
Abstract
Children and youth with autism spectrum disorder presenting in emergency departments face potential cognitive, sensory, and behavioral challenges, and it is crucial for providers to be aware of their unique needs. However, disclosure of a child’s autism spectrum disorder can be complex for parental caregivers and is not well understood. This qualitative study utilized a grounded theory approach and analyzed data from 28 parents and 16 health care providers related to autism spectrum disorder disclosure within two Canadian pediatric emergency departments. Study results indicated that participants identified benefits and risks of disclosure. Encouraging understanding, expediting service, and preparing health care providers for working with children with autism spectrum disorder were identified as benefits of disclosure. Risks related to disclosure included potential negative attributions toward the children and parental discomfort in disclosing a diagnosis in front of the children. Parents discussed the health care encounters they experienced following disclosure and provided recommendations for improving the disclosure process in the emergency department. It is recommended that future research explore the experiences of parents who choose not to disclose their child’s autism spectrum disorder. Greater awareness of the disclosure experience and the development of resources and tools to support communication between parents and health care providers are also recommended.
Introduction
Children and youth with autism spectrum disorder (ASD) are impacted by sensitivity to sensory stimuli such as noise, lighting, touch, physical discomfort, difficulty adjusting to change, and communication difficulties, all of which may result in heightened arousal in the child. These features can impact care delivery in children and youth with ASD, especially when accessing acute medical care (Chun et al., 2013; Giarelli et al., 2014; Muskat et al., 2015). Studies of medical care experiences of individuals with ASD have indicated that strategies to accommodate these challenges such as positive and collaborative interactions between medical staff and parents or caregivers, advanced preparation, understanding the unique needs of a patient, and modification to the hospital environment enhance the health care experience (Chun et al., 2013; Davignon et al., 2014; Muskat et al., 2015; Venkat et al., 2012). It is thus logical that health care providers (HCPs) should know that a child or youth has ASD in order to proactively accommodate their challenges.
Despite indicators that children with ASD frequently access medical services, there is evidence that not all parents choose to report their child’s ASD in medical care settings. For example, data on Taiwanese insurance claims suggest that children with ASD utilize more emergency medical services than their non-ASD peers (Wu et al., 2014). In contrast, a recent health record review in a pediatric emergency department (ED) revealed that only 160 out of a total of 62,092 ED visits (0.2%) were identified as being visits by patients with ASD (Cohen-Silver et al., 2014), much lower than expected based on ASD prevalence indicators (Ouellette-Kuntz et al., 2012).
There is very limited empirical understanding of the process and parental perspective of disclosing a child’s ASD, with extant research primarily focusing on dis-closure decisions of adults with chronic health conditions, sensory challenges, learning disabilities, and mental health issues (Johnson and Joshi, 2014). ASD-based studies of self-disclosure are few (Davidson and Henderson, 2010; Johnson and Joshi, 2014) and have principally focused on adult perspectives of self-disclosure, with little attention paid to parental perspectives on disclosure of their child’s ASD, particularly in health care settings.
One focus of the literature on disclosure of ASD has been directed to stigma associated with the condition. A general lack of understanding and misconceptions about ASD have been found in both health care and broader contexts, contributing to families’ experiences of social stigma (Drainoni et al., 2006; Hoogsteen and Woodgate, 2013; Lutz et al., 2012; McGonigle et al., 2014; Martin, 2012; Quirantes, 2009; Wnoroski, 2008; Woodgate et al., 2008). In a study by Lum et al. (2014), stigmatizing behavior on the part of HCPs proved to be a barrier to patient dis-closure. In an effort to manage stigma, individuals and their families have employed strategies that allow them to make decisions around the delivery of their information (Birenbaum, 1970; Farrugia, 2009; Goffman, 1963; Green et al., 2005; Herman, 1993; Schneider and Conrad, 1980; Tröster, 1997; Voysey, 1972). In one study, parents of children with ASD utilized medical knowledge of ASD as a strategy for explaining their child’s behavior and resisting stigma (Farrugia, 2009). A deeper understanding of the factors involved in the disclosure process, particularly for families of a child with ASD, has yet to be explored.
