
Abstract
This study aimed to confirm whether autistic traits are normally distributed across a population and to describe their association with the sociodemographic characteristics of Japanese workers. The participants were 2075 workers aged 23–65 years from various parts of Japan. Autistic traits were measured using an abridged Japanese version of the Autism-Spectrum Quotient (AQ-Short). The AQ-Short comprises five subcomponents assessing a fascination for numbers and patterns (numbers/patterns), difficulties with imagination, a preference for routine, difficulties with social skills, and difficulties with switching attention. The five subcomponents of the autistic phenotype as well as the overall autistic phenotype itself were continuously distributed across the sample population of Japanese workers. Men had significantly higher AQ-Short scores than women. AQ-Short scores were not associated with age. Except for the numbers/patterns scores, workers of a lower socioeconomic status had significantly higher AQ-Short scores than their respective counterparts. For the numbers/patterns trait, workers of a higher socioeconomic status scored higher. Workers with low general physical activity had or tended to have higher scores for total and all subcomponent traits, except for the numbers/patterns trait. Generally, the autistic phenotype was more prevalent in workers of a low socioeconomic status, while a particular trait was prevalent among workers of a high socioeconomic status.
Keywords
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by impairments in social communication, social interaction, and the presence of restricted and repetitive behaviors (Wing, 1997). Adults with ASD living in a community are socially disadvantaged but tend to go unrecognized (Brugha et al., 2011). Previously, ASDs were considered clinical conditions distinct from the general population. However, Wing (Waterhouse et al., 1996; Wing, 1981, 1988) advocated a hypothesis that autistic traits vary continuously, from mild to severe, and that ASDs merge into what can be called eccentric normality and there is no clear cutoff point. It was indicated that a diagnosis of an ASD is considered only if help is sought by parents or by individuals themselves for difficulties with everyday life (Wing, 1997). Previous studies showed that autistic traits are continuously distributed across the population (Constantino and Todd, 2003; Hoekstra et al., 2011). Specific autistic traits that were classified based on the pattern of impairments and behavioral problems were also suggested to be distributed continuously rather than discretely (Wing and Gould, 1979), but the empirical evidence is lacking.
Some studies have investigated the association between ASD or autistic traits and sociodemographic characteristics. Men have a significantly higher score for autistic traits than women (Baron-Cohen et al., 2001; Brugha et al., 2011; Hoekstra et al., 2011; Kurita et al., 2005; Pisula et al., 2013; Wakabayashi et al., 2006) and ASDs are not associated with age (Brugha et al., 2011). Although individuals with ASD are generally considered to be socially disadvantaged, the empirical data are scarce and inconsistent. Brugha et al. (2011) showed that ASDs were more prevalent among less-educated people in community-dwelling adults in England. Meanwhile, Baron-Cohen et al. (1998, 2001, 2007, 2009) reported that Mathematics Olympiad winners had significantly higher scores for autistic traits than male Cambridge humanities students and indicated that mathematical talent is linked to autism. However, relevant socioeconomic factors other than education, that is, income and occupational position, were not investigated. Concerning health-related behaviors, previous studies showed an association between ASD and low physical activity (Healy et al., 2017; Pan et al., 2016). Children with ASD had lower fitness levels than their typically developing peers (Tyler et al., 2014). Moreover, children with ASD were reported to spend an hour more in sedentary behaviors on weekdays compared with typically developing children, and most of this difference was due to screen time (Must et al., 2014). However, relevant health-related behaviors other than physical activity, that is, drinking habits and smoking habits, were not investigated.
Using a Japanese working population, we aimed to confirm whether the overall autistic phenotype and its subcomponent traits were distributed across the population and to describe their association with sociodemographic characteristics in Japanese workers. Our research might help to determine the mechanisms by which individuals with high autistic traits utilize their skills and the appropriate support they need.
