
Abstract
This study aimed to examine the mechanisms responsible for the association between the broad autism phenotype and depressive symptoms in mothers of a child with autism spectrum disorder. A total of 98 mothers who had a child with autism spectrum disorder between the ages of 2 and 16 years completed assessments of maternal broad autism phenotype, child behavior problems, romantic relationship satisfaction, friend support, family support, and maternal depressive symptoms. Results indicated that only romantic relationship satisfaction was a significant mediator of the relationship between maternal broad autism phenotype social abnormalities and maternal depressive symptoms, where greater broad autism phenotype social abnormalities were associated with lower relationship satisfaction, which in turn was associated with increased depressive symptoms. Child behavior problems were directly related to increased depressive symptoms. Implications regarding maternal mental health outcomes within this population as well as intervention implications are discussed.
Keywords
Autism spectrum disorder (ASD) is a prevalent developmental disorder with rates that recently increased from 1 in 88 children in 2012 to 1 in 68 children in 2014 (Center for Disease Control and Prevention (CDC), 2014). Parenting a child with ASD is a stressful experience, and mothers often report low levels of well-being (Ekas and Whitman, 2010). Mothers of a child with ASD may experience milder symptoms characteristic of ASD, which are referred to as the broad autism phenotype (BAP; Hurley et al., 2007). Indeed, as many as 23.2% of mothers of children with ASD report above the diagnostic cutoff for the BAP (Sasson et al., 2013a). The BAP consists of three clusters of sub-diagnostic ASD behaviors including social abnormalities (also known as aloof personality), rigid personality, and pragmatic language difficulties (Hurley et al., 2007; Sasson et al., 2012, 2013b). These align with the characteristic ASD symptoms of social deficits, stereotyped and repetitive behavior, and abnormalities with respect to communication and are inherently linked to social interactions and relationships. These BAP symptoms are also associated with poor mental health outcomes for mothers, such as experiencing depressive symptoms, beyond the impact of child ASD symptoms (Ingersoll et al., 2011; Ingersoll and Hambrick, 2011). If we consider child ASD and maternal BAP as unique influences on maternal mental health outcomes, mothers may be likely to experience negative outcomes not only by having a child with ASD but also by having an increased likelihood to experience BAP symptoms. Both characteristics of the child with ASD and characteristics of the mother may contribute to the mother’s mental health outcomes. This study aimed to examine not only whether the two factors of child behavior problems and maternal BAP contribute to mental health outcomes but also the mechanisms through which these factors operate.
Associations between child behavior problems and maternal outcomes
Parenting a child with ASD is a stressful experience, and mothers of children with ASD report clinically elevated levels of depressive symptoms, and these rates are higher than those of parents with typically developing children (Bitsika et al., 2013; Ingersoll and Hambrick, 2011). Although the core symptoms associated with ASD have been linked to poor functioning in mothers of children with ASD (Davis and Carter, 2008), children’s behavior problems are also a source of stress for these mothers (Lecavalier et al., 2006). Specifically, research has shown that behavior problems are associated with negative maternal outcomes including greater negative affect and higher depressive symptoms (Barker et al., 2011; Pottie et al., 2009). Furthermore, behavior problems are stronger predictors of maternal outcomes than the core symptoms of ASD (Ekas and Whitman, 2010). Some researchers have speculated that behavior problems may be especially difficult to manage and may also elicit negative attention in social settings (Davis and Carter, 2008). Therefore, behavior problems not only directly impact maternal mental health but may also contribute to feelings of social isolation due to the nature of the behaviors and the situations in which they occur.
Although there is a direct relationship between child behavior problems and maternal mental health outcomes, there has been little research examining potential mechanisms that explain this association. One possible mechanism is the quality of mothers’ social relationships, which have been found to be especially important for positive maternal adjustment (e.g. Smith et al., 2012). Generally, social support refers to a “relationship transaction” between people (Zimet et al., 1988). Social support can be either instrumental (pertaining to physical resources) or emotional (Boyd, 2002) and can come from a variety of sources including friends, family, and significant others (Zimet et al., 1988). In one study, Smith et al. (2012) found that social support was related to better well-being over time for mothers of children with ASD. Social support was also linked to lower levels of reported depressive symptoms for mothers in this population (Falk et al., 2014). However, raising a child with ASD can strain mothers’ social relationships and lead to decreased quality and amount of social support. For example, the presence of a child with ASD, as well as the child’s overall symptom severity, has been associated with lower social support as well as lower relationship satisfaction for mothers (Gau et al., 2012; Ingersoll and Hambrick, 2011). Social support may be particularly important to consider in this population given that parents of a child with ASD often report feeling socially isolated and feeling that they have lost support (Altiere and Von Kluge, 2009; Myers et al., 2009). Taken together, the existing body of research suggests that it is possible that characteristics of a child’s ASD, particularly behavior problems, are a risk factor for poor social relationships and support for mothers, which is associated with negative mental health outcomes for mothers of children with ASD.
