
Abstract
Accumulating evidence indicates that co-occurring alexithymia underlies several facets of the social-emotional difficulties common in individuals with autism spectrum disorder. The mechanisms involved, however, remain poorly understood because measuring alexithymia relies heavily on self-report. To address this issue, carefully matched groups of individuals with autism spectrum disorder and comparison participants rated 70 emotion-inducing pictures on subjectively experienced arousal while skin conductance responses were monitored objectively. The results demonstrated reliable correlations between these subjective and objective measures, and in both groups, around 25% of individual differences in this correlation (i.e. in emotion-relevant interoception) were accounted for by self-reported alexithymia. In the context of the wider literature, this suggests that alexithymia involves a disruption in how physiological arousal modulates the subjective experience of feelings in those with and without a diagnosis of autism spectrum disorder. Since mindfulness-based therapies foster greater awareness of thoughts, feelings and bodily sensations, the findings also have implications for how the symptoms and consequences of alexithymia (e.g. anxiety) might be ameliorated.
Introduction
Recent evidence indicates that several facets of the social-emotional difficulties commonly associated with autism spectrum disorder (ASD) are the consequence of co-morbid alexithymia – a difficulty in identifying and describing one’s own emotions that affects an estimated 40%–50% of individuals with ASD (Berthoz and Hill, 2005). For example, alexithymia has been shown to account for the difficulties many individuals with ASD experience in fixating the eye-region of faces and in recognising facial, vocal and musical expressions of emotions (Allen et al., 2013; Bird and Cook, 2013). Empathic brain responses to the pain of others is also predicted by alexithymia rather than ASD symptoms (Bird et al., 2010), and in general population samples, alexithymia mediates the relationship between sub-clinical autistic traits and certain social reward and empathic processes (Aaron et al., 2015). Such findings are important because they resolve inconsistencies in the literature concerning social-emotional processes in ASD by showing that certain difficulties in this domain are not a feature of ASD per se but a feature of co-morbid alexithymia (see Bird and Cook, 2013; Brewer et al., 2015; Gaigg, 2012 for further discussion).
An important caveat of the above literature is that the measurement of alexithymia relies almost exclusively on self-report questionnaires that require participants to reflect on the difficulties they have in reflecting on their own emotions (Vorst and Bermond, 2001). This is not only counter intuitive but also makes it difficult to specify the mechanisms through which alexithymia impacts social-emotional processes and that could serve as targets for treatment. One possibility is that alexithymia in the context of ASD is a reflection of the broader impairments in mental-state reasoning that characterise the disorder (Moriguchi et al., 2006). This, however, seems unlikely because alexithymia and mental-state reasoning are subserved by distinct neural mechanisms (Bernhardt et al., 2013; Silani et al., 2008). The question therefore remains what it is that makes it difficult for those with alexithymia to identify and describe their own emotions.
From the perspective of models that consider the perception of physiological arousal (interoception) to play a central role in the subjective experience of feelings (Craig, 2009), those with alexithymia might either fail to gain awareness of otherwise typical physiological arousal or demonstrate atypical arousal with consequences for the subjective experience of emotions. Based on evidence that physiological arousal to emotive stimuli is often preserved in ASD, while subjectively reported feelings are not (Ben Shalom et al., 2006), this article tests the prediction that alexithymia represents an impairment in the awareness of otherwise intact physiological facets of emotional experiences in ASD. If this is true, self-reported alexithymia should predict the degree to which objectively measured physiological arousal is associated with subjective reports of feeling aroused.
Methods
Subjects
In total, 13 adults with ASD (1 female, 12 male) and 13 typically developing (TD) adults (all male) were recruited from an existing database to achieve groups that were closely matched on chronological age, intellectual functioning (Wechsler Adult Intelligence Scale (WAIS)-III UK; The Psychological Corporation, 2000) and critically also alexithymia (Bermond–Vorst Alexithymia Questionnaire (BVAQ) 1 ; Vorst and Bermond, 2001). Care was also taken to ensure that the range of alexithymia within each group was representative of the range generally experienced by individuals with and without ASD. For comparison with Table 1, the average BVAQ score in the general population is 41, with scores below 43 thought to indicate the absence, and scores of above 53 the presence, of alexithymia (Deborde et al., 2008). ASD participants were diagnosed according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria by experienced clinicians through the UK health services, and administration of the Autism Diagnostic Observation Schedule–Generic (ADOS-G; Lord, et al., 2000) confirmed difficulties in reciprocal social and communicative behaviours that are the hallmark clinical feature of the disorder. The Autism-Spectrum Questionnaire (AQ; Baron-Cohen et al., 2001) provided further support for the diagnosis and confirmed that none of the TD participants experienced difficulties commensurate with ASD. All study procedures received ethical approval by the host institutions’ ethics committee, and all participants provided informed consent in line with the Declaration of Helsinki.