Methods
Participants
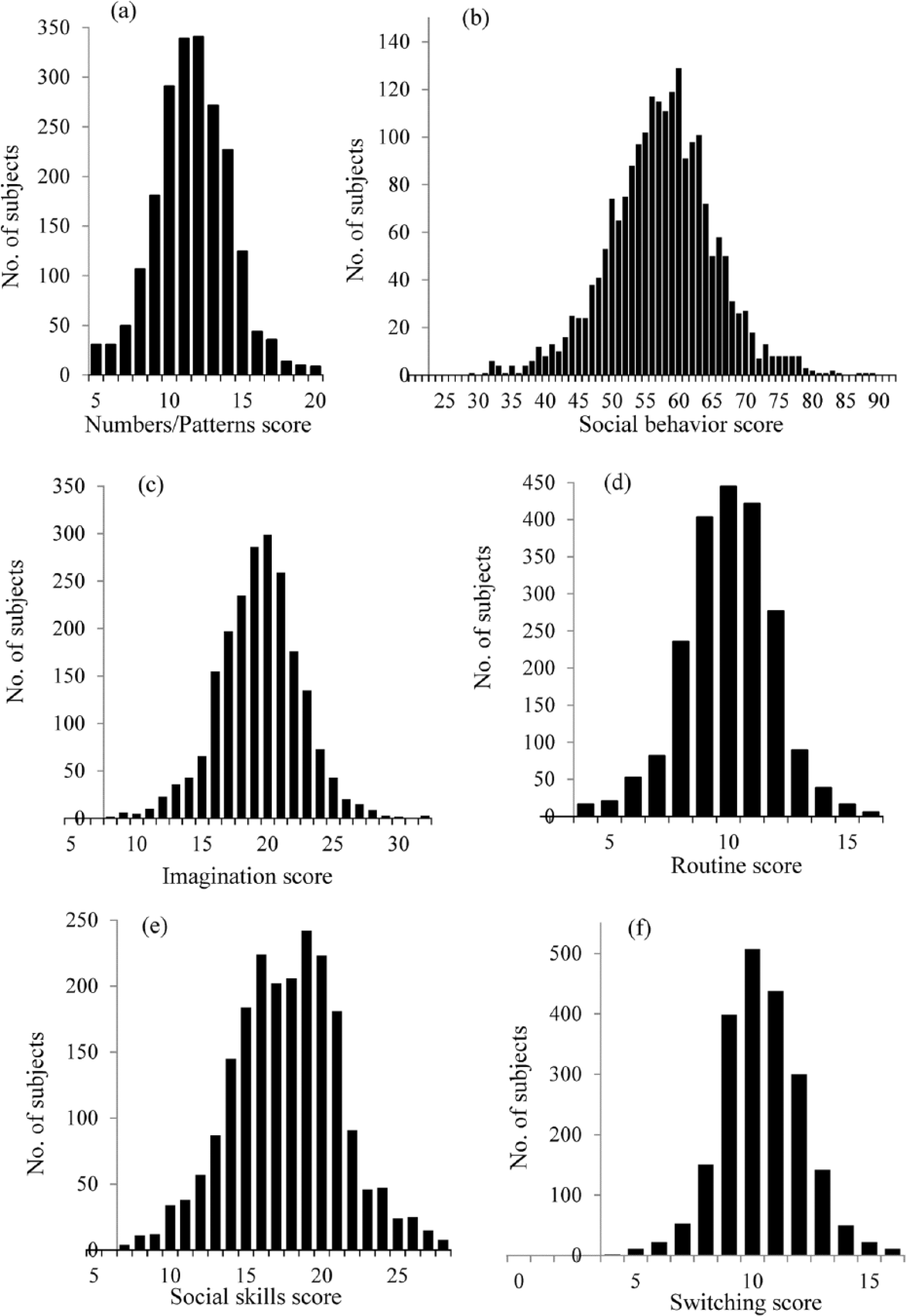
This study used data obtained from a survey, the Japanese study of Health, Occupation and Psychosocial factors related Equity (J-HOPE), conducted to examine social class and health in an occupational cohort (Miyaki et al., 2012; Suzuki et al., 2015). This study was conducted to develop and expand research aimed at elucidating the mechanisms underlying social disparities in health and to establish measures of control. The present analysis was conducted with the J-HOPE data set as of 8 January 2014. Workers at a major Japanese manufacturing company (headquartered in Kyoto, with 11 other main offices throughout Japan) were recruited as participants, including various occupational positions (managers, 26.2%; researcher and professional workers, 8.9%; engineers and technicians, 15.9%; clerical workers, 17.0%; service workers, 4.2%; manufacturing workers, 18.7%; and others, 9.0%). All workers were invited to participate. In the first year of the data collection (2010), 2266 workers agreed to participate (response rate: 90.1%; age range: 21–65 years; 241 women, 2025 men). By the fourth year of the study (2013), there were 2187 participants. We used data from the fourth year, as this was the year in which the autistic traits were assessed. After excluding 112 participants, who had missing autistic traits data, and 2 participants diagnosed with ASD, 2075 participants (age range: 23–65 years) were included for the analysis. All participants were not asked if they were tested for ASD. However, workers suspected to have ASD were assessed using interviews and an abridged version of the Autism-Spectrum Quotient (AQ-Short) and accordingly referred to specialists by industrial physicians. Of these suspected workers, two excluded participants were diagnosed with ASD.
The J-HOPE study obtained ethical approval from the University of Tokyo Ethics Committee, the National Center for Global Health and Medicine Ethics Committee, and Kitasato University School of Medicine Ethics Committee. All participants provided written informed consent before enrolling in the study.
Sociodemographic characteristic
The participants were surveyed using a self-administered questionnaire. Sociodemographic characteristics included gender, age, living state, socioeconomic status (SES; i.e. education, occupational position, and pre-tax annual household income), and health-related behaviors (i.e. drinking habits, smoking habits, and leisure-time physical activity).
