
Abstract
The Social Attribution Task, Multiple Choice is introduced as a measure of implicit social cognitive ability in children, addressing a key challenge in quantification of social cognitive function in autism spectrum disorder, whereby individuals can often be successful in explicit social scenarios, despite marked social adaptive deficits. The 19-question Social Attribution Task, Multiple Choice, which presents ambiguous stimuli meant to elicit social attribution, was administered to children with autism spectrum disorder (N = 23) and to age-matched and verbal IQ–matched typically developing children (N = 57). The Social Attribution Task, Multiple Choice performance differed between autism spectrum disorder and typically developing groups, with typically developing children performing significantly better than children with autism spectrum disorder. The Social Attribution Task, Multiple Choice scores were positively correlated with age (r = 0.474) while being independent from verbal IQ (r = 0.236). The Social Attribution Task, Multiple Choice was strongly correlated with Vineland Adaptive Behavior Scales Communication (r = 0.464) and Socialization (r = 0.482) scores, but not with Daily Living Skills scores (r = 0.116), suggesting that the implicit social cognitive ability underlying performance on the Social Attribution Task, Multiple Choice is associated with real-life social adaptive function.
Keywords
Introduction
With recent changes in the definition of autism spectrum disorder (ASD) and the move away from subtyping to an all-encompassing diagnostic concept (Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5), the need for quantifiers of social functioning capable of grading levels of disability and ability within the broad autism spectrum has increased (Grzadzinski et al., 2013). And while indices of severity can be derived from tools such as the Autism Diagnostic Observation Schedule (ADOS; Gotham et al., 2009; Lord et al., 1999) and the Autism Diagnostic Observation Schedule, 2nd ed. (ADOS-2; Lord et al., 2012), the vast majority of community-based evaluations do not utilize standardized diagnostic instruments because they are costly in time demands, expertise, and training (Wiggins et al., 2006). Well-validated, informant-based rating scales such as the Social Responsiveness Scale (SRS; Constantino and Gruber, 2005) can be helpful and cost-effective, but no performance-based assay to date has been shown to have quantifying value for social function beyond findings of promising between-group differences in some social cognitive tasks, typically involving theory of mind skills (see Baron-Cohen, 2000, for a review). Performance on those tasks shows a strong relationship with verbal ability in typical and atypical populations (Fisher et al., 2005; Milligan et al., 2007). Consequently, the success or failure on such tasks may be confounded by the level of verbal skills. More importantly, verbally proficient individuals with ASD are often able to “pass” some of these tasks, likely using their considerable verbal intelligence skills to compensate for reduced implicit social understanding but, consequently, without exhibiting commensurate social cognitive skills in real-life situations (Klin et al., 2002). ASD individuals with verbal intelligence skills above the threshold for intellectual disability now form the majority of the population affected by ASD (Centers for Disease Control and Prevention (CDC), 2008), yet evidence continues to emphasize the significant gap between their verbal cognition and functional (i.e. adaptive) socialization skills (Kanne et al., 2011; Klin et al., 2007). Thus, the field still lacks a performance-based, cost-effective, quantitative, and minimally verbally mediated procedure to assess elements of social cognitive ability that align with naturalistic social function. Such a procedure could potentially supplement current diagnostic and evaluation practices in the community at large by providing an element of clinically relevant quantification and could also enrich the characterization of participants in large-scale research in which gold-standard protocols are prohibitive because of cost or time constraints (Volkmar et al., 2004).
To address this gap, we set off to develop a short, objectifive, quantitative, and less verbally mediated social cognitive assay intended to measure aspects of implicit social cognitive function thought to be aligned with, and pertinent to, levels of social and communicative adaptive function in children with ASD. In designing this study, we focused primarily on social–communicative abilities rather than disabilities, because (1) cost-effective quantitative assessments for social–communicative impairment or symptoms are available (such as the SRS) and (2) social–communicative adaptive functioning, or the individual’s ability to navigate the demands of everyday social life, is critical for programming and treatment (Klin et al., 2007; National Research Council (NRC), 2001). Finally, we also aimed for performance on our measure to be sensitive to age of the child, with older children performing at a higher level than younger ones, as age has been found to be highly correlated with performance on social cognitive tasks in both typically developing (TD) children (Hu et al., 2010) and in children with ASD (Bal et al., 2013). More pragmatically, we aimed to ensure that there were no basal or ceiling effects with a view to make the Social Attribution Task, Multiple Choice (SAT-MC) relevant to a relatively wide range of age and intellectual function.
