
Abstract
This pilot study estimates the effects of family structure on age of diagnosis, with the goal of identifying factors that may accelerate or delay diagnosis. We conducted an online survey with 477 parents of children with autism. In addition, we carried out novel, follow-up surveys of 196 “friends and family,” who were referred by parents. Family structure and frequency of interactions with family members have significant effects on age of diagnosis (p < 0.05). In all, 25% of parents report that other individuals indicated that their child might have a serious condition before they themselves suspected it. Moreover, around 50% of friends and family report that they suspected that the child had a serious condition before they were aware that either parent was concerned, suggesting that the clues were there to see, especially for experienced viewers. While half of those individuals shared their concerns with the parents, the other half either did not raise any concern (23%) or just “hinted” at their concern (27%). Among children with siblings, children with an older sibling are diagnosed approximately 10 months earlier (p < 0.01) than those without, and children with no siblings were diagnosed 6–8 months earlier than children with siblings (p < 0.01). Interestingly, frequent interactions with grandparents, especially grandmothers, significantly lowered the age of diagnosis by as much as 5 months (p < 0.05). While this pilot study requires replication, the results identify potential causes for accelerated or delayed diagnosis, which if better understood, could ultimately improve age of diagnosis and treatment, and hence outcomes.
Introduction
Early diagnosis of autism spectrum disorder (ASD) is important for earlier intervention, which is, in turn, critical for improving treatment efficacy (Dawson, 2010; Dawson et al., 2010; Dawson and Osterling, 1997; Johnson et al., 2007). Under optimal conditions, ASD can be diagnosed by the age of 24 months or earlier. However, children are usually diagnosed, on average, at the age of 4 years or later (Lord et al., 2000, 2006). Prior research shows that several factors are associated with a delay of diagnosis, including symptom severity, race/ethnicity, and geographic location (Daniels and Mandell, 2014). Prior studies find, for example, lower prevalence of ASD among lower socio-economic status (SES) families, suggestive of either misdiagnosis or overall under-diagnosis (Mandell et al., 2005; Valicenti-McDermott et al., 2012). Mandell et al. (2009) also report that, after controlling for race, gender, intelligence quotient (IQ), and birthweight, children of mothers with at least a college degree are 13% more likely to be diagnosed with ASD than mothers with high-school degrees and 44% more likely to be diagnosed than mothers with less-than-high-school education (Mandell et al., 2009). Kogan et al. (2009) showed similar findings from the 2007 National Survey of Children’s Health (NSCH). Earlier age of diagnosis has also been associated with more severe symptoms (Daniels and Mandell, 2014; Rosenberg et al., 2011; Wiggins et al., 2006) and greater maternal age (Frenette et al., 2013) (for an extended review, please see Daniels and Mandell, 2014). Here, we demonstrate the feasibility of studying social determinants of age of diagnosis by surveying parents of children with ASD as well as friends and family members referred by parents.
Diagnosis of ASD could be delayed beyond the time symptoms appear due to lack of knowledge about typical developmental trajectories or motivational factors such as unconscious ignoring of signs. The motivational factors that can impede early diagnosis are likely to be less pronounced for friends or family members other than parents. Grandparents are especially interesting as they are likely to have experience with, and hence insight into normal development trajectories, and may be in an important social position to advise parents. We therefore hypothesized that the presence of other family members, especially grandparents, is most likely to accelerate diagnosis.
We also investigate the effects of siblings and birth order, factors that have rarely been explored in prior research. Juneja et al. (2005) found that firstborns are diagnosed earlier, but another study with a larger sample observed the opposite (Rosenberg et al., 2011). We hypothesized that the presence or absence of siblings could have three different effects. First, siblings, especially older siblings, could serve as a reference point for the parents, making it easier, by establishing a contrast, to identify delays in, or unusual features of, a subsequent child’s development and behaviors. Since boys and girls are different, one could further expect that a same-sex sibling will serve as a better reference point than an opposite-sex sibling. Our hypothesis, therefore, is that, other things being equal, children with siblings, especially those who are older and of the same sex, will be diagnosed earlier. A second effect of siblings on age of diagnosis could operate via the amount of attention and interaction that each child receives; the more children in the household, the less attention each individual child is likely to receive. The prediction here is the opposite of the first, namely that the presence and number of siblings will delay the age of diagnosis. A third effect could result either from the lack of experience or from the risk aversion of new parents. An only child tends to get more attention and may attract more anxiety from parents than later children. Parents of an only child might be more cautious and alarmed by any sign that their child has a problem. While such behavior might lead to false alarms, in those cases where the child has ASD, we hypothesized that it is likely to result in earlier diagnosis.