Initiation of disclosure of patient information can be complex, particularly in health care settings. Some families may be reluctant to disclose on their own, some may disclose only if asked, whereas others may freely disclose. Similarly, HCPs may vary in their feelings and comfort about asking for information that may be perceived as non-medical. Research has focused on various perspectives regarding the onus of responsibility during a disclosure. In Lunsky et al.’s (2008) study on emergency psychiatric services for adults with intellectual disabilities, HCPs identified that the lack of background information about patients was problematic, and that the lengthy time needed to gather such information created barriers in the ED. Thus, HCPs in the study recommended that both caregivers and patients be trained on how to provide this information in the ED. Other research has reinforced the need for HCPs to be trained in obtaining this information through taking histories from patients with special needs (McGonigle et al., 2014; Pratt et al., 2012), and by asking parents of children with special needs how to best provide care for their children (Owley, 2004).
This article emerges from a program of research conducted by the authors examining the experiences of children and youth with ASD and their families when accessing pediatric ED care, as well as the experiences of HCPs when providing that care. An unexpected finding from the research revealed that the child’s ASD was not always readily shared with hospital staff, or was disclosed with hesitancy on the part of parents. Study data also revealed that HCPs had thoughts about the disclosure process, including the benefits and risks related to disclosure. Based on these findings, the authors performed a secondary analysis of the data exploring themes related specifically to disclosure of a child’s ASD. The purpose of the secondary analysis was to address the following questions: (a) What do parents and HCPs see as being the benefits and risks of disclosure? (b) What are parent and HCP experiences of care delivery after a disclosure occurs? (c) What are suggestions for improving the process of disclosing ASD?
Methods
The overall study employed qualitative methodology and a grounded theory approach, wherein theory is developed from an analysis of themes and categories discovered in the data (Corbin and Strauss, 2008). Qualitative methodology was selected as it is suited to discovering social experience and meaning (Denzin and Lincoln, 2000). In-depth qualitative interviews yielded key concepts, processes, and relationships between themes as related to ED care and delivery for families and HCPs. Grounded theory was also employed in the secondary analysis to develop a theoretical understanding about the phenomenon of disclosure.
The overall study sample was recruited from the EDs of two Canadian high-acuity, specialized pediatric health care settings. Recruitment and study participation occurred between 2012 and 2014. Parents were recruited by ED HCPs after disclosure of a child’s ASD to ED staff. Interested parents were contacted by a research coordinator shortly after their ED visit to obtain informed consent, participate in an interview, and complete quantitative measures and demographic information forms. Parents were also asked to nominate an HCP that was involved in their child’s care to participate in an interview. If a name was not provided or the HCP was unable to participate, another HCP involved in the child’s care was approached. Participants were interviewed about their experiences with either providing or receiving care during a recent ED visit as well as about suggestions for improvement in ED care. Length of time between initial ED visit and participant interviews ranged from weeks to a number of months due to instances of limited availability of some participants. Interviews were semi-structured, based on an interview guide, and conducted by graduate-level research assistants. Interviews were audio-recorded and transcribed verbatim by contracted individuals at each study site. Team members provided guidance to research assistants through both discussion and review of interview transcripts. Across both study sites, 144 families were approached to participate in the overall study; 106 agreed to be contacted by a research coordinator; 31 parents (representing 29 families as two interviews included two parents being interviewed together) and 22 HCPs participated in interviews in the overall study. Reasons for non-participation included not being able to re-connect with families despite multiple attempts, families’ busy schedules, or families experiencing ongoing crises that prevented their full participation.
All parents who participated in an interview disclosed their child’s ASD to an HCP, with the majority of participants explicitly mentioning their experiences with dis-closure in their interviews. During the interviews, these parents shared the circumstances around their disclosures, and HCPs shared opinions about the relevance of disclosure and their expectations around disclosure with parents. Participants revealed rich and insightful information on the topic, thus making this secondary analysis feasible. This secondary analysis comprised 28 parents (representing 26 families as two interviews included two parents being interviewed together) and 16 HCPs across both study sites.
