
Abstract
We examine whether behavioral, mental health, and physical health characteristics of children with autism are associated with baseline and change in health-related quality of life. We measured health-related quality of life with the Pediatric Quality of Life Inventory 4.0 total scores from children enrolled in the Autism Treatment Network. We used linear mixed model regressions with random slopes. Predictors of lower health-related quality of life at baseline included demographic and insurance characteristics, diagnosis, higher Child Behavior Checklist internalizing and externalizing scores, sleep problems by Children’s Sleep Habits Questionnaire, seizures, gastrointestinal problems, and mental health problems. Several characteristics had different associations over time. This study demonstrates that in addition to behavioral and autism-related characteristics, physical and mental health conditions are associated with health-related quality of life in children with autism.
Keywords
Introduction
Autism is a neurodevelopmental disorder. The diagnostic criteria include deficits in social communication and social interaction, and restrictive, repetitive behavior patterns or interests. Symptoms present early in development and cause clinically significant impairment in social, occupational, or other areas of functioning (American Psychiatric Association (APA), 2013). Prevalence is currently estimated at 14.6 per 1000 in the US population based on a sample of 8-year olds (Christensen et al., 2016a, 2016b). Children and youth with autism frequently have a variety of co-occurring conditions including psychiatric and mental health conditions, gastrointestinal (GI) issues, sensory difficulties, sleep, epilepsy, and immune abnormalities (Coury et al., 2012; Gottfried et al., 2015; Levy et al., 2010; Reynolds and Malow, 2011; Simonoff et al., 2008; Viscidi et al., 2013).
Quality of life refers to multidimensional subjective evaluations of positive and negative aspects of life (WHOQOL Group, 1998). Health-related quality of life (HRQoL) focuses on the dimensions more directly related to physical or mental health and includes subdomains related to physical activities, positive health behaviors, school functioning, and psychosocial well-being. At the individual level, it is measured by questionnaires inquiring about satisfaction with aspects of life or level of engagement in different types of activities. Ferrans et al. (2005) provide a conceptual model of HRQoL based on Wilson and Cleary’s (1995) work that includes health-related domains of biological function, symptoms, functional status, and general health perceptions within the context of individual and environmental characteristics.
There is a growing pediatric literature on HRQoL and autism. A recent review of HRQoL among children and youth with autism found eight studies that showed relationships between autism-related assessments and functional abilities (Ikeda et al., 2014). These include associations of HRQoL with measures such as adaptive behavior (Kamp-Becker et al., 2010, 2011; Kuhlthau et al., 2010; Tilford et al., 2012) and behavioral problems as measured by the Child Behavior Checklist (CBCL) and subscales of the Autism Behavior Checklist (ABC) (Kuhlthau et al., 2010, 2013; Varni et al., 2012). These studies generally show lower HRQoL associated with more behavioral problems. A more recent study shows similar findings of associations of the Vineland-II, the CBCL, Cognitive ability, and the Autism Diagnostic Observation Schedule (ADOS) severity score with HRQoL (Payakachat et al., 2014). Symptoms of attention-deficit/hyperactivity disorder (ADHD) and anxiety are also negatively correlated with HRQoL in children with autism (Sikora et al., 2012; Tilford et al., 2012; Van Steensel et al., 2012).
However, very few studies have considered physical health and treatment-related characteristics in this population. Among these studies, lower HRQoL is associated with increased reported sleep problems in two studies (Delahaye et al., 2014; Tilford et al., 2012), one of which also found associations with eating habits (Tilford et al., 2012). An additional study examined the impact of treatment of behavioral symptoms on HRQoL and demonstrated that aripiprazole showed improvements in HRQoL for children with autism compared to controls (Varni et al., 2012). The Delahaye and Tilford articles used a sample that overlaps with the sample used here but examined a limited array of physical health conditions.
This study seeks to expand on previous literature by assessing the relationship of HRQoL with a more diverse range of physical health conditions in autism spectrum disorder (ASD). It further examines HRQoL from both cross-sectional and longitudinal perspectives, using data from a large clinical ASD registry. We hypothesized that reports of physical health conditions would be associated with lower reported HRQoL scores and worse HRQoL over time.
