
Abstract
Much research has documented the elevated levels of stress experienced by families of autistic children. Yet remarkably little research has examined the types of support that these families perceive to be beneficial to their lives. This study, co-produced by researchers and school-based professionals, sought to establish these families’ support needs from their own perspectives. In total, 139 parents of autistic children with additional intellectual disabilities and limited spoken communication, all attending an inner-city London school, participated in an initial survey examining parental wellbeing, self-efficacy and the extent to which they felt supported. Semi-structured interviews were conducted with a subgroup of parents (n = 17), some of whom reported in the survey that they felt unsupported, in order to gain their in-depth perspectives. The results from both the survey and the interviews suggested that existing support (particularly from formal support services) was not meeting parents’ needs, which ultimately made them feel isolated and alienated. Parents who were interviewed called for service provision that adopted a relational, family-centred approach – one that understands the specific needs of the whole family, builds a close working relationship with them and ensures that they are supported at times when the parents and families feel they need it most.
Parenting a child on the autism spectrum can be a hugely rewarding experience (McConnell et al., 2015; Phelps et al., 2009). It can also be stressful for a variety of reasons, with parents often reporting stress levels that exceed those among parents of typically developing children, or those with other developmental conditions (Craig et al., 2016; Dabrowska and Pisula, 2010; Estes et al., 2009; Hartley et al., 2012; Hayes and Watson, 2013). Current research on stress in parents of autistic 1 children has moved away, however, from investigating if they experience higher levels of stress than parents of children with other developmental conditions to why this is the case and, importantly, what factors can help mitigate it (Hayes and Watson, 2013).
Child-level factors, such as symptom severity, adaptive functioning (Ekas and Whitman, 2010; Hall and Graff, 2011; Hayes and Watson, 2013) and behaviour that challenges (McStay et al., 2014), have been shown to impact upon maternal stress and wellbeing. Parents’ characteristics such as personality style (Ingersoll and Hambrick, 2011), sense of optimism (Faso et al., 2013; Lee, 2009) and coping style (Hall and Graff, 2011) have also been identified as influencing the stress experienced by parents. Comparatively less research, however, has focused on the role that external support, including social, professional and respite support, plays in parents’ wellbeing (Bromley et al., 2004; Karst and Van Hecke, 2012; Khanna et al., 2011; Vasilopoulou and Nisbet, 2016).
Existing research shows that parents of autistic children perceive the informal social support received from other parents, both offline and online (Huws et al., 2001; Mackintosh et al., 2005; Mandell and Salzer, 2007; Wynter et al., 2015), as highly beneficial. Indeed, limited social support in such families has been linked with decreased positive mood (Pottie et al., 2009) and parenting efficacy (Weiss, 2002), as well as increased stress (Barker et al., 2011; Ekas and Whitman, 2010). The extent to which formal professional support is available, valued – and indeed, how much it helps – appears to be highly variable (Edwards et al., 2016; Preece, 2014), with parents reporting considerable difficulties accessing such support (Altiere and Von Kluge, 2009; Ludlow et al., 2011; Meirsschaut et al., 2010; Preece, 2014; Woodgate et al., 2008). Respite support (Chan and Sigafoos, 2001; Harper et al., 2013), also referred to as ‘short breaks’ in the United Kingdom (Preece and Jordan, 2007), is also valued by parents but has been suggested to be insufficient to meet the growing needs of autistic children and their families (Carlin and Cramer, 2007).
The absence of external support can have significant implications for parents’ wellbeing. The lack of support to help manage stress can negatively impact upon parents’ self-efficacy (Kuhn and Carter, 2006), decreasing parents’ perceived ability to cope, increasing the impact of stressors and potentially leading to an increased sense of isolation and further reduction in their experience of social support (Donenberg and Baker, 1993; Schaaf et al., 2011). This in effect creates a cyclical process that potentially perpetuates higher perceived levels of stress and poorer wellbeing. It is therefore vital to examine parents’ perspectives on the support that they receive and the perceived challenges in accessing such support in order to modify support systems to improve parental and family wellbeing.
This study investigated these issues by focusing on the support needs of families of autistic children with additional intellectual disabilities and limited spoken communication, all of whom attend a government funded, local special school in inner-city London. The school has been rated by the UK Government’s Office for Standards in Education, Children’s Services and Skills (OFSTED) as ‘outstanding’, that is, ‘highly effective in delivering outcomes that provide exceptionally well for all its pupils’ needs’. Nevertheless, one of the school’s priorities has been to engage more with parents and carers, particularly those that are seldom heard, in regard to their children’s learning – a commitment that formed the impetus for this research. This research is therefore unique in three ways. First, it is co-produced by school professionals and by autism researchers to help the school better understand families’ needs. School professionals were involved as collaborators during all stages of the research process and, in particular, led on the implementation of the research and interpretation of the findings. This collaboration is in response to calls for greater involvement of the autism community in the research that affects them (Pellicano et al., 2014). Second, it placed families at the heart of decision-making, directly eliciting families’ views and perspectives of the services and supports they would like to receive – rather than the services and supports professionals think parents should like to receive. Third, we elicited the perceptions and experiences of an ethnically, culturally and socio-economically diverse group of families (see below for details), whose views are rarely heard in autism research, especially in the United Kingdom (Corbett and Perapa, 2007; Slade, 2014).
Specifically, we sought to elucidate why some families feel supported (and others do not), whom they turn to for support and what types of support they currently receive or would like to receive in the future. To address these aims, we conducted an initial, brief survey with 139 parents whose autistic children attended the school to gain an overall sense of the support needs of these families and, critically, to inform the design of semi-structured interviews. In all, 17 parents were then interviewed in depth about their views on the support they currently receive, if any, and the exact nature of the services they desired.
Method
Participants
All participants were recruited from a government funded, local special school in inner-city London, catering for just over 180 pupils (79% boys) ranging in age from 4 to 19 years. The majority of pupils (around 80%) have a diagnosis of autism spectrum disorder. Of these pupils, approximately, 80% have severe intellectual disability; approximately, 17% have profound intellectual disability and approximately, 3% have a moderate intellectual disability with an additional co-occurring condition. All have communication difficulties, and a high proportion present with behaviour that challenges and complex needs. To attend the school, pupils must have received a Statement of Special Educational Need (SEN) or, more recently, an Education, Health and Care Plan (UK Department for Education, 2014), a legal document that details the child’s needs and services that the local educational authority has a duty to provide.
