
| Like an image |
| Unsure |
| Was this a normal thought for you? |
| Yes |
| No |
| Unsure |
| How long had you been THINKING about this before the alarm sounded? |
| <1 min |
| 1–5 min |
| 5–10 min |
| Over 10 min |
| How often do you think about this? |
| 1 (never) 2 3 4 5 (constantly) |
| How happy were you feeling just before the alarm sounded? |
| 1 (very sad) 2 3 4 5 (very happy) |
| How nervous were you feeling just before the alarm sounded? |
| 1 (very relaxed) 2 3 4 5 (very nervous) |
| You seem to be feeling nervous. What technique would you like to try? |
| Relaxation |
| Attention |
| Deep breathing |
| Positive self-talk |
| Imagery |
| RELAXATION |
| Sometimes when we feel anxious, our muscles are tense, but we often do not realise. |
| Relaxing our muscles can help relax our mind. |
| Work slowly through each muscle in your body, tensing each for 5 s and then relaxing for 5 s. |
| You will gradually relax your muscles up your body, from your feet slowly up to your head. |
| Try to make sure your breathing is relaxed as well; slowly breathe in and slowly breathe out. |
| Start with your toes and feet, then move up your body to your calves … |
| Then, tense and relax your thighs, bottom, stomach, shoulders, arms, hands and face. |
| Remember to tense each muscle for 5 s and then relax each muscle. |
| You can close your eyes while you relax if this helps. |
| Try to be aware of how much less tense you feel. Try this for the next minute. |
| Click the ‘DONE’ button when you are finished. |
| That is the end of the relaxation. This will become easier with practice. Well done. |
| Do you think that this technique helped you feel less nervous? |
| Yes |
| No |
| How nervous are you feeling now? |
| 1 (very relaxed) 2 3 4 5 (very nervous) |
| Would you like to try another technique? |
| Yes |
| No |
| Good work. |
| ATTENTION |
| When we are stressed, we tend to focus on our worrying thoughts. |
| We can become so focussed that it is difficult to focus on anything else. |
| There are strategies you can use to help redirect your attention. |
| Let’s try a couple. |
| Try to focus on the objects around you. Name them in your mind. |
| Look around. There may be furniture, cars, books and so on. |
| Try to be as specific as you can (e.g. chair, coat, sandwich, book, money). |
| Try this for a minute and click ‘DONE’ when you are finished. |
| Let’s try something else now. |
| Try to count back by 3 from 100. |
| 100 … 97 … 94 … 91 … |
| Try this for a minute and click ‘DONE’ when you are finished. |
| Do you think that this helped you feel less nervous? |
| Yes |
| No |
| How nervous are you feeling now? |
| 1 (very relaxed) 2 3 4 5 (very nervous) |
| Would you like to try another technique? |
| Yes |
| No |
| Good work. |
| DEEP BREATHING |
| Sometimes when we are anxious, we change the way we breathe. It becomes quicker and shallower. |
| This makes it harder for us to cope with stressful situations and makes us feel more anxious. |
| We can learn how to change our breathing to help our mind and body relax. |
| Take a slow, deep breath, in through your nose for 4 s. |
| Inhale as fully as you can. One … two … three … four … |
| Now exhale slowly and fully through your mouth, for a count of 4 s. |
| As you exhale, feel the tension and stress leave your body. |
| Keep breathing in and out slowly and deeply. |
| Repeat this rhythm for 1 min. |
| If thoughts or feelings come to mind, just notice them and refocus on your breathing. |
| Click the ‘DONE’ button when you are finished. |
| That is the end of the breathing exercise. This will become easier with practice. Well done. |
| Do you think that this technique helped you feel less nervous? |
| Yes |
| No |
| How nervous are you feeling now? |
| 1 (very relaxed) 2 3 4 5 (very nervous) |
| Would you like to try another technique? |
| Yes |
| No |
| Good work. |
| SELF-TALK |
| What we say to ourselves can affect how we feel. |
| Sometimes we have thoughts that are negative and they can make us feel more anxious. |
| These thoughts can make us feel like we cannot cope and that we want to leave the situation. |
| However, these thoughts are usually unrealistic and not based on evidence. They usually go away eventually. |
| Sometimes saying positive things to ourselves can help these thoughts seem less important. |
| Read the following statements and repeat them to yourself (in your mind) 5 times. |
| Some of them will seem more appropriate for your situation than others. |
| ‘I can get through this’. |
| ‘I have got through it before and been ok’. |
| ‘I do not like this, but it will pass. Let it go’. |
| ‘These are just thoughts. It does not mean that they are true’. |
| Click the ‘DONE’ button when you are finished. |
| Do you think that this technique helped you feel less nervous? |
| Yes |
| No |
| How nervous are you feeling now? |
| 1 (very relaxed) 2 3 4 5 (very nervous) |
| Would you like to try another technique? |
| Yes |
| No |
| Good work. |
| IMAGERY |
| Sometimes worrying thoughts are like images in our mind. |
| When we are anxious, it can feel difficult to get our minds off these images and onto something else. |
| Visualising relaxing situations can help divert our attention and help us relax. |
| Take a few deep breaths. |
| Imagine that you are standing at an empty train station, waiting for a train. Imagine that you are feeling very relaxed. |
| Try to imagine the sound of the train, the feel of the breeze, the smell of the station, as if you are actually there. |
| What else do you see? What do you hear? What do you smell? |
| Imagine your thoughts and feelings as if they are the trains passing by. |
| Try to imagine your thought printed on the side of the train as it passes. They simply pass by, but you do not try to stop them. |
| With each passing train, you feel more calm and more relaxed. |
| Spend a minute imagining the calm station and the trains passing by. Just let them go. One after another. |
| Click the ‘DONE’ button when you are finished. |
| Do you think that this technique helped you feel less nervous? |
| Yes |
| No |
| How nervous are you feeling now? |
| 1 (very relaxed) 2 3 4 5 (very nervous) |
| Would you like to try another technique? |
| Yes |
| No |
| Good work. |
| (If the participant’s subjective rating of anxiety was recorded < 3.) |
| What were you DOING just before the alarm sounded? |
| How many people were you with just before the alarm sounded? |
| I was by myself |
| I was with one other person |
| I was with 2 or more people |
| How much did the alarm upset you? |
| 1 (not at all) 2 3 4 5 (a great deal) |
| Did the interruption to your thinking upset you? |
| Yes |
| No |
| In what way did the interruption to your thinking upset you? |
| It made me feel nervous |
| I lost my train of thought |
| It annoyed me |
| Other (text entry) |
| In what way did the interruption to your thinking upset you? |
| Thank you. Please charge your PDA at the end of the day. |
| Goodbye. |
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.