Associations between BAP and maternal outcomes
Although the behavior problems of children with ASD negatively impact mothers’ mental health outcomes (Ekas and Whitman, 2010), this may not be the only contributing factor for poor maternal outcomes. There are characteristics of the mother that may contribute to her well-being. For example, certain coping styles (i.e. avoidant coping) are used more frequently in parents of children with ASD (Lai et al., 2015) and have been associated with higher levels of depressed mood (Benson, 2010). The maternal characteristic of intolerance of uncertainty was found to be associated with increased levels of anxiety in mothers of children with ASD (Uljarević et al., 2016). Mothers who have a more external locus of control also tend to experience lower well-being (Falk et al., 2014). Although these aforementioned characteristics may contribute to maternal mental health outcomes, the influence of the BAP may be particularly important to examine due to its increased prevalence among mothers of a child with ASD (e.g. Sasson et al., 2013a). Indeed, Sasson et al. (2013a) recently reported that 23.2% of mothers of a child with ASD, compared to 8.1% of mothers in the comparison group, had higher BAP prevalence rates.
Among mothers of children with ASD, the BAP may influence mental health outcomes, with studies showing that BAP symptoms are associated with greater depressive symptoms (Ingersoll and Hambrick, 2011), even after accounting for child ASD symptoms (Ingersoll et al., 2011). However, there is still a need to further investigate the impact of the BAP on mental health due to inconsistent evidence within the literature. Although few studies have examined the influence of the BAP on current depressive symptoms, there are studies that have examined the impact of the BAP on clinical mood disorders. For example, although higher rates of major depressive disorder have been found within the parents of children with ASD, clinical depression (i.e. major depressive disorder) was not associated with the BAP (Bolton et al., 1998; Piven and Palmer, 1999). However, some studies have found that parents often experienced the first episode of depression before the birth of their child (Micali et al., 2004). Therefore, more research is needed to understand the mental health of mothers of a child with ASD, particularly their current experiences.
The BAP inherently contains social deficits whereby those who have elevated levels do not enjoy or have an interest in social interactions, have difficulties in adapting to change, and have problems effectively communicating or participating in conversation (Hurley et al., 2007). Therefore, due to the fact that the BAP consists of social deficits combined with the evidence from above that social relationships are especially important for mental health outcomes, it is possible that social relationships may explain the association between maternal BAP and mental health outcomes. In the general population, the social aspects of the BAP (i.e. social abnormalities and pragmatic language difficulties) have been linked with difficulties in social cognition as well as with lower levels of social skills (Sasson et al., 2012). The BAP has also been associated with detrimental impacts on both friendships and relationships in the general population (e.g. Jobe and White, 2007). For example, the BAP has been associated with lower numbers of friendships, lower duration of friendships, more loneliness, lower relationship satisfaction, and poor interpersonal interactions (Jobe and White, 2007; Wainer et al., 2013). Among college roommates, when social abnormalities were high in one roommate and low in the other, there were lower amounts of relationship satisfaction, suggesting that the mismatch on the BAP was detrimental for relationships (Faso et al., 2016).
Among mothers of children with ASD, the BAP negatively impacts social relationships as seen in lower levels of reported social support (Ingersoll and Hambrick, 2011). However, social support was measured as the type of social support received (e.g. emotional support), and no studies have examined the impact of the BAP on different sources of social support for mothers of children with ASD. Furthermore, romantic relationships are an important form of social support, given that a mother’s significant other is part of her innermost circle of support (Benson, 2012). No studies to date have examined the impact of the BAP on relationship satisfaction within mothers of a child with ASD. Therefore, child behavior problems and maternal BAP are two factors that impact not only maternal mental health outcomes but also social relationships.