The borough in which the school is located has the second highest rate of child poverty in England, with almost half of all children in the borough living in poverty. In the school, over 65% of pupils are eligible for the UK Government’s pupil premium funding for families on low incomes – a figure that far exceeds the national average of 29.8% (Department for Education and Education Funding Agency, 2016). Furthermore, Black, Asian and minority ethnic communities make up a significant proportion of the borough’s population, and the ethnic backgrounds of the pupils attending the school reflect this diversity.
Survey
There were 139 (108 females) survey respondents: 132 were the child’s biological parent, 1 was the adoptive parent, 2 were foster parents and 4 were grandparents. All respondents had autistic children who ranged in age from 4 years 4 months to 18 years 8 months (47% of the sample attended the primary part of the school; 18% females). All children had received an independent clinical diagnosis of an autism spectrum condition according to the International Classification of Mental and Behavioural Disorders, 10th edition (ICD-10; World Health Organization, 1993) or the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) criteria and were in receipt of a Statement of SEN, which specified autism as their primary need. Almost all children had an additional intellectual disability.
Just over half (54%) of the survey respondents lived in a two-parent household. In all, 22 of the 139 respondents (15%) reported having one child only, 44 had two children (31%), 41 had three children (29%), 21 had 4 children (15%) and 11 had more than 4 children (8%). Respondents also reported how many children in their family had an SEN or disability. Of the 110 parents or carers who responded to this question, 20 reported having two children with SEN and one parent reported having four children with SEN in their family. Of the 106 families who chose to answer the question on ethnicity, 30 reported to be of White background, 55 of Black background, 11 of Asian background, 5 of mixed background and 5 of another ethnic group.
Semi-structured interviews
We randomly selected parents from two subgroups, including those who reported feeling supported (n = 16 from a total sample of 109 families) and those feeling unsupported (n = 16 from a total sample of 32 families) and invited them to take part in an in-depth semi-structured interview. This procedure was designed to ensure that we elicited a range of responses and experiences about the challenges they faced and the support needed to address them, including from potentially seldom-heard families. In all, 17 parents (15 mothers, including one foster mother and two fathers) took part in an interview (seven from the ‘feeling unsupported’ group). Despite contacting the remaining parents on multiple occasions, scheduling a meeting proved extremely difficult, even with parents who were initially keen to take part.
The participating 17 parents had 18 children (16 boys, 2 of whom were brothers and 2 girls) who ranged in age from 5 years 6 months to 17 years 7 months (M = 10 years, 8 months; standard deviation (SD) = 3;7) (11 attended the primary part of the school). Most children were of Black background (n = 11; White background: n = 4; Asian background: n = 2). The school uses the Social Communication, Emotional Regulation and Transactional Support (SCERTS®) framework (Prizant et al., 2006), which provides specific guidelines for helping foster children’s social communication, with the necessary support. According to the SCERTS framework, 5 of the 18 children were classified to be within the ‘social partner’ (pre-symbolic) stage, 6 within the ‘language partner’ (emerging language) stage and 7 within the ‘conversational partner’ stage. Of these 17 children, seven were accessing the UK’s National Curriculum (albeit well below age-expected levels) and the remaining children were accessing P scales. 2 The non-participating children (n = 15) were of similar ethnic background but were generally older (M age = 14 years 3 months), with the majority (n = 9) in secondary school, and at a lower developmental stage within the SCERTS framework (social partner stage: n = 9; language partner stage: n = 3; conversational partner stage: n = 3).
Procedure
Survey
All respondents with a child(ren) attending the school were invited to take part in a brief survey. They were told that the school was interested to know how they could best support parents/carers (henceforth referred to as parents) and children and the type of things that might make a difference to their lives. The brief survey asked a series of background questions about parents (e.g. gender, age group) and their family (e.g. number of children, number of parents in household). Next, they received two questions about their general health and mental wellbeing, which they rated on a 5-point scale ranging from ‘poor’ (score of ‘1’) to ‘excellent’ (score of ‘5’). These were followed by a 5-item parental self-efficacy scale (Child Outcomes Research Consortium (CORC), 2016) in which parents were asked to rate the extent to which they agree with a series of statements about their child (Table 1) from ‘strongly disagree’ (score of ‘1’) to ‘strongly agree’ (score of ‘5’). Finally, parents were asked three focused questions on the degree and nature of their support, including a final open question asking them to identify the ‘one thing that would make a difference to you and your child’s life’. The survey took approximately 5–10 min to complete and was delivered by school professionals between April and July 2014 via SurveyMonkey.
Parents’ mean responses on the five items and total score on the brief self-efficacy scale (CORC, 2016).
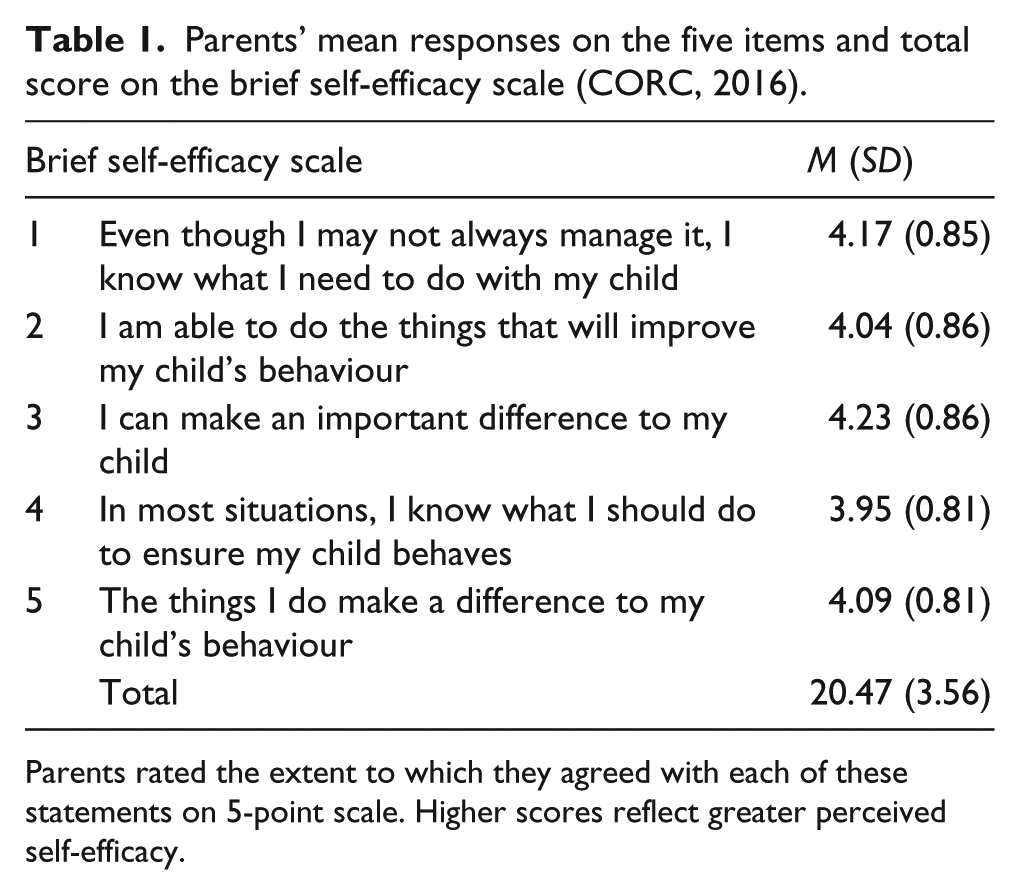
Parents rated the extent to which they agreed with each of these statements on 5-point scale. Higher scores reflect greater perceived self-efficacy.
