
Abstract
Autism is a global phenomenon. Yet, there is a dearth of knowledge of how it is understood and its impact in low-income countries. We examined parents’ and professionals’ understanding of autism in one low-income country, Nepal. We conducted focus groups and semi-structured interviews with parents of autistic and non-autistic children and education and health professionals from urban and rural settings (n = 106), asking questions about typical and atypical development and presenting vignettes of children to prompt discussion. Overall, parents of typically developing children and professionals had little explicit awareness of autism. They did, however, use some distinctive terms to describe children with autism from children with other developmental conditions. Furthermore, most participants felt that environmental factors, including in-utero stressors and birth complications, parenting style and home or school environment were key causes of atypical child development and further called for greater efforts to raise awareness and build community capacity to address autism. This is the first study to show the striking lack of awareness of autism by parents and professionals alike. These results have important implications for future work in Nepal aiming both to estimate the prevalence of autism and to enhance support available for autistic children and their families.
There have been significant and sustained reductions in global mortality rates in the under-fives over the last decade (Wang et al., 2014). Such achievements mean that greater numbers of children are surviving. Consequently, for children and adults, the global focus is shifting from communicable to non-communicable diseases and from premature death to life lived with/without a disability (Murray et al., 2012). The latest global estimate for disability across the age span is 15% (World Health Organization (WHO), 2013), although this varies with context and definition. Mental and behavioural health conditions, which include atypical child development and cognitive, social and behavioural impairments, therefore contribute a rising and significant concern globally – an estimated 10% of all disability-adjusted life years (DALYs) in 2010 (Murray et al., 2012). Indeed, the number of children under the age of 14 years with moderate-to-severe disabilities is estimated at around 93 million worldwide (UNICEF, 2013). The majority of those who might attract a diagnosis of autism will not be recognised as such, but some will have significant functional difficulties and will be of concern to their parents and communities.
These issues are particularly pertinent in Nepal where child mortality rates have fallen and concern over identification and management of children with atypical child development is rising. Nepal is one of just four low-income countries (LICs) outside of Sub-Saharan Africa and has one of the lowest under-fives mortality rates of all LICs (UNICEF, 2015). As a LIC, Nepal has a gross national income (GNI) per capita of USD1147 (the average GNI per capita of South Asian nations is USD3343). Despite substantial reductions in mortality rates, with under-fives mortality rates falling from 87 to 40 per 1000 births over the last 20 years (Ministry of Health and Population, 2012; UNICEF, 2015), relatively few services exist to identify and support children and their families with atypical child development and behavioural disabilities, and those that do exist are largely limited to urban areas (Kathmandu Valley). Furthermore – and most relevant to this study – remarkably little is known about Nepali community members’ perceptions of atypical child development, especially perceptions of autism. As such, Nepal presents an ideal and understudied setting in which to examine understanding of atypical child development and of autism in particular.
According to a recent systematic review, autism is the leading cause of disability among all mental health disorders in the under-fives, where the term ‘mental health disorders’ encompassed attention-deficit/hyperactivity disorder (ADHD), conduct disorder and autism but no other forms of atypical child development (Baxter et al., 2015). Epidemiological studies estimate that 1%–2% of children worldwide lie on the autism spectrum (Elsabbagh et al., 2012). Such estimates vary considerably from country to country, with the variation attributed to disparities in understanding of the term, and in diverse identification and intervention practices across settings rather than to systematic geographic, ethnic, cultural or socioeconomic differences (Elsabbagh et al., 2012).
Although most research on autism occurs in high-income countries (WHO, 2013), there is growing interest in the ways in which autism is manifested and understood in developing and underserved populations, such as Nepal (Bernier et al., 2010; Grinker et al., 2012). Such knowledge is key to raising awareness and building capacity to support autistic 1 people and their families in LICs (Hahler and Elsabbagh, 2015) Furthermore, narrating and understanding the experience of families of autistic children and those who support them are essential to the development of appropriate and acceptable interventions with which to address inadequacies in health, education and social systems for children with atypical child development in LICs (Yousafzai et al., 2014).
Some studies have examined the perceptions and experiences of parents of children with autism from India (Brezis et al., 2015; Desai et al., 2012; Divan et al., 2012; Sarrett, 2015), but research investigating public awareness and perceptions of autism in Nepal or other LICs is scant (Shrestha and Santangelo, 2014). While there is a limited number of studies describing health professionals’ understanding of atypical development, specifically autism, in low-to-middle income countries such as Pakistan (Imran et al., 2011; Rahbar et al., 2011) and Nigeria (Bakare et al., 2009a, 2009b; Eseigbe et al., 2015; Igwe et al., 2010, 2011), only one study has examined professionals’ understanding of autism in Nepal (Khatri et al., 2010). This study surveyed 54 paediatricians in Kathmandu Valley and found that their knowledge of autism was poor, similar to professionals in other LICs, including Pakistan and Nigeria (Elsabbagh et al., 2012): 85% of respondents reporting having received no training on autism.
To our knowledge, no published studies have investigated Nepali parents’ understanding of autism or indeed any other form of atypical child development. Here, we sought to investigate the extent and nature of understanding of autism, within the context of typical and atypical development, in parents of autistic and non-autistic children and among health and education professionals in Nepal. Specifically, we used qualitative methods to elucidate participants’ awareness of autism as a distinct entity and their views and perspectives of how best to support children with the condition – the first step towards identifying the nature of the challenges facing those with autism and those affected by autism in Nepal and the possible ways to respond to their needs.