Age was classified into three groups: 41 years old or less, 42–49 years old, and 50 years old or more. Living state was classified into two groups: alone and not alone. Education was dichotomized into junior college or higher (i.e. 14 years or more) and high school or less (i.e. less than 14 years). Occupational position was classified into two groups: managerial and non-managerial. Pre-tax annual household income was classified into three groups: <500 million yen, 500–1000 million yen, and 1000 million yen (yen = Japanese Yen; 100 yen is approximately equal to US$1). Drinking habits were classified into two groups: rarely and sometimes or daily. Smoking habits were classified into two groups: current smoker and non-current smokers (individuals who smoked previously but do not smoke anymore and those who never smoked). Leisure-time physical activity was classified into two groups: yes (from light physical activity 1 or more times per week to intense physical activity 3 or more times a week) and no. Drinking habits were measured through the following the question: “Do you drink alcohol?” Participants choose from these answers: “I rarely drink,” “I occasionally drink,” or “I drink almost every day.” Smoking habits were measured through the following the question: “Do you smoke?” Participants choose from these options: “I do not smoke,” “I quit smoking,” or “Yes, I do smoke.” Leisure-time physical activity was measured through the following statement: “Please choose the option that applies to your leisure exercise.” Participants selected from “I do not exercise or play sport every week,” “I do light exercise more than once a week (not causing shortness of breath or palpitations),” “I do intensive exercise one to two times a week (with shortness of breath, palpitations, perspiration) for at least 20 minutes,” or “I do intense exercise for at least 20 minutes at least three times a week.”
Autistic traits
The AQ-Short is a self-administered test that measures the degree to which an adult with normal intelligence has traits associated with ASD (Hoekstra et al., 2011). The AQ-Short was developed based on the questionnaire created by Baron-Cohen et al. (2001) and is used worldwide. The AQ-Short total scores have shown accurate differences between control participants and individuals clinically diagnosed with Asperger’s syndrome. It was reported that the distribution of the AQ-Short scores was approximately normal across the Dutch general population and English student population (Hoekstra et al., 2011).