Semi-structured interviews
Interviews were conducted face-to-face (by J.G.) at a place convenient to the family – either at their home (n = 12) or at school (n = 5). Although interpreters were made available for parents whose first language was not English, no interpreters were requested. We asked questions about parents’ perceptions of the specific abilities and needs of their child, their child’s wellbeing and their own wellbeing (physical and emotional), their experiences of support received both at school and at home, and the types of support they have benefited from and/or feel that they would benefit from in the future. The length of interviews ranged from 15 to 39 min (M = 25 min).
All interviews were recorded and transcribed verbatim with the exception of interviews with two parents, who did not agree to be recorded. In these cases, detailed notes were taken throughout the interview. The resulting transcripts were analysed using thematic analysis (Braun and Clarke, 2006). We adopted an inductive approach, providing descriptive overviews of the key features of the semantic content of data within an essentialist framework. Two authors (J.G. and E.P.) independently familiarised themselves with the data, discussed preliminary themes and generated a list of provisional codes. The authors met several times to review the results, resolve discrepancies and decide on the final themes and subthemes.
Ethical approval for this study was granted by the Faculty’s Research Ethics Committee at UCL Institute of Education, University College London (FPS 674). All participants gave informed consent prior to participation.
Results
Survey
Overall status of health and wellbeing
When parents were asked to rate their general health, the most common score (mode) was ‘good’ (M score = 3.59; SD = .99). More than half of parents rated their general health as ‘very good’ or ‘excellent’ (n = 72; 52%) while only 16 of the 139 (12%) rated their health as either ‘fair’ (n = 13) or ‘poor’ (n = 3). A similar pattern was found for ratings of mental or emotional health, in which the most common score was ‘good’ (M = 3.69; SD = .98). In all, 78 parents (66%) rated their mental or emotional health as ‘very good’ or ‘excellent’, while 15 (11%) rated it as either ‘fair’ or ‘poor’. The parents who reported their general health to be ‘fair’ or ‘poor’ were not necessarily the same parents who reported their mental or emotional health as ‘fair’ or ‘poor’. For example, of the three parents who reported their general health to be ‘poor’, one reported their mental/emotional health to be ‘fair’, one as ‘good’ and one as ‘very good’.
Perceived self-efficacy
Table 1 reports the parents’ mean scores on the individual items on the brief parental self-efficacy scale (CORC, 2016) and on total scores (created by summing across the five items). Higher scores indicate higher perceived self-efficacy. The scale showed excellent reliability (Cronbach’s alpha = 0.91). As shown in Table 1, the mean scores were reasonably high. In fact, the distribution for total self-efficacy scores was negatively skewed (i.e. more parents agreeing with these statements, on average) suggesting that these parents generally perceive themselves as capable and effective in their parenting role.
Correlational analyses revealed significant relationships between parents’ perceived self-efficacy and their perceptions of their own health. Parents who reported lower degrees of perceived self-efficacy also rated themselves as having significantly poorer health, r(138) = 0.23, p = 0.006, and poorer mental or emotional health, r(138) = 0.24, p = 0.005.
External support
With regard to social support, 31 of the 136 parents who responded to this question (23%) reported that they did not feel they had anyone to turn to for support. These parents did not differ, however, from those who reported they did have someone to turn to for day-to-day help and support in terms of general health (supported: M = 3.66, SD = 0.95; not supported: M = 3.32, SD = 1.11), t(134) = 1.66, p = 0.10, mental health (supported: M = 3.75, SD = 0.94; not supported: M = 3.48, SD = 1.06), t(134) = 1.36, p = 0.18 or perceived parental self-efficacy (supported: M = 20.62, SD = 3.76; not supported: M = 19.97, SD = 2.90), t(134) = 0.89, p = 0.38.
When parents were asked what types of support they receive when they faced difficulties in their family, they reported receiving a wide variety of social supports (Figure 1). The most common supports were reported to come from partners (n = 56; 40%), relatives (n = 67; 48%) and friends (n = 59, 42%). We were particularly interested in parents who felt unsupported compared to those who felt supported. Examination of Figure 1 suggests that parents who do not feel supported also reported not receiving as much support from partners, other parents of autistic children, local support groups, school staff and other professionals.