Like earlier research examining the effects of social networks on health outcomes, such as obesity (Christakis and Fowler, 2007) and smoking (Christakis and Fowler, 2008), we examine the influence of families’ social interactions on the age of diagnosis of ASD. In these studies, the researchers first construct the social network of a large number of individuals by identifying family, friends, and other individuals with whom they are connected. Then, focusing on a specific condition (e.g. smoking), they try to identify clusters, groups of individuals who are directly connected and carry the same condition. The challenge, however, is to test whether the condition is transmitted from one person to the other through social influence as opposed to other factors that cause individuals with the same condition to be close to each other on the network (e.g. smokers like to be around smokers). This challenge, which amounts to distinguishing between correlation and causation, requires additional information, such as panel data, where through repeated surveys changes in the network over time can be observed and used for the analysis.
Of particular relevance to this research is the work of Liu et al. (2010) who specifically examine the role of the social network in the incidence of autism diagnosis. Using California data, they show that children living close to a child previously diagnosed with autism are themselves more likely to be diagnosed with autism and provide evidence that an underlying social influence mechanism, involving information diffusion, drives their results. Whereas these studies examined the impact of people with different characteristics on an individual’s social network, we focus on the specific interactions between parents and their immediate friends and family members who had exposure to the child who was eventually diagnosed with ASD. By directly surveying the parents as well as friends and family, we are able to learn more about the strength of the relationship as well as the nature of the interactions between the parties.
This pilot study uses novel methodology to examine the effects of family structure and family interactions to identify factors that may accelerate or delay diagnosis. We focus on whether the frequency of interaction with grandparents, birth order, and having siblings present in the household affect the age of diagnosis.
Methods
The Icahn School of Medicine at Mount Sinai Institutional Review Board approved this study.
This study consists of two online surveys. The first, targeting parents of children diagnosed with ASD, was completed by over 477 parents. A total of 569 parents started the survey and 477 reported the age of diagnosis—the central variable of our analysis. Most (86%) of parents’ surveys were completed by the child’s mother, 12% by the father, and 2% by both parents. The second survey targeted friends and family whose contact information was provided to us by parents who answered the first survey. A total of 196 “friends and family” surveys were completed.
In all, 80% of focal children in the survey were male. The overall median age of diagnosis was 33 months (mean = 40, SD = 25.9), and depended on clinical diagnosis (see Table 1), ranging from 30 months (for pervasive developmental disorder (PDD)) to 84 months (for Asperger syndrome (AS)). These ages are similar to those reported in other studies.
Sample characteristics.

ASD: autism spectrum disorder; PDD: pervasive developmental disorder; SD: standard deviation.
The ethnic breakdown is largely similar to that of the US population (Table 2, Panel A), with the exception of African-Americans, who are under-represented in our sample (4.4% compared with 14.9% in the United States).
Sample socio-economic characteristics compared with the US population.

HS: high school.
The parents in our sample are more highly educated than the general population (Table 2, Panel B); roughly two-thirds are college graduates, as compared with one-third of US adults. Other studies report a higher prevalence of ASD among children of more educated parents. Therefore, the educational level of our respondents might reflect these differences in prevalence and/or be the result of a self-selection of more educated parents to the survey. The sample’s income is also substantially higher than that of the typical US household (Table 2, Panel C), as is its level of urbanization (Table 2, Panel D).
Multiple regression analyses were conducted to estimate, simultaneously, the independent effects of various variables on the age of diagnosis. The dependent variable in our regressions is the age (in months) at which the child was diagnosed with ASD. We report the results using the age at first diagnosis. When we control for the specific diagnosis, however, we use the final diagnosis (37.6% of parents reported that the initial diagnosis was later revised). Since the only specific diagnosis that has a significant effect on the age of diagnosis is AS, rather than controlling for each diagnosis, we only used one dummy variable indicating an AS diagnosis.
Results
Presence of siblings
We first examined the effects of siblings on the time of diagnosis using regression models (Table 3). While the dependent variable in all six models is the same (age of diagnosis), the control variables vary by model as indicated in the first column. The socio-economic variables that were controlled for in some models (indicated in Table 3) are race, parents’ education, wealth, and urbanization. The specific effects of these variables on the age of diagnosis are presented in Appendix 1 (Table 8).
Summary of regression analysis for predicting the effects of siblings and birth order on age of diagnosis.