This study
Following the model of maternal mental health outcomes presented above, this study aimed to determine the association between child behavior problems and maternal BAP and maternal depressive symptoms through the mediating factors of social relationships. This study expanded on previous research (i.e. Ingersoll and Hambrick, 2011) by examining child behavior problems instead of core ASD symptoms, the unique contributions of each of the BAP subscales, and different sources of social support and quality of social relationships (relationship satisfaction, friend support, and family support). It was hypothesized that because child ASD symptoms were associated with lower social support for mothers (e.g. Ingersoll and Hambrick, 2011) and poor mental health outcomes (e.g. Barker et al., 2011) that child behavior problems would also negatively influence relationship satisfaction, friend support, and family support, which would in turn be associated with greater maternal depressive symptoms. Furthermore, due to the impact of maternal BAP on social relationships (e.g. Ingersoll and Hambrick, 2011) and mental health outcomes (Ingersoll et al., 2011), a similar relationship was hypothesized for the association between maternal BAP, relationship satisfaction, friend support, and family support (see Figure 1(a)). More importantly, due to the emphasis on social relationships in this model, it was also hypothesized that the symptoms associated with the social abnormalities subscale of the BAP would be most predictive of outcomes.

(a) Hypothesized model and (b) final model containing only significant estimates and standard errors.
Method
Participants
A total of 98 mothers of a child with ASD completed an online survey. Mothers were selected from a larger sample and qualified for the study if they were in a relationship and had no missing data on any of the variables in the study. The mothers in the study were between the ages of 25 and 56 years (M = 37.68 years, standard deviation (SD) = 5.45 years) and reported that they had a child diagnosed with ASD between the ages of 2 and 16 years (M = 8.27 years, SD = 3.10 years). The children were predominantly male (83.7%). The majority of the sample was Caucasian (82.7%) with the remaining mothers identifying as Hispanic or Latin American (9.2%), African American (4.1%), Asian or Pacific Islander (2.0%), or other (3.1%). In addition, the sample was well educated, and the majority of mothers had at least a college degree (73.5%). Finally, 47% of mothers reported a household income between US$40,000 and US$100,000 with the remaining 14.3% reporting an income level below and 38.8% reporting above that range.
Procedure
Mothers were contacted through national online ASD resources and organizations, via social media, and word of mouth. After expressing interest in the study, mothers were emailed to provide additional information about the study and ensure they qualified. After determining that the mothers qualified, they were emailed a link to the online questionnaires where they consented to participate in the study and then completed questionnaires about their demographics, BAP characteristics, child symptoms and behaviors, relationship satisfaction, friend support, family support, and depressive symptoms. After completing the online questionnaires, mothers were mailed a US$10.00 gift card. The study received approval from the authors’ institutional review board.
Measures
BAP
Mothers completed the Broad Autism Phenotype Questionnaire (BAPQ), which is a valid and reliable measure of the qualitatively milder but similar traits of ASD in relatives (Hurley et al., 2007). This questionnaire contains 36 items to which mothers responded on a 6-point Likert-type scale (1 = very rarely to 6 = very often). The scale was divided into three subscales that each contained 12 items: social abnormalities, pragmatic language difficulties, and rigid personality. The social abnormalities subscale reflects difficulties with social interaction, and sample items include “I would rather talk to people to get information than to socialize,” “conversation bores me,” and “I prefer to be alone than with others.” The pragmatic language difficulties subscale reflects difficulties with the social features of language and contains items such as “it’s hard for me to avoid getting sidetracked in conversation” and “I speak too loudly or softly.” The third subscale, rigid personality, describes difficulties with change and includes items such as “I feel a strong need for sameness from day to day” and “I act very set in my ways.” After reverse coding 15 items, a mean was calculated, and higher scores on each subscale indicated more difficulties. The internal consistencies were 0.92, 0.83, and 0.89 for the social abnormalities, pragmatic language difficulties, and rigid personality subscales, respectively.
Child behavior problems
Mothers responded to the Strengths and Difficulties Questionnaire (SDQ), a valid and reliable measure of child behavior problems (Goodman, 1997). It is a widely used measure and has been previously used within the ASD population (e.g. Hastings et al., 2014). This measure contains 25 items to which mothers responded on a 3-point scale (not true to certainly true). Items from this scale include “restless, overactive, cannot stay still for long,” “often loses temper,” and “constantly fidgeting or squirming.” After reverse coding five items, 20 items from the emotional problems, conduct problems, hyperactivity, and peer problems subscales were summed in order to create a total score of child difficulties. Higher scores indicated more behavior problems. The internal consistency for the present sample was 0.83.
Relationship satisfaction
Mothers completed the Couples Satisfaction Index (CSI), which is a valid and reliable measure that assesses how they perceived aspects of their relationship and how satisfied they were with their relationship (Funk and Rogge, 2007). The measure contains 32 items and although the descriptors of each scale point varied, mothers responded on a 6-point Likert-type scale to each question. Sample items include “please indicate the degree of happiness, all things considered, of your relationship” and “I still feel a strong connection with my partner.” After reverse coding seven items, a sum score was calculated, and higher scores indicated a greater degree of relationship satisfaction. Internal consistency for the present sample was 0.98.