Method
Participants
A total of 106 people took part in this study via 12 focus groups and nine semi-structured interviews. Participant characteristics are shown in Table 1. Participants were purposively recruited through community partners, Autism Care Nepal Society (ACNS) and Mother and Infant Research Activities (MIRA), Nepal, from areas within urban (Kathmandu Valley) and rural (Makwanpur District), Nepal. Makwanpur District is a rural hill area in the central region of Nepal in which most households are dependent on subsistence agriculture (population >500,000). We either recruited parents with children aged 16 years and under with a recent (within the last 6 months) diagnosis of autism or recruited parents with children of any age without a known diagnosis of autism. Significant efforts were made to ensure representation from both urban and rural parents and professionals and a range of ethnicities (see Table 1). Focus groups were conducted with parents of children with no known diagnosis of autism (total n = 47), parents of children diagnosed with autism (n = 21), community health workers (n = 8), paediatricians (n = 15, including eight senior and seven junior paediatricians) and primary school teachers (n = 6). Due to logistical constraints of gathering together some professional groups, we also conducted individual semistructured interviews with four Early Childhood Development (ECD) teachers, two traditional healers, one paediatrician (senior and rural based, the only paediatrician in Makwanpur district) and two disability sector workers.
Participant characteristics.

FGD: focus group discussions; SSI: semi-structured interviews; ECD: Early Childhood Development; NR: not recorded.
Ethnicity: 1 = Brahman, 2 = Chhetri, 3 = Newar, 4 = Gurung, 5 = Magar, 6 = Kami, 7 = Damai, 8 = Tamang, 9 = other – 1 and 2 are high-caste people and are highly privileged; 3 are not high caste but economically privileged people; 4, 5 and 8 are hill ethnic people and do not belong to the caste system; 6 and 7 are low caste people, so-called ‘untouchables’ and economically poor.
Part of pilot groups.
Participants’ age and gender, and ages of participants’ children missing from two participants.
Materials
Topic guides were developed in collaboration with community partners and translated (English to Nepali), back translated (Nepali to English) and adapted to ensure consistency, preservation of meaning and cultural appropriateness. The same topic guides were used across all participants, although discussions with professionals included more specific questions around capacity building for children with atypical development.
The interviews and focus groups were implemented by two Nepali facilitators trained in qualitative methods. Upon joining the research team, the facilitators underwent training in autism and (a)typical child development, including a 2-day placement at ACNS and attendance at a series of paediatric clinics hosted by MIRA and ACNS paediatricians and clinical psychologists. Following this training, the topic guide was piloted with three focus groups of parents (one group of parents with a child with autism living in Kathmandu Valley and two groups of parents with a child without a known diagnosis of autism living in Makwanpur District). These pilot focus groups were run by both the MIRA team and the two Nepali facilitators under the supervision of a senior English- and Nepali-speaking clinical psychologist and qualitative researcher. Minor edits were made to the topic guides following feedback from the pilot groups and review of the translated transcripts. Questions were added to the topic guides for health and education professionals asking specifically about their experience and training in managing children with atypical child development and behavioural problems, how the current educational and health systems support such children and their families and how these systems could be changed. As changes to the topic guide were only minor, the pilot data were included for analysis in the final study.
Procedure
The focus-group discussions and semi-structured interviews were carried out face-to-face either in Nepali (for most participants) or in Newari (a language of the Newar people of Nepal, most commonly from the Kathmandu Valley). The discussions initially focused on typical development, followed by atypical development. Specifically, participants were asked their thoughts on how children develop, which behaviours might be signs for concern and at what age, the potential impact of having a child with developmental difficulties and what support should be given to these children and their families.
The topic guides for the focus groups and the semistructured interviews followed the same structure. First, there was a discussion around typical and atypical child development stimulated by six potential prompt questions (e.g. as, ‘How do children typically develop?’ and ‘If a child didn’t have the particular skills and behaviours you expect, what could be the reasons for this?’).
Second, given the limited awareness of autism in Nepal, at least anecdotally (Shrestha and Santangelo, 2014), participants were asked to think about children who develop or behave in noticeable or unusual ways within the context of seven vignettes describing typically developing children and children with various developmental features that might attract a diagnosis, including autism, ADHD and developmental delay. The vignettes were accompanied by illustrations by a local artist to aid understanding of the verbal descriptions. The presentation of each vignette was followed by the same set of questions, including ‘is this like other children of the same age?’, ‘what do community people say about children who show these types of behaviour?’, ‘what might cause this?’ and ‘are there any traditional reasons?’
Importantly, participants were never explicitly told that the behaviours described were necessarily a difficulty for the children. The vignettes were developed through an iterative process in discussion with UK- and Nepali-based paediatricians, clinical psychologists, ACNS and the MIRA research team. The vignettes, always presented in the same order, included descriptions of a typically developing child (vignette 1), three boys with possible autism (vignettes 2, 3 and 6), a boy with more global developmental delay (vignette 4), a boy with possible ADHD (vignette 5) and a girl with possible autism (vignette 7) (see Figure 1; e.g. vignettes).

Examples of vignettes with corresponding illustrations, used in focus group discussions and semistructured interviews.
In the final part, participants were asked to consider all children presented in the vignettes, including what problems they and their families might face and what things could or should be done to support them. Specific prompts were given if necessary to ensure participants discussed social, health and educational issues.
The focus groups/interviews were facilitated by experienced Nepali moderators who asked a predetermined set of questions in a semistructured manner, so that discussion was free-flowing. The moderator ensured that all participants were involved in the discussion, all questions were included in the allocated time and only relevant topics were discussed. Focus groups and interviews ranged between 50 and 110 min (M = 83 min). The sessions were recorded for later transcription and translation. A co-facilitator, who was also Nepali, took notes during the group, which were later added to the transcription as necessary.