To develop such an assay, we aimed at capitalizing on two universal challenges in social–communicative adaptive functioning displayed by individuals with ASD regardless of level of intellectual functioning (reviewed in Klin et al., 2003). First, there is a great discrepancy between what individuals with ASD can do on explicit tasks of social reasoning—a relative strength, when all of the elements of a problem are verbally given to them—and what they do in more naturalistic situations—a significant weakness, when they need to spontaneously apply their social reasoning abilities to meet the moment-by-moment demands of daily social life. One result of this contrast is the typical discrepancy between intellectual abilities and levels of social adaptive functioning in even the highest functioning individuals with ASD, which can reach more than 2 standard deviations (SDs) in standardized assessments (Saulnier and Klin, 2007). Second, the complex, fast-paced and constantly changing nature of the social world requires intuitive and spontaneous tendencies to impose social meaning on most events—indeed, a bias toward social thinking in action and away from inanimate or physical contingencies that are less conducive to, and in fact can interfere with, successful social–communicative adaptation (Klin et al., 2002). Limitations of previous approaches and these two principles defined the framework for our approach: our task had to be implicit rather than explicit, more non-verbally than verbally mediated, and, particularly, it should tap on spontaneous predispositions rather than being amenable to rule-governed problem solving (Klin et al., 2003).
These were the principles upon which we built a social cognitive measure called the Social Attribution Task (SAT; Klin, 2000). The SAT aimed to assess a person’s spontaneous ability to attribute social meaning to ambiguous visual displays that are universally and immediately perceived by typical individuals as social in nature. The SAT uses Heider and Simmel’s (1944) classic animation in which geometric shapes enact a sequence of related social scenes unfolding as a social story. In one study, narratives about the scene were collected from highly verbal adolescents and adults with ASD after multiple viewings of the animation and were coded for socially relevant attributions made about the geometric set of “characters,” their actions, and inter-actions. Despite participants’ high verbal skills and their ability to “pass” advanced tests of theory of mind skills, they showed marked deficits in social attribution encompassing social identity, social action, intentions, feelings, and social outcome, instead providing a range of irrelevant or tangential attributions such as describing the social scenes in physical, not social terms (Klin, 2000).
While the SAT succeeded in capturing deficits in social cognition in even such higher functioning individuals, the coding of narratives required a very laborious process. Once discrete propositions in the narrative were isolated, they were scored according to seven indices generating a detailed profile of social cognition. For example, a Pertinence Index assessed the percentage of propositions that were not pertinent to the social story contained in the participant’s narrative; a Salience Index measured the percentage of social attributions commonly attributed to the animation by typical adults that were contained in the participant’s valid propositions; and Theory of Mind cognitive and affective indices measured the developmental level achieved in the participant’s usage of cognitive and affective attributions. To achieve reliability in coding, the SAT required extensive training in the coding scheme, and familiarity with a glossary of commonly used words and phrases, making the usage of this tool impractical outside a research environment. Additionally, the heavy reliance on a spontaneously generated narrative constrained the use of the SAT to more verbal and older children and adolescents.
The SAT-MC attempts to address these shortcomings. It proposes a simplified measure in which, after viewing the classic animation, discrete scenes from the original cartoon are isolated and participants are provided with questions and answers in a multiple-choice format. “Correct” answer choices were derived from the Salience Index in the SAT coding scheme, which comprised socially relevant attributions made by typical adults and adolescents in response to the animation. The SAT-MC was designed to assess children’s ability to attribute social meaning to ambiguous visual displays as a means of quantifying their tendency toward such attributions and their attempts to adapt to the demands of everyday social life. We had to compromise an important aspect of the original task, namely, that participants were provided with no explicit instructions, and, indeed, many participants would complete the task without fully discerning the social nature of the animation. And yet, in designing the SAT-MC, we strived to maintain the main elements of the original SAT. Chiefly, the SAT-MC retains the focus on a child’s attribution of social meaning to ambiguous stimuli and does so without providing verbal contextual cues that may support the use of verbally mediated deductive reasoning to achieve higher performance. Since its original creation, the SAT-MC has been utilized in adult populations, assessing social cognitive abilities in individuals with schizophrenia and in typical individuals (Bell et al., 2010; Johannessen et al., 2013). This study reports on data obtained for research participants for whom the task was originally designed, namely, TD children and children with ASD.
We tested the following hypotheses: (1) children with ASD display deficits on the SAT-MC relative to controls; (2) performance on the SAT-MC is not mediated by the level of verbal intelligence; (3) performance on the SAT-MC improves with age and our central hypothesis; and (4) performance on the SAT-MC predicts levels of social and communicative adaptive function, which are strongly mediated by social skills, but not of daily living skills, which largely are not, thus providing support for the success of our attempt to assay social cognitive abilities that are associated with social and communicative function in real-life situations. Finally, in an exploratory fashion, we assessed the diagnostic discriminative utility of the 19 items comprising the coding scheme for the SAT-MC with a view to optimize the tool for future research.
Methods
Participants
The SAT-MC was administered to a heterogeneous group of children with ASD (N = 23; age range: 4.7–12.1 years; verbal IQ (VIQ) range: 62–146) and to a control group (N = 57) matched on chronological age and VIQ (age range: 4.3–15.1 years; VIQ range: 79–129). This study was based in the Autism Program of the Yale Child Study Center, New Haven, CT, and the research protocol was approved by the Human Investigation Committee of Yale University School of Medicine.
