
Abstract
The Social Communication Questionnaire is one of the most commonly used screening tools for autism spectrum disorder. The Social Communication Questionnaire is a caregiver-reported questionnaire with 40 items based on questions from the Autism Diagnostic Interview–Revised. This study collected Social Communication Questionnaire data from a community-based, multi-stage case identification design epidemiologic study in one socioeconomically disadvantaged county in Taiwan. The Social Communication Questionnaire was distributed to 3034 school children, aged 6–8 years. Item prevalence results indicate males were reported to have more autism-related behaviors than females (higher prevalence on most items), in the whole study sample as well as in children meeting Social Communication Questionnaire clinical cut-offs (⩾15). Children whose biological fathers completed the Social Communication Questionnaire were reported to have more behavioral issues than children whose biological mothers were the respondent. Lower respondent education levels were associated with reports of clinically concerning autism-related behaviors. However, males were not at higher risk of meeting Social Communication Questionnaire clinical cut-offs than females in this study population. Findings from this study help to better understand reporting patterns on children’s autism-related behaviors potentially due to social demographic characteristics and child sex, which may lead to improved identification of these behaviors.
Keywords
Introduction
Evidence indicates that many children live with autism spectrum disorder (ASD) without being diagnosed (Principal Investigators of the Autism and Developmental Disabilities Monitoring Network, 2016). This finding underscores the urgent need for population-based studies that provide full coverage of case identification in a target population. Though providing clinical assessments to each individual in a population is not practical, multi-stage case identification that involves screening followed by clinical evaluation of those found to be at high risk is a feasible way to identify ASD, especially for populations with lower socio-economic status (SES).
Screeners that aim to identify individuals at high risk of ASD are vital for multi-stage case identification. However, heterogeneity in the severity of autism-associated traits and behaviors across individuals with ASD has led researchers to suggest the disorder forms a continuum that extends into general populations. If the spectrum of the disorder exists, as many researchers agree, it is critical to better establish the distribution of traits and behaviors associated with ASD (i.e. the “normal range”) in the general population.
The Social Communication Questionnaire (SCQ) has been widely used for assessing ASD (Norris and Lecavalier, 2010), with established reliabilities and validities from children with a higher risk of ASD (e.g. children from special education programs or developmental pediatric clinics). Although numerous studies from Western countries recommend a cut-point of 15 on the SCQ for differentiating between likely ASD and non-ASD diagnoses, some research studies that examined the psychometrics of the SCQ indicated that the optimal cut-point of the SCQ may differ depending on the age and other characteristics of the child (Allen et al., 2007; Chen et al., 2009; Corsello et al., 2007; Eaves et al., 2006a, 2006b; Johnson et al., 2010; Lee et al., 2007; Oosterling et al., 2010; Snow and Lecavalier, 2008; Wiggins et al., 2007; Witwer and Lecavalier, 2007). Most studies of this kind are either clinic-based (ASD prevalence is likely high) or special education–based (ASD prevalence is moderately high). However, a study conducted in the United Kingdom enrolled children, aged 9 to 10 years, with special education needs with and without ASD (high-risk group) and two groups of children of similar age from the general population (n = 411 and n = 247). The study authors reported that in the high-risk group, the SCQ strongly differentiated ASDs (including autism) from non-ASD cases with a cut-point of 15 (sensitivity = 0.88, specificity = 0.72) and autism from non-autism cases (other ASDs and non-ASD) with a cut-point of 22 (sensitivity = 0.90, specificity = 0.86) (Chandler et al., 2007). They further reported that children with an ASD diagnosis from the general population samples rarely screened negative (<0.5% had an SCQ < 15), and about 90% of children whose SCQ score was greater than or equal to 15 had an ASD or other type of neurodevelopmental disorder (e.g. language delay, attention-deficit hyperactivity disorder (ADHD)).
To accurately screen for ASD in general populations, psychometrics information is critical as reliabilities and validities from high-risk populations may not be generalizable to lower risk populations. This is the case because the distribution of autism-associated traits and behaviors and the characteristics of the respondents are likely different. In addition to the psychometrics of screening tools, investigating how social demographic characteristics relate to reporting deserves attention. As the majority of ASD screeners for children are caregiver-reported, if a reported outcome is a result of social demographic characteristics rather than “truly” objective observations, screening results would deviate from the truth. Understanding such potential disparities will improve the identification of autism-associated behaviors and reduce false positives and negatives.
Differences in the male to female ASD sex prevalence have been consistently documented. Such differences could possibly be due to a greater proportion of males than females being recognized with ASD (Dworzynski et al., 2012)—a scenario particularly problematic for clinical-based and/or case-control studies. It has been proposed that there are differences in the distribution of ASD traits in males and females, in that the female distribution is shifted toward the nonpathological end, leading to an exaggeration of the sex ratio when cut-offs are used for diagnosis (Constantino, 2011). Sex differences could also indicate that biologic or environmental exposures (e.g. hormonal exposures) exist that make males more susceptible to the disorder (Baron-Cohen et al., 2011; Knickmeyer et al., 2005). Previous research suggests that sex could represent a naturally occurring subgroup that differentiates ASD symptoms (Ben-Itzchak et al., 2013; Carter et al., 2007; Hartley and Sikora, 2009; Holtmann et al., 2007; Kirkovski et al., 2013; Lai et al., 2013; Mandy et al., 2012). Investigations on sex differences may not only provide clinicians with insight as to how clinical presentations of autism differ in each sex, it may also help to identify meaningful subgroups that can guide etiologic research and treatment programs. While behavioral development manifests differently in girls and boys, this difference can vary greatly across cultural backgrounds. Establishing “cultural references” at a population level would be invaluable when conducting research that uses clinical cut-offs of ASD-related behaviors. This is specifically true for studies conducted in cultural backgrounds that differ greatly from the cultures in which many widely used ASD screening and diagnostic tools were derived.