Ethical approval for the study was obtained both from Nepal Health Research Council and the University Research Ethics Committee. Informed verbal consent was granted by all participants prior to participation, which is more culturally appropriate in this setting than written consent.
Analysis
The resulting data were analysed using thematic analysis through the process outlined by Braun and Clarke (2006) including familiarisation with data, generation of initial codes, searching for themes among codes, review of themes, defining and naming of themes and production of the final report. Analysis was carried out manually as well as using NVivo10 (QSR International Pty Ltd, 2012). An inductive approach was used to identify themes within the data. Three authors (M.H., A.A. and E.P.) independently familiarised themselves with the data and met regularly to discuss preliminary themes and codes, resolve discrepancies and decide on the final themes and subthemes. Translation and interpretation of the descriptive terms was confirmed by English/Nepali- and Nepali/English-speaking authors (K.T.) and clinical psychologist (E.M.).
Results
When asked about typical development, most participants could identify major developmental milestones, in the domains of motor development (e.g. walking), language development (e.g. first words) and social development (e.g. ‘when a child is 2, 3 months they start to smile’, junior paediatrician). Many participants described how children learn, highlighting especially how they imitate others (e.g. ‘seeing others doing things and doing by themselves’, community health worker). Many parents also commented that if their children ‘did not develop like other children, parents become worried’ (parent of non-autistic child).
We identified four overarching themes related to atypical development and autism from the discussions including (1) perceptions of atypical development, (2) causal attributions of atypical development, (3) social consequences of having a child with autism and (4) community capacity building.
Theme 1: perceptions of atypical development
When prompted to think about atypical development, all participants perceived the behaviours described in many of the vignettes to be ‘only found in abnormal children’ (parent of non-autistic child). Nevertheless, very few participants could attribute specific terms or labels to these behaviours. Of the four vignettes describing behaviours of children with possible autistic features, only parents of autistic children, paediatricians and the disability sector worker identified them clearly as ‘autistic’ (Nepali: punaraabrittiya byabahaar), either using that word itself or clearly associated other terms. Parents with higher education and knowledge of autism also tended to use scientific descriptors such as ‘echolalia’ in English within their Nepali sentences when explaining the difficulties of these children. Instead, participants commonly used terms that were related to developmental disabilities more broadly, including ‘special child [bisesh prakaar ko bachcha]’ (primary school teacher) or ‘mentally retarded [susthamanasthiti]’ (ECD teachers/community health workers/parents of non-autistic child). Parents, community health workers, ECD and primary school teachers and disability sector workers all most commonly described the autistic children in the vignettes as ‘stubborn [jiddi or ziddi]’ (see Figure 2(a)). This term was rarely used to describe the children with possible ADHD or developmental delay (Figure 2(b) and (c), respectively). The child with developmental delay was often described as ‘slow-minded [susthadimaag]’ or ‘dumb [laato/gungo]’. These terms were also frequently used to describe the children with possible autism, suggesting either that participants were not aware of the differences between these two conditions or that they were implicitly aware of the substantial overlap between more global intellectual disabilities and other communication impairments. Participants, however, clearly distinguished the child with possible ADHD from all other vignettes, using descriptors such as ‘naughty and pampered [chakchake/updryaha/ladiyako]’ (community health worker) or ‘he has an insisting manner [dhipi garera aagraha garne byabahaar]’ (parent of non-autistic child), suggesting some awareness of the differences between the manifestations of ADHD (see Figure 2(b)) and the other developmental conditions. Figure 2(d) shows the terms used to describe the vignette of the girl with possible autism. With the exception of one participant (a parent of a child with autism), none could identify possible autistic features from the description – including those with prior knowledge of autism (parents of autistic boys and paediatricians).
