
Abstract
Autism spectrum disorder-specific knowledge deficits contribute to current disparities in the timing and quality of autism spectrum disorder services throughout the United States and globally. This study conducted a systematic review of Western and International literature to examine measures used to assess autism spectrum disorder knowledge. This review identified 44 unique autism spectrum disorder knowledge measures across 67 studies conducted in 21 countries. Measures used in each study were evaluated in terms of psychometric strength. Of the 67 studies reviewed, only 7% were rated as using a measure with strong psychometric support compared to 45% that were rated as using a measure with no reported psychometric support. Additionally, we examined content overlap and subdomains of autism spectrum disorder knowledge assessed (e.g. etiology, symptoms) and cross-cultural adaptation procedures utilized in the field. Based on these findings, the need for a cross-culturally valid and psychometrically sound measure of autism spectrum disorder knowledge is discussed and recommendations for improving current assessment methods are presented, including suggestions for measure subdomains.
Keywords
Introduction
Low levels of autism spectrum disorder (ASD)-specific mental health literacy (MHL; Jorm, 2012) or knowledge about ASD symptoms, etiology, and treatment can increase the amount of burden experienced by families with children diagnosed with ASD (e.g. Kuhn and Carter, 2006; Obeid and Daou, 2015), and programs designed to educate parents about ASD result in significant stress reduction among parents (for a review, see Schultz et al., 2011). Variability in ASD awareness around the world contributes to vast service disparities, particularly in low- and middle-income countries (Grinker et al., 2011), contributes to the proliferation of stigmas and misconceptions that disadvantage families (Khan et al., 2012), and may impede epidemiological efforts (Elsabbagh et al., 2012). In spite of the heightened awareness of ASD in Western countries, many minority groups in countries such as the United States also face disparities attributable to low ASD knowledge. For US minority groups, knowledge barriers may include lower levels of formal education, less autism-specific knowledge or understanding, and fewer sources of ASD knowledge (Magaña et al., 2013; Mercadante et al., 2009; Zuckerman et al., 2013). Theorists have hypothesized that discrepancies in ASD identification may result from variability in the amount of knowledge of typical developmental milestones across groups (Mandell et al., 2009). Additionally, research has shown that maternal education and sources of ASD knowledge mediate the association between ethnicity and the number of ASD services received (Magaña et al., 2013). Such findings suggest that increasing ASD-specific knowledge would help to reduce known disparities; therefore, the ability to thoroughly assess this construct is important.
Given that disparities in ASD knowledge have become a prominent cause for concern, both in the United States and internationally, raising global awareness of the burden of disorders, such as ASD, has been included as a goal for addressing the grand challenges in global mental health (Collins et al., 2011). In line with this goal, specific efforts to increase global ASD awareness have begun (e.g. Obeid et al., 2015; Wallace et al., 2012) and research focusing on quantifying ASD knowledge deficits has started to emerge. Identifying reliable assessment methods to quantify ASD knowledge is an important step toward increasing global ASD knowledge. Effective measures for quantifying ASD knowledge and stigmas can help to improve conditions in two meaningful ways: (a) they can facilitate the identification of knowledge deficits in specific domains so that interventions can be tailored to increase effectiveness and (b) we can use these measures to examine the efficacy of intervention approaches designed to increase ASD knowledge.
Unfortunately, the rapid progress in the field of ASD knowledge assessment and the ubiquitous focus around the world has led to the introduction of some methodological concerns in this literature base. Such concerns include limited emphasis on best practice psychometric standards, a lack of method consistency and limited study replication, a failure to examine different subdomains of ASD knowledge, and concerns about cross-cultural measurement adaptation procedures. Published guidelines for robust scale development include the following steps: (a) originate with a clear construct conceptualization and test a comprehensive item pool, (b) statistically examine the scale validity (e.g. unidimensionality) using an approach such as confirmatory factor analysis, (c) assess scale reliability, and (d) establish normative data (Cicchetti, 1994; Clark and Watson, 1995; Gerbing and Anderson, 1988). However, the extant research examining ASD knowledge has largely failed to adhere to these psychometric standards.