Social support
Mothers responded to the Multidimensional Scale of Perceived Social Support (MSPSS), a valid and reliable measure of perceived sources of social support (Zimet et al., 1988). Mothers responded to 12 items on a 7-point Likert-type scale (1 = very strongly disagree to 7 = very strongly agree). The scale contains three subscales that each consist of four items. Each subscale asks about support from a different source, and for this study, only the friend and family subscales were used. Items from these subscales include “I can count on my friends when things go wrong” and “my family really tries to help me.” For each subscale, mean scores were calculated, and higher scores indicated more perceived support from each source. The internal consistencies for the friend and family subscales were 0.95 and 0.92, respectively.
Maternal depressive symptoms
Mothers completed the Center for Epidemiologic Studies Depression Scale (CESD), a valid and reliable measure of depressive symptoms (Radloff, 1977). The scale contains 20 items, which reflect different symptoms of depression, and mothers respond how often they experienced those symptoms in the past week on a 4-point Likert-type scale (0 = rarely or none of the time, <1 day, to 3 = most or all of the time, 5–7 days). Sample items include “I felt depressed,” “I felt lonely,” and “I was bothered by things that usually don’t bother me.” After reverse coding four items, sum scores were calculated where higher scores indicated a higher level of reported depressive symptoms. The internal consistency for the present sample was 0.91.
Results
Descriptive statistics and correlation analyses
Descriptive analyses were conducted to examine the prevalence rates of BAP characteristics and depressive symptoms for the current sample. Utilizing the cutoff scores provided by Sasson et al. (2013a), there was a prevalence rate in this sample of mothers of children with ASD of 20.4% for social abnormalities, 16.3% for pragmatic language difficulties, 17.3% for rigid personality, and 17.3% for the total BAP. These are comparable to the rates reported by Sasson et al. (2013a). In the current sample, 18.4% were elevated on only one subscale, 10.2% were elevated on two of the subscales, and 5.1% were elevated on all three subscales. In addition, 48.0% of mothers in this sample reported depressive symptoms above the clinical cutoff score of 16 (Radloff, 1977). Mothers who met the cutoff for the total BAP (M = 22.88, SD = 10.05), F(1, 96) = 7.56, p < 0.01, were more likely to experience depressive symptoms than those who did not (M = 15.02, SD = 10.84). Mothers who met the social abnormalities subscale cutoff (M = 24.05, SD = 11.80), F(1, 96) = 13.60, p < 0.001, also were more likely to experience more depressive symptoms than mothers below the cutoff (M = 14.42, SD = 10.05). Finally, those who were elevated on the rigid personality subscale (M = 22.24, SD = 10.41), F(1, 96) = 6.04, p < 0.05, reported more depressive symptoms than mothers who were not elevated (M = 15.16, SD = 10.87), but no significant differences were found for the pragmatic language difficulties subscale, F(1, 96) = 1.23, p = 0.27.
Before conducting the analyses pertinent to the research questions, analyses were conducted to determine whether any demographic variables (e.g. child age, child gender, maternal age, maternal ethnicity, maternal education, marital status, and household income) needed to be included in the analyses. It was determined that no demographic variables were significantly related to any of the outcome variables in the study. Next, correlations were computed to determine the relationship between the study variables (see Table 1 for descriptive statistics). As seen in Table 2, maternal social abnormalities were significantly associated with lower relationship satisfaction, r = −0.25, p < 0.05; lower friend support, r = −0.42, p < 0.001; lower family support, r = −0.26, p < 0.05; and greater depressive symptoms, r = 0.40, p < 0.001. Pragmatic language difficulties were associated with more depressive symptoms, r = 0.24, p < 0.05, and rigid personality was associated with lower relationship satisfaction, r = −0.21, p < 0.05, as well as greater depressive symptoms, r = 0.31, p < 0.01. Child behavior problems were only significantly associated with greater depressive symptoms, r = 0.32, p < 0.01. Finally, lower relationship satisfaction, r = −0.38, p < 0.001; lower friend support, r = −0.24, p < 0.05; and lower family support, r = −0.29, p < 0.01, were all significantly associated with greater depressive symptoms.
Descriptive statistics.