Data analysis
Although not specifically solicited in the overall study, issues related to ASD disclosure and communication were commonly identified. This led to a more targeted analysis of the data, wherein the authors re-analyzed and coded the data for themes related to disclosure of a child’s ASD diagnosis. Both parent and HCP data were analyzed and integrated into the analytic process. Codes were reviewed and subsequently condensed to the themes presented in this article. Interview transcripts were analyzed using computer-based data management and analysis software, NVivo 10, which aided in the importing, coding, and analysis of data. NVivo is a software program that supports qualitative research by allowing users to analyze and organize qualitative data like the interview transcripts involved in this current study (QSR International, 2012). The following coding methods were implemented (Corbin and Strauss, 2008):
Open coding: Preliminary codes were derived through in-depth analysis of transcripts.
Axial coding: Categories were further developed and themes emerged.
Selective coding (Strauss and Corbin, 1998): Themes were further refined and a larger schema was developed.
The strategy of comparative analysis was employed, wherein all coded data were compared and contrasted. Emerging codes were added to the schema in this way, resulting in increased clarity of themes and depth of analysis (Corbin and Strauss, 2008). Sufficient data were collected to substantively and adequately develop each thematic category, while accounting for identified variation. This allowed for conceptual saturation to be achieved (Corbin and Strauss, 2008).
To address rigor and trustworthiness (Corbin and Strauss, 2008; Guba, 1981; Krefting, 1991; Lincoln and Guba, 1985; Sandelowski, 1986), the following strategies were used: (a) peer debriefing through regular team meetings discussing and clarifying emerging coding categories, (b) “memoing” thoughts and reactions during data collection and coding (Corbin and Strauss, 2008), and (c) the use of reflexivity to explore any potential researcher biases (Fossey et al., 2002; Guba, 1981; Hall and Callery, 2001; Rice and Ezzy, 1999). The process involved monthly team telephone meetings, with frequent communication occurring between meetings as