
Abstract
There is a severe shortage of services for children with autism in Ethiopia; access to services is further impeded by negative beliefs and stigmatising attitudes towards affected children and their families. To increase access to services, care provision is decentralised through task-shifted care by community health extension workers. This study aimed to examine the impact of a brief training (Health Education and Training; HEAT) for Ethiopian rural health extension workers and comprised three groups: (1) health extension workers who completed a basic mental health training module (HEAT group, N = 104); (2) health extension workers who received enhanced training, comprising basic HEAT as well as video-based training on developmental disorders and a mental health pocket guide (HEAT+ group, N = 97); and (3) health extension workers untrained in mental health (N = 108). All participants completed a questionnaire assessing beliefs and social distance towards children with autism. Both the HEAT and HEAT+ group showed fewer negative beliefs and decreased social distance towards children with autism compared to the untrained health extension worker group, with the HEAT+ group outperforming the HEAT group. However, HEAT+ trained health extension workers were less likely to have positive expectations about children with autism than untrained health extension workers. These findings have relevance for task-sharing and scale up of autism services in low-resource settings worldwide.
Keywords
Autism and other developmental disorders (DD) are increasingly recognised as conditions associated with long-term burden, disability and cost, requiring global action (Kieling et al., 2011; Patel et al., 2013; World Health Organization (WHO), 2001). The global prevalence of autism is estimated to be around 0.6% (Elsabbagh et al., 2012). The prevalence of autism in sub-Saharan Africa is unknown (Elsabbagh et al., 2012; Franz et al., 2017), but prevalence studies of general mental health problems and intellectual disability in low- and middle-income countries (LMIC) suggest that these problems are at least as prevalent as in high-income countries (Maulik et al., 2011; WHO, 2008). In most LMIC, mental health and developmental problems are aggravated by a severe shortage in mental health care provision, resulting in large treatment gaps (Saxena et al., 2007).
Ethiopia is a country located in the horn of Africa with a population of almost 100 million people, half of whom are children. Our recent situational analysis of autism services in Ethiopia (Tekola et al., 2016) showed that diagnostic and educational services for children with autism are largely confined to Ethiopia’s capital, Addis Ababa, and therefore unavailable to the majority (85%) of families who live rurally. There is only one child psychiatrist working in Ethiopia; the two schools for children with autism in Addis Ababa are both highly oversubscribed with long waiting lists. The identification, care and treatment of children with autism are further hindered by stigma, negative stereotypes and misconceptions about the causes of DD and child mental illness (Abera et al., 2015; Tilahun et al., 2016). Supernatural explanatory models, for example, attributing a child’s problems to a curse or spirit possession, are common, both in caregivers of children with DD (Tilahun et al., 2016) and in parents of general population schoolchildren (Abera et al., 2015). Ethiopian caregivers of children with DD report high levels of stigma; caregivers who reported seeking help from traditional institutions and caregivers who gave a supernatural (as opposed to a biomedical) explanation for their child’s condition reported higher experienced stigma (Tilahun et al., 2016). Supernatural explanatory models of mental illness and negative attitudes towards people with mental health problems are also common among nursing staff in Ethiopia (Abera et al., 2014; Deribew and Tesfaye, 2005). Examining beliefs regarding autism among health professionals, studies in Kenya (Gona et al., 2015) and Nigeria (Bakare et al., 2009) indicate that similar negative beliefs and misconceptions about the causes of autism are common in other sub-Saharan African countries. People with religious or supernatural beliefs about causation are likely to have less tolerant attitudes towards people with mental health or developmental problems (Gureje et al., 2006). These views and beliefs may, therefore, hamper identification and successful community rehabilitation of children with autism. Consequently, it is likely that the adult community also includes many individuals whose autism goes without recognition or support.
One of the most promising strategies to address the treatment gap for children with autism and other DD is decentralisation of mental health care provision through task-shifted or task-shared care by non-specialists (Patel et al., 2013; Saraceno et al., 2007). Community health workers, referred to as health extension workers (HEWs) in the Ethiopian health system, have a great potential to be involved in decentralised care provision. To improve the general health care facilities for people living in rural areas, Ethiopia launched a community-based health services extension programme in 2003. Since then 38,000 HEWs completed a 1-year training course before starting work in rural Ethiopia. Every rural kebele (the smallest administrative unit in Ethiopia, comprising about 5000 inhabitants, half of whom are children) is assigned two HEWs. The HEWs deliver primary community health care services consisting of health promotion and prevention packages at their health post. In addition, HEWs are actively engaged in outreach services by visiting the houses of people in their community and training model families and community volunteers (Koblinsky et al., 2010). Evaluation of the initial Ethiopian health services extension programme indicated some notable successes, including a significantly higher proportion of children vaccinated against communicable diseases and an increase in the use of bed nets to prevent malaria (Assefa et al., 2009). However, there was little impact of the programme in other health areas. More importantly in the context of autism, the initial programme did not include any training on mental health or DD.