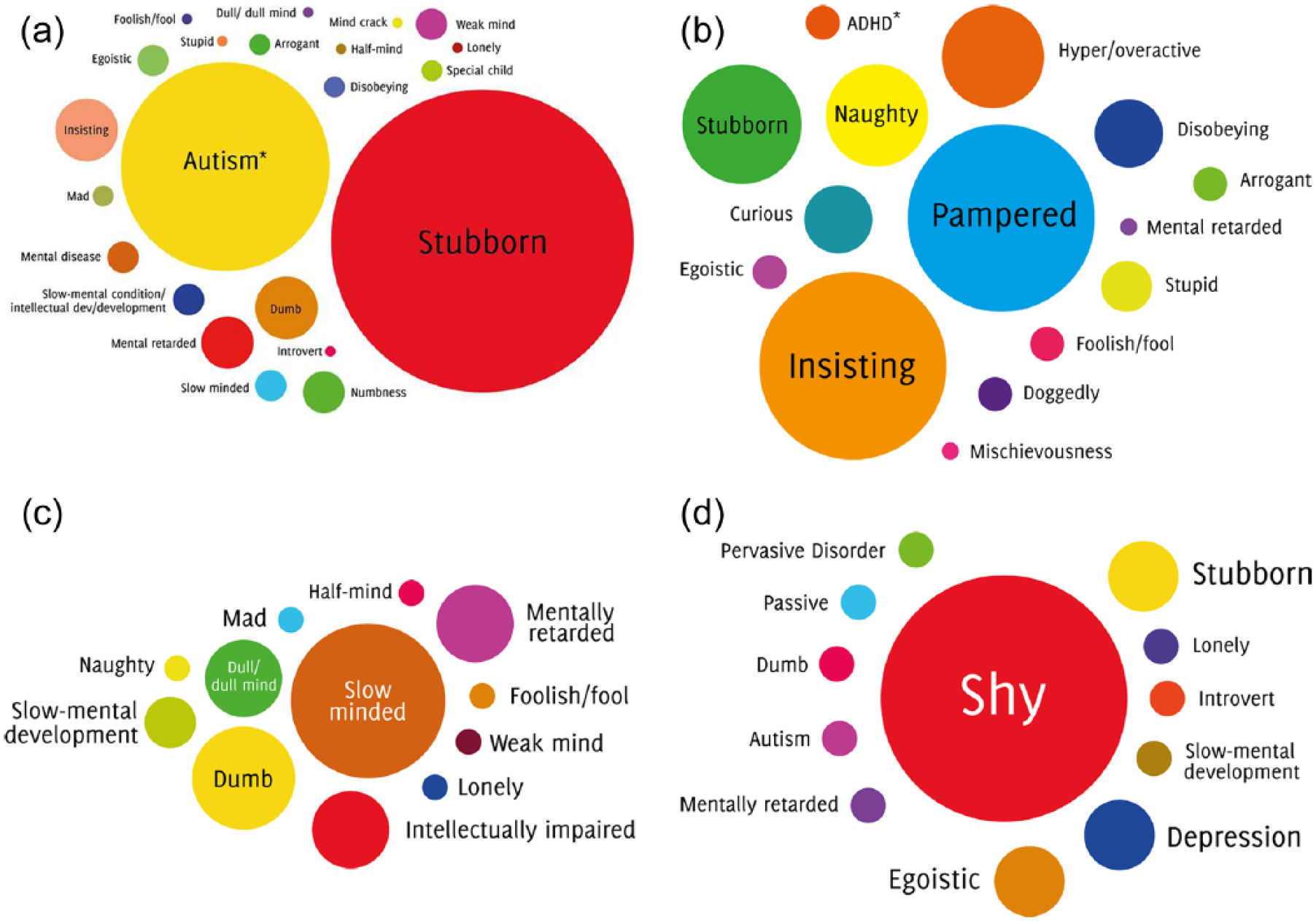
The word diagrams show the range of terms used by participants during discussions of the vignettes describing (a) the boys with possible autism, (b) the boy with possible ADHD, (c) the child with global developmental delay and (d) the girl with possible autism. Larger circles reflect greater usage of these terms by participants. Note that the terms ‘autism’ and ‘ADHD’ in (a) and (b), respectively, are asterisked to indicate that they were used only by those with experience of these conditions (e.g. parents of children with an autism diagnosis and paediatricians) and in English within the Nepali sentence.
Theme 2: causal attributions of atypical development
When asked about the underlying cause of atypical behaviours, participants were divided as to whether they felt these causes either lay within or beyond a person’s control. Relatively few participants believed that a child’s atypicalities were beyond a person’s control; of those some felt that children’s atypical behaviours were controlled either by environmental factors that they could not influence or by chance or fate. Some participants identified genetics as a primary cause of atypical development: ‘family heredity can also be one of the causes’ (parent of non-autistic child). Some parents, community health workers and paediatricians further suggested that the causes of impairments resided in birth complications, including ‘difficulties in delivery’ (parent of autistic child) and ‘premature birth’ (senior paediatrican, rural). Other participants, especially faith healers, emphasised that ‘the child comes born with their fate already written’, which cannot be changed. Some parents, however, questioned this view, suggesting that only villagers or ‘old people say that it is written in your fate that you gave birth to this child’ (parent of autistic child). Of the few participants with some awareness of autism, some were aware that ‘even scientists don’t understand the causes of autism’ (parent of autistic child).
Most participants perceived children’s atypical behaviours to be driven by factors within a person’s – predominantly the parent’s – control. Poor parenting was the most common cause for childhood disability identified by participants across all groups, with the exception of paediatricians. One community health worker expressed how ‘it is the parents’ role to make their children normal’. In response to the descriptions given in the vignettes, especially of the boy with possible ADHD, participants described how ‘children appear insisting in nature because their parents over-pamper them’ (ECD teacher) or ‘there is probably no one in the family to teach him proper behaviour’ (ECD teacher). Participants broadly agreed that it is the parents’ responsibility to teach their own children, so that they can become fully functioning members of society: the ‘first school for children is home’ (parent of non-autistic child).
Participants also identified maternal behaviours during pregnancy, especially ‘the lack of balanced diet and nourishment during pregnancy’ (ECD teacher), as another source of children’s atypical behaviours, particularly when discussing the vignettes of children with possible autism. Some parents also mentioned how the ‘careless use of medication during pregnancy’ (parent of autistic child) could cause atypical development, while some suggested that failed abortions were the primary cause: ‘a women of our village tried to abort child by eating medicines but [with] no success and gave birth to a dumb child’ (parent of non-autistic child).
The mother’s behaviour was also perceived as crucial during their child’s early development. The child’s diet and nutrition was frequently mentioned as an underlying cause for atypical development: ‘mothers should feed [the child] nutritious food’ (parent of non-autistic child). One teacher described how ‘if children didn’t get enough nutritious food from a young age, this can affect their mental development’ (ECD teacher). Participants also described how the broader social environment can affect a child’s development, whether this is the family home, school or wider society. One parent of a child without autism said, ‘we parents should create a proper environment and teach them morals’, while one ECD teacher described how children ‘are mentally affected by their family environment’.