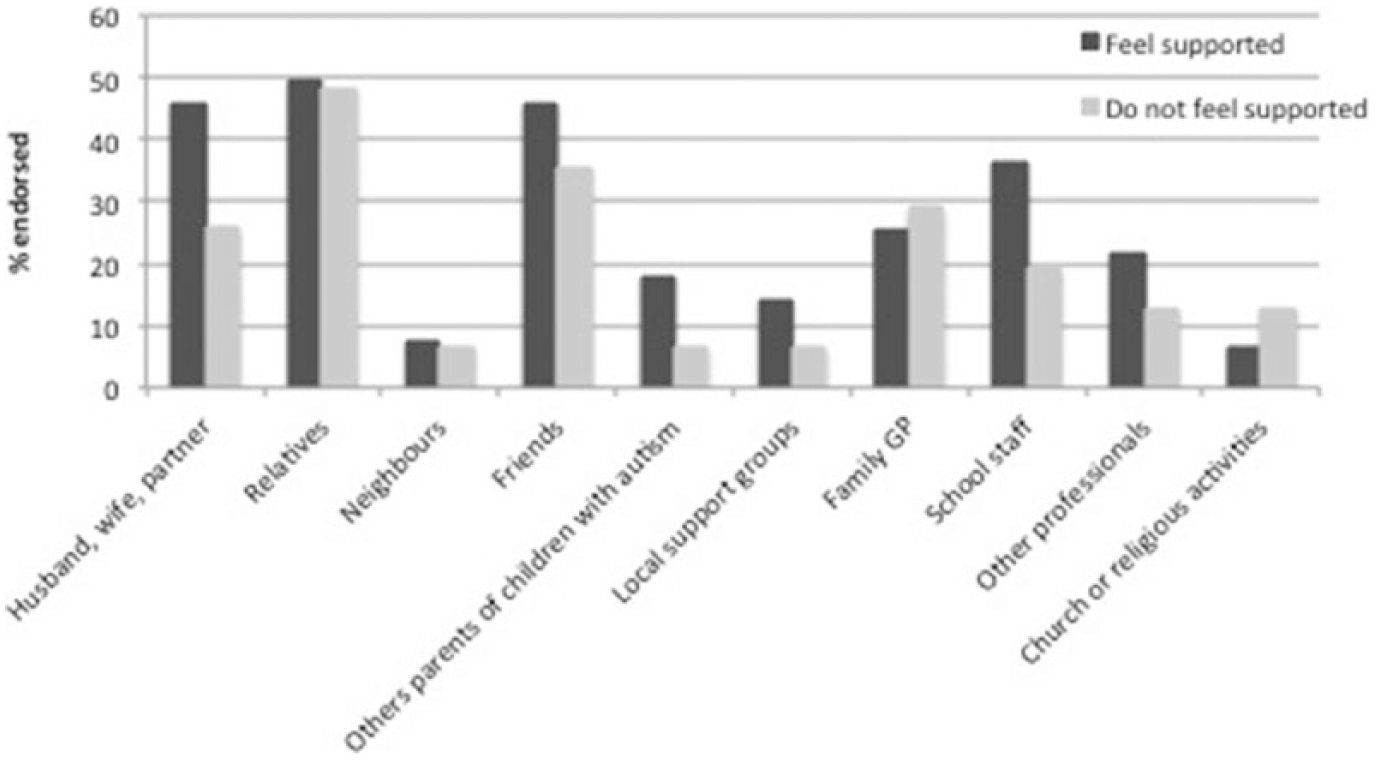
Survey: graph showing the percentage of parents endorsing each type of social support according to perceived support.
When we asked parents about the types of social and other support that would make the most difference to them or their child’s lives, parents again endorsed a range of options. The three most endorsed types of support were as follows: (1) a better understanding of who is working with their child (48%); (2) being in touch with other parents who are or have been in a similar situation (37%) and (3) more time by themselves to ‘recharge their batteries’ (36%). Figure 2 shows the type of support that parents would like to receive as a function of whether they felt supported on a day-to-day basis. A greater percentage of parents who felt unsupported wanted more communication with school staff and more time to spend with their other children than parents who felt supported. Fewer unsupported parents wanted workshops at schools or one-to-one guidance from professionals than supported parents.
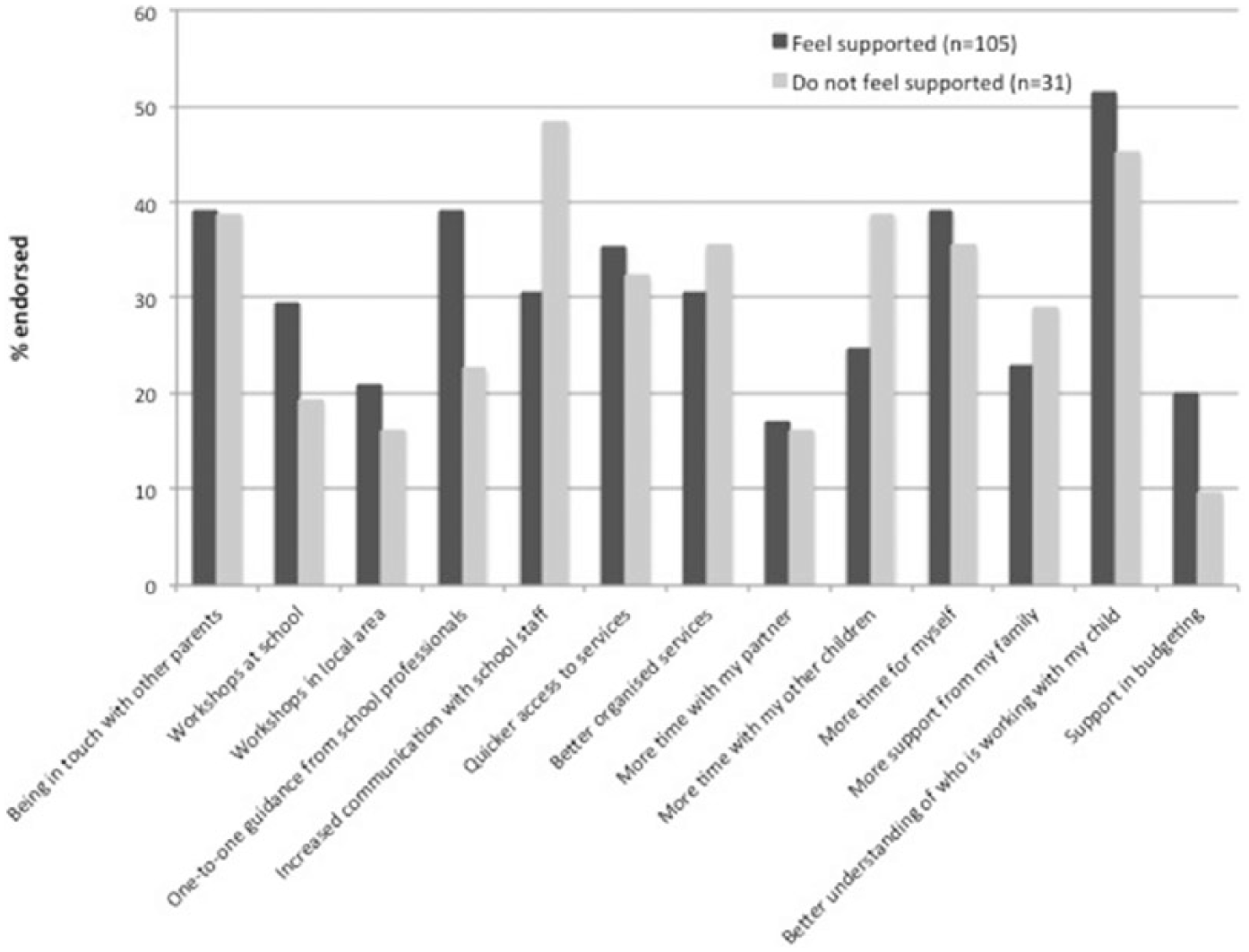
Survey: graph showing the percentage of parents endorsing those supports they felt would make a difference to them or their child’s lives according to whether they reported feeling supported or unsupported.