Methods
Sample
The Autism Speaks Autism Treatment Network (ATN) is a network of clinics throughout North America that provides multidisciplinary care to children with autism (Perrin et al., 2016). The Autism Intervention Research Network on Physical Health (AIR-P) is a federally funded initiative to study and improve the physical health of children with autism. There are 19 current or former ATN/AIR-P sites from which we draw data. Individuals treated at these centers are enrolled in a registry upon consent to the registry and potential future studies. Main registry inclusion criteria are as follows: 2–18 years of age, plan for ongoing care at the ATN site, parent speaks English, and confirmation of an autism diagnosis using an ADOS (Lord et al., 2000) or the Diagnostic and Statistical Manual of Mental Disorders (4th ed. or 5th ed., text rev.; DSM-IV-TR; APA, 2000; DSM-5; APA, 2013). (Note all but a few months of this study took place while DSM-IV-TR was in place.) The registry collects information about behavioral and physical health, as well as HRQoL assessments at intake and annually thereafter (Murray et al, 2016). From March 2008 to July 2015, 4910 children were enrolled in the registry and completed the baseline Pediatric Quality of Life Inventory 4.0 (PedsQL) assessment within ±60 days of enrollment. These 4910 participants, 55% of whom had follow-up PedsQL assessments up to 4.7 years post baseline, were included in this analysis. This work is approved by the Institutional Review Boards (IRB) of the sites involved and the IRB of the clinical coordinating center.
Variables
HRQoL
We measured HRQoL using parent proxy reports of the PedsQL, an assessment tool commonly used in pediatrics and in studies of children with autism. The PedsQL is a generic (i.e. not condition specific) 23-item survey that includes a total score, a physical health, and psychosocial health summary score with subscales for emotional, social, and school functioning. Each item has a five-point response scale. The tool uses a 1-month recall period, and scores are converted into a 0–100 scale with higher scores indicating better HRQoL (Varni et al., 2001). The survey takes 5–7 min to complete. This measure of HRQoL was included in the registry because it is short, widely used in pediatrics, and has parent proxy report version.
The PedsQL has good psychometric properties for measuring HRQoL among healthy populations and children with chronic conditions with internal consistency alphas ranging between 0.90 and 0.92 (Varni et al., 2001, 2003). The tool has also demonstrated feasibility and reliability among children with Asperger’s syndrome and children with psychiatric disorders (Bastiaansen et al., 2004; Limbers et al., 2009); it was used in 5 of the 13 studies in the review article (Ikeda et al., 2014).
Socio-demographic characteristics
We examined age, gender, race (Caucasian vs others), and socioeconomic status. Family income above or below US$50,000 was determined by parent report where available, otherwise by the 2006–2010 median income in the reported zip code provided by the Population Studies Center Institute for Social Research at the University of Michigan (http://www.psc.isr.umich.edu/dis/census/Features/tract2zip/index.html). Insurance status was categorized into two distinct variables: (a) whether the individual had any private insurance and (b) whether the individual had any public insurance (individuals could report yes to both).
Autism-related and developmental characteristics
All children were administered a baseline cognitive instrument based on their age and ability to participate in testing. These include the Mullen Scales of Early Learning (for children from birth to 68 months; Mullen, 1995) and the Abbreviated IQ from the Stanford Binet Intelligence Scale, Fifth Edition (for children at least 2 years; Roid, 2003), among other standard scales. All scales are individually administered. Choice of scale was based on child’s age and developmental level. All measures use standard scoring with a mean of 100 and a standard deviation of 15.
Children had an ADOS (Lord et al., 2000) evaluation and the clinical severity score was calculated. The ADOS is a semi-structured autism observation measure that is the basis for an overall measure of autism severity (Gotham et al., 2009). The resulting severity score ranges from 1 to 10 with higher scores indicating more autism symptomatology.
Behavioral measure
We examined the CBCL internalizing and externalizing scores. The CBCL is a caregiver-completed behavioral checklist used to assess behavior problems and psychiatric symptoms among children. Parents report on their child’s behavior within the past 2 months. CBCL scores are expressed as T-scores for appropriate age and gender groups (mean = 50, standard deviation = 10) with higher scores indicating more reported behavior problems (Achenbach and Rescoria, 2000).
Health measures
We used the revised Children’s Sleep Habits Questionnaire (CSHQ), a 35-item tool designed to identify medically- and behaviorally based sleep problems in children (Owens et al., 2000b). Participants are asked to report on their child’s sleep behaviors over a typical recent week when completing the survey questions. Ratings are summed to generate an overall sleep score with higher scores indicating more severe sleep difficulties. Scores range from 33 to 99; scores ⩾41 indicate clinically significant sleep problems (sensitivity of 0.80 and specificity of 0.72; Owens et al., 2000b). The CSHQ has acceptable reliability and it discriminates community and sleep-disordered groups (Owens et al., 2000a). The raw total score was used in this analysis.