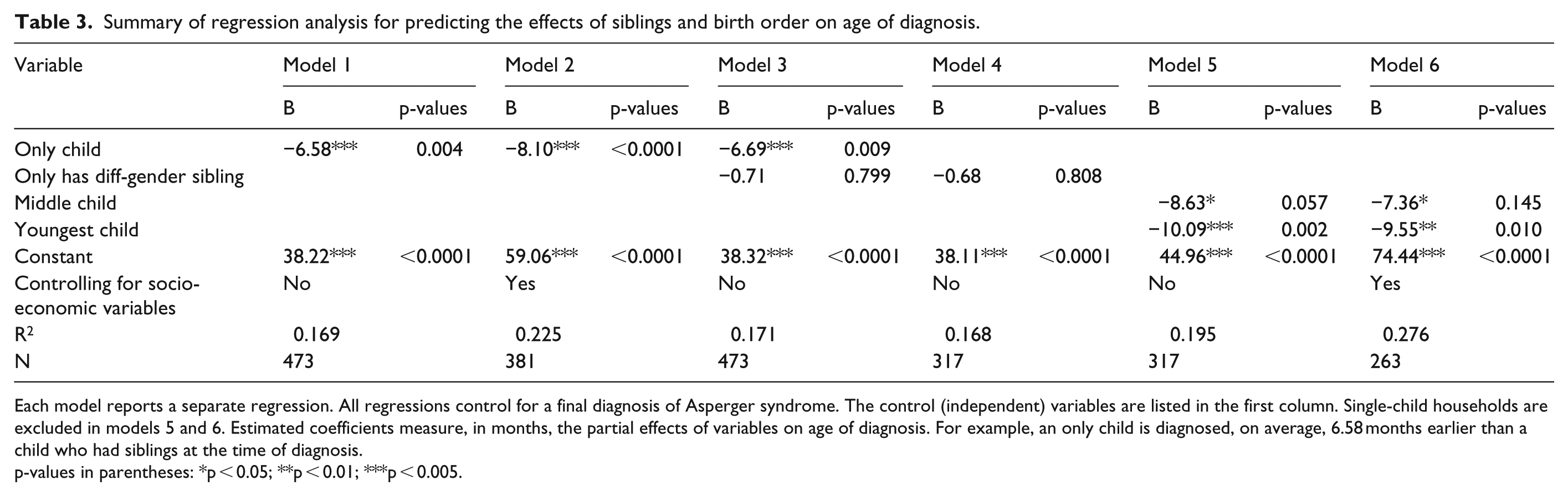
Each model reports a separate regression. All regressions control for a final diagnosis of Asperger syndrome. The control (independent) variables are listed in the first column. Single-child households are excluded in models 5 and 6. Estimated coefficients measure, in months, the partial effects of variables on age of diagnosis. For example, an only child is diagnosed, on average, 6.58 months earlier than a child who had siblings at the time of diagnosis.
p-values in parentheses: *p < 0.05; **p < 0.01; ***p < 0.005.
The first two models reported in Table 3 show that an only child is diagnosed, on average, 6–8 month earlier than children who had siblings present in the household around the time of their diagnosis (p < 0.01), consistent with the notion that new parents pay more attention to their only child and are especially cautious or risk averse due to lack of experience. When controlling for various socio-economic variables (model 2), the results are even stronger.
The results reported in models 3 and 4 do not support the prediction that the presence of a same-sex sibling accelerates age of diagnosis (p > 0.05).
The results reported in models 5 and 6 (regressions restricted to households in which the child has siblings) confirm that the birth order has a significant effect on the age of diagnosis. In households with more than one child, the presence of older siblings, especially being the youngest child, reduces age of diagnosis by 9.5–10 months, relative to children who have only younger siblings. This supports the idea that older children can serve as referents, helping parents to calibrate whether younger siblings are on-target developmentally.
Interactions with family members
Approximately 25% of parents reported that other people who had frequent contact with their child indicated a concern that the child “might have a serious condition” before they started suspecting it themselves (Table 4).
Did any of the people who had frequent contact with the child indicate any concern before you started suspecting?

Table 5 lists, in decreasing order, the relationship to the child of individuals who were the first to raise concerns, as reported by parents (note that parents could list more than one individual). The two most common categories of individuals are maternal grandmothers (27%) and teachers (24%). If one adds maternal and paternal grandmothers and grandfathers together, then 59% of respondents who reported that anyone had raised concerns before they were aware that their child had a problem identified grandparents as having done so.
Person who indicated concern before parents.

In the survey, we asked parents to report the frequency in which their child interacted with their grandparents. We observed that the likelihood that grandparents raise concerns is correlated with the frequency with which they interacted with the child (Figure 1).