Parent- or caregiver-reported screeners have been applied in several studies to investigate the association between child sex and autistic features. No significant sex differences in autistic symptoms were reported in a clinical-based study using the Autism Behavior Checklist (Volkmar et al., 1993). On the contrary, results from two different screeners—the Autism Spectrum Screening Questionnaire (ASSQ) and the Social Responsiveness Scale (SRS)—applied separately in population-based studies illustrated significantly higher scores in boys than girls, indicating boys had more autistic traits than girls (Constantino and Todd, 2003; Posserud et al., 2006). Another screener, the Child Behavior Checklist (CBCL), is broadly used in studies of children with ASD to identify behavioral problems. Sex differences in rated behavior problems were inconsistent among those studies. For instance, Holtmann et al. (2007) reported significantly more social problems and attention problems in girls than boys, which contradicted the results from another study (Hartley and Sikora, 2009). These inconsistent results might be attributed to factors such as different sample sizes or study settings. For example, in general, children from clinical-based studies have relatively more severe ASD symptoms or traits compared to those from population-based ones. Therefore, differences in the severity of ASD symptoms and problem behaviors would be much smaller among children from clinical settings, decreasing the likelihood of identifying significant sex differences.
In addition to sex differences in autistic traits, other social demographic characteristics, such as respondent’s educational level, could also have effects on the accuracy of reporting and thereby the ability to detect autistic traits. Supporting this premise is evidence from a study that screened a diverse low SES population in the United States using the Modified Checklist for Autism in Toddlers (M-CHAT) during a clinical visit. Results showed that primary caregivers with a lower education level were more likely to report that their child had autism compared to those with a higher education level (Scarpa et al., 2013).
Furthermore, different informants reporting on the same child may not agree on behavior or emotional issues (Achenbach et al., 1987), which can lead to differences in reported scores. Previous studies have found discrepancies in the reporting of anxiety or depression symptoms in the same child between father and mother (Ivens and Rehm, 1988; Moreno et al., 2008). With respect to ASD symptoms, a number of studies have compared scores from different raters of the same child with ASD; however, findings vary across studies (Bolte et al., 2008; Hurley et al., 2006; Kalyva, 2010; Matson et al., 2011; Mattila et al., 2009; Posserud et al., 2006; Seidman et al., 2011). For example, one recent study from the Netherlands that focused on the reporting bias of ASD traits with the use of the SCQ found that while fathers reported higher mean SCQ total scores than mothers, there were no statistically significant differences between parental ratings (Möricke et al., 2016).
The objectives of this study are (1) to obtain a population reference of SCQ-measured ASD-associated traits and behaviors, and distributions of these measured behaviors by sex in a large population of school-age children, and (2) to examine disparities in caregiver-reported SCQ scores by social demographic characteristics in these school-age children.
Methods
Study participants
A community-based epidemiologic study of ASD in children aged 6–8 years involving a multi-stage case identification design was conducted in Pingtung, Taiwan from 2008 to 2010. Pingtung County is located on the west coast of southern Taiwan, with a population of less than one million (Pingtung County Government Department of Civil Affairs, 2015). Farming, in which nearly one-third of the population is engaged, is the main economic activity, in addition to fishery and business. Of 130 schools in the selected regions of Pingtung County, there were 122 schools with 3034 first and second graders to whom we distributed enrollment packets. Of the 3034 children, 928 had primary caregivers who were not available or were illiterate; in these cases, teachers of the subject children were asked to complete the SCQ instead. A total of 2917 respondents signed the consent form and returned the demographic survey and SCQ without missing child sex (117 children had missing sex): 1401 male children and 1516 female children. Furthermore, because the study required child sex and SCQ scores, 62 males and 64 females with missing SCQ scores (missing more than 15% of items) were excluded. As a result, data from 2791 children (1339 males and 1452 females) are included in the subsequent analysis.
Procedures
The Kaohsiung Medical University Institutional Review Board and the Johns Hopkins Bloomberg School of Public Health Institutional Review Board reviewed and approved all study procedures. With support from the Pingtung County Department of Education, research investigators contacted school principals for recruitment of first- and second-grade children and their primary caregivers. School teachers distributed enrollment packets to the children for their primary caregiver to review and sign. The enrollment packet included a study flyer, a consent form, a demographic survey (which included parental education level), a form for the primary caregiver’s contact information, the SCQ, and a stamped return envelope. It is not known how many caregivers did not receive an enrollment packet for reasons such as a teacher not distributing the packets or a student not bringing it home for any reason.