Finally, parents were asked to state which one thing would improve them and their child’s life. For parents who felt unsupported, their brief qualitative responses focused on their child’s communication (e.g. ‘understanding him when he’s trying to tell me something’), behaviour (e.g. ‘more help to manage him’) and independence, respite, and information on ‘advice around supporting my child’. These types of support were also identified by parents who felt supported, but these parents also felt that more ‘tolerance’ and ‘understanding’ within the community, ‘help with housing issues’, including more space at home, and activities and out-of-school (weekend and holidays) support for their child would improve them and their child’s lives.
Semi-structured interviews
We identified four main themes in parents’ interview data, including (1) everyday challenges of living with autism, (2) sense of isolation and alienation, (3) service providers need to adopt a family-centred approach and (4) desire for a sense of community and togetherness (corresponding subthemes are shown in italics).
Theme 1: everyday challenges of living with autism
All parents mentioned specific needs and characteristics of their autistic child/ren, which they felt were particularly difficult to cope with, including expressive language, diet, self-care skills and sleep. These areas were also the ones in which parents felt their children needed to make the most progress. Parents spoke of how their children’s expressive language difficulties were disempowering (‘she can’t say what she needs’) and were a ‘frustrating situation’ not only for parents but also for children, who ‘feel people don’t understand them’ and could show behaviour that challenges as a result. Difficulties with diet was another area highlighted by many parents (‘there’s lots of things, with taking food, giving food’), with food refusal or a restricted diet a particular concern as sometimes this meant that ‘[child] goes without food’, which they found distressing. Many parents, predominantly of primary-aged children, highlighted self-care skills as a specific area of difficulty, including ‘a lot of problem with toilet training’ and brushing teeth. Finally, sleep was raised as a significant area of difficulty, with children ‘waking up a lot at night time’ and inconsistent sleep routines for their child (e.g. ‘maybe she sleep late, very late or if she sleep early she wake up in the middle of the night’). Parents’ concerns meant that they needed to ‘lock the door’ for fear that their child could leave the house during the night, a significant worry for some parents; one father pointed out his son had ‘escaped twice’. An additional concern cited by parents of older children was the transition from secondary school: ‘the challenge of the future because [their child]’s due to leave the school’. They felt that the move to adulthood was ‘a big unknown’, especially since children had often been in the same setting for the entire school career.
Parents felt that these challenges meant that they did not feel part of the community. They reported being anxious ‘about going out in public’, ‘always worried about what’s going to happen’ and how others might react to them and their child. These worries meant that families were often missing out on activities that gave them a sense of community, such as going to church (‘it’s difficult, even Sunday they [extended family] went to church, we couldn’t go’), visiting friends, which was ‘very upsetting, so very hard’, or even enjoying outings together as a family (‘we don’t go places together, we don’t go on holidays’). Parents also noted practical constraints, particularly around transport, which limited their opportunities to take part in community activities. While there might be an activity or service available for their child to access, ‘where there’s no transport [it] is a bit tricky’ to use this service, with other parents echoing this problem: ‘we don’t drive so that was a bit difficult’.
Consequently, parents highlighted the need for respite, to be able to ‘recharge your batteries’ or take care of everyday ‘things what I need, like dentists and appointments’. This was particularly pronounced during school holiday time, with parents noting ‘that’s where we get stuck, that’s where we need a little bit of support’. They felt that support during the school terms, like after-school clubs, was beneficial because it allowed them to ‘have time to myself’ and ‘the time to do all the things, the cooking and cleaning’. But parents wished there was more support available, including ‘a larger variety of play schemes’ in the holidays as this time, especially if they were also working, was ‘just too hard, sometimes we need a break’. They also wanted respite that was flexible including, for example, support available during the evenings so that parents ‘could go out’ every once in a while.
Theme 2: sense of isolation and alienation
Parents raised several factors that they felt caused them to feel ‘very isolated’ and alienated. One of these was a lack of understanding of autism. They felt that the general public ‘don’t understand what autistic means, they are not aware’ and ‘are very quick to judge’. One parent spoke of how they ‘used to get parents approaching me in the street’ regarding their child’s behaviour, leaving parents having often ‘to explain myself’. Indeed, for some, again particularly those who had previously reported feeling unsupported, this meant withdrawing from their community or being ignored ‘because they come from a community where when people know that you have a child with a disability they ostracise you’. Those in positions of authority were also perceived to have limited knowledge of autism. Some felt that there could have been better support for their child in mainstream education settings but, instead, they ‘felt lonely and pushed aside, [the school] did not do anything or know anything’. Similarly, when parents spoke to the local educational authority about their ‘child with special needs, autism, they don’t seem to understand’, they were seen as adopting a one-size-fits-all approach. One parent noted that, when applying for support, the council insisted that her pre-verbal son should undertake a verbal interview before they would process her application for support: ‘I think when they first had the form they were, “I must tick this box, I must do this”’.
Parents also felt that limited collaboration with the school had a negative impact upon their ability to manage day to day, and on their wellbeing. They spoke of the lack of home–school communication, which meant that ‘we are not aware much what they are doing in school, we can’t continue at home’. Others felt that ‘there should be more contact with parents’ from the school and more ‘opportunities for families to work with professionals’. The lack of this support led to a sense of alienation: ‘I don’t really feel connected to [the school], I don’t really understand how things work there’. Sometimes, engaging with professionals was perceived to just be ‘too hard’, which meant that they were missing out on learning key skills for supporting their child: ‘it’s not just your child being educated [there], it’s you as well’.