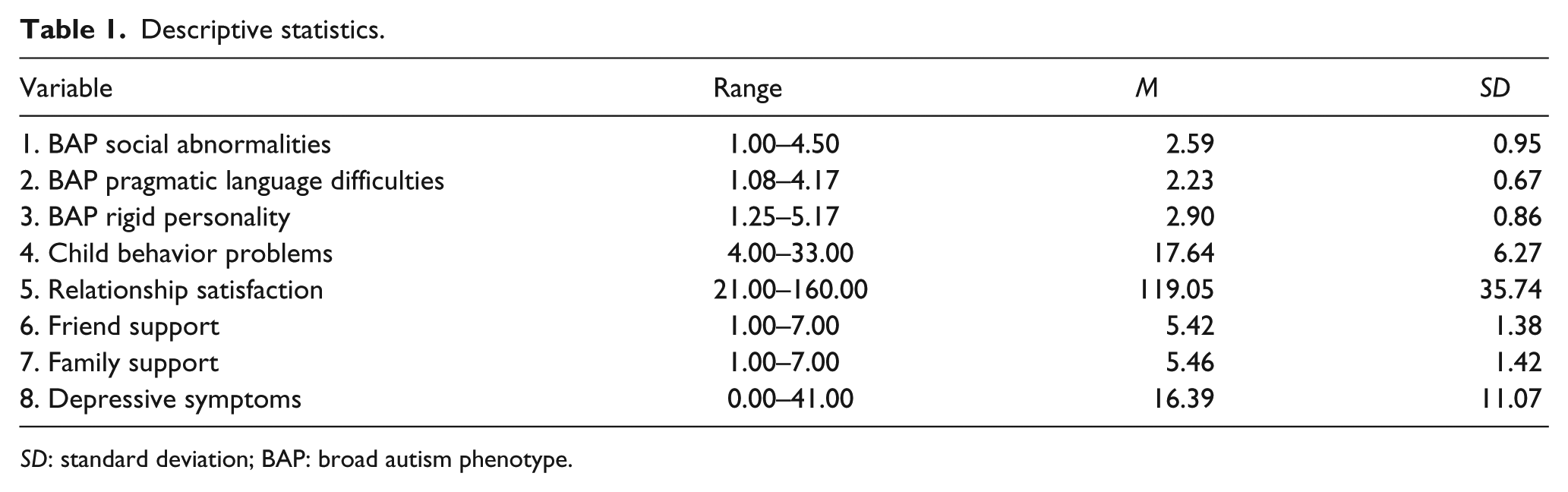
SD: standard deviation; BAP: broad autism phenotype.
Correlations between study variables.

BAP: broad autism phenotype.
p < 0.05; **p < 0.01; ***p < 0.001.
Mediation analyses
In order to test the hypothesized model (see Figure 1(a)), the MEDIATE macro in SPSS (Hayes and Preacher, 2014) was used to produce the 90% Monte Carlo confidence intervals of the indirect effects of maternal social abnormalities, pragmatic language difficulties, rigid personality, and child behavior problems on depressive symptoms through relationship satisfaction, friend support, and family support using 10,000 resamples. As seen in Figure 1(b), only relationship satisfaction was a significant mediator for the relationship between BAP social abnormalities and depressive symptoms (indirect effect = 0.68, standard error (SE) = 0.45, 90% confidence interval (CI) = (0.07, 1.52)), where greater BAP social abnormalities were associated with lower relationship satisfaction, b = −8.82, SE = 4.42, p < 0.05, which in turn was associated with greater depressive symptoms, b = −0.08, SE = 0.03, p < 0.05. Furthermore, child behavior problems were only directly related to increased depressive symptoms, b = 0.42, SE = 0.06, p < 0.01. Friend support and family support did not emerge as significant mediators in this model. This entire model accounted for 32.5% of the variance in depressive symptoms (see Table 3 for the results of the entire model).
Results of the mediation model.