Research has examined the construct of ASD knowledge using a range of different assessment approaches (e.g. responding to questions following ASD vignettes and true/false or Likert-style response options for factual questions), and there is little consensus regarding the most effective method. Additionally, most measures of ASD knowledge appear to examine the broader construct of ASD rather than particular elements of MHL such as symptoms, etiology, and treatment. This more in-depth understanding is critical for designing targeted interventions (Jorm, 2012). Given the global importance of evaluating ASD knowledge and stigmas to improve ASD awareness (Khan et al., 2012), there is a particular need for a measurement tool that has cross-cultural utility but also meets robust psychometric standards. While the ability to tailor a questionnaire to a particular region or sample is important, it need not occur at the expense of standardization.
To date, the most widely acknowledged measure used to assess autism knowledge is the autism knowledge survey (AKS; Stone, 1987), a Likert-style questionnaire comprised of ASD-facts for which respondents rate their agreement. An analysis of the original survey revealed that it was unidimensional, had reasonable internal consistency (alpha = 0.66), stable reliability, and showed initial reasonable validity (Campbell et al., 1996). The measure has since been revised multiple times to reflect new knowledge informed by research in the field of ASD. The first revision occurred in 2007 (AKS-R; Swiezy, 2007) and was used in several subsequent studies (Bauer et al., 2015; Hartley-McAndrew et al., 2014; Tipton and Blacher, 2014). The measure was revised again in 2015 by a different group of researchers, who adapted the AKS to align with the Diagnostic and Statistical Manual of Mental Disorders–5th edition (Gillespie-Lynch et al., 2015; Obeid et al., 2015). These different versions of the AKS have been used primarily in the United States to demonstrate knowledge variability across various respondents (e.g. caregivers, educators, mental health professionals, and individuals in the medical field; Ables et al., 2011; Campbell, 2008; Hartley-McAndrew et al., 2014; Tipton and Blacher, 2014), but also to measure the outcome of interventions designed to improve ASD knowledge and stigmas (Bauer et al., 2015; Gillespie-Lynch et al., 2015). While there has been some initial use of this measure in cross-cultural contexts (Hoekstra et al., 2014; Obeid et al., 2015), little has been published about the specific nature of cultural adaptations to the measure, which seems to primarily reflect Western-specific knowledge of ASD. Additionally, despite the wide use of AKS revisions in the field, little psychometric data for these updated versions exist. While this measure has provided an excellent start to ASD knowledge assessment, its limited psychometric support and undocumented cross-cultural adaptations pose a problem.
In this article, we review existing peer-reviewed research articles that utilize quantitative instruments to examine ASD knowledge from around the world, and provide an evaluation of the methodological strengths and weakness of this literature. The different methods used for assessing the construct of ASD knowledge and the psychometric support of these methods are examined in detail. In addition to discussing psychometric considerations, we will review questions pertaining to where, how, and among whom ASD knowledge research is being conducted. We provide both an overview of existing measures as well as recommendations for making methodological improvements to future measures designed to quantify ASD knowledge.
Method
A systematic search of empirical research focused on the assessment of ASD knowledge was conducted to identify studies relevant to the current review. PsycINFO, Web of Science, and Google Scholar were used to identify literature. Authors searched for articles using the following keywords: knowledge, awareness, or understanding, and autism. Titles and abstracts of obtained articles were reviewed to eliminate duplicates and exclude irrelevant studies. The text and reference sections of the remaining articles were then reviewed to identify additional relevant studies and to confirm that each study satisfied the criteria for inclusion in the review. Inclusion criteria were as follows: (a) the article must feature a survey instrument used to specifically assess ASD knowledge with quantitative methods and (b) the article must be published in a peer-reviewed journal prior to November 2015. Assessment instruments were considered distinct if they had less than 50% of items with near identical wording derived from a pre-existing measure.
The review included both domestic and international articles and we report the location of data collection in alignment with the global category assignment used in Elsabbagh et al. (2012). After identifying all relevant articles, information was extracted about the characteristics of the participants for whom autism knowledge was assessed (e.g. participant age, profession, and other descriptive factors relevant to study inclusion). Data were also collected about the assessment measure used, including the number of items, and the method of assessment used to quantify the construct of ASD knowledge (e.g. checklist, true/false questions, multiple choice, semi-structured interview, and vignette). We also examined measure subdomains and assessed the most frequent words used in each measure to get a sense of coverage within identified subdomains or subscales of autism knowledge (e.g. etiology, symptoms, treatment).