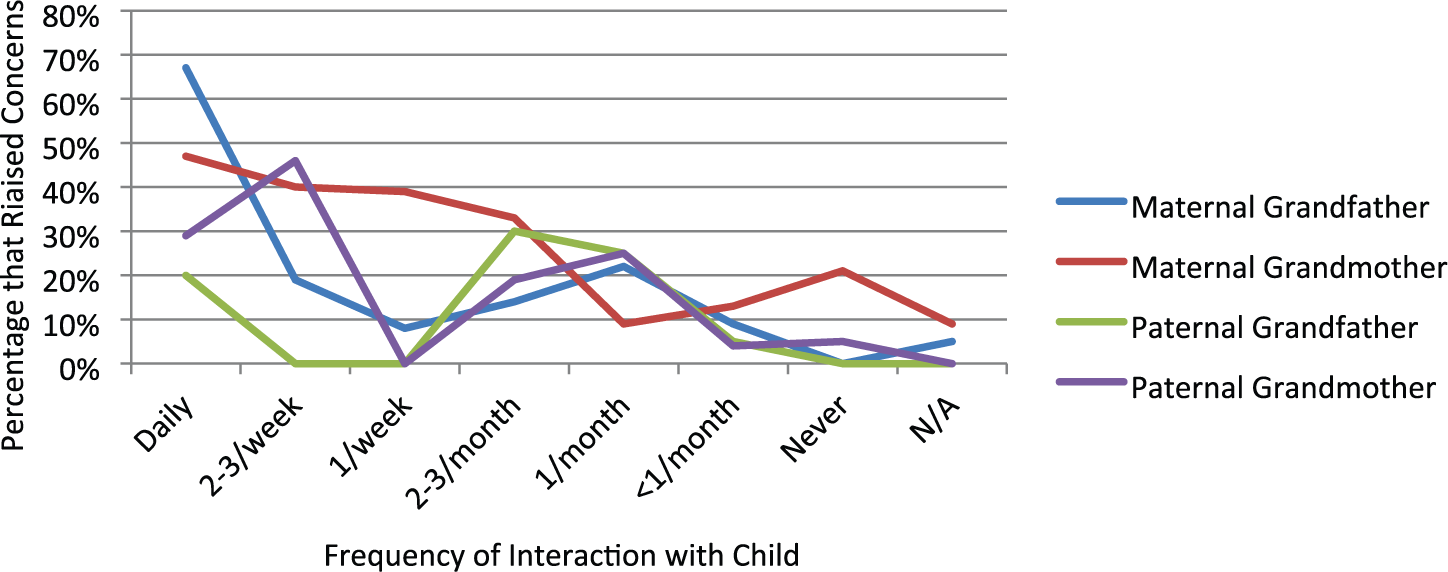
Percentage of grandparents raising concerns by level of interaction with child.
Table 6 reports the effects of frequent interaction with grandparents (at least once a week) on the age of diagnosis. We also test whether the effect is different between grandfathers and grandmothers. While the estimated coefficients are all negative (indicating that frequent interaction with grandparents accelerates the age of diagnosis), the effect is substantially stronger for grandmothers. While frequent interaction with a grandmother reduces the age of diagnosis by 5.18 months (p = 0.026), frequent interaction with a grandfather reduces the age of diagnosis by 3.78 months (p = 0.105). The results reported in model 3 further show that when both grandmother’s and grandfather’s interactions with the child are included in the regression, the grandmother’s interactions are the significant ones.
Summary of regression analysis for predicting the effect of interactions ϵ with grandparents on age of diagnosis.
