
Abstract
The external validity of behavioral treatments for elopement (i.e. leaving supervision without permission) remains unclear because studies to date include only small samples (n = 1–3). This study quantified the overall effectiveness of behavioral treatments for elopement by retrospectively examining treatment data from all patients seen for the treatment of elopement at an intensive day treatment clinic (n = 11), irrespective of treatment success. Reductions in elopement from baseline to the final treatment for each participant demonstrate that behavioral intervention is a highly effective treatment for elopement, as determined by the large effect size (Cohen’s d = 1.18).
A recent study by Anderson et al. (2012) found that an alarming 49% of children with autism spectrum disorder (ASD) had attempted to leave a caregiver or designated area without permission, a behavior also known as elopement (Bodfish, 1992). The effects of elopement are potentially lethal, such as drowning or being struck by an automobile, contributing to the fact that accidents are one of the leading causes of premature death for this population (Shavelle et al., 2001).
Yet despite the potential for significant negative consequences due to elopement, the research on treatments remains limited. To date, only eight published studies adhere to best practice recommendations from Lang et al. (2009) by including individualized treatments for elopement based upon the results of a functional analysis (Call et al., 2011; Davis et al., 2013; Falcomata et al., 2010; Kodak et al., 2004; Lang et al., 2010; Perrin et al., 2008; Piazza et al., 1997; Tarbox et al., 2003). Using single-subject methods, each of these studies demonstrated the effectiveness of one or more behavioral treatments to decrease elopement in a manner that maximized internal validity. However, their external validity remains unknown, in part because of a potential for publication bias. That is, because publication practices can favor data demonstrating effective treatments, examples of these same treatments being ineffective may exist but are unlikely to have been reported in the literature (Sham and Smith, 2014). Moreover, the current literature reflects the treatment outcomes from only very small sample sizes (i.e. n = 1–3 participants).
Ideally, randomized clinical trials of treatments for elopement would address questions regarding external validity. Unfortunately, clinical trials are resource-intensive and generally require preliminary evidence as justification, something that is currently lacking given the small number of heterogeneous small-n studies to date. However, an outcome study reporting the effectiveness of treatments for elopement across multiple participants, multiple functions, and multiple treatment packages could serve as an important step that bridges the gap between the existing literature and larger clinical trials (Call et al., 2015). Moreover, an outcome study that presents all cases treated within a clinical sample, regardless of treatment effectiveness, will help to ascertain the likelihood of such treatments producing positive results and the magnitude of reductions produced by behavioral treatments for elopement. The purpose of this study was to perform this type of analysis by conducting a retrospective chart review of all cases of elopement treated within a clinical setting that specializes in the development of function-based treatments for individuals with ASD and other developmental disabilities.
Method
Participants
A comprehensive review of medical records was conducted to identify archival data from the patient record database of an intensive day treatment clinic that specializes in the treatment of severe problem behavior, including elopement. All patient records between October 2003 and August 2013 that included the search term elopement were analyzed for potential inclusion. From this pool of potential participants, selection criteria for inclusion in the analysis were as follows: (a) elopement was the primary dependent variable, (b) treatment was based upon the results of a prior functional analysis that operationally defined elopement as leaving a caregiver or therapists’ supervision, and (c) data sets were complete.
Clinical procedures
For all participants, the clinical team consulted with caregivers throughout their admission to identify treatment goals and evaluate the acceptability and feasibility of the treatment. Whenever possible, an observation was also conducted in the natural environment(s) in which elopement occurred (e.g. home, school, and community outings) to aid clinicians in designing functional analyses and treatments that were socially and ecologically valid.
Bachelors- and masters-level therapists with a background in applied behavior analysis and specific training on all clinical procedures conducted all assessment and treatment sessions and collected data on elopement. Interobserver agreement data were collected by a second data collector who simultaneously, but independently, recorded occurrences of elopement during no fewer than 20% of sessions for each participant. Interobserver agreement exceeded 80% agreement for elopement for all participants.
Functional analysis
All functional analysis sessions were conducted in a manner similar to those described by Piazza et al. (1997): during test conditions, participants always had the opportunity to elope from a session room that established a potential source of reinforcement (e.g. a therapist presented demands, restricted attention, or a preferred item) to another room that included the associated potential reinforcer (e.g. a break from demands, attention, or a preferred item). One such potential reinforcer was evaluated in each test condition. The rate of elopement in each test condition was then compared to elopement observed in a control condition that did not systematically manipulate any such sources of reinforcement (e.g. free access to attention and preferred items and no demands). Sessions were typically 10 min in duration.
Treatment evaluation
PhD-level clinicians selected individual treatment components based upon the results of the functional analysis and recommendations from the research literature, with consideration given to client variables and caregiver preference. The clinical team used a reversal design to evaluate treatment data by systematically introducing and withdrawing treatment components to demonstrate treatment effects.