In order to compare psychometric properties across studies, we assigned each instrument a rating of psychometric strength in alignment with operational definitions (Table 1). Instruments were rated as having “strong psychometric evaluation,” “modest psychometric evaluation,” “weak psychometric evaluation,” or “no reported psychometric evaluation.” Once validity or reliability was published for a measure, subsequent publications using the same measure were coded with that score or higher depending on elaborations to reliability and validity so the highest score possible could be assigned.
Operational definitions of psychometric support.

ROC curve: receiver operating characteristic curve.
To evaluate the presence of subdomains, we first noted whether the authors reported formal subscales or clear subdomains comprised of a specific collection of items. We also examined themes in measure content to measure the amount of overlap and to identify commonly occurring subdomains of ASD knowledge. To do this, we used NVivo (version 10 for Windows) qualitative coding software (QSR International Inc, 2015) to look for trends in word frequency. We conceptualized three distinct subdomains of ASD knowledge: (a) symptoms or diagnosis (including comorbidity), (b) etiology (including population prevalence variability), and (c) treatment and outcomes. Using operational definitions, three coders examined the top 99 keywords identified using NVivo software and coded each word into one of four categories: either a general word or as a word in one of three subdomains of ASD knowledge (symptoms, etiology, or treatment). Consensus coding was utilized to reconcile initial differences in codes.
Results
Overview of existing research
The previously described literature search resulted in 67 total peer-reviewed articles that used some form of questionnaire to examine ASD knowledge. Although the initial ASD knowledge articles were published in the 1980s, this has become a more popular area of study in the past decade. More specifically, 85% (n = 57) of the reviewed articles have publication dates in the past 10 years and of these, 49 were published in the past 5 years and 14 in 2015 (see Appendix 1).
Research examining ASD knowledge has occurred in 21 different countries around the world, 52% (n = 35) were conducted in North America (United States or Canada), 14% (n = 9) in the Eastern Mediterranean region (including, Palestine Authority, Pakistan, Saudi Arabia, Oman, Lebanon, and Iraq), 12% (n = 8) in Europe (including, the United Kingdom, Northern Ireland, Greece, France, Denmark, and Poland), 9% (n = 6) in the Western Pacific region (including Japan, China, and Australia), 9% (n = 6) in Africa (Nigeria), 3% (n = 2) in Southeast Asia (including India and Nepal), and 1% (n = 1) in South America (Brazil). The countries in which ASD knowledge has been studied most widely (e.g. those with three or more publications on this topic) include the United States (n = 34), Nigeria (n = 6), Pakistan (n = 4), and Australia (n = 3). See Appendix 1 for specific details regarding the country of origin of each article included in the review.
Across the studies reviewed, there was a wide variety regarding the target populations investigated. The reviewed studies included between one and six different target groups. Target populations ranged from peers and parents to professionals. The most widely studied population consisted of various medical professionals such as pediatricians, general practitioners, nurses, pharmacists, other specialists, and residents or medical students (n = 27; 40%). In all, 23 studies (34%) included an examination of school professionals (i.e. teachers, speech and language pathologists, school administrators). Seven studies (10%) examined ASD knowledge among mental health professionals such as licensed psychologists or psychiatrists. Totally 20 studies (34%) examined mixed samples comprised of individuals from the lay public, college students, or unspecified ASD experts. Six studies (9%) examined other children including siblings and same-aged peers and four (6%) examined caregiver or parent perspectives.
Assessment methods
Results from this review revealed 44 distinct measures used to assess the construct of autism knowledge. Measures with the same name and citation that appeared in multiple papers were carefully examined and considered distinct if more than half of the questions differed. Measure numbers assigned to each publication are presented in Table 1 to show measure overlap across distinct studies. Of these 44 measures, 84% (n = 37) appear in only one peer-reviewed publication and seem to be created specifically for the study in which they are reported. The most commonly used measures were the AKS (Stone, 1987), the Knowledge about Childhood Autism among Health Workers (KCAHW) Questionnaire (Bakare et al., 2008), the Autism Knowledge Questionnaire (AKQ; Kuhn and Carter, 2006), a revised version of the AKS (Bauer et al., 2015), and the Autism Inclusion Questionnaire (AIQ; Segall, 2008).