well. These regular discussions involved reviewing and revising emerging themes as well as reviewing quotes and language of participants. This helped to ensure consensus around themes. Six Delphi consultation sessions were held across both sites with parents of children and youth with ASD, ED HCPs, and ED administrators who may or may not have been involved in initial interviews (Nicholas et al. in press). Feedback was requested from participants about study results as well as future research and policy objectives.
Results
Parents in our sample represented diverse cultural backgrounds and countries of origin. In addition, various family constellations were reported, with the majority of families comprising nuclear or blended families. HCPs varied in their roles and years of experience in their current positions. Presenting concerns for children in the ED were primarily medical in nature, including gastrointestinal issues, respiratory issues, flu symptoms, and injuries (see Table 1 for participant demographics).
Parent, child and health care provider demographics.
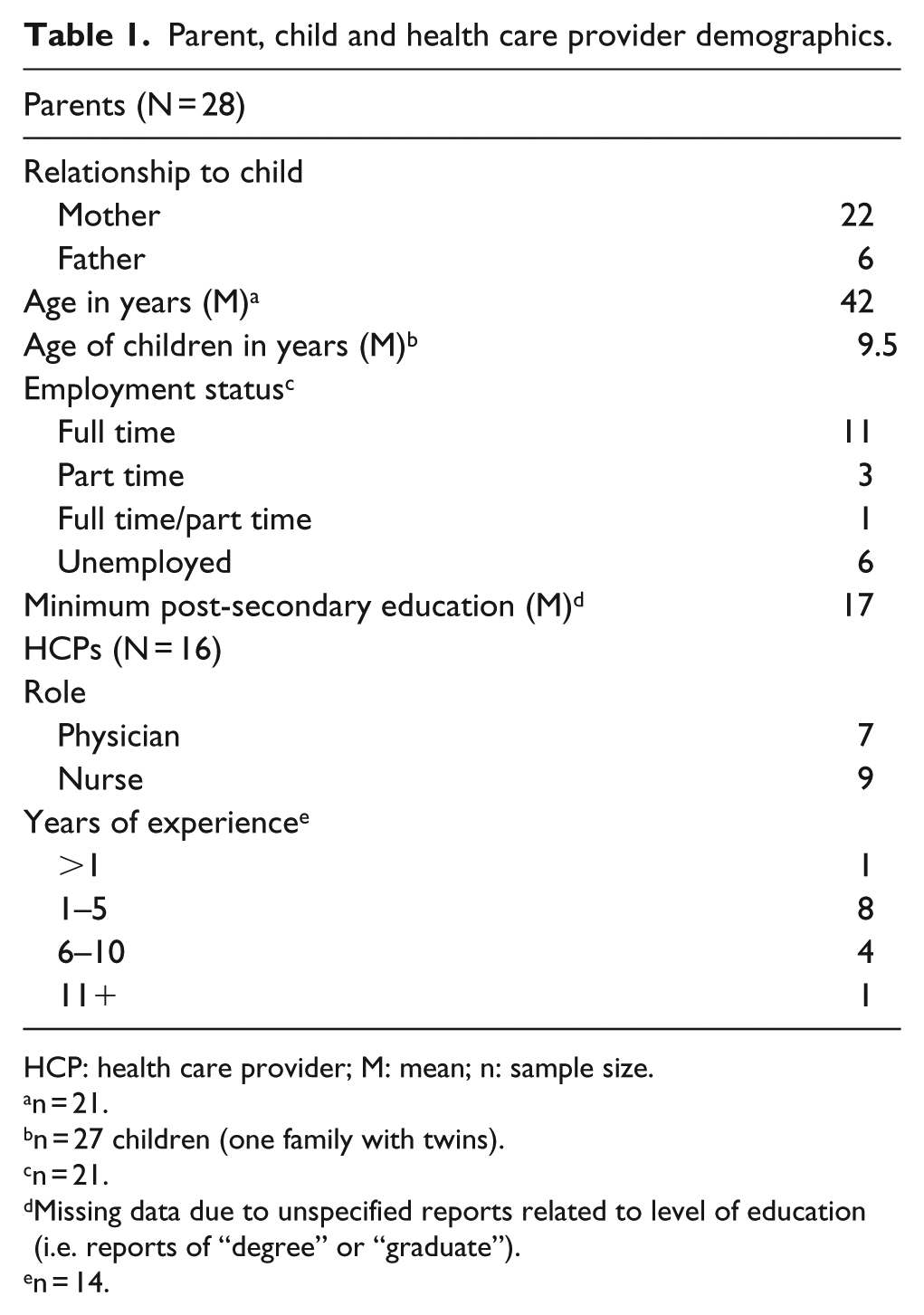
HCP: health care provider; M: mean; n: sample size.
n = 21.
n = 27 children (one family with twins).
n = 21.
Missing data due to unspecified reports related to level of education (i.e. reports of “degree” or “graduate”).
n = 14.
Three broad themes emerged relative to parental disclosure of a child’s ASD in the ED: the benefits and risks of disclosure, outcomes in care delivery resulting from a disclosure, and recommendations for improving the process of disclosing and communicating information. Sub-categories emerged within the respective themes, each of which is described and illustrated below.
Decision to disclose
All parents in the study disclosed their child’s ASD; however, some described a process of considering potential benefits and risks prior to doing so. Reasons for disclosure identified by parents included the following: to assist HCP understanding of the child and to avoid the child being perceived as “badly behaved,” to expedite service, and to prepare HCPs to provide care suited to the child’s needs. Alternately, risks related to disclosure included the potential for negative labeling associated with ASD and reluctance to disclose in front of the child.