Caregiver training and generalization
Caregivers were involved in the identification of treatment goals, including identifying settings in which elopement was most problematic (e.g. at home or some specific location in the community) and treatment development was informed through caregiver consultation, consideration of long-term treatment goals, and feasibility of the treatment in the natural environment. Once an acceptable treatment effect was observed within the session room, the clinical staff evaluated the same treatment in more naturalistic settings around the clinical facility (e.g. classroom, playroom, hallways, and outdoor playground). In addition, caregivers for all participants were trained to implement treatment using didactic instruction and role plays with staff before being systematically and gradually introduced into in vivo treatment sessions. Caregivers conducted treatment sessions until they achieved ⩾90% procedural fidelity conducting all treatment components, requiring 37 sessions on average. Lastly, treatment was generalized outside of the clinical facility to the participant’s home, school, and/or the community. During these generalization sessions (and thereafter), caregivers implemented all components of the final treatment while the clinical staff collected data and provided the caregivers with feedback on their treatment fidelity.
Analysis of outcome data
We computed an effect size for the treatment of elopement using the standardized mean difference in the rate of elopement observed in the first baseline phase and final treatment phase (Shadish et al., 2014). Percent reduction in elopement was also calculated for each participant and converted to an overall mean percentage reduction across participants. To calculate percent reduction, the mean rate of elopement in the final treatment was subtracted from the mean during baseline, then divided by the baseline mean and multiplied by 100. For participants with multiple treatments (to address elopement that served multiple functions), we calculated an average percent reduction. All analyses were performed on the original raw clinical data.
Results
The record review identified 1458 participants who received services in the day treatment clinic between October 2003 and August 2013. Of those participants, 1405 were excluded because they did not engage in elopement. Another 18 participants were eliminated because elopement was not the primary problem behavior targeted during their admission. Of the remaining 35 participants, 22 were excluded because their elopement was not operationally defined as leaving the presence of a therapist or caregiver. Examples of elopement for participants who were excluded for this reason included pulling on the handle of the session room door or leaving their seat during an academic task. Lastly, two participants were excluded due to incomplete data sets. In all, 11 participants remained after applying all the inclusion criteria (Table 1).
Participant characteristics.

ASD: autism spectrum disorder; ID: intellectual disability; ADHD: attention-deficit/hyperactivity disorder.
Overall, the total number of sessions conducted across participants ranged from 71 to 389 (M = 171.90). Results of the functional analyses found that elopement was maintained by access to preferred tangible items for two participants, access to attention for two participants, automatic reinforcement for two participants, escape from demands for one participant, and multiple functions for four participants.
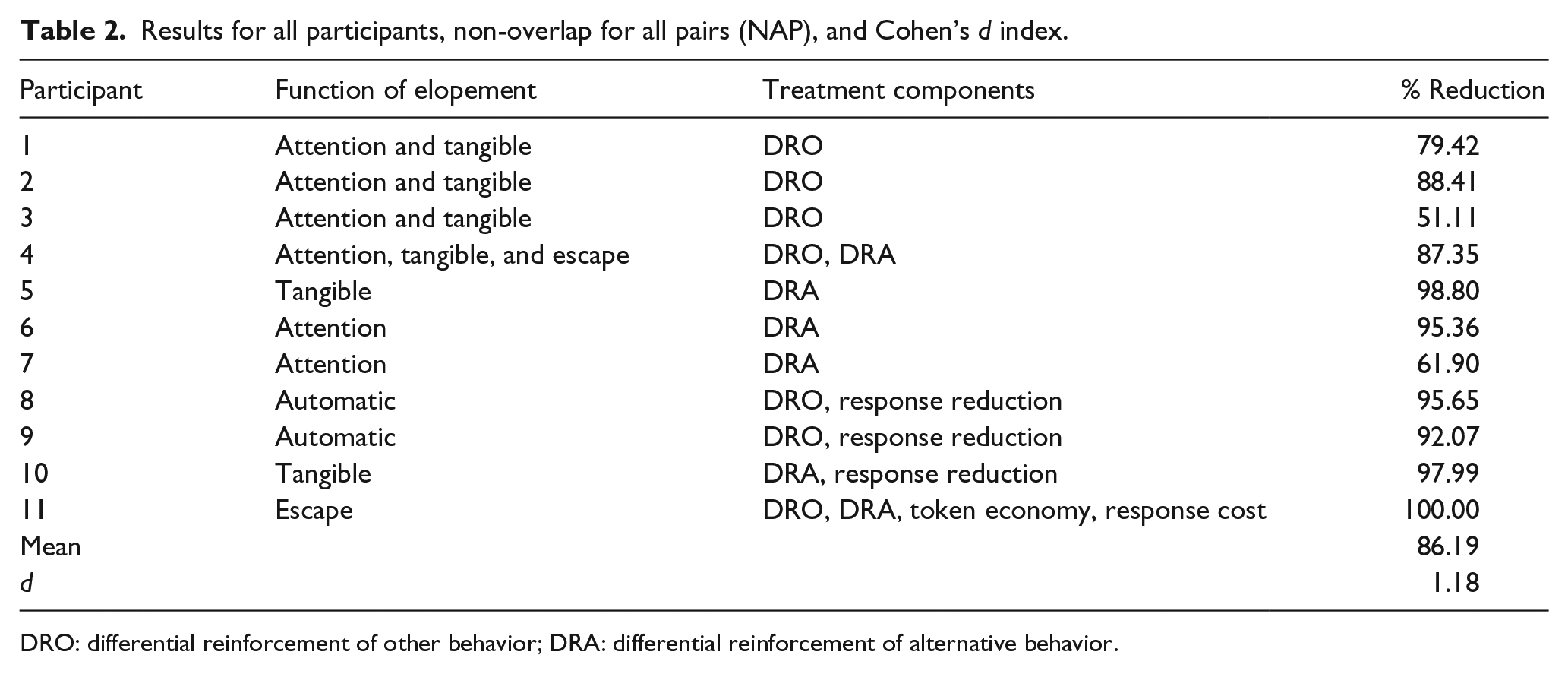
For most participants, several combinations of treatment components were evaluated before a treatment was finalized. The final treatment consisted of one treatment component for six participants, two components for four participants, and four components for one participant. Differential reinforcement of other behavior (DRO) was the most common treatment component, implemented with seven participants. Other treatment components implemented with several participants included differential reinforcement of alternative behavior (DRA) and reductive procedures, such as time-out. All treatments included extinction, defined as no longer delivering, or preventing access