The signed consent form, demographic survey, and completed SCQ were either brought back to the school by the students in a sealed envelope where research staff were available to collect them or they were mailed back to research staff in the enclosed return envelope. The majority of SCQs and demographic surveys for the 2791 children included in this analysis were filled out by primary caregivers, most of whom were biological mothers (n = 1381), followed by biological fathers (n = 406), and other relatives (n = 118). The SCQ and demographic survey were filled out by teachers for 872 children whose primary caregivers were not available or were illiterate, while 14 were returned without an indication of the respondent’s relationship to the child. Each child had only one respondent.
SCQ
The SCQ (Rutter et al., 2003a), formerly known as the Autism Screening Questionnaire (Berument et al., 1999), contains 40 yes-or-no items that focus on three areas of functioning: Reciprocal Social Interaction (RSI); Communication; and Restricted, Repetitive, and Stereotyped Patterns of Behaviors (RRSB) (Figure 1). Based on the Autism Diagnostic Interview–Revised (ADI-R) algorithm (Rutter et al., 2003b), the questions on the SCQ were modified into an understandable form for primary caregivers to answer without further explanation. Item 1 of the SCQ asks whether the child has the ability to use phrase speech and is not a scored item. If the child is nonverbal, the next six items are skipped. As a result, the range of total scores is from 0 to 39 for individuals with language and from 0 to 33 for individuals without language. The SCQ is appropriate for subjects whose chronological age is more than 4 years with a mental age of at least 2 years. For this study, the “Lifetime” version of the SCQ was translated into traditional Chinese Mandarin and back-translated into English to assure accuracy. We tested the translated SCQ before its use in the study population. Testing consisted of giving the translated version of the SCQ to 20 parents who had a child in an elementary school in Pingtung or the nearby Kaohsiung City to ensure its readability for the target populations.
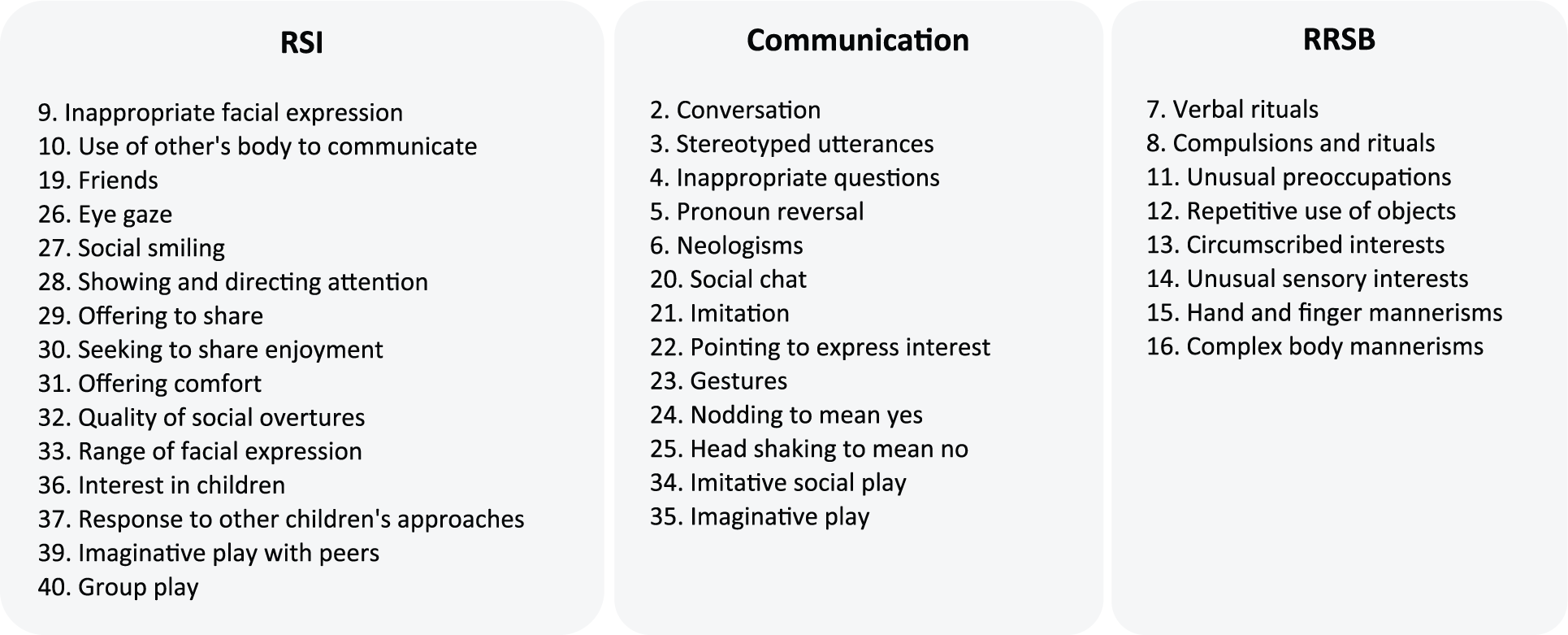
SCQ items listed under the domains of the ADI-R.
Statistical analysis
The total SCQ score was not calculated for SCQs that were missing 15% or more of the items to avoid underestimating the “true” value, which may result in false negatives (assuming that missing values would have been treated as “negative” for autism-related behaviors). A cut-off of 15 was used for subset analyses.