GI problems are based on parent reports of whether the child had problems with any of the following (reported separately): vomiting, reflux, diarrhea, constipation, and stomach pain now or in the past. Depending on the date of enrollment into the ATN registry, parents reported either the extent (none, mild, moderate, or severe), timing (never, past problem, or current problem), or prevalence (never or yes ever) of each problem. For the purposes of this analysis, each symptom was considered prevalent if the parent indicated there was ever at least a mild problem. Seizures, depression, bipolar disorder, anxiety, and obsessive compulsive disorder (OCD) were reported as whether the child had ever been diagnosed with the problem.
Data analysis
Linear regression models were fit to identify socio-demographic and autism-related characteristics associated with HRQoL at enrollment. The individual’s PedsQL summary score was the dependent variable. For associations between baseline characteristics and HRQoL over time, we fit linear mixed models with random slopes to account for within-subject correlation of measurements. All 4910 patients contributed to longitudinal analyses regardless of available post-baseline PedsQL scores. To correct for loss to follow up, defined as failing to return for a follow up visit after 2013, we constructed inverse probability weights. These weights are defined as the inverse probability of remaining in follow up through a given time, conditional on not yet being censored before that time and also conditional on the whole set of socio-demographic and autism-related characteristics. Conceptually, the weights allow patients with available PedsQL data during follow up to represent both themselves and patients with similar characteristics who were previously lost to follow up. A robust variance estimator was applied to accommodate the weights in the regression models. Given that complete data on all characteristics is required to estimate these weights, missing baseline characteristics were imputed using multiple imputations only for the construction of the weights. The longitudinal analysis was repeated without weights as a sensitivity analysis. No imputation was made when fitting linear models of PedsQL; analyses of a particular characteristic on PedsQL were based on patients with complete data for that characteristic. We conducted sensitivity analyses examining only those children with complete data for the predictor and outcome. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Descriptive data
Our sample at baseline was 6.2 ± 3.5 years (range: 1.5–17.6 years), 84% male, 80% Caucasian, 53% covered at least in part by private insurance, 53% covered at least in part by public insurance, and 52% with an income of US$50,000 or higher. The most common diagnosis was autism (72%) followed by pervasive developmental disorder not otherwise specified (PDD/NOS; 20%) and Asperger’s syndrome (8%). Average ADOS severity score was 7.1 (±1.9) and average full-scale IQ was 76.1 (±23.4). Mean CBCL T-scores for internalizing and externalizing scales were 62.8 (±10.5) and 59.6 (±12.0), respectively (Table 1).