to, the reinforcer that was determined to maintain the participant’s elopement via the functional analysis. To improve the social validity of the treatment, reinforcement-based strategies for most participants included schedule thinning (i.e. gradually increasing the amount of time participants had to wait, or the amount of work required, prior to reinforcement). Another common approach to increasing the social validity of treatment was to implement a multiple schedule of reinforcement (Hanley et al., 2001). This strategy was often used as a follow-up to DRA and involved teaching a discrimination between periods during which reinforcement was available versus unavailable (Table 2).
Results for all participants, non-overlap for all pairs (NAP), and Cohen’s d index.
DRO: differential reinforcement of other behavior; DRA: differential reinforcement of alternative behavior.
The resulting treatment outcome across participants was an overall mean reduction in elopement of 86.19%. The final treatment packages yielded a 90% or greater reduction for 6 of 11 participants (54.55%), a 95% or greater reduction for 4 participants (36.36%), and a 100% reduction for 1 participant (9.10%). Of note, a 100% reduction required no occurrences of elopement during the entirety of the final treatment phase. However, for three participants, the trend in the rate of elopement during the last treatment phase suggested that elimination of elopement may have been achieved eventually. The d score (effect size) across all cases was 1.18.
Discussion
Behavioral interventions effectively reduced dangerous levels of elopement for all of the participants in this clinical sample, with an overall effect size of d = 1.18. This magnitude of treatment effect exceeds the standard for a large effect that has been established in the literature (Cohen, 1988). This result confirms the results of previous single-subject research on the treatment of elopement showing the effectiveness of behavioral interventions, but expands on that prior literature in two important ways. First, previous studies all had very small samples of three or fewer participants. Second, this study included all potential data sets from a clinical sample regardless of treatment success. Thus, these results are not subject to the potential for bias against negative results that have been noted in the treatment literature (Sham and Smith, 2014).
Although this study expanded the current literature on the treatment of elopement, it is not without some limitations. First, the degree to which these findings are representative of the reductions in elopement produced by behavioral interventions for other individuals depends upon the extent to which those interventions and individuals are similar to this clinical sample and setting. For example, participants in this study received intensive treatment in a day treatment setting. It is unclear whether treatments implemented in a less intensive setting or manner would produce such large treatment effects. Similarly, all participants in this study received a functional analysis prior to the implementation of treatment. Although the inclusion of a functional analysis has been described as best practice in the treatment of elopement (e.g. Lang et al., 2010), the results of this study cannot be generalized to individuals who have not experienced this type of assessment.
Despite these limitations, this study represents an incremental but important step toward necessary future research on the treatment of elopement in this population by demonstrating that behavioral interventions for elopement are able to have very large treatment effects and that such large effect sizes may be typical. Given the potential life-threatening consequences of elopement for a child and the tremendous impact of elopement on family functioning, these outcomes provide compelling evidence for an effective means of treatment. Demonstrations of efficacy such as this may serve as a framework for future studies evaluating the probability of such large treatment effect sizes, the maintenance of treatment gains over time, and the cost–benefit of these outcomes.
Footnotes
Compliance with ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.