Cohen et al. (2008) define a “well-established” measure as one published by at least two distinct research groups. Of the 44 measures examining ASD knowledge, only 7 meet this best practice assessment standard. These included the original AKS (Stone, 1987), the revised AKS (Swiezy, 2007), KCAHW (Bakare et al., 2008), the Knowledge of Autism Questionnaire (KAQ; Ross and Cuskelly, 2006), the AIQ (Segall, 2008), the AKQ (Kuhn and Carter, 2006), the Knowledge of Autism/Asperger Syndrome measure (KAAS; Ross and Cuskelly, 2006), and a measure developed by Ling et al. (2010). Following the original citation, published in the United States, the AKS appeared in four additional studies (Campbell et al., 1996; Heidgerken et al., 2005; Helps et al., 1999; Stone and Rosenbaum, 1988), three in the United States and one in the United Kingdom. Similarly, the KCAHW Questionnaire appeared in four publications following the initial development study (Bakare et al., 2009; Igwe et al., 2010, 2011; Shaukat et al., 2014). Of these studies, four occurred in Nigeria and one in Pakistan.
Psychometric methods used
In addition to examining whether the measures used met replication criterion for a “well-established measure,” set by Cohen et al. (2008), we also rated the reported psychometric evaluation of each article. This was accomplished using the previously mentioned, operational definitions of strong (4), modest (3), weak (2), or no reported (1) psychometric evaluation. Two independent coders who achieved an initial inter-rater reliability of 71.64% rated each article. Rating disputes were resolved via review by a third rater. The average psychometric score of all 67 measures fell just above the “weak psychometric evaluation” rating of 2, M = 2.06 (standard deviation (SD) = 1.06). Of the studies reviewed, 45% (n = 30) were coded as having no reported psychometric evaluation, 12% (n = 8) had weak psychometric evaluation, 36% (n = 24) had modest psychometric evaluation, and only 7% (n = 5; Al-Sharbati et al., 2015; Campbell and Barger, 2011; Furnham and Buck, 2003; Garg et al., 2014; Talib and Paulson, 2015) were coded as having strong psychometric evaluation.
Internal consistency scores were the most commonly reported type of reliability (Bakare et al., 2008; Campbell and Barger, 2011; Campbell et al., 1996; Furnham and Buck, 2003; Garg et al., 2014; Gillespie-Lynch et al., 2015; Haimour and Obaidat, 2013; Johnson and Van Hecke, 2015; Kuhn and Carter, 2006; Mavropoulou and Sideridis, 2014; Obeid et al., 2015; Ross and Cuskelly, 2006; Segall and Campbell, 2012, 2014; Talib and Paulson, 2015), with some studies also reporting test–retest reliability (Al-Sharbati et al., 2015; Bakare et al., 2008; Vijayarani, 2014) or inter-rater reliability (Al-Sharbati et al., 2015). Occasionally, studies reported measure construct validity (e.g. Al-Sharbati et al., 2015; Jensen et al., 2015); however, more commonly authors reported content validity as assessed by informal or formal measure review by experts (e.g. Basha, 2014; Gilliam and Coleman, 1982; Hughes et al., 2012; Johnson et al., 2012). Several studies also used factor analytic statistics to examine subscale properties (Campbell et al., 1996; Furnham and Buck, 2003; Garg et al., 2014; Talib and Paulson, 2015), but few other statistical approaches were implemented to examine measure psychometrics.
Cross-cultural adaptations
While the majority of studies examining ASD knowledge around the world developed novel surveys specific to their culture, others used measures designed for use in one country and adapted it for use in another cultural context. Although multiple measures reported formal translation and back-translation steps (e.g. Voelkel et al., 2013), few reported the steps involved in the cross-cultural adaptation process. For example, Obeid et al. (2015) reported using an “adapted version” of the AKS (Stone, 1987) to compare knowledge among college students in the United States and Lebanon but did not describe any specific cultural adaptations made to the measure to ready for use in Lebanon. Additionally, Shaukat et al. (2014) used a measure developed for Nigeria in Pakistan without providing any information about cultural adaptations. Similarly, while the KAAS was originally developed for use in Australia, the authors who use this measure in Greece (Mavropoulou and Sideridis, 2014) do not discuss whether cultural adaptations were needed to ready this measure for cross-cultural use. Cultural validity was referenced in one instance but with little additional information provided (Igwe et al., 2011). Similarly, Rahbar et al. (2011) only briefly described pilot testing their measure with two individuals to help account for vernacular differences between English spoken in the United States and Pakistan but with few other details.