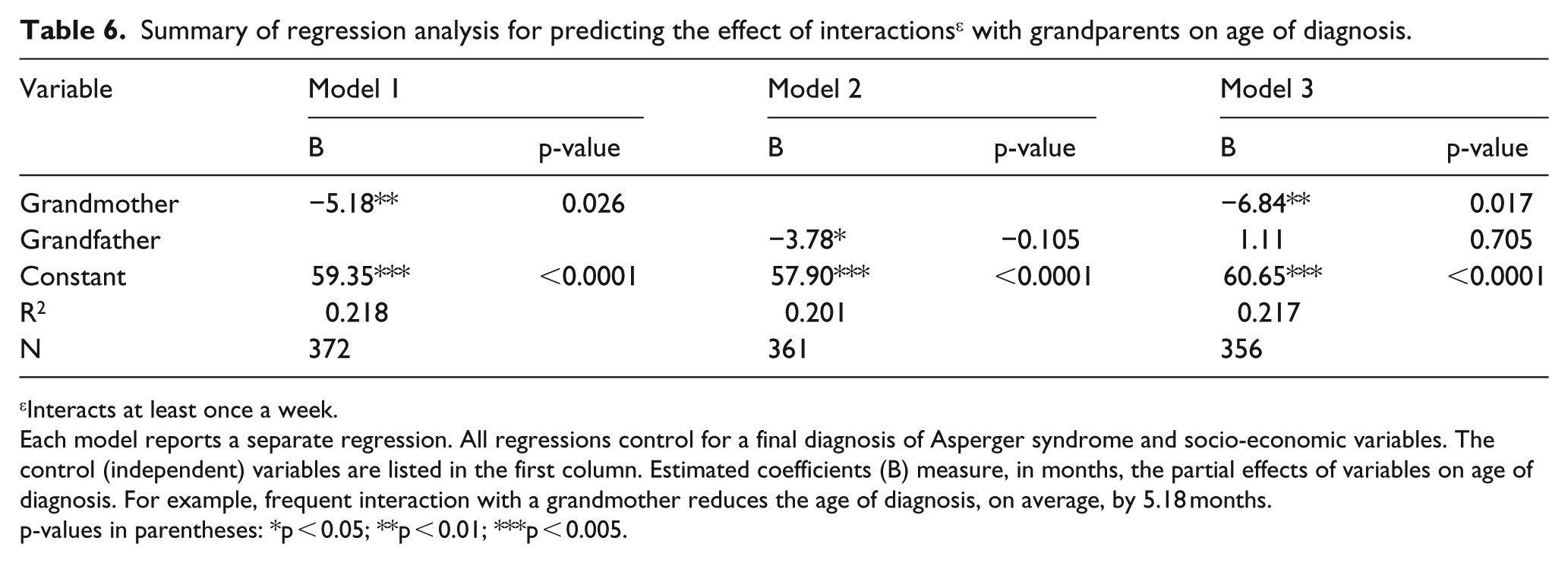
Interacts at least once a week.
Each model reports a separate regression. All regressions control for a final diagnosis of Asperger syndrome and socio-economic variables. The control (independent) variables are listed in the first column. Estimated coefficients (B) measure, in months, the partial effects of variables on age of diagnosis. For example, frequent interaction with a grandmother reduces the age of diagnosis, on average, by 5.18 months.
p-values in parentheses: *p < 0.05; **p < 0.01; ***p < 0.005.
Friends and family survey
At the end of our parents’ survey, we asked respondents to provide up to five contacts—for example, extended family, friends, neighbors, or caretakers—who saw their child frequently around the time of diagnosis. A total of 196 individuals completed this friends and family survey (Table 7). The bottom row reports the distribution of the different categories of individuals who took the survey. Over half of the respondents to this survey were either the child’s grandmother (28%) or aunt/uncle (26%). As expected, the respondents to this survey were individuals who were close to the child, 58% of whom saw the child at least once a week. The key finding from the perspective of our focus on age of diagnosis, however, is that 48% of respondents overall report that they suspected the child had a serious condition before they were aware that either parent was concerned. Remarkably however, among those who reported that they suspected that the child had a problem before the parents did, only 51% report that they expressed their concern to the parents, with a further 27% reporting that they “hinted concern” to either parent and 22% reporting that they did not express their concerns.
Friends and family survey—main findings.
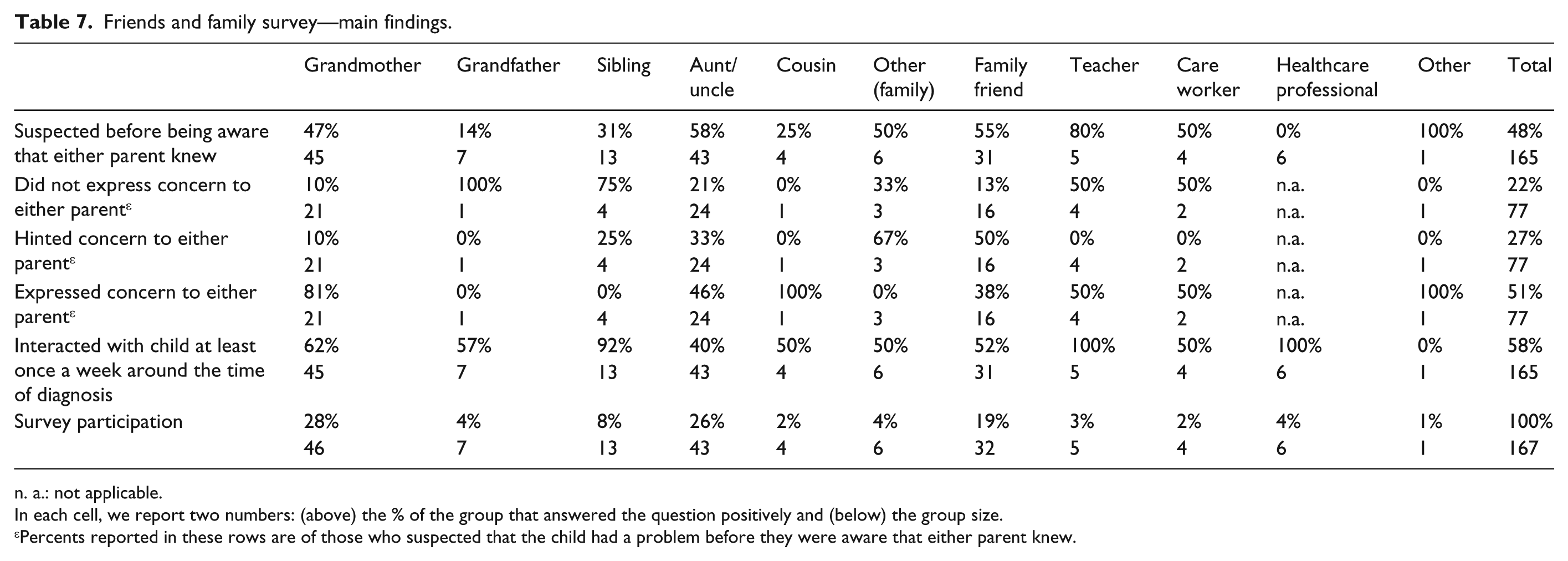
n. a.: not applicable.
In each cell, we report two numbers: (above) the % of the group that answered the question positively and (below) the group size.
Percents reported in these rows are of those who suspected that the child had a problem before they were aware that either parent knew.
In all, 17% of respondents were parents who did not complete the main survey; they are not included in the table.
Discussion
This study documents significant effects of family structure on the age of diagnosis of children with ASD. We provide a comprehensive look at the significant effects of siblings, birth order, family structure, and interactions with individuals outside of the nuclear family on time to diagnosis. Previous studies found that parents’ behavior affects the age of diagnosis (Daniels and Mandell, 2014; Perryman, 2009). A major finding from this study is, however, that individuals other than parents play, or can play, a key role in initial recognition that there is a problem. In all, 25% of parents reported that other people who had frequent contact with their child indicated a concern that the child “might have a serious condition” before they started suspecting. Likewise, almost 50% of family and friends indicated that they suspected that the