Finally, parents repeatedly lamented the adversarial nature of the system, the fact that ‘as a parent you have to battle for everything’ and that you have to ‘keep pressing, keep pressuring them and keep pushing them and ringing them’. Many parents noted the stress that this caused, ‘the constant fighting, knocking away on the doors for support, support that is supposed to be there but you are not getting it and then you have to keep knocking and knocking’ and the feelings of helplessness, particularly from parents who felt unsupported, that they ‘can do nothing really’ as ‘the process is too long, too hard’ and they ‘don’t really know what happens’. They also reported feeling guilty for not having the time or resources to keep ‘fighting’ or ‘asking for enough help’, not doing everything they could to ensure their child received support. Parents felt that accessing support often ‘comes down to who is more able’ or those who ‘shouts loudest gets heard’. Those parents who ‘don’t really deal well with paper and things that come through the post’ felt the most alienated from support, with some stating they ‘don’t even know who to turn to’. They also reported being let down by the system. For example, one family who had received a visit from a social worker a year before pointed out that they ‘haven’t heard anything from [them] again’. Another parent reported being told that they ‘could get one hour [of home support] a day, that would help, but I am still waiting’. Some went so far as to say that the nature of the bureaucracy felt ‘like there’s a sort of investment in separating people’ with no ‘interactive quality’ to the way support is provided.
Theme 3: service providers need to adopt a family-centred approach
Parents felt that existing support does not fit with their lives. Many parents spoke of work commitments impacting on their ability to access weekday, daytime support. They were ‘very busy working’, ‘so busy [they] don’t really have the time’, which meant that they were unable to access parents groups or courses: ‘because I work I don’t really get to go there very often’. Parents noted that more could be done ‘in the evenings every now and then’ and to provide ‘help during the weekends’. Parents, particularly those who had reported feeling unsupported in the survey, felt that ‘we need someone who will help us [on] our time’.
Parents frequently drew attention to the fact that, while there may be some support available for their autistic son or daughter, there was a serious lack of whole-family support. This was perceived to result from a lack of financial support for family activities as ‘the council gives only for the [autistic] child’ and that ‘you are not supposed to spend [the personal budget] on other children’. They mentioned that ‘there are very few opportunities for siblings to attend places with their disabled siblings’, which resulted in them missing out on opportunities to ‘help them be closer together, to understand their brother or sister better’, which ‘can be quite upsetting for them’. Parents noted that this lack of focus on the whole family ‘seems to isolate people’ and did not promote ‘developing relationships and connections’ as a family. Indeed, one parent said, ‘you manage your life as a family, you don’t manage it in these isolated pockets’.
Finally, all parents highlighted the need for tailored post-diagnostic support. The experience of receiving a diagnosis was highly emotional for parents and many reported feeling unable to cope (‘I was exhausted’) as the experience ‘was so full on’. They reported finding it difficult to come to terms with their child’s diagnosis, describing it as ‘a sort of traumatic experience’ that can ‘come out of the blue’ or ‘as a bit of a shock’. As a result, many parents indicated that the initial support they received was not entirely beneficial, either because it was simply not enough, or that they were not in a position to process any support they were offered as, ‘emotionally, you are a bit incapable of dealing with anything other than trying to get through your trauma’. Some parents felt that professionals simply bombarded them with ‘too much information’ that ‘doesn’t sink in’. Instead, they suggested ‘counselling to come to terms with a diagnosis’ should be the primary focus for initial support, with ‘follow-up maybe a couple of weeks later’ to provide further information, or to go over the earlier information given, as the initial period around the diagnosis ‘was actually quite an awful time’.
Theme 4: desire for a sense of community and togetherness
Parents consistently reported wanting to feel more connected to others. They highlighted the importance of close home–school partnerships, having clear and open lines of two-way communication, including via home–school diaries, face-to-face meetings and phone calls. They felt this was critical given that school staff were often the first ‘people that I turn to because [my child] spends a lot of time there’ and that ‘if they need something they contact me, if I need something I can call them’. Such communication enabled them to collaborate more effectively to support their child (‘when you work together, it can help’) and ensured consistency of support across home and school settings (‘they tell us what they are doing there, so here we do the same thing’). Home visits from professionals were felt to strengthen the perceptions of support with one parent noting it allowed them ‘to talk together about what we can do’. They also felt that it was extremely beneficial when the school was able to provide support with difficulties in areas other than education and learning such as housing and help with Disability Living Allowance (a social security benefit in the United Kingdom) and ‘do some courses’.
Many parents identified the benefits of support from family and other parents. Family was seen to provide ‘mainly moral support’; they were ‘always there for us, understanding’. Some parents felt that the support they received from family meant that they did not need ‘any support from outside’, preferring to ‘deal with it as a family’ and ‘manage it in our own dysfunctional way’. Other parents of autistic children were universally identified as being an additional source of support and helped to create a sense of community and togetherness. Being able to connect with other parents meant ‘not feeling like you are isolated’ because there are times when ‘you feel so alone’. Parent groups were seen as excellent forums for support and advice ‘because they [other parents] have similar situations’. For some, having contact with other parents in the period immediately following diagnosis was particularly important: ‘the only useful thing they done, professionals at the time, was getting other parents to contact me’. Other parents helped to provide ‘more of an idea about the condition’ and a source of emotional support where parents could go and sometimes just ‘cry together and then by the time they finish crying, they all feel better’. Having ‘other people who were in the same boat’ from a similar culture also helped as ‘people understand things from different cultures differently’ – something that they felt professionals rarely understood.
Parents also spoke of the need to be armed with knowledge about autism. For some, this was a case of learning from experience so that ‘after six years I know what [my child] wants’. Others noted the need to actively ‘do some research’ into autism, which helped them to cope. Specific courses aimed at developing parents’ understanding, such as the UK’s National Autistic Society’s Early Bird course (Shields, 2001), were also seen to be highly beneficial: ‘thank God I did that. I knew nothing about [autism] and that was really helpful’. Being more informed had the biggest impact on their day-to-day lives, leading them to ‘understand [my child], how to communicate [with him]’. Nevertheless, they noted that the vast amount of information on autism was also overwhelming, with ‘a lot of information that is probably best avoided’.