Different methods for construct assessment
The reviewed studies contained a diverse array of assessment approaches to quantify ASD knowledge. These included the following types of question formats: responses to vignettes, checklists, short answer or interviews, and fact-based questions with multiple choice, True/False or Yes/No, and Likert-scale response options. Among the studies, 24% (n = 16) employed a combination of two or more types of assessment approaches (e.g. True/False, Likert scale, and checklists). Many studies listed phrases or facts about ASD and had individuals respond to either True/False or Yes/No questions (25%; n = 17) or to questions using a Likert scale (25%; n = 17). Additionally, 14 surveys (21%) incorporated multiple-choice questions, two studies (n = 3%) applied interview protocols or had participants respond in short answers, and in one study, (2%) participants responded to questions about a vignette.
Measure unidimensionality and subscales
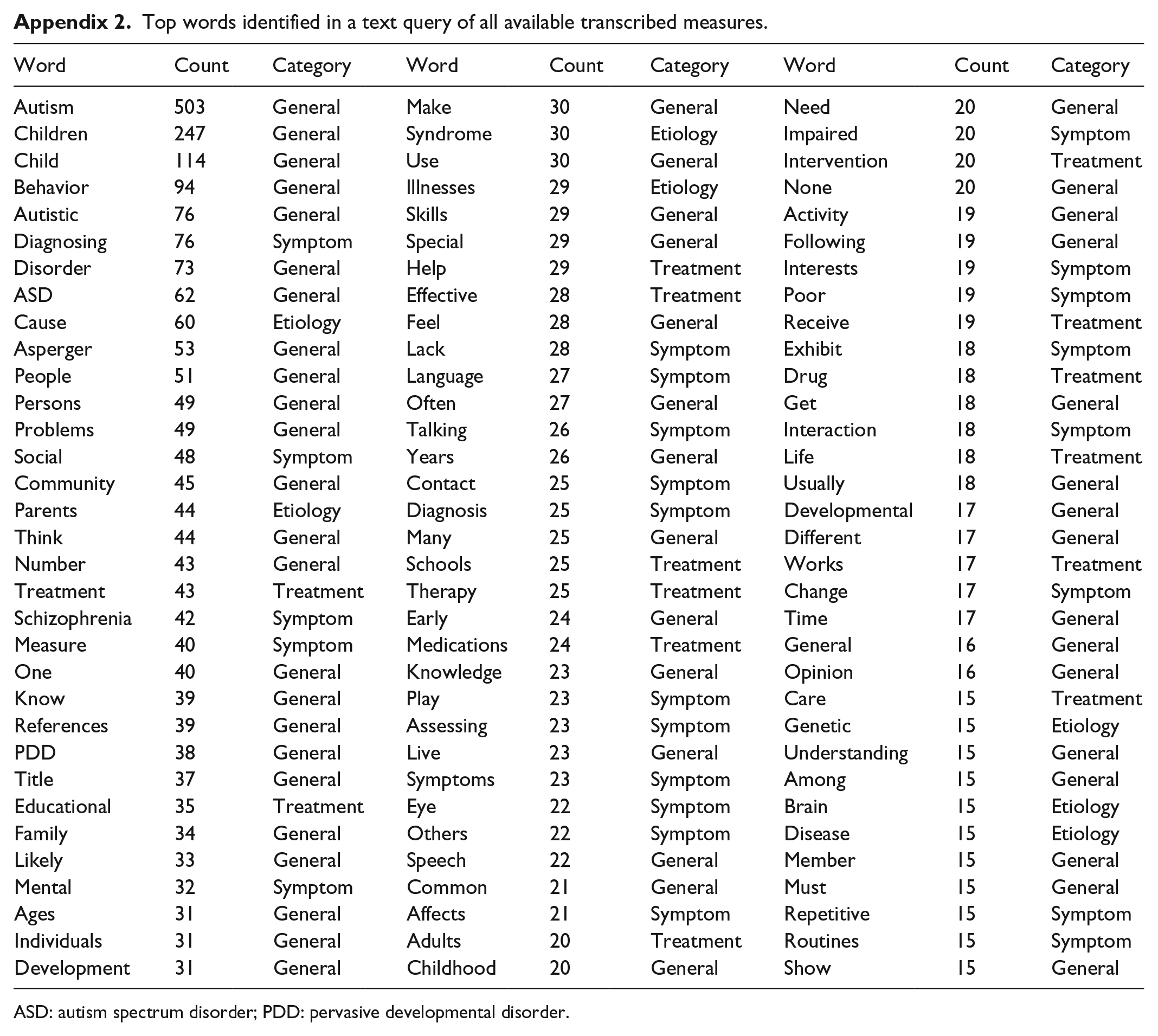
Of 44 different measures, 68% (n = 30) examined specific subdomains of ASD knowledge through the use of subscales, such as diagnosis and symptoms (e.g. Kuhn and Carter, 2006; Segall and Campbell, 2012; Shaukat et al., 2014), etiology (e.g. Bakare et al., 2009; Furnham and Buck, 2003; Koyama et al., 2009), treatment (e.g. Furnham and Buck, 2003; Heidgerken et al., 2005; Koyama et al., 2009), and course and prognosis (e.g. Durand-Zaleski et al., 2012; Ross and Cuskelly, 2006; Stone, 1987). While the emergence of subscales measuring subdomains of etiology, symptoms, and treatment were common, formal inclusion only occurred in less than half of the measures. Therefore, we wanted to examine whether similar topics were covered in the remaining measures. To further examine item content and subdomain coverage, we identified the 99 most commonly occurring words (combing root words only, such as cause and causes or education and educational) across all of the measures for which we were able to transcribe items (n = 38). For a list of these 99 words (see Appendix 2). We coded each of the most common words into the three previously identified subdomains of ASD knowledge: (a) symptoms, (b) etiology, and (c) treatment to determine whether commonly occurring words found across the measures were representative of these subdomain