The diagnosis of ASD was ascertained with standardized diagnostic instruments and clinician-based procedures: information from the administration of the ADOS (Lord et al., 1999) and the Autism Diagnostic Interview—Revised (ADI-R; Rutter et al., 2003) formed the basis for a Best Estimate Diagnosis procedure performed by two expert clinicians, resulting in a consensual clinician-assigned diagnosis for every child in the ASD group. VIQ was assessed in both the TD and ASD groups using the Wechsler Intelligence Scale for Children, 3rd ed. (WISC-III; Wechsler, 1991). Adaptive skills in the areas of Communication, Socialization, and Daily Living Skills were assessed for the ASD group only with the Vineland Adaptive Behavior Scales, 2nd ed., Survey Form (Vineland-II; Sparrow et al., 2005). None of the participants in the control group had a first-, second-, or third-degree relative with ASD. Table 1 summarizes descriptive data on participants’ characterization.
Participant characterization.
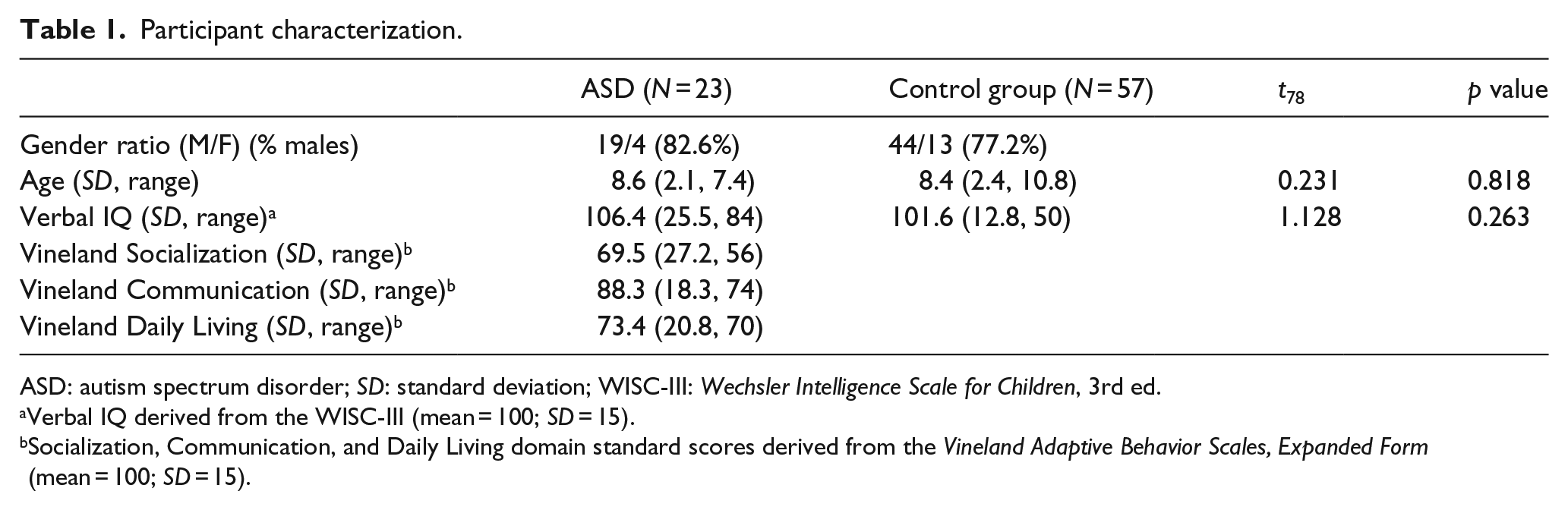
ASD: autism spectrum disorder; SD: standard deviation; WISC-III: Wechsler Intelligence Scale for Children, 3rd ed.
Verbal IQ derived from the WISC-III (mean = 100; SD = 15).
Socialization, Communication, and Daily Living domain standard scores derived from the Vineland Adaptive Behavior Scales, Expanded Form (mean = 100; SD = 15).
Although there was a wide range of scores in both VIQ and Adaptive Behavior in the ASD group, VIQ for the ASD group was overall within the average range of intellectual ability, while their adaptive behavior skills were over to 2 SDs below VIQ in the Socialization and Daily Living domains, and over 1 SD below VIQ in the Communication domain.