The AQ-Short subcomponent scores were used as a measurement for specific autistic traits. The AQ-Short comprises two higher-order subcomponents assessing a fascination for numbers and patterns (numbers/patterns, 5 items) and social behavioral difficulties (social behavior, 23 items) (Hoekstra et al., 2011). The social behavior subcomponent further comprises four lower-order subcomponents assessing difficulties with imagination (imagination, eight items), a preference for routine (routine, four items), difficulties with social skills (social skills, seven items), and attention switching difficulties (switching, four items) (Hoekstra et al., 2011). Participants responded to given statements using a 4-point Likert scale: 1 = definitely agree, 2 = slightly agree, 3 = slightly disagree, and 4 = definitely disagree. Scoring was reversed for items in which an “agree” response reflects the presence of a characteristic of autism. Scores are summed, with a minimum AQ-Short score of 28 indicating no autistic traits, and a maximum score of 112 indicating a full autistic phenotype. We used a Japanese version of the AQ-Short form, which had been translated into Japanese by the authors of this study and independently back-translated by a native English speaker. If participants answered all 28 items, and then, the data of AQ-Short were considered acceptable.
Statistical analysis
Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were presented as percentages to show participants’ sociodemographic characteristics. Distributions of the AQ-Short scores and the AQ-Short subcomponent scores were estimated to determine whether they were continuous. Analysis of covariance (ANCOVA) was used for comparison of adjusted averages of the AQ-Short scores and the AQ-Short subcomponent scores according to each sociodemographic characteristic. This model was adjusted for age and gender. Two-tailed p values of <0.05 were considered statistically significant. All analyses were conducted using SPSS (version 20 for Windows, IBM Inc., New York, USA).