Benefits of disclosure
To increase understanding and avoid child being perceived as badly behaved
The avoidance of the child being perceived as badly behaved was a motivating factor for some parents when disclosing their child’s ASD. As one parent said,
… I never want his disability to come across as willful bad behavior and for him to be looked upon poorly as though this is a cognitive decision that he is making to have the anxiety and the issues … (Parent of 13-year-old boy)
Another parent reinforced this belief:
… we told the paramedics, we told the nurse in Triage … just because, I mean, some people think … you need to control your son, he’s (a) spoiled brat, he’s not doing this. No, that’s not the case … It’s more than that … it is a diagnosis … He is autistic … (Parent of 8-year-old boy)
This sentiment was also echoed by HCPs when commenting on the benefit of disclosure in reducing judgments and negative labels:
… if it’s [child’s ASD] not disclosed to us, we could be thinking … this kid doesn’t listen or he’s such a brat … those labels may become attached to the child and/or family when maybe we would have appreciated a little bit differently, had we known that diagnosis. (Nurse)
Expediting service
While parents understood the structure of the ED triage system, many spoke about the challenges for their child while waiting for ED care. Some described how this impacted their decision to disclose, as explained by one parent:
… In the case of an emergency room, if it’ll help us get through there faster, honestly, that’s the reason [for disclosure]. And I don’t mean to think that my son’s more important than any other child, by all means if my son only had a minor injury or something that could wait then … I wouldn’t try to push it … (Parent of 10-year-old boy)
Another parent similarly described the hope of expedited service in the ED:
I was kind of hoping that once they knew he had autism that they might see him a little quicker … But at the same time there were two or three ambulances in that night … it’s hard for him to wait, but life threatening injuries … (are) more important. So I was okay with that. (Parent of 11-year-old boy)
Preparation of HCPs to provide care suited to the child’s needs
Parents reported disclosing to HCPs as a way of preparing them to effectively care for their children. Parents hoped that disclosure would increase awareness around a child’s communication challenges and sensory needs, and encourage the implementation of suitable accommodations. As noted by one parent, “… Whether it be autism or any other social disorder or mental disorder, you need to know this when you’re going in …” (Parent of 3-year-old girl). As reported by another parent, “… we always explain the circumstances … like this is the situation, he’s gonna get a little bit tense, kind of getting a little bit anxious, what can we do about it?” (Parent of 17-year-old boy). Another parent stated,
… I always let them know … they need to know that he’s autistic and non-verbal when they’re practicing whatever medicine they have to practice at the time, whatever steps they have to take for whatever injury could be, I want them to know. I just want them to know every aspect of it and be prepared … (Parent of 10-year-old boy)
This need for HCPs to know about their child’s ASD was further illustrated by another parent:
… your child is different, therefore they should be treated in a different manner … it should be front and center and very well-known because then they [HCPs] have the right tools to deal with the right situation. They’re not walking in with their NT, which is neuro typical, toolbox, then they can walk in with their ASD toolbox. This is my autism spectrum disorder toolbox. And they can walk into a situation having the right tools to deal with that … (Parent of 13-year-old boy)
Similar to parent reports, HCPs noted the importance of knowing about a child’s ASD diagnosis. As stated by one HCP, “As soon as we’re starting to get information from them … anything that could affect what happens while they’re here … is important to know right away” (Nurse). Another HCP stated, “I would say it’s [ASD diagnosis] very important because it really changes how I do my assessments and the kind of care I give to the patient” (Nurse). HCPs reported that disclosure allows them to prepare prior to interacting with a family:
… when parents are forthcoming with information about their own child, it really helps us, we know in advance how we psychologically and mentally prepare ourselves better to take care of their needs and we put our thinking hat on. (Physician)
HCPs also agreed that disclosure facilitates appropriate accommodations:
… if we know from the get-go, it’s easier for us to say like, are you okay waiting in the waiting room for a few minutes, or do you think it would be better to step into the atrium or should we get you right into a room and sort of take those steps … if they’re able to be more forthcoming, then we’re able to meet their needs better … (Nurse)
Risks of disclosure
Negative attributions related to ASD
Some parents reported a hesitance to disclose their child’s ASD in the open, public venue of the ED for fear of negative attributions related to ASD. Parents were concerned about their child being labeled as not “normal,” and that their child might internalize these labels. As explained by one parent, “… I would prefer not to disclose that information [publicly]; people start looking at my daughter in different ways” (Parent of 7-year-old girl). One parent indicated that these concerns were a reason for not disclosing her son’s autism in her daily life; however, she acknowledged the benefit of disclosing in a hospital setting:
… We don’t like (child) … to be labeled at all … we want him to feel as normal … and as included as possible … We never really openly speak about it and let people know so that they look at him differently … We thought in a hospital setting that was important … we felt … medically that was useful … for the doctors and the hospital to know … (Parent of 6-year-old boy)
HCPs acknowledged these potential risks experienced by parents when describing how they question parents once they suspect some sort of unique difference in the child. As one HCP noted, “We basically prompt it—we don’t actually say … does your child have autism? Because I think it could be a sensitive subject to the families, …” (Nurse). This point was echoed by another HCP: “ … [disclosure] may be challenging for some people especially if, something like autism is a barrier for that family to kind of accept or disclose” (Nurse).