Finally, some participants also discussed spiritual or religious explanations for children’s atypical development, which they often appeared to believe to be within a person’s control. Some participants spoke about how ‘the curse of God or spiritual power affected them because [parents] haven’t fulfilled what they promised with God’ (community health worker), causing them ‘to give birth to a disabled child’ (parent of non-autistic child). There were also many examples of superstitions around rituals or social situations that should be avoided during pregnancy. For example, ‘mothers should not see hitting [of others] or shootings [of birds] during her pregnancy’ (parent of autistic child) or ‘if there is a pregnant woman in the village they shouldn’t allow her to see autistic children because if she saw those children she will also give birth to an autistic child’ (parent of autistic child).
Theme 3: social consequences of having a child with autism
Parents of autistic children talked at length about the largely negative impact of having a child with autism. They described how ‘it brings so many disturbances in life’ to the extent that ‘we are not able to do what we want to do’, affecting families ‘socially, mentally and economically’. Parents explained that these impacts arise because ‘community people don’t understand exactly about autism … they don’t know about it, so they think negatively about autistic children, saying our child is crazy’ [pagaal/baula/sanki] (parent of autistic child). These negative attitudes towards children who are atypical can lead to financial insecurity as they ‘are not able to work, we must resign from our job’ (parent of autistic child). The stigma experienced by these families was attributed to the stigma attached to disability, especially mental disability, in Nepal more broadly.
Theme 4: building capacity to address atypical child development
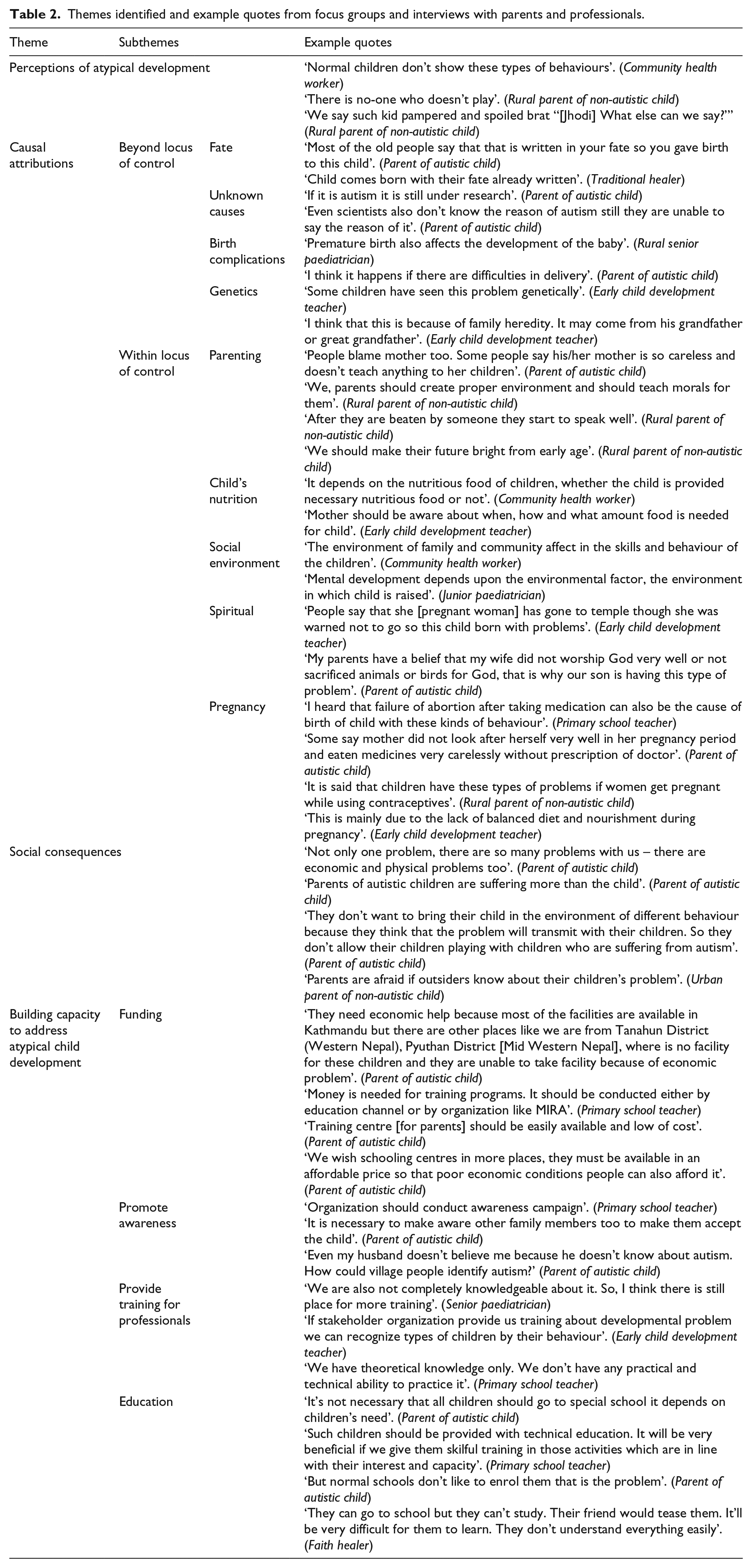
The final theme identified ways to build capacity in order to meet the needs of children with atypical child development, including autistic children and their families, in Nepal. These were through (1) increased funding, (2) awareness raising, (3) training for professionals and (4) education (see Table 2).
Themes identified and example quotes from focus groups and interviews with parents and professionals.