Experimental measure: the SAT-MC
The SAT-MC utilizes Heider and Simmel’s (1944) silent video display. The geometric “cast of characters” consists of a rectangle with a small opening that opens and closes, as if on a hinge, a big triangle, a small triangle, and a small circle. Movements of shapes are contingent upon one another. For example, a sequence of social scenes depicts an episode of bullying in which the small shapes escape, together, from the big triangle (the bully). Multiple-choice questions assess social attribution. The correct answer from the four alternatives provided corresponds to the social attribution commonly attributed to the scene by TD adults in previous research (Klin, 2000): Illustration: Experimenter replays video segment in which little circle moves slowly behind the “door” of the “house,” pulling the “door” back to “shield itself” from “view” of the big triangle. A question is asked: What is the little circle doing? Correct answer: It is “hiding” from the big triangle. Additional multiple-choice answers provided: It got stuck in the “door” of the “house”; it is “painting” the “house”; it is “playing” in the “house.”
As noted, there are 19 questions (see Appendix 1), and the participants’ global score on the SAT-MC is the sum of “correct” answers.
Procedure
The version of the SAT-MC used in this study was a computer program written to a CD-ROM. While the video presentations and written display of multiple choices follow a standard order and the accompanying reading of the multiple choices is pre-recorded, an examiner administers the program so as to ensure that the participant is attending to the screen prior to advancing to a question or a subsequent video segment. Thus, administration is standard across participants. An examiner starts the program by clicking on the screen and a narrator’s voice tells the participant that she will be shown a silent video twice and then asked some questions. Upon the examiner’s click on the screen, the video is played twice, uninterruptedly, displaying the original Heider and Simmel (1944) video, which lasts 76 s per presentation. Following the second viewing, short segments are shown again, ending with an image frozen with shapes highlighted that are relevant to the given multiple-choice question. The question and the multiple choices are displayed on the screen and read aloud by the pre-recorded narrator. This procedure is repeated until all 19 questions have been administered, the full administration lasting approximately 10 min.
Results
In order to assess the SAT-MC’s power to quantify social attribution and discriminate school-age children with ASD as a group from their typical peers, we compared SAT-MC global scores—the total number of correct answers (ranging from 0 to 19)—across the two groups and calculated the corresponding effect size via Cohen’s d coefficient in order to assess the degree of overlap between the two distributions. Average global SAT-MC scores differed significantly between ASD (10.2, SD = 4.9) and TD (13.6, SD = 2.5) groups (t = 4.099, p < 0.0001), with a global score range of 16 for the ASD group and a range of 10 for the TD group. This comparison yielded a large effect size (Cohen’s d = 0.875), thus demonstrating significant deficits in social attribution in the ASD group relative to the control group and a relatively large separation in SAT-MC score distributions across the two groups.
In order to assess the developmental nature of the SAT-MC and the desired intent for relative independence between this measure of social cognition and verbal skills, correlations between the SAT-MC global score, chronological age, and VIQ were performed for each of the two groups. To assess the predictive utility of the SAT-MC relative to measurements of adaptive functioning in the social and communicative domains, but not relative to the daily living domain, SAT-MC global scores were correlated with standard scores on the Socialization, Communication, and Daily Living domains of the Vineland-II (Sparrow et al., 2005). Table 2 summarizes the results.
Correlations between SAT-MC global score and age, VIQ, and Vineland domains. a
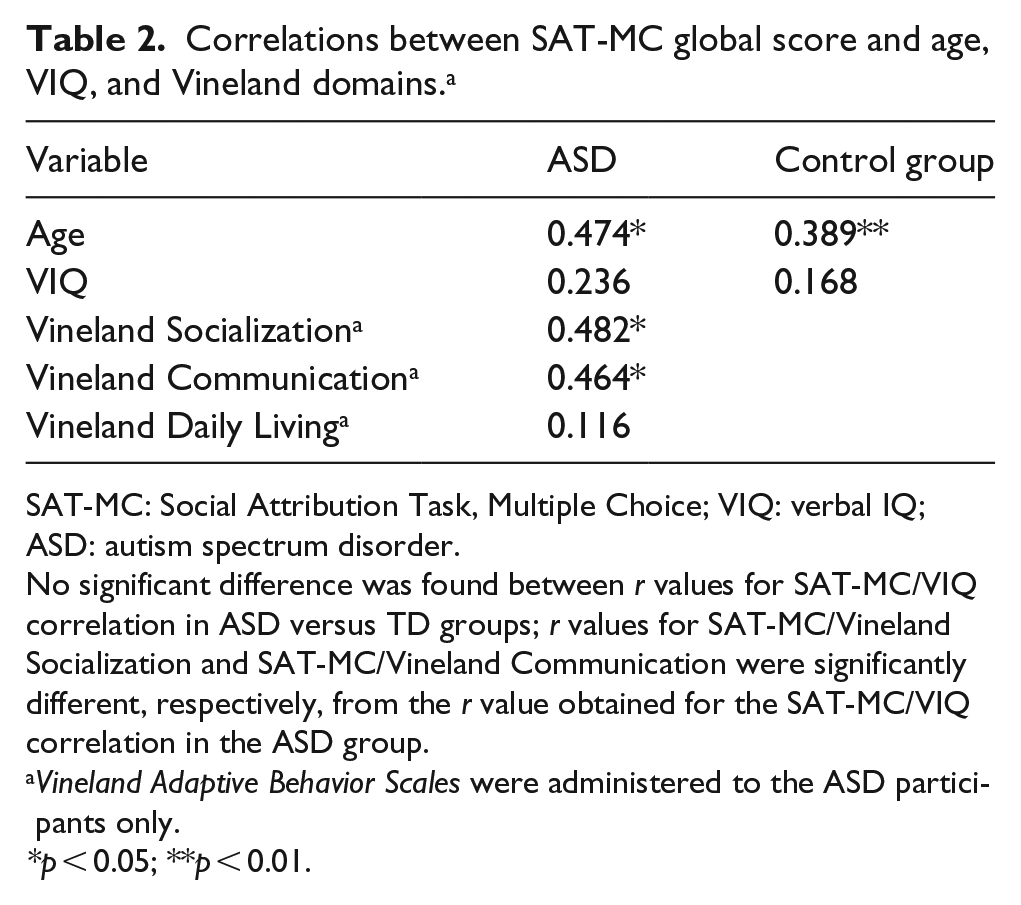
SAT-MC: Social Attribution Task, Multiple Choice; VIQ: verbal IQ; ASD: autism spectrum disorder.