Cronbach’s alpha was calculated to evaluate the internal consistency of the full-scale SCQ and its three subscales. Chi-square tests were used to compare each item prevalence between males and females in the whole study population and in those with SCQ ⩾ 15. Descriptive statistics, including means and standard deviations, were used to establish the distribution of SCQ scores by social demographic characteristics in the full scale and three subscales. Analysis of variance (ANOVA) with Bonferroni post hoc tests was conducted for data with equal variances. Non-parametric Kruskal–Wallis tests were performed for data with unequal variances, followed by Dunn’s post hoc tests to compare differences between groups in each social demographic characteristic (results shown in Table 1). Additionally, odds ratios (ORs) with 95% confidence intervals (CIs) were computed using logistic regression models to evaluate the magnitude of associations between categorical SCQ scores with clinical cut-offs and each social demographic characteristic.
Distributions of SCQ full-scale scores and subscale scores by social demographic characteristics.

SCQ: Social Communication Questionnaire; RSI: Reciprocal Social Interaction; RRSB: Restricted, Repetitive, and Stereotyped Patterns of Behaviors; AA: associate of arts; SD: standard deviation.
Because SCQs that were missing ⩾15% of the items were considered as missing, the sum of subgroup sample sizes may not add up to the total study sample.
Same letters denote not statistically significant between levels of each social demographic variable; different letters denote statistically significant at p < 0.05. For example, RRSB score in the father’s education at “High school” is not significantly different from “⩽Middle school” nor from “AA/college or higher” at the p < 0.05 level.
Results
Reliability
Internal consistency of the full-scale SCQ, measured by alpha, was 0.83 in the total study sample, 0.83 in males, and 0.84 in females. Regarding the subscales, the alpha was 0.80, 0.78, and 0.81 for RSI and 0.81, 0.79, and 0.82 for RRSB in the total study sample, males, and females, respectively. The communication subscale had the lowest alphas as compared to the other two subscales (i.e. RSI and RRSB)—0.67, 0.66, and 0.68 for the total study sample, males, and females, respectively.
SCQ score distributions
The distribution of SCQ scores in this study sample is presented in Figure 2(a). Similar proportions of males and females have SCQ ⩾ 15 (9.16% for males, 9.38% for females). Using 22 as the cut-off, the gap between males and females widened: 2.46% for males and 2.05% for females. However, the difference was not statistically significant, which could be a result of small samples above the 22 cut-off. Figure 2(b) displays the cumulative distribution of SCQ scores in both sexes graphically. Figure 2(a) and (b) shows that SCQ score distributions are similar between males and females; ASD traits, as measured by the SCQ, do not appear to have higher variance in males than females in this general population.
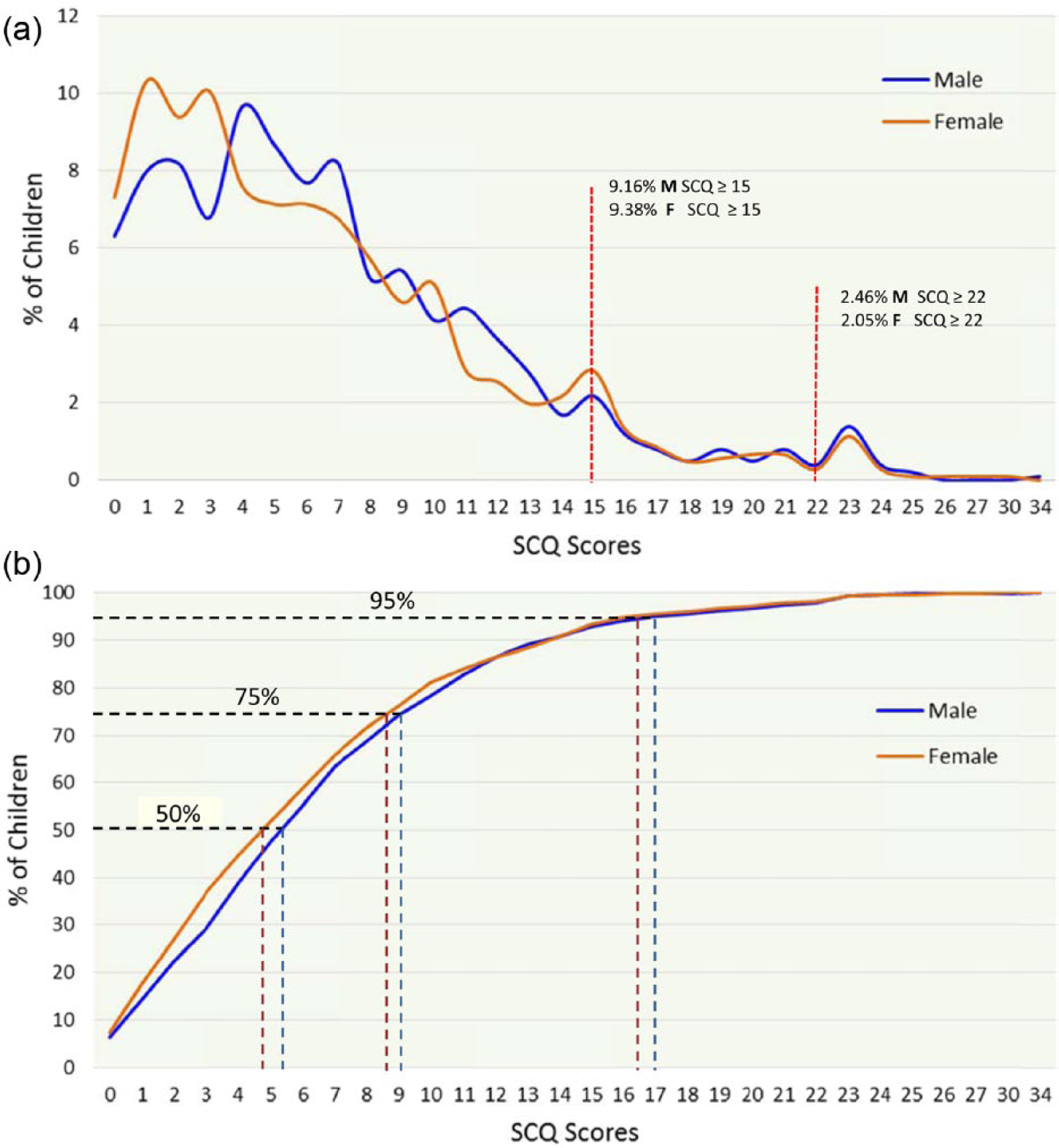
(a) SCQ score distribution by percentage of children and (b) cumulative distribution of SCQ scores by child sex.