Parents of children with autism, in particular, appealed for increased funding to provide health, education and training facilities outside of Kathmandu, ‘where is no facility for these children and they are unable to take [to a] facility [in Kathmandu] because of economic problem’ (parent of autistic child). The suggested training facilities were needed for parents and professionals alike. The desire for increased funding for educational facilities was echoed by primary school teachers.
Participants called for greater efforts to promote awareness about autism. Parents described how their children with autism could ‘easily live in society if there is awareness about it and if the support system is good for them’ because ‘the main thing is knowledge’ (community health worker). Any awareness about existing advocacy and support organisations such as ACNS and MIRA was limited to paediatricians, parents of autistic children and those who worked in the disability sector. Furthermore, many participants emphasized the need to promote awareness of autism in rural areas and villages because ‘people [who] live in the city know about it, but it must be promoted in villages too’ (parent of autistic child). Both training for educational and health professionals and special schools were thought to be needed in rural areas, in particular, as some participants described how they needed to move to Kathmandu for such facilities, ‘we came here only for training, my home is in Damauli [town in Tanahun District, Western Nepal]’ (parent of autistic child), although some did not have sufficient funds to do so. Primary school teachers suggested that ‘there should be school in every Village Development Committee [term given to the lower administrative areas within a district] to teach such children’ and ‘the monthly fee should be reasonable’ (parent of autistic child) because currently they are ‘out of reach of poor people’ (parent of non-autistic child).
Moreover, professionals, such as paediatricians, teachers and community health workers, expressed the need for more training because ‘we have theoretical knowledge only, we don’t have the opportunity to practice it’ (primary school teacher). All professionals admitted that they did not have sufficient knowledge or training about how to manage atypical behaviours and/or help support children with developmental conditions. Health workers and teachers described how typical development is clearly ‘detailed in [their] psychology Masters degree’ but they ‘haven’t received any training during our jobs’ (community health worker) about how to detect and deliver services for those children who do not follow typical trajectories. Junior paediatricians also called for more training because they need to know ‘how to handle and where to refer [these children]’.
Many participants further suggested that improvements must be made to children’s education. All participants emphasised that children with autism and other atypical child developmental disorders could and should be educated in some way. The exception to this was parents of non-autistic children, some of whom suggested that autistic children and children with atypical child development ‘can’t learn what teachers teach, [or] can’t grasp the knowledge’ and therefore should not go to school. Parents of autistic children highlighted the fact that many mainstream schools often do not enroll children with disabilities because ‘they think that this child also disturbs the learning of other children so they don’t want to admit this type of child’. This was perceived to be a particular problem for parents who live in rural areas: ‘what can they do? There is only one school in the village’ (ECD teacher).
Participants were divided, however, about whether autistic children and other children with atypical child development should attend ‘regular’ or special schools. On one hand, many participants including parents of autistic children, ECD teachers and those working in the disability sector stressed that children with atypicalities would learn more effectively in a regular school environment ‘because while associating with normal behaviour, unusual behaviour can also improve a little bit’ (community health worker). On the other hand, other participants felt that ‘there must be special schools for them’ (parent of autistic child). One ECD teacher said that ‘learning [in regular schools] doesn’t go smoothly because children with problems can’t understand matters that are explained just once or twice, their learning follows a much slower pace’. One paediatrician said that if ‘they go to a regular school then they’ll find it difficult to cope and mix with other normal children’ and potentially disrupt the learning of others. Furthermore, primary teachers said that they should attend a special school with a different, more appropriate curriculum because ‘normal and abnormal children can’t learn from the same teaching method’. Some participants emphasised that this alternative curriculum should include ‘skill oriented training so they are able to get work’ (primary school teacher) and ‘become independent’ (parent of autistic child). One primary teacher emphasised the need for vocational training: ‘if we give them technical training, then their life will move along the right track’.
Discussion
We examined for the first time parents’ and professionals’ understanding of autism in rural and urban Nepal. Overall, we found a lack of awareness of autism as a specifically named concept, particularly in parents of non-autistic children and in primary school teachers, community health workers, early child development teachers and traditional healers – professionals who are usually the first point of access to health and education support for families of atypically developing children. This was perceived to be especially the case in rural areas. With the exception of those parents with a child diagnosed as being on the autism spectrum, very few participants could explicitly identify autism from the descriptions presented in the vignettes. The lack of knowledge and awareness of respondents without prior knowledge of the condition is both significant and concerning. Encouragingly, however, most participants appeared to demonstrate some implicit awareness of autism as a distinct entity, as suggested by the descriptions given to the vignettes of children with possible autism compared to those with other developmental conditions (see Figure 2). Furthermore, parents’ and professionals’ causal beliefs about autism predominantly focused on factors that were within the realm of a person’s control – factors that they believed were potentially preventable – and which reflected a lower level of understanding of genetic causes of autism.
Participants’ lack of awareness of autism in this study is consistent with the few existing studies of knowledge of autism in LICs. Reports of health professionals’ understanding of atypical development, specifically autism, in countries such as Pakistan (Imran et al., 2011; Rahbar et al., 2011) and Nigeria (Bakare et al., 2009a, 2009b; Eseigbe et al., 2015; Igwe et al., 2010, 2011), all clearly demonstrate limited understanding of autism as a distinct named entity. This is perhaps not unexpected given that adults’ conceptualizations and expectations of how children should behave vary considerably across cultures, including in the importance and value of play, use of eye contact and initiation of conversation (Ingstad and Whyte, 1995). Variations from what is expected in a particular context might be labelled as ‘abnormal’ but this will vary at least to some extent (Scheer and Groce, 1988). Yet, in Nepal, anecdotal evidence following the first Autism Awareness Day (run in April 2012) suggested an unusually severe lack of understanding of autism in medical professionals (Shrestha and Santangelo, 2014) – reports that were confirmed by the only Nepali study showing that the majority of paediatricians surveyed had inadequate understanding of, and clinical practice in dealing with, autism (Khatri et al., 2010). Furthermore, one-fifth of the paediatricians sampled mistakenly believed autism to result from parental neglect and half believed that autism was preventable (Khatri et al., 2010). Our study critically extends these findings to educators and allied-health professionals, as well as parents of typically developing children, in Nepal.