Socio-economic and autism-related characteristics at enrollment.
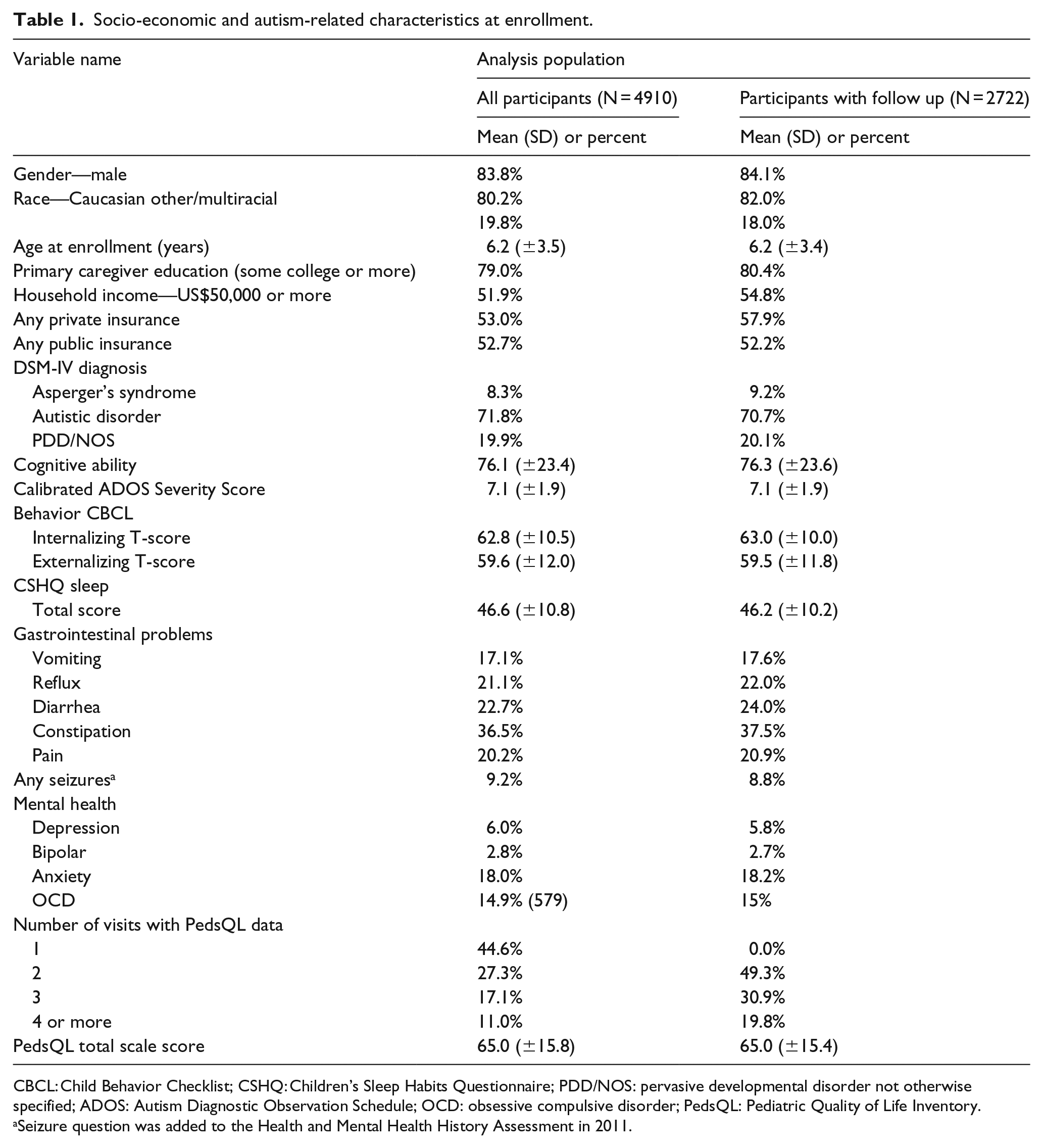
CBCL: Child Behavior Checklist; CSHQ: Children’s Sleep Habits Questionnaire; PDD/NOS: pervasive developmental disorder not otherwise specified; ADOS: Autism Diagnostic Observation Schedule; OCD: obsessive compulsive disorder; PedsQL: Pediatric Quality of Life Inventory.
Seizure question was added to the Health and Mental Health History Assessment in 2011.
Mean CSHQ total score was 46.6 (±10.8) which indicates that the average score is higher than the sleep problem threshold. The prevalence of GI issues in the overall population ranged from 17% of the sample reporting vomiting to 37% reporting constipation. In all, 9% of the sample reported seizures. The prevalence of reported mental health–related problems ranged from less than 3% (bipolar disorder) to 18% (anxiety) as shown in Table 1.
Mean PedsQL total score at baseline was 65 (range = 11.4–100). Participants with any follow up data were representative of the overall study population in terms of socio-demographic, autism-related, health, and behavioral characteristics at baseline (Table 1). In a mixed effects linear regression model, mean PedsQL scores did not significantly vary over time (slope = −0.08 PedsQL points per year; 95% confidence interval (CI) = −0.25 to 0.19 pointers per year; p-value = 0.57).
Univariate models
Results from univariate regression models of baseline PedsQL as a function of each socio-demographic or autism- and health-related characteristic are presented in Table 2. Each row describes the univariate effect of a given characteristic on mean baseline PedsQL without adjusting for any other factors (first column of numbers). Among all participants, we observed that individuals who were female, Caucasian, older, have a household income of less than US$50,000, or have public insurance, were all associated with lower PedsQL score at baseline. Mean PedsQL total scores were 5.8 points lower among participants with Asperger’s syndrome than autism at baseline. Neither IQ nor the ADOS severity score were associated with PedsQL. Higher (worse) CBCL T-scores for internalizing or externalizing behavior scores and higher (worse) CSHQ total scores were all associated with lower PedsQL scores. Each of the GI problems was associated with a lower score on the PedsQL, with pain having the strongest association. Similarly, having seizures or any of the four mental health conditions (depression, bipolar, anxiety, and OCD) were all associated with lower PedsQL scores in the univariate baseline models; participants with depression and participants with bipolar disorder differed from their non-depressed and non-bipolar counterparts by more than 15 PedsQL total score points.
Univariate associations of HRQoL at enrollment and over time.