SCQ-measured traits/behaviors
Overall, the item prevalence of each SCQ-measured trait/behavior varies in this school-aged study population, ranging from 3.3% (item 33: abnormal range of facial expression) to 36.2% (item 19: no friends). Males and females have similar patterns of item score distributions, where both sexes have higher item prevalence in the Communication subscale than in the other two subscales (Figure 3(a)). Sex differences in item prevalence in this population are presented in Figure 3(b). In general, males have a significantly higher prevalence of SCQ-measured traits/behaviors than females in the Communication and RRSB subscales.
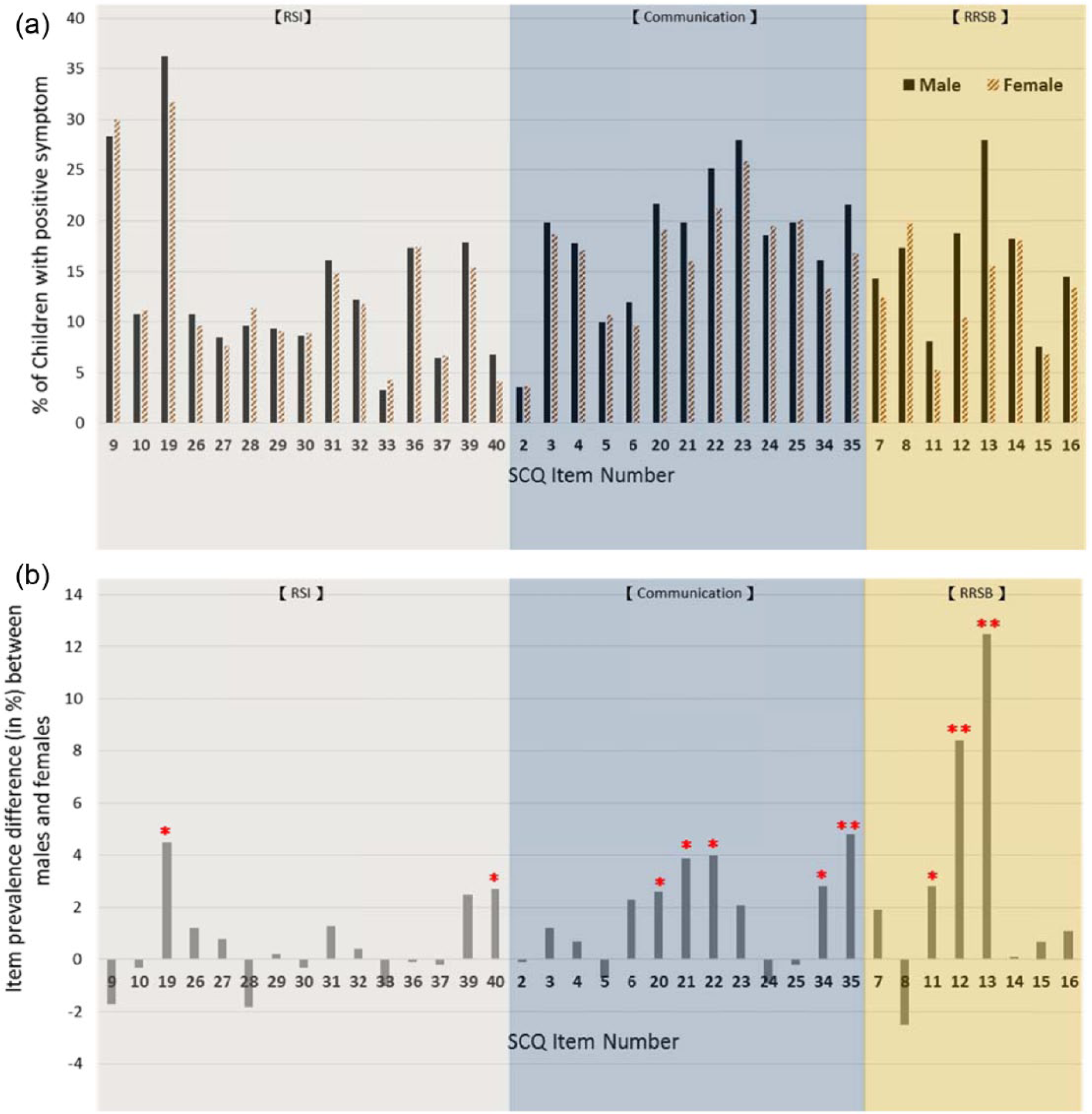
(a) SCQ item prevalence in a general child population and (b) sex difference on SCQ item prevalence (male–female) in a general child population.