Reluctance and risks of disclosure in front of the child
A few parents in our sample described particular reluctance to disclose in front of their children. As relayed by one parent,
… I don’t like saying well, he’s Autistic … in front of my son because you become your diagnosis … I really think it’s important for [child] to … realize that he is not ASD; he is [child] and he will grow up to be what he needs to be. So if I’m constantly saying it front of him, you know, I don’t like doing that … (Parent of 8-year-old boy)
Another parent requested that his child’s special needs already be noted in her medical file, “… so I don’t have to explain to them in front of my child, that you know, she’s autistic and because she doesn’t even know that yet …” (Parent of 7-year-old girl).
Similar to parent reports, HCPs considered that stigma and negative labeling may contribute to parents’ decisions to disclose or not disclose, and that the child being present might act as an additional barrier to disclosure. As one HCP noted, “so definitely if the child is in the room … That can influence whether they [parents] say something or not … sometimes they wait for the child to leave the room, before they say something” (Nurse). Similarly, another HCP noted that
… there [are] peoples’ perceptions … your child is, you know, wild and because you didn’t enforce anything when they were growing up and you let them do whatever they want … I feel like a big part of it is negative perceptions of other people and then they [parents] internalize that … (Nurse)
Outcomes of a disclosure
Accommodation
Some parents reported satisfactory accommodation following the disclosure of their child’s ASD. As described by one parent, “… perhaps maybe the staff were even a step above because they knew she had certain conditions” (Parent of 3-year-old girl). This was similarly relayed by another parent: “… I think when the word autism is mentioned … Everybody was very, accommodating sounds like the wrong word, very understanding, wanted to be proactive, 5 stars across the board to everybody …” (Parent of 13-year-old boy).
Communication of ASD diagnosis
Some parents reported that their child’s health information was noted in the ED medical record and disclosed to other HCPs: “… everyone we spoke to seemed to already know he had autism, so that message had been filtered which was nice …” (Parent of 13-year-old boy). And, “… I always tell ’em he’s autistic … and they write it down on the chart, so when they come in … it’s usually … on there” (Parent of 9-year-old boy). Alternatively, some participants noted that this was not the case and, in fact, disclosure had to be repeated. As one parent explained, “… I had to explain to the different people who came in that she had autism, they’re like oh okay, but the information wasn’t passed on” (Parent of 3-year-old girl). One parent expressed uncertainty about whether or not HCPs were aware of a diagnosis:
… they would come and they would just start. Like asking him all these questions and they would be like long complicated questions and just talking too much and confusing him … Just I would wonder did they read his information. (Parent of 3-year-old boy)
HCPs acknowledged these parental frustrations, as illustrated in the comments of one HCP:
… in a teaching institution like this, everybody’s required to take their own history and physical. So they have to ask again. And that is a frequent complaint when people come to the emergency department is that they are saying the same thing … (Physician)
Lack of understanding about ASD
Some parents reported a lack of understanding about ASD among HCPs following their disclosure. One parent felt that an HCP made an assumption regarding her child’s communicative ability, specifically that the child’s symptoms were related to her ASD as opposed to a medical condition:
… there was a definite assumption made when I told them that she was only (on the) autistic spectrum that they assumed she was nonverbal … I really feel like he pigeonholed her. And then I almost said, Ok forget I said that because he was so going down that line that he wouldn’t, perhaps, look at other things … (Parent of 17-year-old girl)
Recommendations
Means for improving communication were suggested by participants. Parents recommended that an “alert” be placed in the child’s file, to facilitate the transfer of information about a child’s special needs. Some parents described that this may alleviate the responsibility placed on them to repeatedly disclose to multiple HCPs as well as reduce feelings of discomfort around public disclosure. One parent suggested that formal notification of a child’s disability be accessible system-wide:
There still should be a big red tag on their file because they are not 100% the same as a regular child. In other words, if everybody else has got a green tag, special needs children should have a red one … (Parent of 11-year-old boy)
Parents also suggested that HCPs ask questions about how to adapt care to the needs of the child. As one parent noted,
as soon as they find out a kid’s got autism, they need to ask these questions … you know like the old saying, if you meet one kid with autism, you’ve met one kid with autism. Because they are so different. (Parent of 8-year-old boy)
As another parent noted, “… maybe it could be a question like, does your child have any special needs? … Very open … so it’s not so voluntary” (Parent of 8-year-old boy).