Finally, parents sought proactive services that ‘asked what I wanted’ and actively contacted them (‘they called me’). Being ‘consulted a lot’ contributed to a sense of togetherness and made accessing support ‘an easy process’ as well as eased ‘a bit of the battle’, the constant fighting parents felt they had to engage in to access support. Parents also reported wanting community services that are aware of the needs of their child and actively look to involve them in activities, including when settings such as local swimming pools have a ‘special needs session’ or when doctors ‘take [the child]’s needs into account’ during visits. Many also wanted support to help them navigate support services because, at the moment, they felt ‘the dots just don’t join up’. One parent said, ‘the best kind of support you can get, something that gives you a tool to actually navigate the system that you are about to engage with’.
Discussion
This study sought to understand the perceived support needs of families of autistic children with additional intellectual disabilities and limited spoken communication, all of whom attended a special school in inner-city London. An initial survey established the support needs of this particular sample of parents. Following this, semi-structured interviews were conducted with a subset of parents to identify the specific areas parents found most challenging for their family and, critically, the exact nature of the services they desired. The survey and interview data pointed to a combination of formal and informal supports that parents felt would best meet their needs, including personal support (time to ‘recharge their batteries’, short breaks), social support (contact with other parents) and professional support for their child (better understanding of those working with their child); generally corroborating the findings from existing studies within (e.g. Preece, 2014) and outside (Hodgetts et al., 2013; Meirsschaut et al., 2010; Weiss et al., 2016; Woodgate et al., 2008) the United Kingdom. Yet, when we probed issues surrounding support during interviews, parents highlighted the distinct lack of services and supports available to address them and their child’s specific needs, which ultimately made them feel isolated and alienated. When support was available, it was often perceived to be extremely difficult or even impossible to access and failed to fit with the realities of their everyday lives. Instead, they called for services that are proactive and family-centred in their approach, ultimately making them feel more connected and cared for.
Notwithstanding, parents’ reports of their own mental and emotional health were encouraging: in the survey, the majority of parents rated their health as ‘good’, ‘very good’ or ‘excellent’ and over three-quarters of parents reported having someone to turn to for help and support if they needed it. Similar to previous findings, parents reported that the majority of support they received when they faced difficulties in their family came either from people close to them (family and friends) (Twoy et al., 2007) and, to a lesser extent, from official sources (school staff) (Preece, 2014) or the ‘third sector’ (parent support groups or religious activities). Notably, however, the survey results also suggested that different types of support might be required for different groups of parents. Parents who felt unsupported reported, on the whole, receiving less social support, and wanted greater access to more formal than informal support, including service provision and communication with service providers (school staff and others working around the child) – as well as more time and space for them and their family (see also Tehee et al., 2009), compared with parents who felt supported.
The interviews with parents further contextualised the findings from the initial survey. Parents’ reports of the challenges they faced caring for their child’s complex needs often went beyond their specific autistic symptoms and included children’s sleep, dietary, language and self-care needs. This finding chimes with many recent studies demonstrating that autistic children’s co-occurring behavioural difficulties, adaptive functioning and communication skills are associated with parental stress (Giovagnoli et al., 2015; Hall and Graff, 2011; Hartley and Schultz, 2015; Zaidman-Zait et al., 2016) and family quality of life (Gardiner and Iarocci, 2015). There are some studies, however, that have found no significant relationship between such difficulties and parental stress (Davis and Carter, 2008; Estes et al., 2009; McStay et al., 2014). A potential explanation for these discrepant findings may relate to differences regarding how ‘severity’ or everyday challenges are conceptualised and measured. Brei et al. (2015) showed that while clinically rated levels of autism severity did not show any relationship with parental stress, parents’ own perception of severity did, highlighting the subjective nature of definitions of severity and therefore of need. Families will also vary considerably in their ability to manage the challenges they face. Consequently, formal support services need to take a more holistic approach to support provision that looks beyond the categorisation of need and subsequent allocation of resources based solely on clinically defined difficulties experienced by the child him/herself (Derguy et al., 2016) to the perceived stress experiences of families more broadly.
This is not, however, the approach adopted by existing local support services, at least as reported by this sample of parents of autistic children. They repeatedly highlighted that existing support often fragments their families rather than brings them together. One key example of the lack of attention towards families’ needs was parents’ sentiments towards respite support. Not only did they want more respite support, they wanted more flexible support, allowing parents the chance to recharge their batteries when they need it most. This finding is consistent with previous studies showing both that flexible respite is highly valued by parents and that parents and formal support services may hold different conceptions of what useful respite provision looks like (MacDonald and Callery, 2004; Welsh et al., 2014).
The need for a family-centred approach to support has long been recognised as the natural progression from institution-centred and child-centred support (e.g. Wehmann, 1998). In line with this approach, and just like similar legislation in the United States (Individuals with Disabilities Education Act (IDEA)), England’s recent Children and Families Act (2014) places a greater emphasis than preceding legislation on outcome focused, person-centred practice when considering assessment, planning and support (UK Department for Education, 2014). Under the Act, local education authorities have a duty to involve parents and young people in educational decisions, giving them greater choice and control in the support and services they receive. The implementation of this Act is still in its infancy but critics have warned previously that legislation of this kind could lead to an oversimplification of support needs based on a rigid, indiscriminate, prescriptive approach defined simply by within-child characteristics (e.g. Sanderson et al., 2006). Furthermore, the reliance on standardised assessment measures for support, the constant form-filling to which parents in this study referred, also tacitly implies that greater value is given to the expertise of the professionals who create and interpret the assessment measures than parents’ own understanding of their support needs (Dempsey et al., 2009) and can lead to parents seeing themselves as viewed as a category rather than an individual member of a wider community. Many of the parents interviewed herein supported this view, reporting that they felt disconnected from formal services, which they perceived to have little understanding of their child and family and their specific needs.
Interviewed parents also reported that their encounters with formal support services were overly bureaucratic, that they needed constantly to ‘fight’ to obtain the services to which they were entitled, and ultimately felt isolated from, and misunderstood by, services they perceived should be supporting them. This discourse of struggle with bureaucracy and the sense of an adversarial relationship with formal support services for parents of autistic children are not new (Fleischmann, 2005; McNerney et al., 2015; Makin et al., 2016; Marshall and Long, 2009; Paradice and Adewusi, 2002; Preece, 2014; Tissot, 2011; Truss, 2008; Woodgate et al., 2008). Nevertheless, the Children and Families Act promised to cut the bureaucratic ‘red tape’ that too-often besets families’ interactions with government departments and engage with key stakeholders (including parents) to collaborate in the planning and subsequent commissioning of joint services to provide a ‘local offer’ of services available in each local education authority (UK Department for Education, 2014). The findings from this study suggest that there is some way to go to ensure that these legislative changes have a positive impact on families. They also suggest, rather worryingly, that the brunt of the perceived systemic failures are potentially being borne by parents who already feel unsupported, who, in this study, appeared to be accessing less social support and felt that they did not have the resources (time, energy, money) or the opportunities to engage with formal support services.