Psychometric characteristics of the ASD and TD groups.

ASD: autism spectrum disorder; TD: typically developing; SD: standard deviation; BVAQ: Bermond–Vorst Alexithymia Questionnaire; ADOS-G: Autism Diagnostic Observation Schedule–Generic.
Verbal (VIQ), Performance (PIQ) and Full-Scale (FIQ) WAIS-III UK Intelligence Quotients.
ADOS-G communication (Com.), reciprocal social interaction (RSI) and total (Tot.) algorithm scores.
Materials and design
For the experimental task, 50 images were chosen from the International Affective Picture System (IAPS; Lang et al., 2008) 2 to cover as wide a range as possible on the nominal valence (M = 4.59; standard deviation (SD) = 2.16; range = 1.51–8.03) and arousal (M = 5.60; SD = 0.96; range = 3.56–7.15) ratings that comprise this stimulus database. An additional 20 images were drawn from various websites to generate a final pool of 70 images that varied widely in content and emotional salience. Images were presented for 6 s each in one of two fixed pseudo-random orders.
Throughout the experiment, skin conductance responses (SCRs) were monitored at 1 kHz using an ADInstruments PowerLab System through stainless steel bipolar SCR electrodes attached to the medial phalanges of the index and ring fingers of the non-dominant hand. LabChart 7 (ADInstruments, 1994–2011) was used for the recording and offline processing of the data. Following standard procedures (Bradley et al., 2001), SCRs were quantified as the peak response within the 6-s picture presentation window, applying a log transformation (log(SCR + 1)) to normalise the distribution of the data. It is worth noting that the magnitude and the range of SCRs reported in this study are comparable to those of previous studies using similar materials and procedures (e.g. Bradley et al., 2001; Lang et al., 1998).
Procedure
Participants rated each of the 70 images on how positive or negative it made them feel (the valence dimension) and how intense this emotional experience was (the arousal dimension). Instructions emphasised that ratings should reflect the participants’ actual feelings at that moment rather than what they thought an appropriate feeling would be. Ratings were given through a keyboard on a 9-point scale, where valence ranged from very negative (1), through neutral (5) to very positive (9) and arousal ranged from calm and peaceful (1) to highly aroused and excited (9). After explaining the task in full, participants were asked to give their written consent.
Results
Prior to testing the principle prediction that self-reported alexithymia would predict the degree of association between objectively measured and subjectively reported levels of arousal in both groups, it was important to establish that groups did not differ overall with respect to these dependant variables. In terms of the average responses across all images, there were no group differences with respect to the arousal ratings (TD: M = 5.52, SD = 0.63; ASD: M = 5.22, SD = 1.24; t = 0.77, df = 24, p = 0.45), valence ratings (TD: M = 4.58, SD = 0.51; ASD: M = 4.43, SD = 0.63; t = 0.66, df = 24, p = 0.51) or SCRs (TD: M = 0.089, SD = 0.053; ASD: M = 0.075, SD = 0.081; t = 0.54, df = 24, p = 0.59). In addition, an item analysis confirmed that the average arousal and valence ratings for each image within the ASD group was highly correlated with the average image ratings of the TD group (valence: r = 0.95, p < 0.001; arousal: r = 0.82, p < 0.001), and average SCRs were also correlated between groups (r = 0.50, p < 0.001). Thus, there was no indication of substantive group differences with respect to the key dependant variables.