As for children with SCQ ⩾ 15, the pattern of item score distribution is distinct from that in the whole study population. Figure 4(a) presents higher item prevalence of SCQ-measured traits/behaviors in the RSI and Communication subscales compared to that in RRSB. Sex differences are greater for items in the RSI and Communication subscales than in those of RRSB, where males have more items showing higher prevalence than females (Figure 4(b)). Despite higher item prevalence observed in males, only items 40 and 22 reached statistical significance (Figure 4(b)). Given that the sample size for the group with SCQ ⩾ 15 is significantly smaller than the full study sample, it was expected that significant sex differences would be detected in fewer items.
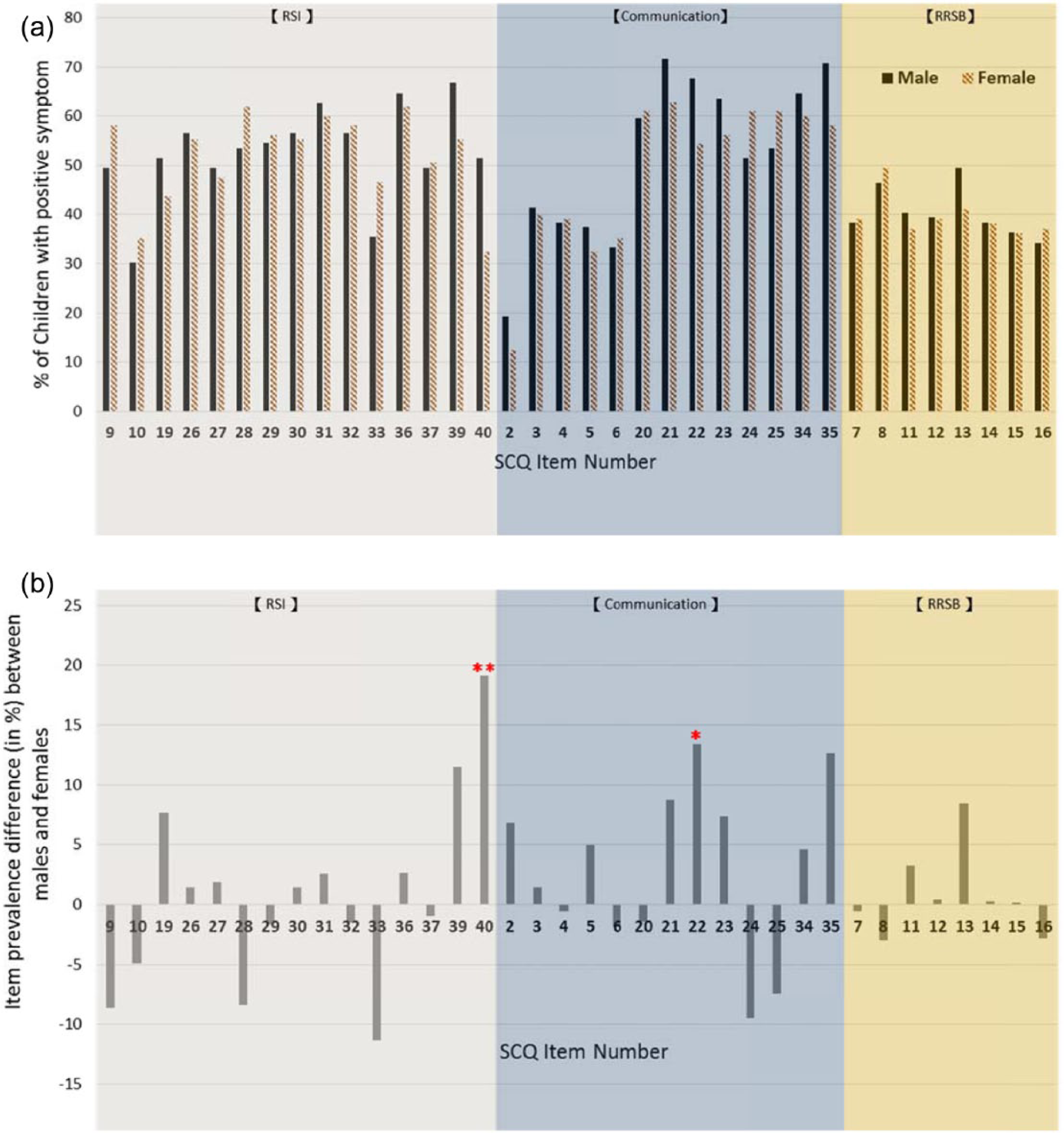
(a) SCQ item prevalence among children with SCQ ⩾ 15 and (b) sex difference on SCQ item prevalence (male–female) among children with SCQ ⩾ 15.