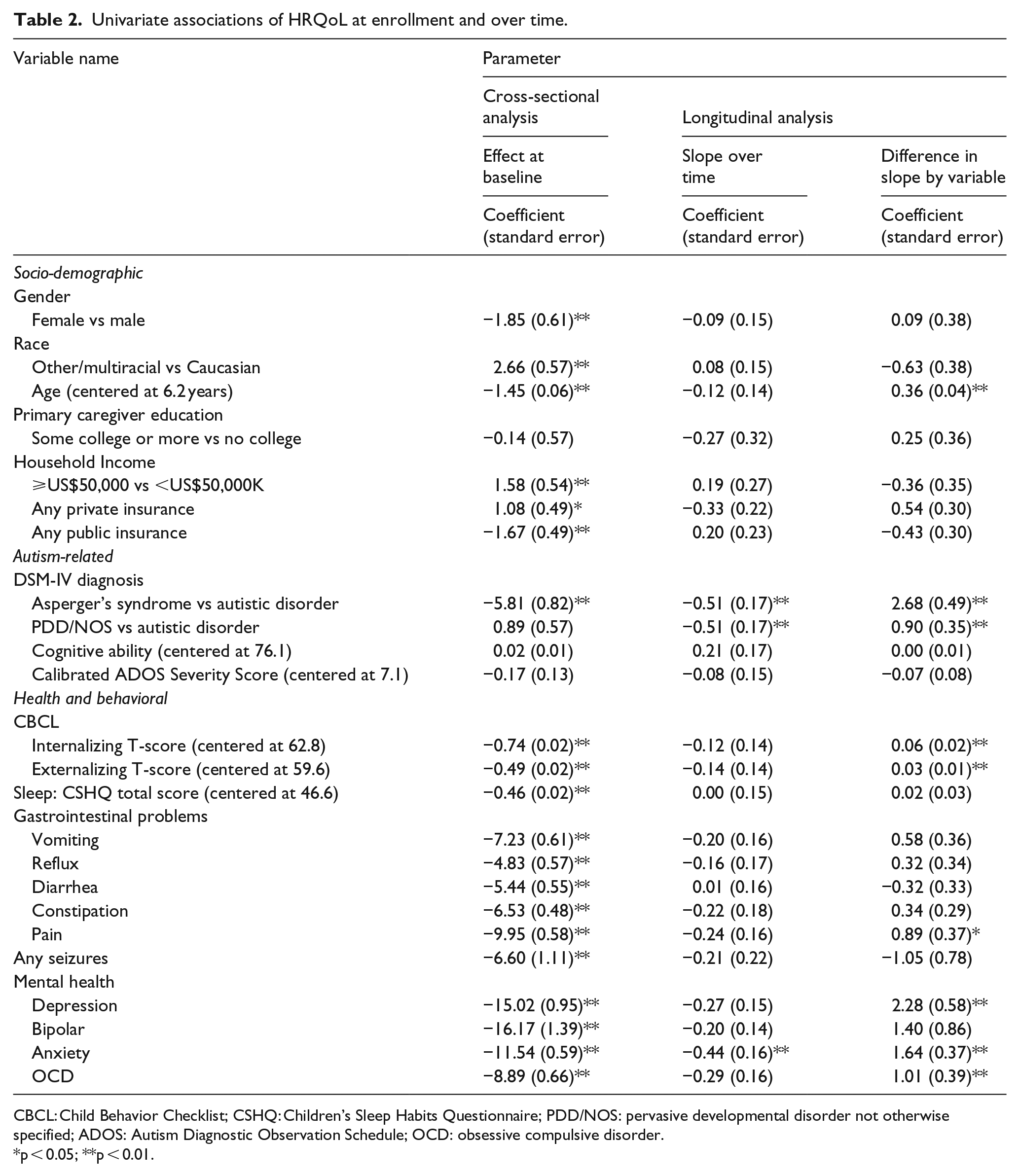
CBCL: Child Behavior Checklist; CSHQ: Children’s Sleep Habits Questionnaire; PDD/NOS: pervasive developmental disorder not otherwise specified; ADOS: Autism Diagnostic Observation Schedule; OCD: obsessive compulsive disorder.
p < 0.05; **p < 0.01.