Such lack of awareness is not surprising. Autism is a relatively new medical diagnosis in Nepal, with relatively few reported cases before 2004 (Shrestha and Santangelo, 2014). Indeed, Nepali language has not yet developed its own terminology to refer to the concept of autism – reflected in our study by the use of English terminology within Nepali sentences to refer to autism and other scientific descriptors. A case review of characteristics of children presenting to the only centre for the diagnosis and management of autism in Nepal, ACNS, reported a mean age of diagnosis of 55.6 months (range = 12–180 months) – often too late for many children to receive early intervention of the sort typically delivered in Western nations (Shrestha and Shrestha, 2014). A review of available epidemiological evidence from five other low-to-middle income countries demonstrated a similarly late age of diagnosis of 47–56 months compared to children with autism in high-income countries (37 months) (Mandell et al., 2005). Anecdotal reports also suggest that diagnosis is likely to be restricted to children with more severe cases of autism, which means that children with less severe symptoms and with higher intellectual functioning are not likely to seek help outside the family or their immediate community in LICs. The lack of awareness of autism as a distinct entity, for which specific interventions might be possible, in parents and professionals is deeply concerning and represents a major barrier to the timely recognition and support for these children and their families (Samms-Vaughan, 2014), who are likely to be the main sources of support and care for such children.
A recent review of published evidence on interventions aimed at improving outcomes for children with disabilities in LICs called for a move beyond merely counting numbers of children to learning from the experience of families of children with autism (Yousafzai et al., 2014). To this end, our study also sought to understand the impact of autism on the lives of the children and their families in an understudied, under-resourced setting, including the types of support and actions parents and professionals feel are needed to improve these children’s lives in Nepal. Participants clearly prioritised two key issues with significant implications for future research and policy, including (1) promoting awareness and (2) training for front-line professionals combined with continued service provision.
The first issue related to raising awareness of the condition, both its causes and its consequences, in urban and especially rural Nepal. Parents of autistic children reported being subject to significant stigma from their communities. Consistent with these parents’ reports, the terms used by other participants to describe the vignettes of the children with atypical development generally had negative connotations (see Figure 2). The stigmatising reported by our parents of children on the autism spectrum is not isolated to Nepal: parents in high-income countries also often feel that others are critical of their parenting abilities, leading to overwhelming feelings of guilt and shame (Broady et al., 2015; Gray, 1993, 2002). There may, however, be differences in the underlying nature of the stigma in the different cultural contexts, including in the widely reported (at least anecdotally) hierarchy of stigma, where those with social, behavioural and communications difficulties are usually the most excluded (Wickenden and Elphick, 2015). Unfortunately, there is little formal research on the stigma and its hierarchy associated with different types of disabilities in distinct cultural settings.
With the exception of parents of children with autism and paediatricians, many of our participants further felt that the causes of autism and atypical child development were firmly rooted within parents’ control. Poor parenting was consistently highlighted as one such cause. At first glance, these beliefs seem to echo those of now-disproven theories attributing autism to parents’ failure to bond effectively with their child (Bettleheim, 1967; Kanner, 1949). But the participants in this study did not view autism to be caused by so-called ‘refrigerator mothering’ parenting. Rather, autism and childhood atypicalities were consistently attributed to poor parental discipline and control – a different, albeit equally mistaken, view. It is also akin to the kinds of theories of causation that many have about a range of other types of impairments in low-income settings where scientific information is scarce (Ingstad and Whyte, 1995). Nevertheless, in Nepal, this perceived stigma around atypical child development in general and autism, in particular, is likely to be a significant obstacle both to the timely seeking of support for these children and to opportunities for the children and their families to participate actively in their communities.
Importantly, our participants also identified other potential causes of autism, which they believed to be within a person’s – particularly the mother’s – control, including maternal malnutrition, prenatal medication and birth complications. There is increasing attention towards preconception and prenatal genetic and environmental risk factors for autism, although the evidence is still mixed (Chaste and Leboyer, 2012). Several studies of Western families have identified associations between such non-genetic risk factors, including pregnancy complications, and autism (Chaste and Leboyer, 2012; Gardener et al., 2009; Lyall et al., 2014). Very few studies, however, have examined these associations in LICs such as Nepal, where poverty and maternal malnutrition is substantially more common compared with high-income countries. The role of these non-genetic risk factors in the development of autism is virtually unknown in these settings and is an important avenue for future research.
The wide-ranging – and often erroneous and culturally constructed – explanations provided by our participants are concerning for those affected by autism as they do not necessarily promote a positive attitude to either the child or their parents. Promoting awareness of autism and (a)typical child development in general in communities is one way to address these beliefs, and the resulting stigma and discrimination for the individuals concerned and their families. Indeed, most of our participants called for greater awareness of autism. But they also identified a second key issue: an urgent need to train professionals on the identification and management of children with developmental difficulties including autism and their families, especially in rural areas. This call is consistent with a recent report from the WHO (2013), which recognised that inadequate knowledge and skills to identify and manage autism and other developmental conditions by healthcare professionals is a serious barrier to improving access to services globally. The report recommended that efforts to improve services for autistic people should take place within the context of service improvement for developmental conditions, child and family health and mental health more broadly, with primary healthcare workers providing early detection of impairments and facilitation of coordinated care and support.