themes. Results of the qualitative data coding of all of the transcribed measures revealed that 45 of the 99 most frequently occurring words were ASD knowledge content specific (e.g. cause, language, intervention) as compared to general terms (e.g. child, number, often). Coding of these 45 content-specific words using subcategory operational definitions revealed that 24 words (53.3%) address the subdomain of symptoms (e.g. diagnosis, symptom, stereotyped), 7 words (15.6%) address the subdomain of etiology (e.g. cause, prevalent, occurs), and 14 words (31.1%) address the subdomain of treatment (e.g. therapy, training, medication).
Discussion
A review of the existing literature examining autism knowledge revealed a recent increase in studies examining this construct in the United States and internationally. In spite of the growing importance of quantifying autism knowledge, a great deal of variability in the current research base makes comparisons across studies challenging. We found that across the 67 published studies included in this review, 44 distinct measures have been used to quantify the construct of ASD knowledge. This large number of measures indicates that instead of identifying a specific measure as a gold standard of ASD knowledge assessment, research groups often newly create a measure each time the construct is evaluated. This makes it difficult to both examine the psychometric properties of any one measure and to compare across studies. This is also indicative of a failure to adhere to the important standard of research replication (Singh et al., 2003). In line with this approach, guidelines for designation as a “well-established assessment” indicate that, among other criteria, a measure must appear in at least two different peer-reviewed articles by different investigatory teams (Cohen et al., 2008). Most measures examined did not meet the definition for a “well-established assessment” as most researchers developed independent surveys for their specific studies. As evidence of this, among the 44 measures examining ASD knowledge, only seven meet this best practice assessment standard (AKS (Stone, 1987), revised AKS (Bauer et al., 2015; Swiezy, 2007), KCAHW (Bakare et al., 2008), KAQ (Ross and Cuskelly, 2006), AIQ (Segall, 2008), AKQ (Kuhn and Carter, 2006), and a measure developed by Ling et al. (2010)).