Models with characteristics and time
Also presented in Table 2 are results from regression models of a given baseline characteristic’s association with HRQoL over time. For each characteristic, PedsQL scores were modeled as a function of the characteristic, time from enrollment (slope), and the interaction between the baseline characteristic and time (difference in slope by variable). The slope over time and interaction are included in Table 2 (second and third columns of coefficients). Although baseline PedsQL was negatively associated with age, T-scores for CBCL internalizing, and CBCL externalizing behaviors, higher baseline scores for each of these measures were associated with more rapid HRQoL improvement over time. Similarly, the negative associations between baseline PedsQL and stomach pain, depression, anxiety, and OCD diminished over time. In terms of autism diagnosis, participants with Asperger’s syndrome had worse mean PedsQL scores at baseline compared to those with autistic disorder, but this difference diminished over time. However, those with PDD/NOS had similar baseline PedsQL scores compared to those with autistic disorder but had a better HRQoL trajectory. Differences in PedsQL scores by gender, race, household income, insurance type, baseline CSHQ, and most GI problems, seizures, and bipolar disorder remained stable over time. In other words, the gaps in HRQoL observed at baseline by these characteristics did not narrow or widen over time.
Sensitivity analyses
Univariate regression models for each baseline characteristic’s association with HRQoL’s change over time were also done with complete data only and without any weightings. Significant results over time from weighted models held in unweighted models. Weighted results for depression and OCD showed diminished negative associations with PedsQL scores over time; however, in the unweighted models, having either depression or OCD was related to a small but significant increase in the negative associations with HRQoL over time. Although weighted models showed stable HRQoL over time in relation to private insurance, no private insurance was significantly associated with more rapid HRQoL improvement over time in relation to private insurance.
Multivariable models
We further examined multivariable models of HRQoL. We fitted a model for the cross-sectional PedsQL at baseline using 2873 participants with complete data (Table 3). The cross-sectional analysis selected and retained variables that predicted baseline PedsQL scores at a 0.05 significance level after adjusting for the other variables in the model. The resulting model included race, age, primary caregiver education, DSM diagnosis, CBCL internalizing and externalizing T-scores, the CSHQ total score, and prevalence of reflux, constipation, stomach pain, and bipolar disorder. Adjusting for all other characteristics, Caucasian children, older children, and children whose parents have some college (vs no college) have statistically significantly lower PedsQL scores. Contrary to the unadjusted analysis, after adjusting for socio-demographic, health, and behavioral characteristics, those with Asperger’s syndrome have the highest baseline HRQoL among the three DSM-IV diagnosis groups, followed by PDD/NOS, and then autistic disorder. As was the case in the bivariate analyses, higher CBCL externalizing and internalizing scores are associated with worse HRQoL. Similar findings are seen for the sleep scores (CSHQ) with worse sleep scores associated with worse HRQoL. Among the physical and mental health variables, negative associations between HRQoL and reflux, constipation, pain, and bipolar disorder lessen in magnitude compared to the bivariate analyses but remain statistically significantly associated with HRQoL after adjusting for all other characteristics.