SCQ by social demographic characteristics
As shown in Table 1, mean scores of the full-scale SCQ, Communication subscale, and RRSB subscale are significantly higher in males than females. Children who are of greater birth order (third or greater) were reported to have higher mean scores on the RSI and Communication subscales. However, there is no statistically significant difference across the categories of birth order in the full scale or RRSB subscale. In terms of respondents (each child was only rated by one respondent), biological fathers and other relatives reported significantly higher SCQ scores (more behavioral concerns) than did biological mothers and teachers in the full scale, as well as the RSI and Communication subscales. Teachers reported significantly lower scores, on average, compared to all other respondents across the full scale and all three subscales. Furthermore, parental education level plays an important role in SCQ scores. As parental education level increased, the SCQ score decreased. This is also true for the respondent’s education level, where a lower respondent’s education level was associated with reporting a higher SCQ score.
Table 2 expands on the role of respondent relationship and education level in SCQ scores and describes the magnitude of the association between the two. Biological fathers were 2.35 times (95% CI: 1.65–3.35), and other relatives were 2.55 times (95% CI: 1.43–4.54), more likely to report a child with SCQ ⩾ 15 than were biological mothers. This pattern was different from teachers who were less likely than biological mothers to report a child with SCQ ⩾ 15, though the difference was not statistically significant. Compared to fathers with an associate/college degree, fathers with an education level less than or equal to middle school were 4.15 times (95% CI: 2.60–6.63) more likely to have a child with SCQ ⩾ 15, while those with a high school degree were almost twice (OR = 1.71, 95% CI: 1.09–2.68) as likely. A similar pattern was observed with mother’s education level where those with less than or equal to a middle school education were 5.50 times (95% CI: 3.36–8.99), and those with a high school degree were 1.74 times (95% CI: 1.08–2.81), more likely to have a child with SCQ ⩾ 15 compared to those with an associate/college degree. With regard to the respondent’s education levels, the results showed a nearly identical pattern as the parental education levels. Respondents with an education level of less than or equal to middle school were 5.56 times (95% CI: 3.63–8.51), and those with a high school degree were 1.34 times (95% CI: 0.92–1.96), more likely to report SCQ ⩾ 15 compared to those with an associate/college degree.
Associations between demographic characteristics and SCQ using 15 as the cut-off.

SCQ: Social Communication Questionnaire; OR: odds ratio; CI: confidence interval; AA: associate of arts.
Because SCQs that were missing ⩾15% of the items were considered as missing, the sum of subgroup sample sizes may not add up to the total study sample.
Values in boldface indicate those odd ratios that are statistically significant.
In addition to the educational findings from logistic regression models, children whose biological father or other relative completed the SCQ were also more likely to have SCQ scores ⩾ 15 (OR = 2.35, 95% CI: 1.65–3.35 and OR = 2.55, 95% CI: 1.43–4.54, respectively). Regarding birth order and child sex, children of third or greater birth order were 1.76 times (95% CI: 1.15–2.69) more likely to have SCQ scores ⩾ 15 than those of first birth order, whereas child sex was not associated with SCQ scores ⩾ 15.
Discussion
Data on sex differences in autistic traits or symptoms in a general child population are scarce. Studies that exist on the related topic are mainly from clinical-based studies, and they present inconsistent associations between autistic traits or symptoms and child sex. Lord et al. (1982) reported that male children have more stereotypic play or routines than do females. A study that used the ADI to assess symptomatology reported that males with autism had more deficits in social interaction and communication than females before the age of 5 years after controlling for IQ. No sex differences, however, were noted on any item of RRSB (McLennan et al., 1993). In contrast to that study, Carter and colleagues reported that boys had significantly lower scores on the Autism Diagnostic Observation Schedule (ADOS) Communication subscale compared to girls in findings from 90 ASD toddlers aged 18–33 months. There were no other significant sex differences in autism symptoms based on ADOS Module 1 and ADI scores (Carter et al., 2007). A UK study included children with higher functioning ASD aged 3–18 years and reported that females had less repetitive stereotyped behaviors than males, and suggested that such an observation is a consistent feature of a female ASD phenotype from toddlerhood through adulthood (Mandy et al., 2012).
We found that males were reported to have higher mean SCQ scores in the full scale than were females in this community-based general population, a finding similar to that reported by Mulligan et al. (2009). However, the item distribution of our study differs from that reported by Mulligan and colleagues. Some possible explanations for discrepancies are sample size and age range differences—there were 153 SCQs conducted in children aged 4–12 years in Mulligan’s study. Another possible reason is the different cultural backgrounds of the two study populations, as parents perceive their child’s behaviors differently across cultures. This underscores the importance of having a “reference” of cultural norm when evaluating a behavior. For example, we reported that females were rated as having higher mean scores in the Communication and RRSB subscales, which could be due to different cultural expectations on how a girl versus a boy should act. Our data uniquely allowed us to examine sex differences by the SCQ subscales and their individual items, which, to our knowledge, has not been reported on in previous literature. While the autism research community has been making efforts to advance global autism research, the importance of establishing cultural norms that capture a full picture of the population in its specific cultural context cannot be overstated.