child had a problem before they believed that parents did. Although not all informed the parents of their concerns, this does suggest that family and friends are a potential source of useful information, which might eventually help to reduce the age of diagnosis. Note, however, that the fact that someone else noticed before the parents that the child had a problem could be a reflection on the parents’ failure to pick up on signs, but it could also reflect the actual (or self-perceived) powers of observation of the individuals who were able to do so.
Especially prominent among individuals who raised concerns were maternal grandmothers. Our study found that the presence of a grandmother reduces the age of diagnosis, on average, by around 5 months when controlling for various socio-economic variables. Not surprisingly, the likelihood that grandparents raise concerns is strongly correlated with the frequency with which they interacted with the child.
In our data set, children with no siblings are diagnosed earlier than children who have siblings. An only child (at the time of diagnosis) is diagnosed, on average, 6–8 months earlier than children with siblings. When we focus only on children with siblings, however, diagnosis is earlier for children who have older siblings, especially for a youngest child. Interestingly, in our study, the gender of the sibling does not seem to have an effect.
At the outset of the study, we considered different potential effects that siblings might have on age of diagnosis. Our results provide support for two of the three hypotheses that the research tests. The finding that single children are diagnosed earlier than children with siblings supports the hypothesis that the greater attention such children receive, or the greater caution on the part of new parents, leads to earlier diagnosis. When children do have siblings, however, the finding that youngest children (those with only older siblings) are diagnosed around 10 months earlier supports the hypothesis that older siblings can serve as reference points. Having prior children may give parents the same insight that grandparents seem to have, making them better able to notice departures from normal developmental trajectories or to identify aberrant behavior on the part of the focal child.
Friends and family were asked whether they suspected that the child had a serious condition before they were aware that either parent was concerned and 48% responded affirmatively. This suggests that close family and friends have the potential to accelerate the age of diagnosis. While half of these individuals expressed concern to parents, the other half either did not raise any concern or just “hinted” at their concern. While few teachers, care workers, or healthcare professional completed the friends and family survey, it is of special concern that none of the respondents in these groups alerted parents to their concerns. This should be examined in larger studies targeting these groups to validate this finding and to understand the factors behind this apparent reluctance to communicate concerns.