How should formal support services work towards providing support services that families feel are best suited to their needs and promote family wellbeing? According to one promising model (Cottam, 2011), collaboration is not enough. Rather, support services need to adopt a more relational approach, that is, one that is ‘more human, caring and time rich’ (p. 136) and takes the time to develop strong relationships with the family, understanding their specific needs (Hodgetts et al., 2013). Adopting a shared, collective, relational approach should be critical to identifying families’ unique culture (Benevides et al., 2016; Searing et al., 2015), family (especially sibling; Orsmond et al., 2009) and community characteristics, ensuring that the support received is tailored to the context of families’ everyday lives (Steiner et al., 2012), and thus has a positive impact on family wellbeing.
One excellent example of this model in practice is an autism waiver programme in Massachusetts, USA – a participant-directed, in-home service programme for autistic children from birth to 8 years (Warfield et al., 2014). At the crux of the programme is the belief that developing and maintaining a collaborative working relationship among families and service providers – relational coordination (Gittell, 2011) – is critical to delivering effective services from the perspective of families. Warfield et al. (2014) found that families in the Massachusetts programme who reported greater relational coordination between themselves and multi-disciplinary teams experienced less stress and greater wellbeing. Importantly, it was not just that parents received greater control over the support they wished to receive; they also worked closely with staff in home and community-based services, who helped them navigate the support system and develop a support plan for their child and family. These two elements were precisely the ones highlighted by parents interviewed in this study. They noted both how difficult it can be to navigate the support system (‘the dots just don’t join up’) and how they wished professionals would be more proactive and understanding of their needs as a family.
The consequences of building positive partnerships – relationships (Cottam, 2011) – between professionals and families should be far-reaching. One of the main themes identified from the parents who were interviewed was the alienation and exclusion they experienced as carers for their autistic children. It is well established that stronger family cohesion and time spent together are positively associated with coping and quality of life for parents (Dodd et al., 2009; Frantzen et al., 2016; Mactavish and Schleien, 2004; Pruitt et al., 2016). Services that adopt a relational, whole-family approach should foster such cohesion, which, in turn, should provide the foundations for building a wider sense of community and togetherness – another theme identified by parents. The benefits of a greater sense of community and being part of a larger social support group have been highlighted in previous studies as a factor that is associated with decreased parental stress (Ekas et al., 2010), increased access to formal support (Pickard and Ingersoll, 2015), reduced isolation (Mandell and Salzer, 2007), increased sense of control (Frantzen et al., 2016), self-efficacy (Benson, 2016; Burke and Heller, 2016) and wellbeing (Benson, 2012; Lovell et al., 2012; Smith et al., 2012) and, therefore, parents’ perceptions that their needs are being met – which, in turn, can increase overall family quality of life (Jones et al., 2016). Future work needs to test the impact of a relational approach on formal support services delivered to families of children on the autism spectrum living in different countries and localities – on the functioning of both the family and the child.
Limitations
There are several potential limitations to this study. First, although one strength of this study was that it used mixed methods to examine the support needs of a previously unexamined group (socioeconomically diverse and culturally diverse parents of autistic children living in inner-city London), it is also possible that the issues raised by parents could well be idiosyncratic to this context. The fact, however, that the findings from the survey and the interviews are consistent with each other and also with those from similar studies conducted both in the United Kingdom (Ludlow et al., 2011; Preece, 2014), in North America (Altiere and Von Kluge, 2009; Vohra et al., 2014; Woodgate et al., 2008) and Europe (Meirsschaut et al., 2010) warrants confidence in the generalisability of these findings. Second, we did not measure the children’s intellectual or language abilities specifically for the purpose of either study so could not examine the possible relationship between these child-level characteristics and parental perceived self-efficacy and levels of support. Our study would have been strengthened by the inclusion of these measures, but it was felt that doing so would have overburdened parents, many of whom were considered already to be ‘hard to reach’ by the school. Finally, although another strength of the study was that it was a collaboration between autism researchers and school professionals (see Pellicano and Stears, 2011), the fact that the research was conducted by school employees might have affected the results in some way. Indeed, parents’ self-reports on their mental and physical health and parental self-efficacy in the survey were surprisingly high and could be related to demand characteristics. Notwithstanding, many parents still reported ways in which they felt unsupported by the school suggesting that the interviewer gained a significant amount of trust with them. Furthermore, the active involvement of the school in the research ensured, we believe, a greater rate of participation in both studies (see Ennis and Wykes, 2013), especially for the interviews, in which there were a number of parents who were especially difficult to engage.
Conclusion
Supporting parents of autistic children with additional intellectual disabilities and limited spoken communication around the specific areas of expressive language, diet, sleep and self-care skills should be seen as priorities for service providers. Critically, providing this support should be done within the context of a relational, family-centred approach – one that takes the time to understand the specific needs of the whole family (including siblings), building a close working relationship with them and ensuring that they are supported at times when the parents and families feel they need it most. The involvement of school professionals at the forefront of service delivery in the research process has ensured that the findings can have a more immediate, practical impact, with considerable changes made to school practice and the relationship that school professionals have with the families they support.
Supplementary Material
Supplementary Material, AUT687989_Lay_Abstract – ‘The dots just don’t join up’: Understanding the support needs of families of children on the autism spectrum
Supplementary Material, AUT687989_Lay_Abstract for ‘The dots just don’t join up’: Understanding the support needs of families of children on the autism spectrum by James Galpin, Penny Barratt, Edward Ashcroft, Scot Greathead, Lorcan Kenny and Elizabeth Pellicano in Autism
Footnotes
Acknowledgements
We are very grateful to the families who so generously gave their time to take part in this research. Many thanks also to Laura Crane and Marc Stears for comments on a previous version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported through UCL Institute of Education’s Higher Education Innovation Funding (HEIF) Major Initiatives scheme. Research at the Centre for Research in Autism and Education (CRAE) is also supported by The Clothworkers’ Foundation and Pears Foundation.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.