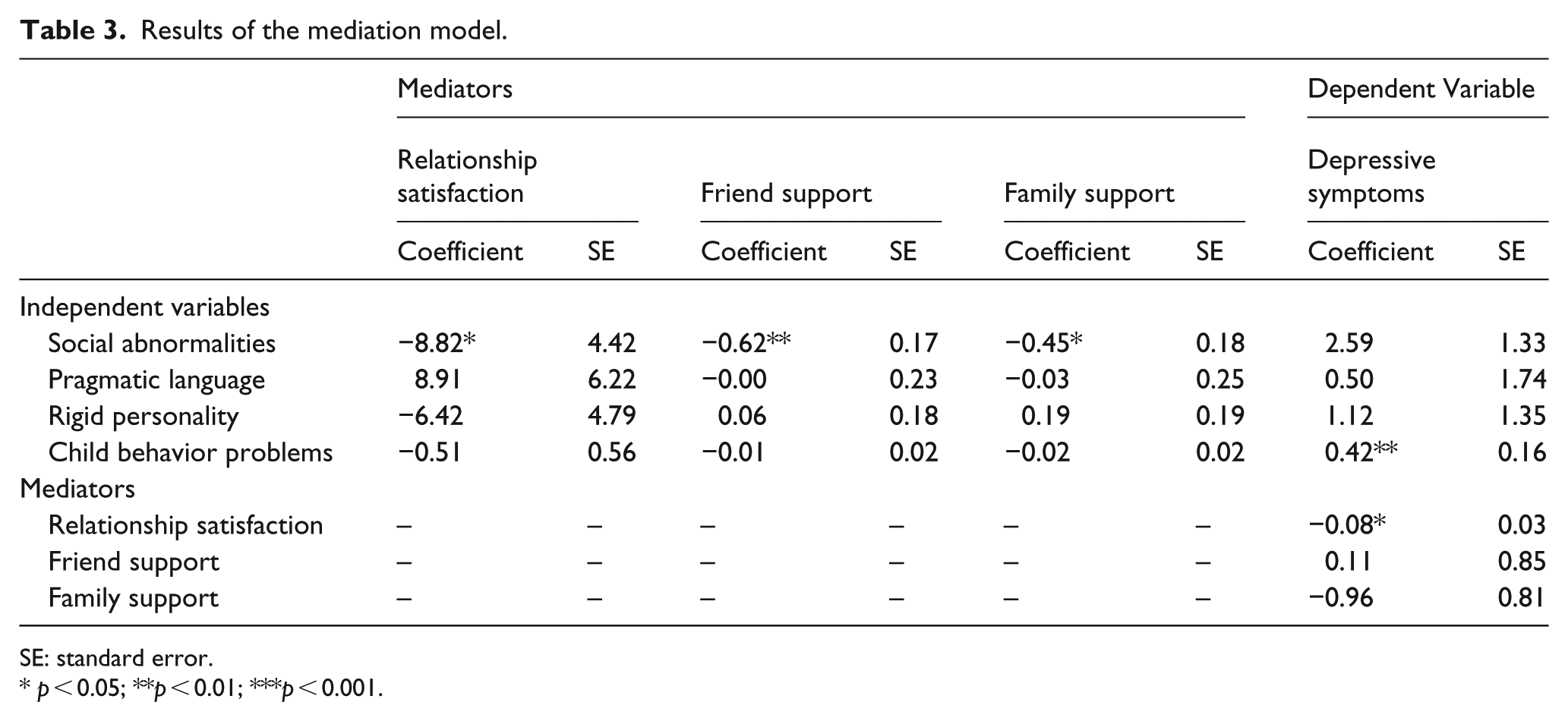
SE: standard error.
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This study investigated the contributions of child behavior problems and maternal BAP to maternal depressive symptoms through the mediating factor of social relationships. It was hypothesized that above and beyond child behavior problems, maternal BAP characteristics, particularly the social abnormalities subscale, would be associated with lower relationship satisfaction, friend support, and family support, which in turn would be associated with the presence of greater maternal depressive symptoms. Consistent with these hypotheses, child behavior problems were associated with the presence of greater maternal depressive symptoms; however, this relationship was not mediated by any of the social relationships measured. However, maternal BAP, specifically the social abnormalities subscale, was associated with the presence of greater depressive symptoms, and this relationship was mediated by relationship satisfaction. In sum, child behavior problems were directly associated with greater depressive symptoms, and maternal BAP social abnormalities were associated with lower relationship satisfaction, which in turn was associated with the presence of greater depressive symptoms.
Associations between BAP and maternal outcomes
The study findings confirmed the hypothesis that maternal BAP characteristics contribute, above and beyond child behavior problems, to maternal mental health outcomes for mothers of a child with ASD. Consistent with previous research (e.g. Ingersoll and Hambrick, 2011), the association between maternal BAP and mental health outcomes was mediated by maternal social relationships. However, expanding on that research, it appears that sources of social support (i.e. significant other, family, and friend) are also important to consider. Although BAP negatively impacted each of these social relationships, only relationship satisfaction was associated with maternal mental health outcomes. Therefore, this study suggests that a mother’s romantic relationship may be a particularly important social relationship for mothers with BAP. Previous research has also demonstrated that relationship quality is associated with greater well-being beyond the contribution of social support in mothers of children with developmental disabilities (Kersh et al., 2006). Indeed, mothers have reported that their significant other is their most helpful source of informal support (Searing et al., 2015).