No significant difference was found between r values for SAT-MC/VIQ correlation in ASD versus TD groups; r values for SAT-MC/Vineland Socialization and SAT-MC/Vineland Communication were significantly different, respectively, from the r value obtained for the SAT-MC/VIQ correlation in the ASD group.
Vineland Adaptive Behavior Scales were administered to the ASD participants only.
p < 0.05; **p < 0.01.
Consistent with our predictions, the SAT-MC was positively correlated with age for both the ASD and control groups, demonstrating, as expected, a developmental progress toward higher social cognitive abilities with age; and the SAT-MC was not significantly associated with VIQ, demonstrating its relative independence from verbal ability. Establishing an age effect on SAT-MC performance bodes well for future psychometric refinements given our aim to measure social cognitive ability over a wide range of age and improving levels of social cognitive ability. Given the samples’ wide range of VIQ, the lack of association between performance on the SAT-MC and VIQ bodes well for our goal to measure social cognitive ability in ways that are not mediated by verbal skills. In regards to the main hypothesis of the study, the SAT-MC was correlated with both the Vineland’s Socialization and Communication scores, but was not significantly correlated with the Vineland’s Daily Living scores. These results suggest that the SAT-MC has predictive utility—relative to the social and communicative aspects of adaptive functioning in real life (the higher the SAT-MC scores, the higher the child’s social and communicative adaptive skills)—and discriminant utility—the relationship is specific to social and communicative skills, being unrelated to areas of adaptive functioning less impacted by social cognition (such as the skills contained in the Vineland’s Daily Living domain).
To further assess the specific contribution of adaptive function in explaining variability in social cognitive skills as measured by the SAT-MC, we performed hierarchical linear regression, beginning the model with age in the first block, Vineland’s Daily Living Skills in the second block, and Vineland’s Socialization and Communication scores in the third. Table 3 presents resulting coefficients and model fit. Age significantly predicted SAT-MC scores, β = 1.096, t = 2.468, p < 0.05. As is expected in a developmental relationship, age also explained a significant proportion of variance in SAT-MC scores, r2 = 0.225, F(1, 21) = 6.090, p < 0.05. The unrelated construct of Daily Living Skills did not explain any significant additional amount of variance in the second block, thus corroborating the discriminant validity of the SAT-MC relative and specifically to social and communicative adaptive skills. As expected, Vineland’s Socialization and Communication scores were inter-correlated, given their derivation from a single overall measure of adaptive function a critical psychometric property of which is that its domains inter-correlate. These two scores explained a significant proportion of the variance in SAT-MC scores, r2 = 0.682, F(2, 18) = 10.814, p = 0.001, predicting 38.3% more of the variance, above and beyond what can be accounted for by age.
Regression coefficients for hierarchical linear regression in ASD group (N = 23) with SAT-MC score as dependent variable.