This review also revealed concerns about the psychometric quality of the measures utilized. An examination of the quality of reported psychometric information demonstrated that only 7% of the studies reviewed met our operational definition for strong psychometric evaluation. This designation required the inclusion of statistical reliability and validity information, which is also listed as another criterion for consideration of a “well-established assessment” (Cohen et al., 2008). Instead, 45% of measures had no reported psychometric evaluation. Interestingly, only one of the measures identified as “well established” based on replication was among those with reported strong psychometric support (the AIQ; Segall, 2008). These findings introduce great concern as the development and adherence to assessment standards ensure that, as a field, we are correctly assessing constructs and have effective tools to examine intervention outcomes. Importantly, they also reveal that the field of ASD knowledge assessment could greatly benefit from increased consistency with regard to measure use across studies.
Of utmost import is the global nature of research examining ASD knowledge. This review identified studies examining this construct in 21 different countries and demonstrates that vast disparities remain with regard to ASD knowledge around the world (Khan et al., 2012). Continued research quantifying ASD knowledge in different countries helps to identify the extent of the need for knowledge dissemination and helps to tailor interventions for specific regions. The lack of consistency in measure use across studies indicates limited collaboration across countries in the identification of an assessment method with cross-cultural utility. While many challenges are associated with the cross-cultural translation and adaptation of measures (Bracken and Barona, 1991), this may be possible with a measure that asks generally about ASD knowledge and minimizes regional specifics or jargon. A more cross-culturally neutral measure would allow for ASD knowledge to be compared across populations and regions so that we might further quantify the amount of disparity experienced in different places around the world. It is possible that steps have been made toward increasing the cross-cultural neutrality of existing measures; however, a lack of reported information regarding cultural adaption processes hinders an understanding of this process.
Interestingly, our analysis revealed similarities in subdomains or subscale themes among measures. Although less than 50% of measures identify specific subscales within the broader construct of ASD knowledge, clear diagnostic, etiological, and treatment subdomains reliably emerge. By identifying areas of knowledge deficits in needs assessments, a useful ASD knowledge measure can help to target areas most in need of intervention. This can also allow for a modular development of interventions to increase knowledge. For example, many of the interventions targeting improvements in MHL often target subdomains of diagnosis or early identification and treatments (for a review, see Jorm, 2012). While much of the broader MHL research does not examine etiology as frequently as treatment or diagnosis, including an etiology subdomain may be important specifically within the field of ASD. This is especially true for ASD given that etiological beliefs impact treatment decisions (Elder, 1994) and that etiological misconceptions have historically resulted in increased stigmas for families (Liu et al., 2010). Additionally, although many of the existing ASD knowledge measures do not explicitly include subscales to assess stigma, an assessment of ASD stigma is often implicitly imbedded in questions, indicating that the constructs of stigma and knowledge seem to be intrinsically linked. For example, if one were to indicate that ASD was caused by a religious curse, this would demonstrate low ASD knowledge, particularly in the domain of etiology, and would also reflect a negative belief or stigma about ASD. Subsequent research assessing ASD knowledge may also benefit from a more thorough evaluation of knowledge-based questions that specifically assess stigma (e.g. autism is preventable; autism is a result of a curse or evil eye inflicted on the family). Thoughtfulness about the different domains of ASD knowledge and attention to subdomain coverage will help to identify the most effective measures to use and may inform the development of stronger measures in future research.
Study target populations varied greatly across the reviewed studies. Target populations included medical professionals (e.g. pediatricians, general practitioners, nurses, pharmacists, and medical students), school professionals (e.g. teachers, speech and language pathologists, school administrators), mental health professionals (e.g. psychologists, psychiatrists), caregivers, siblings, peers, and members of the lay public. This variability lends the question: for whom is it important to have high literacy about ASD symptoms, etiology, and treatments? One could argue that a certain level of ASD awareness is necessary across these groups to ensure that individuals with ASD receive a high standard of care. Parents and primary care physicians must understand the early signs and symptoms of ASD to help trigger early diagnostic evaluations (Janvier et al., 2015). Early childcare providers can also aid in referring children for more timely diagnostic evaluations. Parents, teachers, and special educators must also be able to navigate the buffet of treatment options available to select those with empirical support. Finally, policy makers must understand the etiological underpinnings of ASD and prevalence estimates to make educated decisions about service funding. As such, it is important to be able to effectively assess ASD knowledge among people with a range of educational backgrounds and experience with individuals with ASD. Therefore, an ideal measure of ASD knowledge would have utility across a range of groups.