With regard to birth order, some previous studies presented the firstborn child as being more likely to be at risk of autism than later ones (Croen et al., 2007; Durkin et al., 2008; Tsai and Stewart, 1983). Those findings are inconsistent with our results that showed children with later birth order had more autistic traits. A possible explanation for the birth order effect observed in previous studies is the “stoppage” phenomena where parents of one child with ASD choose not to have subsequent children because of the demands of parenting a child with a disability or a concern over genetic susceptibility. Such a decision increases the likelihood that a child with ASD is of lower birth order. Although the stoppage phenomena can occur for any developmental concern or medical condition, the likelihood of stoppage is greater if the family is aware of the medical diagnosis. The community where our study was conducted is one of the lowest SES regions in the country. Very limited health care or education programs are available to provide diagnoses, treatment, or intervention for children with ASD, as there are no clinicians in the region who specialize specifically in developmental disabilities, including ASD. Thus, it is likely that children with ASD in this community were not diagnosed or their parents did not know about the diagnosis before having other children. We therefore hypothesized that the stoppage effect may be less as compared to those reported in western countries.
Another finding from our study revealed that SCQ scores were dependent on the respondent; other relatives and biological fathers tended to report significantly higher SCQ scores than did biological mothers in the full scale, RSI, and communication subscales. Interestingly, children whose biological father had a lower education level were more likely to have children with higher SCQ scores than those with a higher education level. A similar pattern was present for maternal education level. This result is akin to that of a previous study that used the M-CHAT, another parent-reported questionnaire, illustrating that mothers with lower education levels reported more autistic traits than those with higher education levels (Scarpa et al., 2013). Clearly, respondents’ education level is an important factor in determining SCQ scores in community-based studies. A systematic review pointed out that socioeconomically disadvantaged children (e.g. household income, poverty, parental education, or parental occupation status) were two to three times more likely to develop mental health problems (Reiss, 2013). Whether the observed association between lower education level and higher reported SCQ scores is due to SES disadvantage or reporting bias cannot be answered by our study as we do not have data from multiple respondents or objective observation on the same child. We, therefore, cannot evaluate whether our above-mentioned finding is due to reporting bias.
We found that teachers reported lower SCQ scores than did other respondents. Teachers were asked to fill out the SCQ for a child when the primary caregivers were not available or illiterate. There are many reasons as to why primary caregivers are not available or illiterate. For example, some children come from single-parent families and the grandparents become primary caregivers because the mother or father works and lives outside the home. This type of family is common in Taiwan, especially in low-SES populations. However, in Taiwanese and Chinese societies, it is also common and acceptable for parents to live and work outside the home and for grandparents to take care of the children in middle-class families. In either case, questionnaires cannot be filled out by the father or mother, and it is not unusual for grandparents to be illiterate across SES levels. Because we did not have more information on the family conditions of the group of children whose teacher completed the questionnaires, we were unable to make the assumption that children whose questionnaires were filled out by teachers were more likely to be lower SES.
As expected, prevalence is higher on each item in the sample with SCQ ⩾ 15 compared to the whole study population; however, the overall distribution patterns are similar between both groups. This finding suggests that each of the three domains contributes to the SCQ total score meeting the clinical cut-off rather than a specific domain contributing disproportionally.
Findings from this study need to be interpreted with the caution as there were limitations. We learned that some teachers did not distribute the enrollment packets to students given their busy schedule and workload; however, we do not know how many did not make the distribution. Additionally, for those whose teachers distributed the package, we have no information on how many students actually brought the packets home to their caregivers. For this reason, it is challenging to estimate the extent and magnitude of potential sample selection bias, that is, whether the study sample is representative of the eligible population. However, because we collected SCQ data from either a caregiver or teacher for the majority of children, 2791/3034 (91%), bias due to non-response should not be a major concern. Despite this limitation, the study uniquely provides SCQ data at the population level from a large study population. The data provide important baselines on ASD-related behaviors, which are crucial for determining cultural cut-offs for ASD screening. In addition, the sex difference analysis at the item- and domain-level of the SCQ would not have been possible if the data were not collected from such a large study population.
Conclusion
Caregiver-reported autism-related behaviors are associated with respondents’ characteristics in this large-scale population-based study in Taiwan. While the majority of previous published reports on the SCQ are from higher risk populations, this study demonstrates the distribution of SCQ-measured behaviors in a “general population.” Overall, males have higher prevalence on item scores than females; however, they are not at higher risk than females of meeting the SCQ clinical cut-off in this defined population. In other words, our results do not support the observations that more males than females are meeting SCQ-defined ASD clinical thresholds. While the global autism research community has made every effort to find causes of ASD, it is necessary to examine the extent to which ASD-associated traits and behaviors are distributed in the “general population.” Without such baseline information, cut-offs of a screening test are irrelevant. Understanding the population distribution of these traits and behaviors would not only help with ASD identification, but would also shed light on finding etiologic factors of the disorder. As for the social demographic characteristics, our results suggest that lower education levels are associated with reports of clinically concerning autism-related behaviors. This finding indicates that the education level of the respondents is an important determinant of reported autism-related behaviors in children. Better understanding respondent characteristics that could lead to systematic differences in scores is crucial when using questionnaires like the SCQ as a screening instrument. Future studies are warranted to further explore potential reporting biases between different respondents by using multiple respondents for each child.
Footnotes
Acknowledgements
The authors would like to thank the Pingtung County Department of Education and the participating schools for their assistance and support in this study. Special thanks to the participating teachers, students, and their primary caregivers for their effort, time, and participation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection for the study was supported by Autism Speaks (grant number 2109).