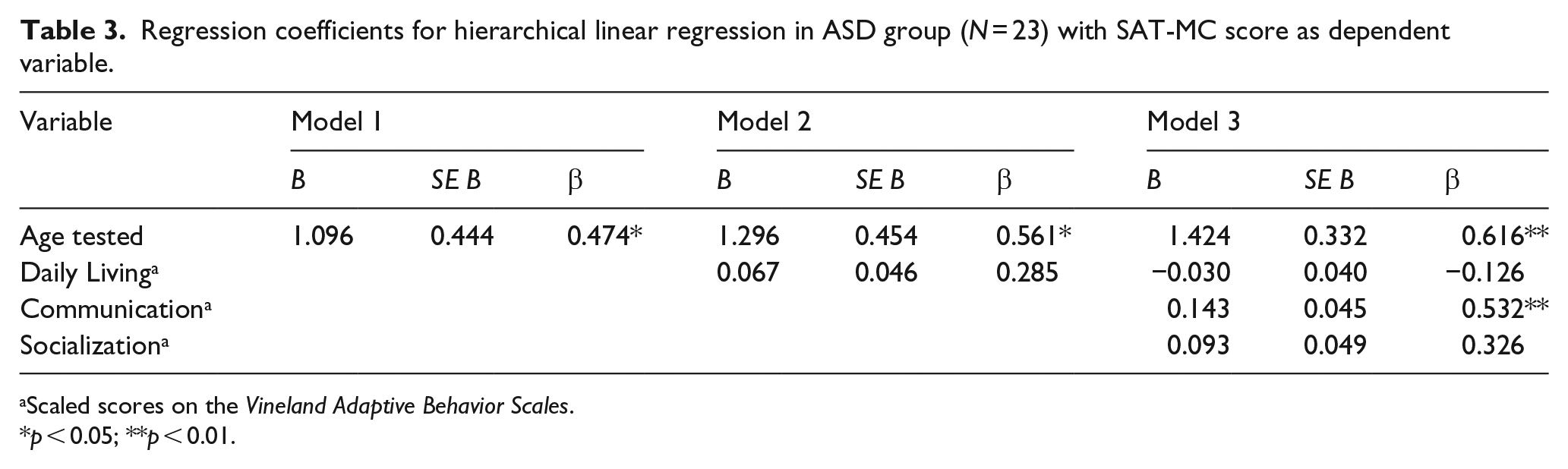
Scaled scores on the Vineland Adaptive Behavior Scales.
p < 0.05; **p < 0.01.
We next proceeded in an exploration of the diagnostic discriminative power of individual SAT-MC items. We entertained this analysis in order to further refine the test’s power to segregate TD and ASD groups and to possibly also shorten the list of items that need to be administered. We began by creating 2 × 2 contingency tables for each item, established by the number of participants who answered each item correctly or incorrectly for the ASD and control groups. The following statistical analyses were performed for each contingency table or SAT-MC item: Fisher’s exact test, yielding the exact probability of observing the particular set of frequencies as well as the phi coefficient r measuring the extent of association between the groups and the SAT-MC scores, and a test of the statistical significance of this association (Siegel and Castellan, 1988). The values of phi were also described in terms of Cohen’s (1988) categories for effect sizes of association (pp. 224–225), according to which phi values are defined as 0.10 < phi < 0.30 = “Small,” 0.30 < phi < 0.50 = “Medium,” and 0.50 < phi < 0.70 = “Large.” Table 4 lists the results of analyses performed for the 19 contingency tables corresponding to number of children answering correctly or incorrectly on each one of the 19 SAT-MC questions in the ASD and control groups.
Individual SAT-MC item analysis: Fisher’s exact test, phi coefficients r, and Cohen’s effect sizes for the 19 items.

SAT-MC: Social Attribution Task, Multiple Choice; ASD: autism spectrum disorder; TD: typically developing; S: small (0.1 < phi < 0.3); M: medium (0.3 < phi < 0.5); L: large (0.5 < phi < 0.7).
Bolded items comprise the optimized nine-item SAT-MC.
p < 0.05; **p < 0.01.
Considering that some items within the SAT-MC appeared to predict diagnosis better than others, the measure was assessed for internal consistency, depicted in Table 5. Both items 1 and 5 were poorly correlated with global score. Aside from these two items, however, the items in the measure hang together. Removing items 1 and 5, nine items significantly discriminated the two groups, with varying degrees of discriminative power, whereas eight items did not. With a view to optimize the discriminative power of the instrument, we re-calculated an SAT-MC global score based solely on the nine items capable of discriminating the two groups, thus creating a scale of 0–9. We then compared results for the new mean global SAT-MC score for the ASD (4.65, SD = 3.02, range = 9) and TD (7.56, SD = 1.24, range = 4) groups. The comparison continued to be strongly significant (t = 6.137, p < 0.0001), but now the effect size was much larger, with a Cohen’s d of 1.261, improving upon the original Cohen’s d of 0.875 which calculated a global score comprising all 19 items. In sum, using only the nine discriminating items resulted in a very substantial separation of the two distributions, thus demonstrating improved diagnostic power.
Internal consistency: item-total statistics.