Results
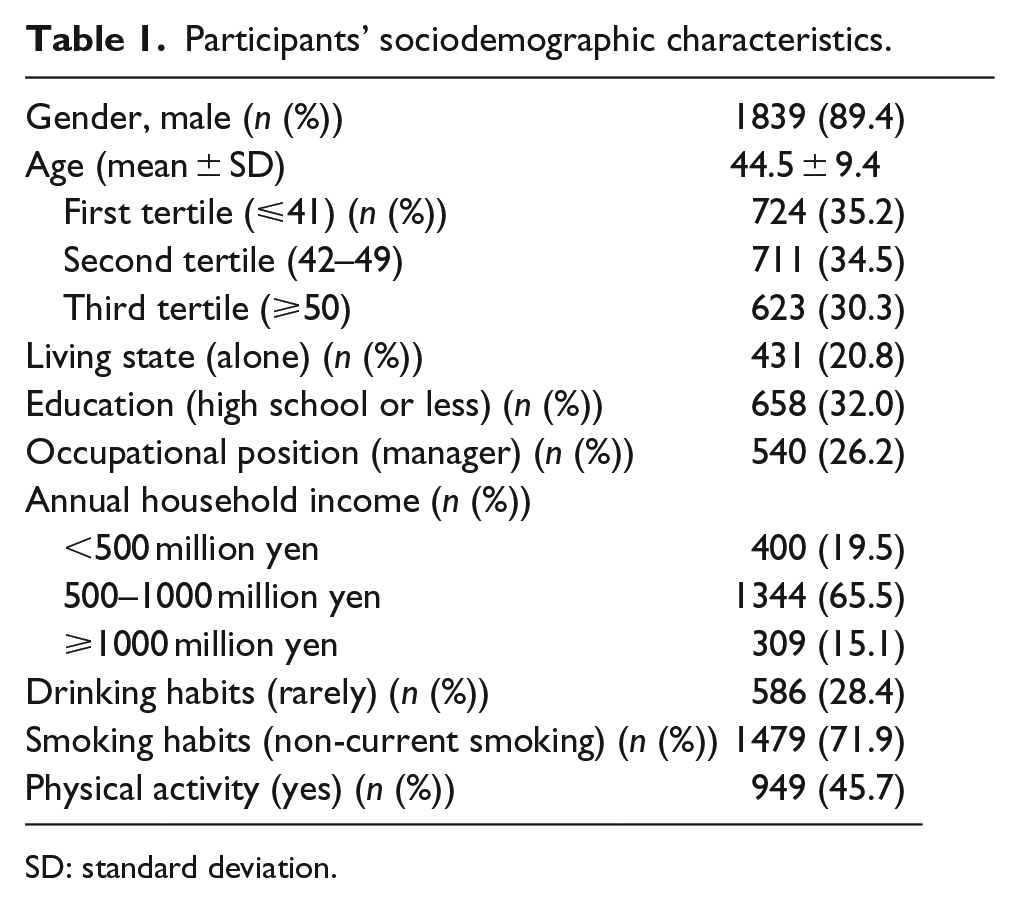
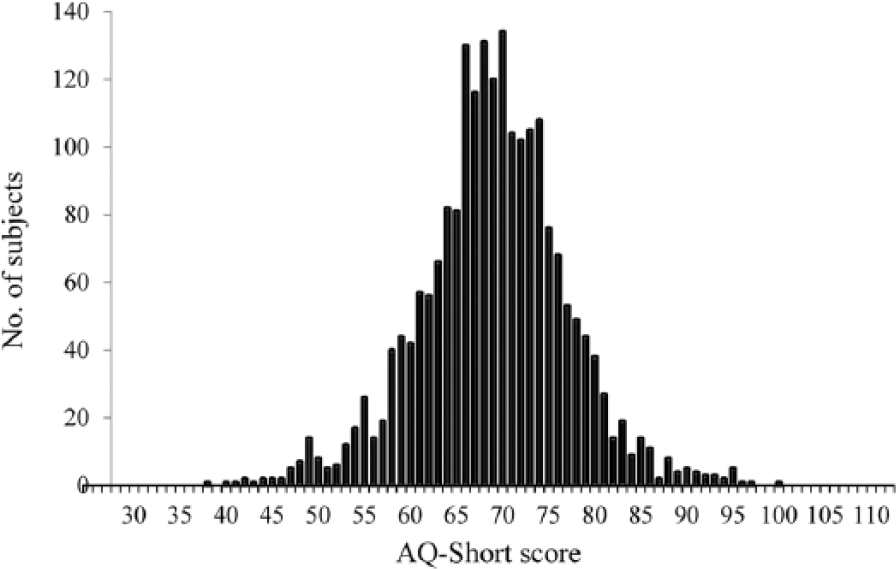
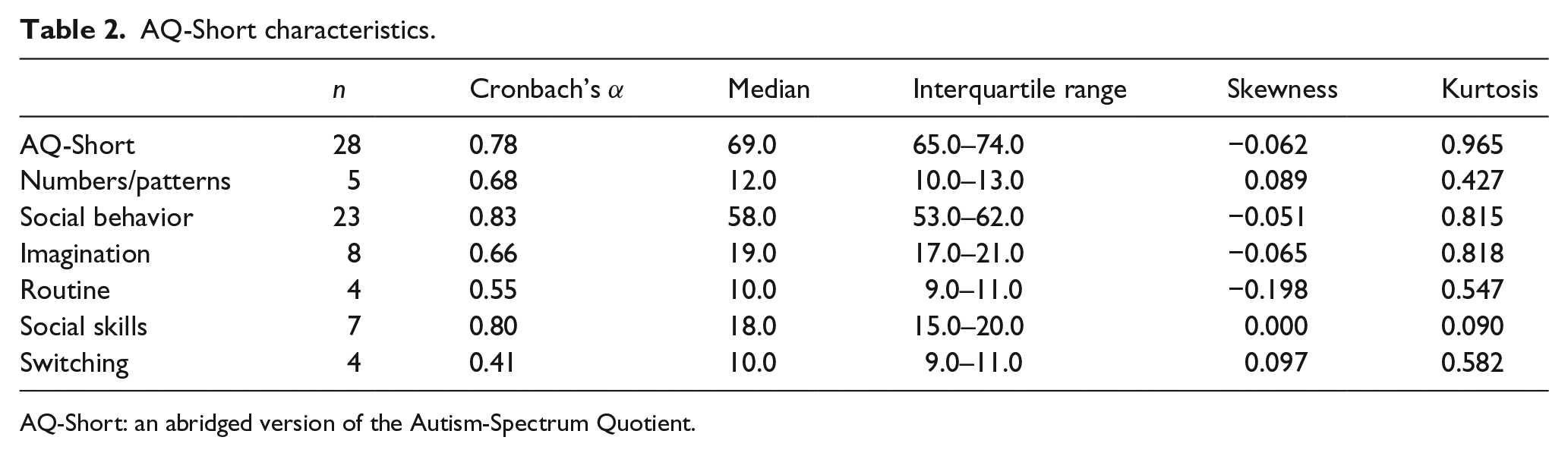
Participants’ characteristics are presented in Table 1. Distributions of the AQ-Short scores and the AQ-Short subcomponent scores of the workers are shown in Figures 1 and 2. The participants’ AQ-Short scores and all AQ-Short subcomponent scores (numbers/patterns, social behavior, and the four social behavior subcomponents: imagination, routine, social skills, and switching) showed continuous distributions. Table 2 also shows that the skewness or kurtosis values of both the AQ-Short and the AQ-Short subcomponent did not depart from normality, indicating that they were distributed normally in our sample. The internal consistency of the Japanese AQ-Short was calculated with Cronbach’s α coefficient of 0.79, indicating an acceptable internal consistency (Table 2). Cronbach’s α values of the AQ-Short subcomponents, namely, numbers/patterns, social behavior, imagination, and social skills, were all moderate to high. The internal consistency for the subcomponent routine and switching is low, but this is probably due to the small number of items in both subcomponents, and the results are consistent with previous reports (Hoekstra et al., 2011; Kuenssberg et al., 2014).
Participants’ sociodemographic characteristics.
SD: standard deviation.
Distribution of AQ-Short scores in Japanese workers.
Distribution of AQ-Short subcomponent scores in Japanese workers.
AQ-Short characteristics.
AQ-Short: an abridged version of the Autism-Spectrum Quotient.