There are several possible explanations for why the romantic relationship, and not friend or family support, was found to mediate the association between maternal BAP and mental health outcomes. First, a mother’s romantic partner is in her innermost circle of support (Benson, 2012), so that relationship may be more salient for the mother. In addition, because raising a child with ASD may contribute to feelings of social isolation (Myers et al., 2009), mothers may feel that only their significant other understands the situation since their significant other may face the same challenges on a daily basis. Therefore, if mothers are not feeling satisfied or happy with their romantic relationship, there may be adverse consequences for their mental health. In families that consisted of both biological parents, it is possible that the father may also have elevated BAP symptoms (Klusek et al., 2014; Seidman et al., 2012). In a small percentage of families of a child with ASD, both parents have elevated scores on the composite BAP (4.3%) or on any one component of the BAP (15.1%; Sasson et al., 2013b). If both members of the dyad experience social difficulties, this could contribute to lower relationship satisfaction and then poorer mental health outcomes for mothers. Given the findings of this study, it may be especially important to intervene at the level of the romantic relationship since individuals with a child with ASD are at risk of lower relationship satisfaction (Gau et al., 2012), and relationship quality is particularly important for maternal outcomes (Kersh et al., 2006).
Consistent with findings in the general population (Sasson et al., 2012) and in parents of children with ASD (Losh and Piven, 2007), only the social aspects of the BAP, namely, social abnormalities, were associated with social outcomes. It is possible that because those high in BAP social abnormalities struggle with using appropriate social skills and have difficulties with social cognition (Sasson et al., 2012), they may not be able to identify friend and family member’s actions as being helpful or supportive and then are unable to use those individuals as a coping mechanism to reduce depressive symptoms. The social abnormalities subscale of the BAPQ contains items such as “I would rather talk to people to get information than to socialize,” “conversation bores me,” and “I prefer to be alone than with others.” Someone who identifies with these items may not possess the skills necessary to utilize supports that are available or may not have supports available due to difficulties in engaging in social interactions. Therefore, mothers who are endorsing these items may be less socially motivated and not rely on social support as much as mothers who do not score high on the BAP. In the context of their romantic relationship, these mothers could be less motivated to seek support and comfort from their partner. We did not find the other BAP characteristics to be associated with maternal social relationships or mental health outcomes. This could be due to the salience of BAP social abnormalities, as discussed above, or because the rates of pragmatic language difficulties were approximately 6% lower in this study compared to other studies of mothers of children with ASD (Sasson et al., 2013a). Further research is needed to replicate these findings. Future studies should examine both the quantity and quality of social relationships in order to test the explanations posited above.
Although this study provides evidence that maternal BAP is associated with depressive symptoms, this is contrary to studies that found no association between BAP and major depressive disorder (e.g. Bolton et al., 1998; Piven and Palmer, 1999). The cross-sectional nature of the study does not allow us to determine the directionality of the effects. For example, previous studies have found that parents experienced the first episode of depression before the birth of their child with ASD (Micali et al., 2004). Therefore, it is possible that depressive symptoms may negatively impact maternal BAP symptoms and social relationships. Nonetheless, this study provides additional support for the relationship between the BAP and current depressive symptoms (e.g. Ingersoll and Hambrick, 2011). Overall, this study suggests that mothers of children with elevated BAP social abnormalities may experience difficulties in their romantic relationship that contribute to mental health problems.
Associations between child behavior problems and maternal outcomes
Consistent with previous research, we found that child behavior problems were directly associated with poor maternal functioning (Ekas and Whitman, 2010), in the form of elevated depressive symptoms. Although previous studies (e.g. Ingersoll and Hambrick, 2011) found that core ASD symptoms (i.e. communication deficits, social deficits, and restricted and repetitive behaviors) were associated with lower social support and in turn greater depressive symptoms, this study did not replicate those findings. There are several possible explanations for these discrepant findings. First, this study assessed child behavior problems and not core ASD symptoms. Although behavior problems have been shown to be better predictors of maternal outcomes compared to core symptoms (e.g. Ekas and Whitman, 2010), this study suggests that behavior problems are not associated with social relationships. This could be because behavior problems are more relatable for outside sources, since children other than those with ASD can also exhibit behavior problems. Thus, mothers may feel supported regardless of their child’s behavior problems. Due to the direct nature of the effect of child behavior problems, there may be characteristics of the mother that reflect her response to these behavior problems, such as the presence or absence of optimism. Indeed, researchers have found that optimism mediates the relationship between child behavior problems and well-being in mothers of children with developmental delay (Baker et al., 2005).