Turning to the inter-correlations between variables, in line with previous studies (Bradley et al., 2001), arousal and valence ratings were inversely correlated in both the TD (r = −0.63, p < 0.001) and ASD groups (r = −0.62; p < 0.001). Partial correlations, controlling for valence ratings, furthermore confirmed that SCRs were highly associated with arousal ratings in both groups (TD: r = 0.55; p < 0.001; ASD: r = 0.51; p < 0.001), demonstrating that SCRs represent a reliable physiological correlate of participants’ subjective experience of arousal. 3 Most importantly, as illustrated in Figure 1, individual differences in participants’ BVAQ scores were inversely correlated with their overall SCRs (Figure 1(a); r = −0.46; p < 0.05), indicating that alexithymia is associated with reduced levels of peripheral arousal. In addition, however, BVAQ scores were also inversely correlated with individual differences in the association between subjectively reported and objectively measured levels of arousal (Figure 1(b); r = −0.57; p < 0.005), suggesting that alexithymia may also be associated with a reduced awareness of peripheral arousal. To maintain this latter conclusion, however, it is important to rule out the possibility that reduced awareness of arousal is not simply the consequence of reduced levels of arousal and therefore the last correlation analysis was repeated while controlling for overall SCR levels. Importantly, the association between BVAQ scores and the association between subjectively reported and objectively measured arousal held (r = −0.50; p < 0.05). Thus, over and above attenuated levels of arousal, alexithymia is associated with reduced awareness of arousal. Importantly, Fisher’s r to z transformations indicated that there were no significant group differences in any of these correlations (z < 0.56; p > 0.58), and power calculations indicated that at least 300 participants would be required in each group for an 80% chance of detecting reliable group differences.
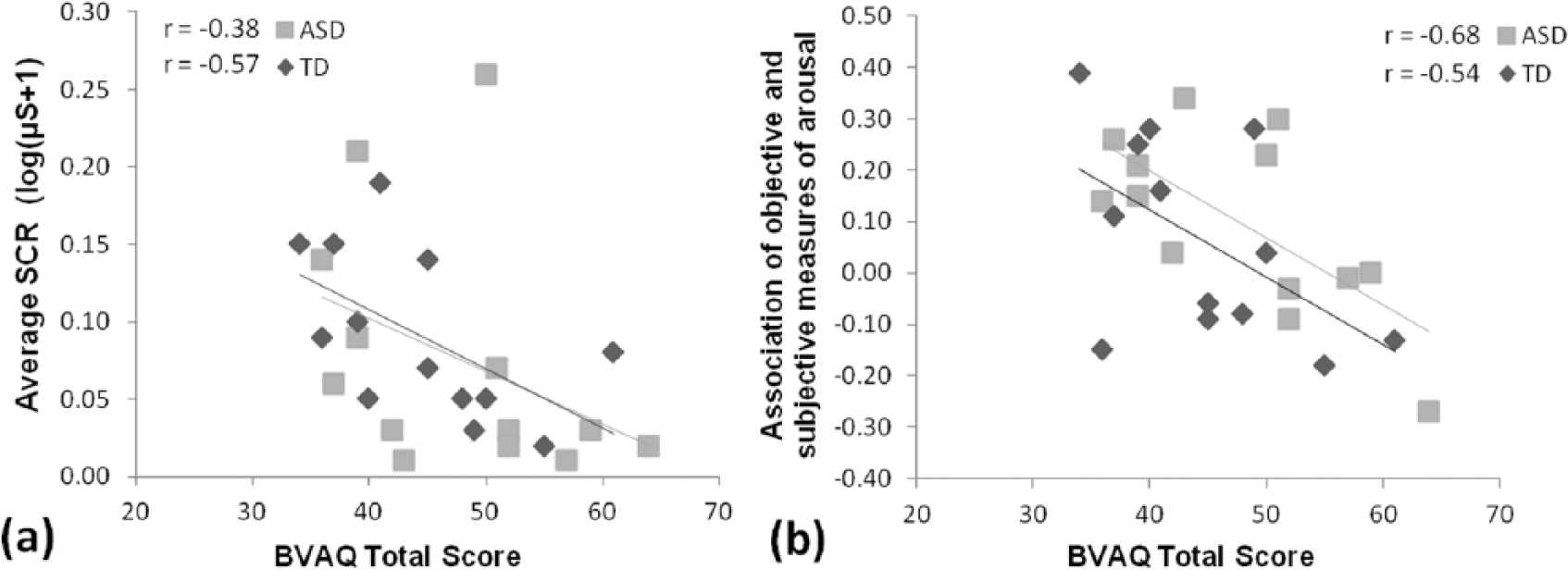
(a) Association between the participants’ BVAQ alexithymia scores and average SCRs across all images and (b) association between BVAQ alexithymia scores and the magnitude of the correlation between SCRs and arousal ratings.