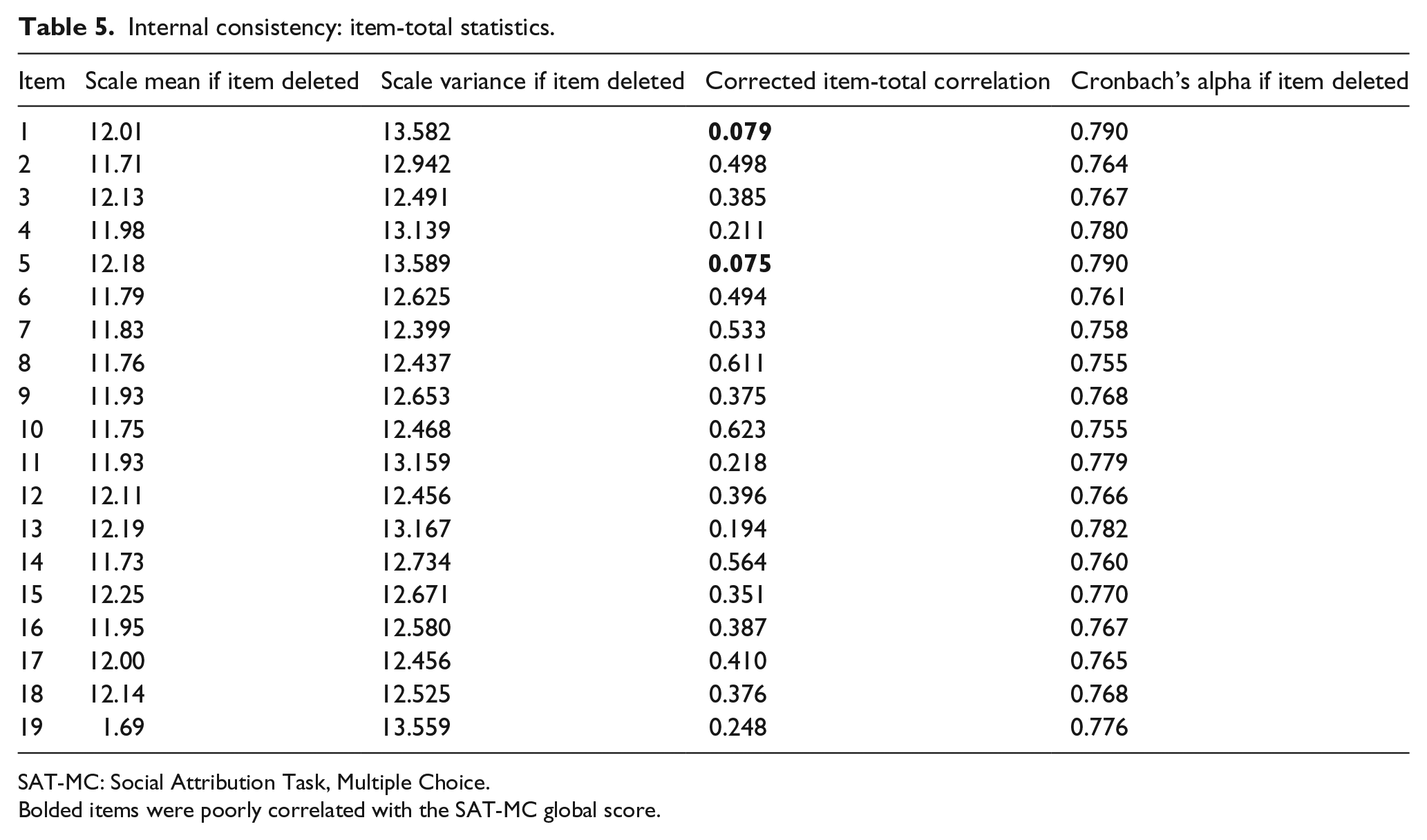
SAT-MC: Social Attribution Task, Multiple Choice.
Bolded items were poorly correlated with the SAT-MC global score.
Discussion
As an initial step toward developing a brief, quantitative, and performance-based measure of implicit social cognitive function associated with real-life social adaptation, we tested the SAT-MC; this is a simplified version of a more detailed, but quite laborious, assessment of social cognition that had been shown to capture social attribution deficits even in highly verbal individuals with ASD (the SAT; Klin, 2000; Klin and Jones, 2006). Results showed that the SAT-MC could demonstrate between-group deficits in school-age children with ASD relative to age- and VIQ-matched controls, with a relatively large separation of the two distributions (Cohen’s d = 0.875). In an attempt to optimize the tool’s diagnostic discriminative power, we analyzed the 19 items comprising the SAT-MC and segregated the nine items that significantly discriminated the ASD group from the control group. Now using only these nine items, we were able to further separate the two distributions, with a Cohen’s d of 1.269. The fact that the SAT-MC correlated strongly with age but not with VIQ in both the ASD and the control groups demonstrated that the tool was sensitive to developmental growth and yet less vulnerable to the confounding effects of verbal intelligence, thus attesting to its specificity to social cognition. In future refinements of this measure, the developmental nature of performance on the SAT-MC will potentially allow for more meaningful scoring in relation to benchmark age expectations.