In sum, although the amount of research examining ASD knowledge has increased in the past 5 years and the global scope of this research is exciting, efforts are needed to synchronize the research within this topic area. Most important, the field needs to come together to identify a measure with cross-cultural utility that can be used to more systematically assess the construct of ASD knowledge and to take the necessary steps to thoroughly evaluate the psychometric properties of this measure. An increased emphasis on replicating and extending existing research using identified steps to cross-culturally adapt assessment measures (Bracken and Barona, 1991) will serve to increase the robustness of this research. While several of the measures with existing psychometric support may be reasonable targets for further examination and more consistent, wide spread use, it is possible that these measures lack the generalizability and cross-cultural utility called for and instead a new measure may be necessary.
Footnotes
Appendix
Top words identified in a text query of all available transcribed measures.
| Word | Count | Category | Word | Count | Category | Word | Count | Category |
|---|---|---|---|---|---|---|---|---|
| Autism | 503 | General | Make | 30 | General | Need | 20 | General |
| Children | 247 | General | Syndrome | 30 | Etiology | Impaired | 20 | Symptom |
| Child | 114 | General | Use | 30 | General | Intervention | 20 | Treatment |
| Behavior | 94 | General | Illnesses | 29 | Etiology | None | 20 | General |
| Autistic | 76 | General | Skills | 29 | General | Activity | 19 | General |
| Diagnosing | 76 | Symptom | Special | 29 | General | Following | 19 | General |
| Disorder | 73 | General | Help | 29 | Treatment | Interests | 19 | Symptom |
| ASD | 62 | General | Effective | 28 | Treatment | Poor | 19 | Symptom |
| Cause | 60 | Etiology | Feel | 28 | General | Receive | 19 | Treatment |
| Asperger | 53 | General | Lack | 28 | Symptom | Exhibit | 18 | Symptom |
| People | 51 | General | Language | 27 | Symptom | Drug | 18 | Treatment |
| Persons | 49 | General | Often | 27 | General | Get | 18 | General |
| Problems | 49 | General | Talking | 26 | Symptom | Interaction | 18 | Symptom |
| Social | 48 | Symptom | Years | 26 | General | Life | 18 | Treatment |
| Community | 45 | General | Contact | 25 | Symptom | Usually | 18 | General |
| Parents | 44 | Etiology | Diagnosis | 25 | Symptom | Developmental | 17 | General |
| Think | 44 | General | Many | 25 | General | Different | 17 | General |
| Number | 43 | General | Schools | 25 | Treatment | Works | 17 | Treatment |
| Treatment | 43 | Treatment | Therapy | 25 | Treatment | Change | 17 | Symptom |
| Schizophrenia | 42 | Symptom | Early | 24 | General | Time | 17 | General |
| Measure | 40 | Symptom | Medications | 24 | Treatment | General | 16 | General |
| One | 40 | General | Knowledge | 23 | General | Opinion | 16 | General |
| Know | 39 | General | Play | 23 | Symptom | Care | 15 | Treatment |
| References | 39 | General | Assessing | 23 | Symptom | Genetic | 15 | Etiology |
| PDD | 38 | General | Live | 23 | General | Understanding | 15 | General |
| Title | 37 | General | Symptoms | 23 | Symptom | Among | 15 | General |
| Educational | 35 | Treatment | Eye | 22 | Symptom | Brain | 15 | Etiology |
| Family | 34 | General | Others | 22 | Symptom | Disease | 15 | Etiology |
| Likely | 33 | General | Speech | 22 | General | Member | 15 | General |
| Mental | 32 | Symptom | Common | 21 | General | Must | 15 | General |
| Ages | 31 | General | Affects | 21 | Symptom | Repetitive | 15 | Symptom |
| Individuals | 31 | General | Adults | 20 | Treatment | Routines | 15 | Symptom |
| Development | 31 | General | Childhood | 20 | General | Show | 15 | General |
ASD: autism spectrum disorder; PDD: pervasive developmental disorder.
Acknowledgements
The authors would like to thank members of the UGA CAARE Lab, Madison Paff, Ashley Dubin, Brianna Cochran, Sidra Shakil, and Margaret Naughton for their help preparing this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.