The AQ-Short scores according to sociodemographic characteristics are presented in Table 3. Men had significantly higher AQ-Short scores than women. No significant difference was found in adjusted averages of the AQ-Short scores based on age or living state. Workers with an education level of high school or less had significantly higher AQ-Short scores than workers with an education level of junior college or higher. Workers in non-managerial positions had significantly higher AQ-Short scores than those in managerial positions. Workers from a low-income background had significantly higher AQ-Short scores than workers from a high-income background. Workers who drank rarely had significantly higher AQ-Short scores than workers who drank sometimes or daily. Non-current smokers had significantly higher AQ-Short scores than current smokers. Finally, workers with no leisure-time physical activity had significantly higher AQ-Short scores than workers with leisure-time physical activity.
Adjusted averages of AQ-Short scores or AQ-Short subcomponents scores according to sociodemographic characteristics.

SE: standard error; AQ-Short: an abridged version of the Autism-Spectrum Quotient.
This model was adjusted for age and gender. Analysis of covariance (ANCOVA) was used for the comparison of adjusted averages.
p < 0.05.
Except for one subcomponent score (routine), the association between the other subcomponent scores and gender showed the same trend as the association between total AQ-Short scores and gender. While the scores for the three subcomponents, social behavior, imagination, and social skills, did not differ based on age, younger workers showed higher AQ-Short scores for the routine and switching traits than older workers. No significant difference was found in adjusted averages of the subcomponent scores based on living state.