Multivariate regression model of HRQoL at baseline.
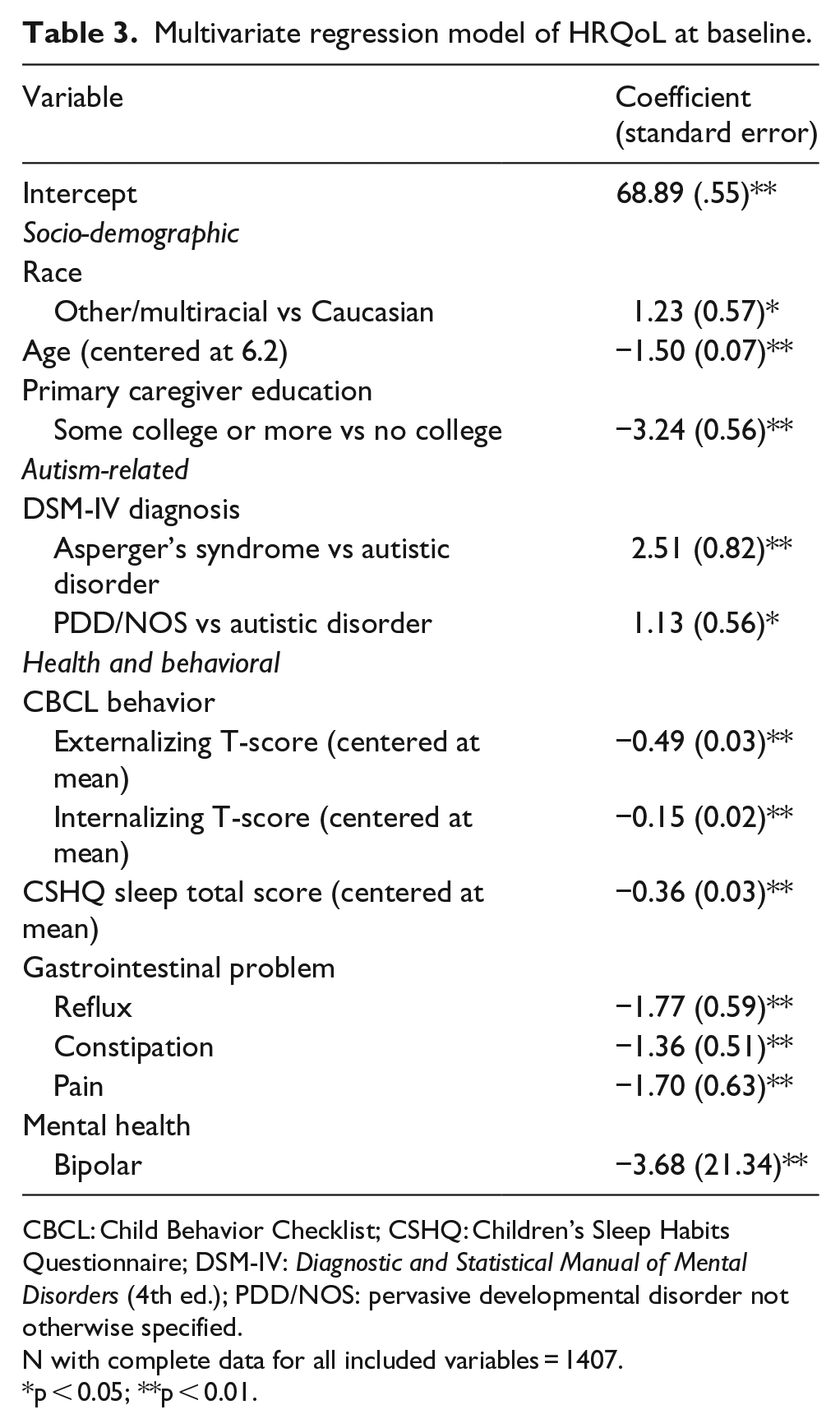
CBCL: Child Behavior Checklist; CSHQ: Children’s Sleep Habits Questionnaire; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.); PDD/NOS: pervasive developmental disorder not otherwise specified.
N with complete data for all included variables = 1407.
p < 0.05; **p < 0.01.
Discussion
This is the first study to examine the associations of HRQoL with physical health and mental health and the first to look at trajectories over time for these characteristics, as well as sleep and behavior characteristics. We showed in our univariate regression models that the cross-sectional HRQoL of children with autism was associated with sleep problems, GI problems, seizures, and mental health problems. The sleep associations have been demonstrated in a previous study using data from the ATN network (Delahaye et al., 2014). In our models, they were consistently statistically significant in bivariate and multivariate models and the association of sleep and HRQoL did not change over time. A variety of strategies have been identified to treat sleep disorders among children with autism which if successful may have an impact on the child’s HRQoL (Devnani and Hegde, 2015).
All GI issues were strong predictors in bivariate analyses and, except for stomach pain, these relationships did not change over time. In our multivariate model, we found that reflux, constipation, and pain were associated with HRQoL. Increasing attention has been paid to GI issues among children with autism. The bivariate relationships show quite large associations with GI symptoms, with the relationships attenuated in the multivariate cross-sectional analyses. A better understanding of the impact of GI symptoms on HRQoL, and whether treatment of issues improves HRQoL may be important (Coury et al., 2012; Ghaisas et al., 2016; Lange et al., 2015; Mahony and Stilling, 2015). Similarly, the relationship between mental health diagnoses and HRQoL in the context of high prevalence of co-morbid mental health issues for children with autism (Levy et al., 2010; Simonoff et al., 2008) may suggest that greater attention to treatment of co-morbid issues could result in improvements in HRQoL. Further research to understand the relationships between disease, symptoms, treatment, and HRQoL are warranted.
These findings show that baseline physical health and mental health characteristics are important predictors of HRQoL. These baseline associations suggest that physical health, mental health, and sleep issues are important characteristics to consider along with characteristics of autism and behavioral characteristics, when trying to understand the HRQoL of children with autism. These findings lend support to the notion that clinicians should screen and treat these physical health issues in addition to the screening and treatment of behavioral issues. Optimal treatment of underlying medical conditions could also potentially help children with autism to benefit more from behavioral interventions since co-existing conditions may interfere with learning progress, health, and HRQoL (Myers et al., 2007). Thus, there may be direct and indirect ways that co-existing conditions influence HRQoL in this population.