Limitations
By estimating a single regression equation for the whole sample, we implicitly assume that the relationships between various variables and age of diagnosis are similar across people of different socio-economic backgrounds. Yet the idea that “status attainment” or “social capital” interacts with social networks (Lin, 1999) implies that the effects of variables such as “frequent interaction with grandparents” or birth order might depend on income, education and, more broadly, SES. To understand the role played by such variables, the standard approach would be to make them interact with the variables that we use in our analysis. Given the pilot nature of our study, however, the number of observations is too small to allow for such analyses. We do, however, control for the main effect of individual socio-economic characteristics in our regressions.
Another, related, limitation of our investigation is the non-representative nature of our sample, which limits our ability to generalize from our results to the broader population. The parents in our sample are more highly educated and wealthier than the average US adult population, and African-Americans are under-represented. In addition, our sample is concentrated in urban areas. Although this could reflect non-representativeness in our sample of respondents, it is also possible that the mismatch reflects, at least in part, differences in actual prevalence rates or rates of diagnosis.
Given the non-representative nature of our sample, our analysis is subject to two especially important selection issues. The first is that we do not have a representative sample of either children who have been diagnosed with autism or children who are at risk of being diagnosed with autism. Assembling either type of sample is, however, by no means a trivial task, especially given that autism diagnosis has changed considerably over time (Eyal et al., 2010). It must be acknowledged, however, that the parents who participate in an online survey are likely to be different from the general population of parents of children with autism.
The second source of selection issues is that all of the children in our sample have been diagnosed with autism; our analysis, therefore, focuses on variations in how early the children were diagnosed, given that they were diagnosed. Undoubtedly, there is a group of children with ASD who are never diagnosed. These children will not be part of our sample or in any study that, as is true of virtually all studies, focuses on individuals who are diagnosed. The bias introduced by the non-inclusion of never-diagnosed children is, however, likely to be conservative: To the extent that the factors we identify as associated with late diagnosis are also associated with not being diagnosed, our results will understate their importance.
Conclusion