Another possibility may be the difference in how social relationships were conceptualized and measured. Ingersoll and Hambrick (2011) measured different functions (i.e. emotional and informational) of social support and relationships as opposed to perceptions of social support from friends and family and relationship satisfaction. It is possible that merely perceiving availability of support is not enough, but rather, it is the function that the support serves for the mother. For example, a mother may feel that she has a friend she can turn to, but it may matter whether she is turning to that person for emotional support or informational support. Regardless of the pathway through which child behavior problems impact maternal well-being, child behavior problems do indeed appear to be one risk factor for the presence of depressive symptoms in mothers of children with ASD. Taken together, the results of this study suggest that a dual risk model of maternal health outcomes may be appropriate for mothers of children with ASD. Both child behavior problems and maternal BAP were associated with mental health outcomes; however, the pathways were different. While child behavior problems were directly associated with maternal depressive symptoms, the association between maternal BAP and depressive symptoms was mediated by relationship satisfaction.
Limitations and future directions
Although this study expanded on previous research by exploring a dual risk model of maternal functioning in the context of social relationships, there were some limitations. First, this study only utilized self-reports of all study variables, which may bias the results. With respect to maternal ratings of BAP symptoms, it is important to include multiple informants, as mothers often report themselves as higher on certain symptoms compared to their partners’ ratings (Seidman et al., 2012). Future studies should obtain both measures and average the two sources (Sasson et al., 2014) to obtain a more accurate report of BAP characteristics. In addition, child ASD diagnosis and behavior problems were also self-report, and diagnosis was not confirmed with diagnostic testing. Given our online sampling method of data collection, it was not possible to independently confirm children’s diagnosis. However, many studies of parents of children with ASD rely on self-report of children’s diagnoses (e.g. Lai et al., 2015; Maljaars et al., 2014). Other child characteristics, such as intellectual functioning, may influence the results of this study, and this study did not have a measure of this child characteristic. Maternal levels of depressive symptoms are also an important consideration. Depressive symptoms may make parents more accurately report child behavior problems, but this could also distort their report as well (Parent et al., 2014). In addition, this study only utilized self-report of current depressive symptoms and was not able to conduct comprehensive clinical interviews that would allow for not only investigation of clinical depression history but also of other affective disorders. This may be especially important since parents of a child with ASD often experience other affective disorders (e.g. social anxiety; Kuusikko-Gauffin et al., 2013).
Given the important role of relationship satisfaction in this study, it would be important to include the perspective of mothers’ partners, in order to investigate how one partner’s characteristics impact not only themselves but also their partner, as other studies have done (e.g. Ekas et al., 2015). This would allow for an in-depth investigation of the complex interplay of social relationships and interactions and more accurately reflect quality of relationships. In addition, fathers may also be particularly important to include as fathers often score higher on the social abnormalities subscale of the BAP (Seidman et al., 2012). The selection of only mothers currently in a relationship may also have influenced the findings. Mothers who are not currently in a romantic relationship often report greater social support needs (e.g. Bromley et al., 2004), and this may be because they lack the daily support that an intimate partner provides. Finally, this study was cross-sectional in nature, and although we tested a mediation model, longitudinal data are necessary to establish the temporal sequence that we hypothesized. Maxwell and Cole (2007) recommend three time points of data collection to test for true mediation. Therefore, the results of this study should only be viewed as an initial exploration of the association between child behavior problems, maternal BAP, maternal social relationships, and mental health outcomes. Future studies should incorporate a longitudinal design to determine the directionality of the associations found in this study.
Despite these limitations, this study provides preliminary evidence for a model of mental health outcomes for mothers of children with ASD that considers both characteristics of the child and characteristics of the mother. Although a mother may be impacted directly by child behavior problems, having a child with ASD is not the sole risk factor. In addition to child behavior problems, maternal BAP, particularly social abnormalities, negatively impacts a mother’s relationship satisfaction, which then is associated with the presence of greater depressive symptoms. The implications of this study are twofold. First, because maternal BAP is associated with increased depressive symptoms, the BAPQ could be used to screen for mothers who are at particular risk of poor well-being. Additionally, for those who are identified as possessing these social BAP symptoms, social skills training and relationship counseling could potentially help to positively impact a mother’s mental health outcomes. Therefore, it is important to consider both characteristics of the child and characteristics of the mother in determining how to promote greater well-being in this population.
Footnotes
Acknowledgements
The authors thank the mothers who participated in this research.
Funding
This research was supported by the Science and Engineering Research Center, Texas Christian University.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.