While the WHO report focused on training specifically for primary healthcare workers, the participants in this study identified the need to enhance the knowledge base of a broader range of professionals, including community health workers and educational professionals. Here, we demonstrate that there is insufficient knowledge of developmental conditions like autism across all of these front-line professionals. The size of some of our participant groups meant that we were unable to compare levels of knowledge of atypical child development by parental or professional status. Nevertheless, our findings suggest that the parents of children without a known diagnosis of autism and faith healers knew the least, followed by community health workers and ECD teachers who had lower levels of knowledge than primary school teachers. Together with participants’ perception that knowledge was particularly lacking in community members and professionals from rural Nepal, our results suggest that training should be specially targeted on rural communities, community health workers and ECD teachers.
Capacity building around service provision for children with autism and their families must first address increasing awareness and knowledge of the full range of developmental atypicalities, including the careful identification of the overlapping conditions of cognitive/intellectual impairment and various social, communication, behavioural and attention difficulties. But it also needs parallel programmes designed to target both the detection and the identification of autism together with early intervention and ongoing educational input for autistic children, young people and adults and their families. Indeed, many of our participants believed strongly that education should be a priority for children diagnosed with autism, although they were divided as to whether these children should learn in regular classroom alongside their non-autistic peers or in segregated classes within specialist provision.
Globally, there is a shift towards inclusive education approaches, where all or the majority of children with disabilities attend their local schools, which adapt the curriculum to their individual needs (Centre for Studies on Inclusive Education, 1994). Unfortunately, however, Nepal has not been actively engaged in this movement and has as yet to develop truly inclusive provision for disabled children (Lewis and Little, 2007). Notwithstanding these pedagogical differences, there is an urgent need to develop brief educational modules, using innovative and open access e-learning approaches (see Durkin et al., 2015) for front-line health and education professionals in Nepal, especially in rural areas. Such interventions with teachers have been shown to enhance knowledge of childhood psychiatric disorders (including autism) in a lower middle-income country setting, urban India (Daniel et al., 2013). Similar efforts to develop low-cost, evidence-based interventions for delivery by non-specialist professionals and parents are essential for addressing both the key difficulties associated with autism and their characteristic learning and everyday needs.
Conclusion
This is the first study to examine Nepali parents’ and professionals’ understanding of atypical development and autism, in particular. Its strengths include the wide range in professionals interviewed – both from health and education – and the inclusion of parents of children both with and without a diagnosis of autism, the study of both typical and atypical child development, the use of vignettes and locally created artwork to support discussion, the collaborative nature of the work with community partners, ACNS and MIRA, and the study sites, which represented both urban and rural settings in a LIC with relatively low rates of under-fives mortality.
There were also, however, several limitations of this work. First, our parent groups were not matched in terms of age or socioeconomic status. The parents of children with a diagnosis of autism, however, are a highly select group, mainly derived from professional classes, urban settings and with enough financial resources to move to the capital, Kathmandu, to seek out medical review. A study focused on parent groups matched in terms of age and other variables would have resulted in a highly selective sample, the results of which would not have been generalisable to parents in Nepal more broadly. Second, we were unable to conduct focus groups for all participant groups, instead conducting semistructured interviews for some professionals. This approach was unavoidable, however, due to the challenges of gathering some of the groups (e.g. ECD teachers and faith healers) together and the fact that for one group, the rural paediatricans, there was only one such professional in the entire district. Although we used the same topic guides in the focus groups and interviews, these different methods may have nevertheless yielded slightly different results. Finally, our participants came from a wide range of ethnic backgrounds, which precluded us from examining the role of ethnicity on people’s perceptions of autism and typical development.
This study clearly demonstrates a vital need for greater community awareness and recognition of autism in Nepal. This need was perceived by our participants to be greatest in rural areas. Key issues for policymakers are the need to educate communities that autism and other developmental disabilities are not caused by poor parenting, that professionals (and parents) need more information and targeted training about practical ways to help autistic children and to develop services for parents particularly in rural areas. Future work should seek to evaluate the best ways to increase awareness and enhance support available for autistic and other disabled children, their families and those who support them in Nepal.
Footnotes
Acknowledgements
The authors are grateful to all of the participants who so generously gave up their time to take part in this study, to Marc Stears for comments on a previous draft of this article, to Dan Sinclair for creating ![]() , to AutismCare Nepal Society for hosting training days for the researchers (in particular, Dr Sunita Maleku Amatya, Rena Shrestha and Sijan Shakya) and to Lynn Babbington and Shiobain Corsie for their role in providing an insight into existing services in Nepal and introducing the UCL and MIRA research teams to AutismCare Nepal Society.
, to AutismCare Nepal Society for hosting training days for the researchers (in particular, Dr Sunita Maleku Amatya, Rena Shrestha and Sijan Shakya) and to Lynn Babbington and Shiobain Corsie for their role in providing an insight into existing services in Nepal and introducing the UCL and MIRA research teams to AutismCare Nepal Society.
Funding
The facilitator training and pilot study for this project was funded by the Institute of Education (IOE)/UCL Strategic Partnership Incubator Fund. Dr Michelle Heys is funded by the National Institute for Health Research, UK. Research at the Centre for Research in Autism and Education (CRAE) is supported by The Clothworkers’ Foundation and Pears Foundation