HCPs described their experiences with how information may be obtained from parents:
… when you ask does this child have any past medical history and the parents say no, you’re sorta fishin’ around … until you actually come right (out) and say does your child have a history of autism? … it’s awkward because if they don’t have a history of autism and you’ve just put that label out there, the parents can then be offended … Unless the parents are forthcoming with that information right off the bat it can be a little bit delicate trying to find that information out. (Nurse)
Discussion
This article explored the communication of a child’s ASD in pediatric ED settings. Even among this sample of parents who shared information related to their child’s ASD, the decision to disclose was not always straightforward, with some parents weighing both benefits and risks of disclosure. These findings illustrate the need for greater awareness of the intricacies related to this issue for both parents and HCPs.
The reasons for disclosure described by parent participants included the need to help HCPs understand and accommodate their children’s needs and to potentially expedite service. This desire to expedite service was also reported in Muskat et al.’s (2015) study, when parents described the challenges faced by their children during waiting and transitions over the course of planned hospital visits. Participants in that study explained the importance of flexibility in HCPs’ approach and, thus, the “need to know” when working with children with ASD (Muskat et al., 2015). HCPs in our sample identified the need to obtain information about a child’s ASD, consistent with previous research on the importance of providers communicating with caregivers around a child’s history and needs (Mackenzie et al., 2013; Vaz, 2010).
Concerns about negative labeling attributions were also identified as contributing factors in parents’ decision to disclose. Intriguingly, both disclosure and non-disclosure were considered to be potential safeguards against stigma. Some parents feared that not disclosing would leave their child vulnerable to negative attributions about their behavior and thus chose to disclose their child’s diagnosis. Alternatively, others worried that choosing to disclose would result in their children being looked at as “different.” These parents were particularly reluctant to disclose publicly and in front of their children. The fact that decisions related both to disclosure and non-disclosure reflected parents’ attempts to limit stigma speaks to the pervasiveness of this phenomenon in the lives of families affected by ASD. Advancing understanding and decreasing negative attitudes and responses are priorities in moving forward.
Varying levels of their children’s understanding of ASD, the risk of them internalizing the ASD label, and feeling forced to publicly disclose were among reasons for hesitancy around disclosure. These impeding factors were ultimately balanced with parents’ understanding of the benefits of disclosure within an ED setting. It is possible that the decision to disclose was dependent on context for parents, with recognition of the need for disclosure being greater in the ED than in other settings. This may be identified as a form of selective disclosure of information that is shared in some circumstances while hidden in others (Corrigan and Rao, 2012; Herman, 1993; Mason et al., 2014; Schneider and Conrad, 1980; Tröster, 1997). While research is scarce around selective disclosure in acute health care settings, data from this study indicate that a “need to know” exists within this setting.