The presence of grandparents, especially grandmother, significantly accelerates age of diagnosis, and the number of siblings and birth order also has significant effects. There is also a strong indication that other individuals close to the child often suspect that the child has a problem before parents do, but many do not express, or only hint at, their concerns to parents. Taken together, these findings suggest that there are opportunities for readily achieving earlier diagnoses, tapping into the wisdom and information of family, friends, and caregivers with exposure to children in a family.
Supplemental Material
AUT679632_Lay_Abstract – Supplemental material for Grandma knows best: Family structure and age of diagnosis of autism spectrum disorder
Supplemental material, AUT679632_Lay_Abstract for Grandma knows best: Family structure and age of diagnosis of autism spectrum disorder by Nachum Sicherman, George Loewenstein, Teresa Tavassoli and Joseph D Buxbaum in Autism
Footnotes
Appendix 1
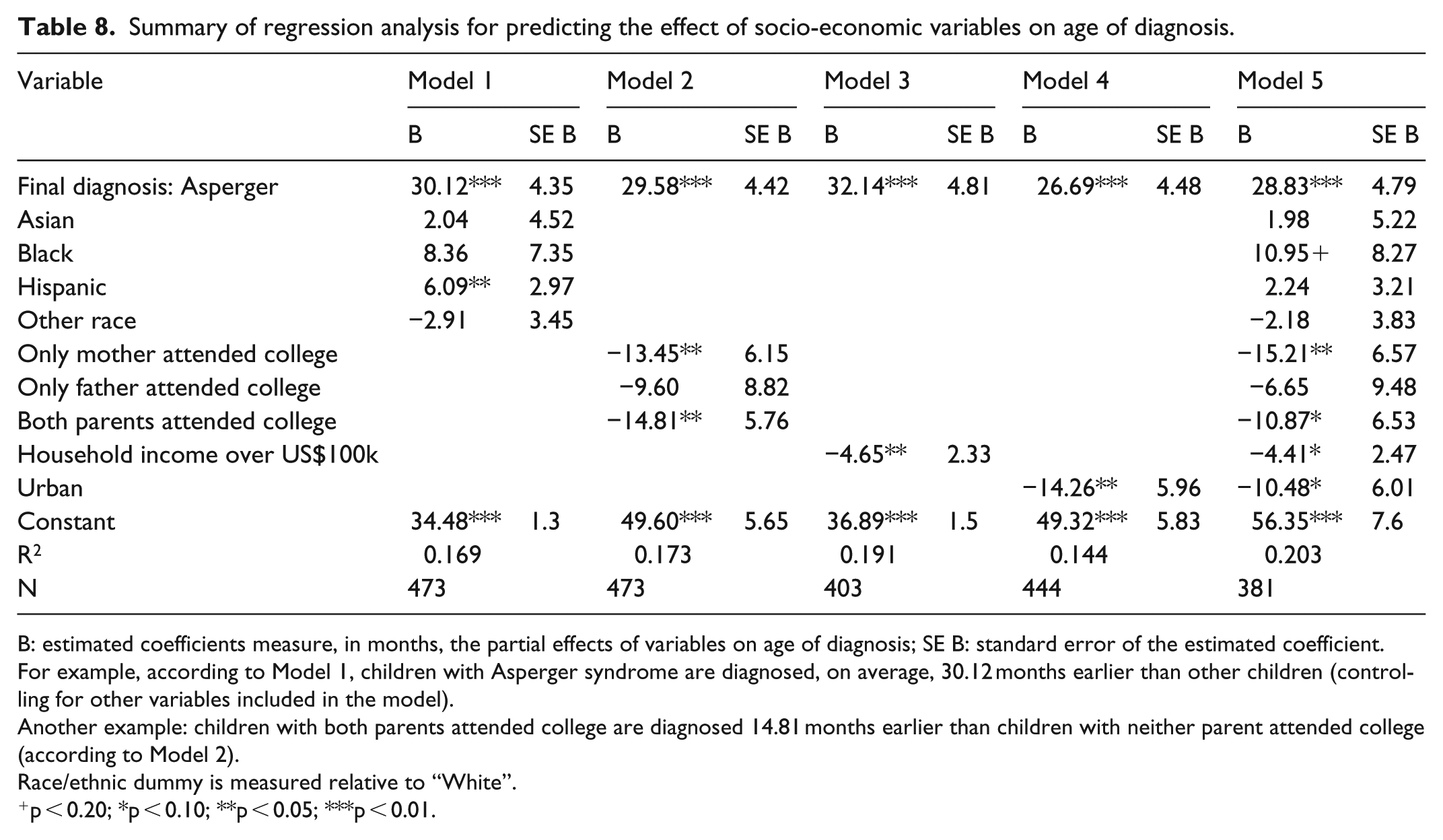
Summary of regression analysis for predicting the effect of socio-economic variables on age of diagnosis.
| Variable | Model 1 |
Model 2 |
Model 3 |
Model 4 |
Model 5 |
|||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | SE B | B | SE B | B | SE B | B | SE B | B | SE B | |
| Final diagnosis: Asperger | 30.12*** | 4.35 | 29.58*** | 4.42 | 32.14*** | 4.81 | 26.69*** | 4.48 | 28.83*** | 4.79 |
| Asian | 2.04 | 4.52 | 1.98 | 5.22 | ||||||
| Black | 8.36 | 7.35 | 10.95+ | 8.27 | ||||||
| Hispanic | 6.09** | 2.97 | 2.24 | 3.21 | ||||||
| Other race | −2.91 | 3.45 | −2.18 | 3.83 | ||||||
| Only mother attended college | −13.45** | 6.15 | −15.21** | 6.57 | ||||||
| Only father attended college | −9.60 | 8.82 | −6.65 | 9.48 | ||||||
| Both parents attended college | −14.81** | 5.76 | −10.87* | 6.53 | ||||||
| Household income over US$100k | −4.65** | 2.33 | −4.41* | 2.47 | ||||||
| Urban | −14.26** | 5.96 | −10.48* | 6.01 | ||||||
| Constant | 34.48*** | 1.3 | 49.60*** | 5.65 | 36.89*** | 1.5 | 49.32*** | 5.83 | 56.35*** | 7.6 |
| R2 | 0.169 | 0.173 | 0.191 | 0.144 | 0.203 | |||||
| N | 473 | 473 | 403 | 444 | 381 | |||||
B: estimated coefficients measure, in months, the partial effects of variables on age of diagnosis; SE B: standard error of the estimated coefficient.
For example, according to Model 1, children with Asperger syndrome are diagnosed, on average, 30.12 months earlier than other children (controlling for other variables included in the model).
Another example: children with both parents attended college are diagnosed 14.81 months earlier than children with neither parent attended college (according to Model 2).
Race/ethnic dummy is measured relative to “White”.
p < 0.20; *p < 0.10; **p < 0.05; ***p < 0.01.
Acknowledgements
We thank Abraham Bae, Jimmy Charite, Stacie Lurie, and Julia George-Jones for their superb research assistance, and Alison Singer of the Autism Science Foundation for early discussions of the study and for alerting families about the study. We thank all participants for taking part in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this research was provided by a generous grant from the Organization for Autism Research (OAR). T.T. and J.D.B. received support from the Seaver Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.