Our results also showed that the SAT-MC is a strong predictor, on a group level, of adaptive social and communicative skills measured by the Vineland-II. The Vineland requires (as do most standardized measures of adaptive functioning) a third party respondent to assess functional “real-life” skills. The SAT-MC, however, could be used as a direct measure of implicit social cognitive ability that supplements the assessment of more comprehensive adaptive behavior profiles obtained solely by parent report. Moreover, the SAT-MC also shows promising discriminant validity in that its scores were uncorrelated to adaptive skills less mediated by social cognitive competence, such as the skills contained in the Vineland’s Daily Living Skills domain. This offers further support that the SAT-MC is tapping into the specific construct of social cognition.
This pilot work has several limitations to be addressed in future research. First, the sample of school-age children with ASD was relatively small, particularly in the younger, kindergarten age range for which the procedure might be particularly sensitive. Even this multiple-choice version of the SAT (aimed at assessing those individuals with more impaired verbal skills than was the original SAT) might not achieve meaningful ascertainment of a child’s implicit social cognitive abilities in a very young cohort of children, especially those with pronounced language delays. Future, larger studies are needed to establish the age and verbal ability boundaries within which there is adequate sampling in this critical domain of social function. Second, the sample of age- and VIQ-matched controls was not clinically characterized in relation to adaptive ability or symptomology. We expect implicit social cognitive function to be normally distributed across the larger population of children, but this will have to be ascertained with low-risk samples whose typicality is adequately measured. Finally, the control group did not, by design, include children with learning vulnerabilities or psychiatric conditions. Demonstration of the tool’s ability to discriminate between ASD and TD groups was a necessary first step before exploring diagnostic specificity of the measure, but the latter will need to be explored in future larger scale studies.
The fact that we could further optimize the SAT-MC by segregating the items that are more likely to separate children with ASD from their peers suggests that modifications could further improve the tool. Possibilities include reducing the number of viewings of the entire cartoon, thus further taxing immediate, spontaneous reactions to its implicit social nature, and rephrasing “incorrect” multiple-choice answers to include commonly made, non-pertinent answers (as in Klin, 2000). This might recapture a proxy of the Pertinence Index of the original SAT procedure, which was, at times, diagnostically striking. For example, the “celebration” of the two little triangles (which had just “escaped” the big, “bully” large triangle) was often described by individuals with ASD as little shapes attracted to each other via a magnetic field.
These limitations notwithstanding the fact that a short procedure, such as the SAT-MC, was able to positively predict social and communicative adaptive “real-life” skills suggests some theoretical implications for developmental accounts of social adaptation—chiefly that spontaneous social attribution skills develop concurrently, and predictively, with adaptive social and communicative skills in the real world (Klin et al., 2003). Recent research has shown that very young children with ASD, even in toddlerhood, already exhibit deficits in developmentally early-emerging and evolutionarily highly conserved social skills, such as visually entraining to caregivers’ eyes (Jones et al., 2008) and preferentially orienting to social movement or biological motion (Klin et al., 2009)—skills that in typical development are already online from the first weeks of life (Haith et al., 1977; Simion et al., 2008). When intact, these skills guide subsequent social experiences, biasing attention and learning, and move social adaptation and social cognition forward through iterative, interaction-based engagement with caregivers and peers (Jones and Klin, 2009). Children with ASD appear to learn about the social world differently, scaffolding their adaptive action through explicit associations, literal language, and rule-governed behavior, typically missing the implicit associations, non-literal language, and context-dependent behavior that are so critical for intuitive, immediate, and integrative social–communicative adjustment (Klin et al., 2003). It is thus not surprising to see adaptive socialization deficits in ASD as early as age 2 (Paul et al., 2014; Ventola et al., 2014). As evidenced in Heider and Simmel’s (1944) classic cartoon, TD individuals seem to have a virtual obsession with the “social,” leading them to immediately anthropomorphize inanimate objects. This intuition is significantly attenuated in individuals with ASD who are more likely to use physical rather than social reasoning. The SAT-MC taps into several of these longstanding discrepancies in social learning and allows for quantifiable assessment of social cognition in broader populations and does so with less elaborate coding than did the original SAT.
Footnotes
Appendix 1
Acknowledgements
We wish to thank the children and their families included in this study for their time and participation. We also wish to thank Katherine Tsatsanis, PhD, Kathleen Koenig, MSN, APRN, Pamela Ventola, PhD, Julie Wolf, PhD, and Fred Volkmar, MD, for their contributions to the clinical characterization of children with ASD. We wish to thank Catalina Hooper, Sanno Zack, Amy Augustyn, Julie, Klunk, Brian Wolff, Melissa Extein, Sam Loria, Stephanie Jones, Melissa Simons, and Jonas Anderson for their contributions to the recruitment and characterization of children with typical development.
Funding
This research was funded by a grant from the National Institute of Child Health and Human Development [P01 HD003008].