This study finds that reports of HRQoL are related to behavioral characteristics in the direction consistent with the literature (Kamp-Becker et al., 2011, 2010; Varni et al., 2012). We further show that the relationships between HRQoL and both the internalizing and externalizing T-scores of the CBCL lessen over time. CBCL T-scores were also included in the multivariate cross-sectional models and higher scores (indicating more problems) remained associated with lower HRQoL. ADOS scores showed no relationship in the bivariate models although they have been associated with HRQoL in other studies. In a study looking at associations with the ADOS and the Health Utilities Index mark 3 (HUI3; Feeny et al., 2002) and the Quality of Well-being Self-Administered Scale (QWB-SA; Kaplan et al., 1989) using a sample that likely overlapped with the data presented here, the relationship with the ADOS was negative with the HUI3 and positive with the QWB-SA (Tilford et al., 2012).
The longitudinal findings show that few of these associations change over time. Where they do change over time, in all cases, there is regression to the mean with the baseline association of problems with HRQoL ameliorated somewhat over time. Further work to explore what factors influence the trajectory of quality of life over time is important to inform clinical care. It also could inform expected potential changes with different treatment regimes. Prospective assessments of the impact of treatments over time may help to determine whether behavioral issues and physical and mental health conditions predict HRQoL. The fact that most children with an ASD receive an array of treatments (behavioral, medical, speech, OT, PT, etc.) with varying evidence of benefit complicates such studies but would nonetheless help inform future treatment choices.
This study is subjected to several limitations. First, the data come from a small number of autism treatment centers across North America. The patients seen in these centers may not be representative of patients with autism in the United States. As Table 1 shows, the sample has relatively educated parents (nearly 80% have education of some college or higher) with over 40% of the sample having annual household incomes over US$50,000. This is higher than that seen in a general population of US parents of children with special health care needs (National Survey of Children with Special Health Care Needs (NS-CSHCN), 2009). Of note, income was only obtained on a subset of the population. In the regression results, zip code median income was used where direct measurement was not available. Second, baseline data are not complete for all patients, and only about half of the sample has follow-up HRQoL data. Although Table 1 suggests that returners and non-returners are similar with respect to baseline characteristics, we have no way of knowing whether our sample is biased due to other factors. In an attempt to combat this potential bias, our analysis utilized inverse probability weighting, which essentially places weight on available follow up data such that a returner represents both himself or herself and non-returners who share similar characteristics (Hernán et al., 2004; Howe et al., 2016). However, this method fails to correct bias if returners and non-returners still differ by some unmeasured confounder.
Third, the reports of sleep, behavioral, mental health, and physical health issues are all based on parent report. Although parent report is a common source of such data (e.g. from national surveys such as the National Health Interview Survey), it is subjected to reporting biases and having one reporter may contribute to confounding. In addition, we do not have a measure of severity for these conditions. Finally, the measure of HRQoL is based on parent proxy report rather than self-report. However, this is consistent with published literature as most studies of HRQoL of children with autism (Ikeda et al., 2014) are based on proxy report and those that are not limit their samples to adolescents and higher functioning groups (Burgess and Turkstra, 2010; Cottenceau et al., 2012; Jennes-Coussens et al., 2006; Kamp-Becker et al., 2010, 2011; Sheldrick et al., 2012; Shipman et al., 2011).
This study examined associations of health characteristics with HRQoL with an emphasis on physical health conditions. Many health characteristics are related to HRQoL in cross-sectional models suggesting that along with core characteristics of autism, other co-morbidities should be considered important characteristics to consider when trying to improve HRQoL. A better understanding of causal relationships and relationships between treatment and HRQoL would further the field.
Supplemental Material
AUT704420_Lay_Abstract – Supplemental material for Associations of quality of life with health-related characteristics among children with autism
Supplemental material, AUT704420_Lay_Abstract for Associations of quality of life with health-related characteristics among children with autism by Karen A Kuhlthau, Erin McDonnell, Dan L Coury, Nalin Payakachat and Eric Macklin in Autism
Footnotes
Acknowledgements
The authors would like to thank all of the families who contributed data and the clinicians who collected the data. This work was conducted through the Autism Speaks Autism Treatment Network.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Autism Speaks and cooperative agreement UA3 MC11054 through the US Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Research Program to the Massachusetts General Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.