Parents shared their experiences with HCP approach and communication of their child’s health information following a disclosure. Many parents felt that HCPs were able to accommodate and adjust their approaches. Some parents also reported that their child’s ASD was recorded in the child’s chart and that HCPs involved in the child’s care were aware of the condition. However, some parents reported that disclosure had to be regularly repeated and that a lack of understanding about ASD may have impacted their child’s care. Parents offered recommendations aimed at mitigating potential barriers before and after a dis-closure occurs. Parents suggested that staff ask questions about a child’s needs and that these special needs be noted in the health record as an “alert.” This is similar to other recommendations around noting patients’ learning disabilities in their health records (Royal Society for Mentally Handicapped Children and Adults, 2004). Pratt et al. (2012) made similar recommendations and consequently developed a comprehensive checklist to gather health information from families with a child with ASD and to assign a specific provider to gather this information from parents. For the parents in this current study, this strategy would likely align itself with their goals around disclosure and communication of their child’s needs.
Based on these results, it appears that disclosure assists HCPs in understanding and effectively caring for a child with ASD in the ED. However, disclosure is not a straightforward option for families but rather is layered and purposeful. Similarly, HCPs are not always clear about how to approach the issue and how to make families most comfortable. HCPs are also tasked with managing competing demands throughout the ED. Currently, there is a shortage of training resources for frontline ED staff, further inviting the development of information, tools, and materials (McGonigle et al., 2014). Based on this gap in resources as well as our team’s research, we believe that a hospital-based tool aimed at facilitating communication between parents and HCPs would be an appropriate next step to explore. We also recommend that future research about disclosure include individuals who have decided not to disclose. This would provide deeper understanding into this decision-making process. Increased awareness of the dynamic interplay of factors occurring around disclosure may encourage sensitivity and discussion about how to facilitate this communication in a safe and productive way.
Limitations
This study has a number of limitations. First, only the perspectives of parents who voluntarily disclosed their child’s ASD were included as it was not possible to independently verify potential missed cases of ASD using other data sources. Thus, the perspectives and experiences of parents who did not disclose their child’s ASD during their ED visits were not included. The lack of inclusion of these families creates a gap in data related to the experiences of those choosing not to disclose. Concerns about disclosure among families who share information about the child’s condition with HCPs may be just the “tip of the iceberg” relative to concerns that ultimately lead other families not to disclose. As well, the study was conducted at two large tertiary, urban pediatric health care settings and thus may not represent experiences of families at smaller, rural, or general hospital settings. Furthermore, the presenting concerns of the children in the sample were largely medical. While children and youth presenting in the ED with mental health concerns were recruited into the larger study, ongoing mental health issues prevented them and their families from actively participating in interviews for the study. This limited the inclusion of disclosure experiences from these families. Similarly, there was a significant disparity between participants who enrolled in the study and the number of participants recruited into the study due to lack of availability or unsuccessful attempts at re-contacting participants. In turn, this limited the study’s sample size. Finally, length of time between ED visits and interviews may have impacted participants’ recall and perceptions of their ED experiences.
Conclusion
The findings from this study highlight the complexity surrounding disclosure of ASD by parents of pediatric ED patients. Best practices and clinical guidelines around ASD disclosure are not yet well developed, and the range of experiences with disclosure had by families and their HCPs invites practice and program advancement. Frontline staff, policy-makers, and health care consumers have an important role in this conversation, with a common goal of ensuring that salient information is conveyed within the clinical encounter to optimize care for children and youth with ASD and their families.
Footnotes
Acknowledgements
Withheld to protect anonymity during peer-review process. The authors would like to thank the parents and health care providers who generously gave their time to participate in these interviews.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project/research activity is supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under co-operative agreement UA3 MC11054—Autism Intervention Research Network on Physical Health (AIR-P). This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the US Government. This work was conducted through the Autism Speaks Autism Treatment Network serving as the AIR-P.
Research ethics
Institutional Research Ethics Board approval was obtained at both study sites: Research Ethics Board at the Hospital for Sick Children (File no. 1000034237 withheld to protect anonymity during peer-review process) and Health Research Ethics Board at the University of Alberta (File no. Pro00030375 withheld to protect anonymity during peer-review process).