Except for scores for one subcomponent (numbers/patterns), workers of a lower SES had significantly higher AQ-Short scores for the other subcomponents than their respective counterparts. On the contrary, workers of a higher SES showed higher AQ-Short scores for numbers/patterns than workers of a lower SES.
With a few exceptions, the association between each subcomponent score and health-related behaviors showed the same trend as the association between total AQ-Short score and health-related behaviors. There was no difference in the routine subcomponent based on smoking habits. The numbers/patterns scores showed an opposite association for total AQ-Short scores in terms of leisure-time physical activity. Workers with no leisure-time physical activity had significantly lower numbers/patterns scores than workers with leisure-time physical activity.
Discussion
The total AQ-Short scores for the Japanese workers were normally distributed and showed a bell-shaped curve. In addition, all subcomponent traits were also normally distributed and showed a bell-shaped curve. All autistic traits were generally more prevalent in workers of a low SES, except for one particular subcomponent that was more prevalent among workers with high SES.
This is consistent with the hypothesis that “autistic traits are continuously distributed across the population” as advocated by Wing (Waterhouse et al., 1996; Wing, 1981), and with a previous report (Hoekstra et al., 2011) that sampled the Dutch general population, Dutch student population, and English student population. Our study confirmed Wing’s suggestion (Wing and Gould, 1979) with empirical data. Men had significantly higher total AQ-Short scores than women. We found no significant difference in total AQ-Short scores based on age. Thus, we replicated the findings observed in previous studies (Baron-Cohen et al., 2001; Brugha et al., 2011; Hoekstra et al., 2011; Kurita et al., 2005; Pisula et al., 2013; Wakabayashi et al., 2006) in terms of distribution of autistic traits across gender and age in Japanese workers.
Workers of a lower SES had significantly higher AQ-Short scores than their respective counterparts. Our results may reflect the fact that people with ASD are socially disadvantaged. A previous study showed only an association between ASD and low education (Brugha et al., 2011). Our study showed that workers with high total AQ-Short scores were associated with not only low education but also low income and low occupational position.
It seems that workers with low general physical activity had higher total AQ-Short scores than workers with high general physical activity. After adjustment for SES, the results remained essentially unchanged (data not shown). Previous studies showed only an association between ASD and low physical activity (Healy et al., 2017; Pan et al., 2016). Individuals with ASD are at a high risk of associated psychiatric disorders, particularly depression and anxiety (Lugnegard et al., 2011; Skokauskas and Gallagher, 2010; Sterling et al., 2008). Such comorbid conditions could explain the phenomenon that people with ASD have lifestyles characterized by social withdrawal.
All subcomponent traits were also normally distributed and showed a bell-shaped curve. Furthermore, having a particular type of autistic trait may not become disadvantageous. The results for each AQ-Short subcomponent, based on gender, were consistent with those of the total AQ-Short scores, except for the routine trait. Our results for the three autistic traits (social behavior, imagination, and social skills) based on age were consistent with that of the total AQ-Short scores. This would suggest that the lack of an association between ASD and age was consistent with there being no increase in prevalence because the causes of autism appear to be temporally constant (Brugha et al., 2011). Younger workers were found to have higher scores for the routine or switching traits than older workers. A possible explanation for this was that workers with high scores for these traits could gradually quit the company.
In general, each autistic trait was prevalent in workers of a low SES, while a particular type (numbers/patterns) was prevalent among workers of a high SES. A possible explanation was that workers with high scores for these autistic traits could be discriminated at work not because of their lack of skills but because of prejudice and lack of understanding regarding these traits. Meanwhile, Baron-Cohen et al. (1998, 2001) indicated that scientists, including mathematicians, gained significantly higher total AQ scores than both humanities and social sciences students and that Mathematics Olympiad winners scored significantly higher than male Cambridge humanities students. Chen et al. (2009) indicated that some individuals with ASD performed more superiorly in rote memory skills or visuospatial processing and suggested that restricted and repetitive behaviors were associated with the ability to concentrate. These autistic traits reported by Baron-Cohen et al. (Baron-Cohen and Wheelwright, 1999; Baron-Cohen et al., 1998, 2001, 2007, 2009) and Chen et al. (2009) resemble the numbers/patterns trait.