Discussion
The present results make three important contributions to the literature. First, they elucidate the psychophysiological mechanisms that underlie the emotional interoception difficulties of alexithymia. The data show that self-reported difficulties in identifying and describing own emotions are associated with reduced SCR and independently also with a reduced concordance between subjectively reported and objectively measured levels of arousal in both groups. This confirms that at least two distinct processes can contribute to alexithymia – one involving a blunting of emotional experiences (Type 1 alexithymia) and the other involving reduced awareness and cognitive processing of otherwise preserved emotional experiences (Type 2 alexithymia) (see Vorst and Bermond, 2001 for further discussion).
The second contribution is that the present findings confirm that self-report alexithymia questionnaires identify qualitatively very similar emotional interoception difficulties in those with and without a diagnosis of ASD. Specifically, the pattern of correlations between alexithymia questionnaire scores and subjective and objective measures of arousal were very similar in both groups. This is consistent with the observation that self-report levels of alexithymia also predict neural activity in the insula cortex to the same extent in those with and without ASD during emotional interoception and empathy tasks (Bird et al., 2010; Silani et al., 2008). It is important to remember, however, that both in the current and previous studies, care was taken to compare ASD and non-ASD samples who were closely matched on self-reported alexithymia. Such sampling ensures that the analysis of within-group correlations is not confounded by between-group differences in critical measures. However, it also means that samples are not necessarily representative of the populations from which they are drawn because high levels of alexithymia are rare in the general population but common in ASD. In representative samples, we would expect to find significantly lower or no correspondences between subjective and objective measures of arousal in ASD, which is precisely what previous studies have indicated when groups are not purposefully matched on alexithymia (Ben Shalom et al., 2006). We would also expect attenuated levels of arousal in ASD but the evidence here is less consistent (see Gaigg, 2012; Rogers and Ozonoff, 2005), which may reflect a greater prevalence of Type II rather than Type I alexithymia in this population (Berthoz and Hill, 2005).
It is important to acknowledge the relatively small sample size as a possible limitation of this study. This was, unfortunately, inevitable given a very careful sampling procedure that ensured that groups were closely matched in terms of age, IQ as well as alexithymia, while also ensuring a representative range of alexithymia within each group. Importantly, the inclusion of a substantial number of experimental trials, and the fact that robust correlations were observed where expected, suggests that the sample size was sufficient for the aims of this study. Moreover, a power analysis suggested that over 300 participants would be needed in each group to observe reliable differences between ASD and TD participants in the correlations of key interest. Although this further suggests that differences between groups are negligible, the present findings should be considered preliminary and further studies are necessary to establish how far the current observations generalise to the broader autism spectrum.
Assuming that the findings do generalise, it is interesting to consider the wider implications for how we might support individuals with ASD who experience co-morbid alexithymia. It is well known that alexithymia negatively impacts psychotherapeutic treatment efficacy (Lumley et al., 2007) and that many individuals with ASD seek treatment for mental health difficulties such as depression and anxiety (Simonoff et al., 2008). Given that the current observations suggest that alexithymia involves a difficulty in gaining awareness of the body’s state of arousal, it follows that mindfulness-based therapies, which foster greater awareness of inner moment-to-moment experiences of thoughts, feelings and bodily sensations (Hölzel et al., 2011), may prove useful in unlocking the full treatment potential of primary therapies for individuals with ASD and alexithymia. Evidence for a close link between alexithymia and anxiety in ASD (Maisel et al., 2016) and of the impact of mindfulness on alexithymia levels (Baer et al., 2006) lends support to this suggestion, but systematic studies are necessary to thoroughly examine this issue.
Footnotes
Acknowledgements
The authors would like to thank Prof. James Hampton for offering invaluable advice on aspects of the analyses reported in this paper.
Funding
This work was supported by a Biomedical Vacation Scholarship awarded to A.S.F.C. by the Wellcome Trust (London, UK) and by a City University London (London, UK) Pump Priming grant awarded to S.B.G. and G.B.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.