Concerning health-related behaviors, the results of each autistic trait were consistent with those of the total AQ-Short scores, with a few exceptions including the numbers/patterns trait. After adjustment for SES, the results remained essentially unchanged (data not shown). It is unknown why the numbers/patterns trait was an exception. However, the association with general physical activity and numbers/patterns trait was not investigated. Further studies are needed.
Limitations
Our study had several limitations. First, the AQ-Short may not be appropriate for participants with a low intelligence quotient, as it requires reading comprehension skills (Baron-Cohen et al., 2001). Therefore, our participants were limited to workers with normal intelligence. Second, all our participants were workers from the same large company, and therefore, the results may not apply to the general Japanese population. However, as workers were recruited from 12 offices located throughout Japan (from Hokkaido in the north to Kyushu in the south), our sample population was geographically distributed across Japan. Third, the accuracy of AQ-Short score in predicting ASD is important because autistic traits were measured using a self-administered test (AQ-Short) and not through individual diagnosis. The accuracy of the AQ-Short in distinguishing individuals with ASD from controls was evaluated using receiver operating characteristic (ROC) analysis, and the area under the curve was 0.97, indicating excellent test accuracy (Hoekstra et al., 2011). Furthermore, the measurement equivalence of the AQ-Short because it is a popular measure of autistic traits used frequently in individuals both with and without ASD (Murray et al., 2014) and structural validation of the AQ-short in a clinical sample of people with ASD (Kuenssberg et al., 2014). Our study focuses on ASD-related traits, that is, autistic traits, and not ASD. Fourth, our results were obtained through self-report, that is, these were from individuals who declared consuming alcohol rarely rather than actually “drank rarely.” However, if all of the participants tended to report less than the actual amount, our results would not be affected because the aim is to compare autistic traits between frequent and occasional drinkers in the study samples.
Conclusion
Our findings suggest that the five subcomponents of the autistic phenotype as well as the overall autistic phenotype are continuously distributed across Japanese workers. Gender-based differences were consistent with previous reports. No significant difference in the total AQ-Short scores among different age groups was found. In general, autistic traits were prevalent in workers of a low SES, while a particular subcomponent of the phenotype (numbers/patterns) was prevalent among workers of a high SES. Workers with low general physical activity had or tended to have higher AQ-Short scores for all subcomponent traits and the overall autistic phenotype, except for the numbers/patterns trait.
Supplemental Material
AUT716605_Lay_Abstract – Supplemental material for Distribution of autistic traits and their association with sociodemographic characteristics in Japanese workers
Supplemental material, AUT716605_Lay_Abstract for Distribution of autistic traits and their association with sociodemographic characteristics in Japanese workers by Tomoko Suzuki, Koichi Miyaki, Hisashi Eguchi and Akizumi Tsutsumi in Autism
Footnotes
Acknowledgements
The authors greatly appreciate Dr Baron-Cohen for giving permission to create their Japanese version of the AQ-Short. They express their sincere gratitude to all participants for their involvement in their studies. They also thank those who cooperated with them in the study for their sustained support during data collection and entry.
Funding
This research was supported by JSPS KAKENHI (grant number: JP16K09105 (chief: Dr Tomoko Suzuki), JP24390160 (chief: Dr Koichi Miyaki), and JP26253042 (chief: Dr Akizumi Tsutsumi)) and a Grant-in-Aid for Scientific Research on Innovative Areas (Research in a Proposed Research Area) from the Ministry of Education, Culture, Sports, Science and Technology (grant number: 21119001 (chief: Dr Norito Kawakami)), Japan.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.