To address these concerns, the Federal Ministry of Health of Ethiopia worked with The Open University (United Kingdom) to develop the Health Education and Training programme (HEAT; http://www.open.ac.uk/africa/heat/) to upgrade the training of existing HEWs. The HEAT curriculum covers topics in child and maternal health, family planning and sexual health, environmental hygiene, communicable and non-communicable diseases. A total of 10 study sessions specifically concern mental health, though child mental health and developmental problems receive only limited attention, with virtually no content on autism spectrum disorders.
About 1300 HEWs were trained using the HEAT modules in a pilot project across the country at the launch of HEAT in 2012; since then, over 12,700 have completed the upgrading training using HEAT study materials (Federal Ministry of Health, 2016, personal communication). Following their HEAT training, we examined the experiences and remaining training needs of 104 HEWs who had just completed the HEAT pilot (Tilahun et al., 2017). The majority of surveyed HEWs were satisfied with the HEAT training materials on mental health and over two-thirds of HEWs indicated they used these study materials at least once a month in their job. However, 74% of the HEWs also indicated they would benefit from additional training on child mental health and DD. Qualitative interviews with a subsample of HEWs indicated HEWs feel they lack knowledge and skills to adequately support children with DD in their community. In response to these findings, we developed an enhanced version of the HEAT mental health training, called HEAT+. This covered a range of adult and child mental health problems and included training materials specifically focussing on autism and intellectual disability in children. In the HEAT+ research project, we surveyed the experience, knowledge and attitudes of HEWs who were trained using HEAT or HEAT+ and compared their experience, knowledge and skills with HEWs not yet trained in mental health or DD. The aim of this study was therefore to evaluate the impact of the basic and enhanced Health Education and Training (HEAT and HEAT+) materials on the beliefs and attitudes towards children with autism in rural HEWs in Ethiopia.
Methods
Study setting
The study was conducted in the Southern Nations, Nationalities, and Peoples’ Region (SNNPR), one of the 11 federal administrative regions of Ethiopia. From the Ethiopian 2007 census (Ethiopian Central Statistical Agency, 2012), SNNPR has an estimated population of around 15 million people, comprising 45 ethnic groups. The region is predominantly rural; nearly 90% of inhabitants reside in rural areas. Upon the launch of the community-based health services extension programme, 7492 rural HEWs were trained in SNNPR between 2003 and 2009 (WHO, 2010). In 2011, the first cohort of 208 HEWs from SNNPR enrolled in the HEAT training, of which 204 successfully completed the training. In 2013, a new cohort was trained using the enhanced (HEAT+) mental health training materials.
Participants
This cross-sectional study comprised three groups: (1) HEWs who completed the original HEAT mental health module (HEAT group; N = 104); (2) HEWs trained using the enhanced HEAT mental health module (HEAT+ group; N = 97); and (3) practicing HEWs not yet enrolled in the upgrading programme, who had not yet received any mental health training (untrained group; N = 108). The study participants in the HEAT and HEAT+ groups had all received their training in the study sites Hawassa or Hosanna, two of the four available training facilities in SNNPR at the time of the study. The HEAT group had completed their training on average 16 months prior to the data collection and had since returned to their local community to work. All HEAT-trained HEWs who studied in Hosanna and Hawassa (N = 116) were invited to take part in this study; complete data are available for 104 HEWs (participation rate 89.7%). HEWs enrolled in the HEAT+ training had completed the HEAT+ mental health module on average 4 months prior, but were still completing other modules of their upgrading training and had thus not yet returned to their local community. Out of the 104 HEAT+ trained HEWs invited to take part, 97 participated (93.3%). Finally, a total of 116 HEWs not yet trained in HEAT or HEAT+ were invited to take part, of which 108 participated (93.1%). All participating HEWs were female, following the policy of the Federal Ministry of Health of Ethiopia. Each HEW works alongside one HEW colleague in her local community. Working alongside a colleague who had already completed mental health training may affect a HEW’s knowledge and attitudes about autism; we therefore asked whether a HEW worked alongside a trained or untrained colleague. This information and further demographic data are provided in Table 1.
Participants’ socio-demographic characteristics in all three study groups.
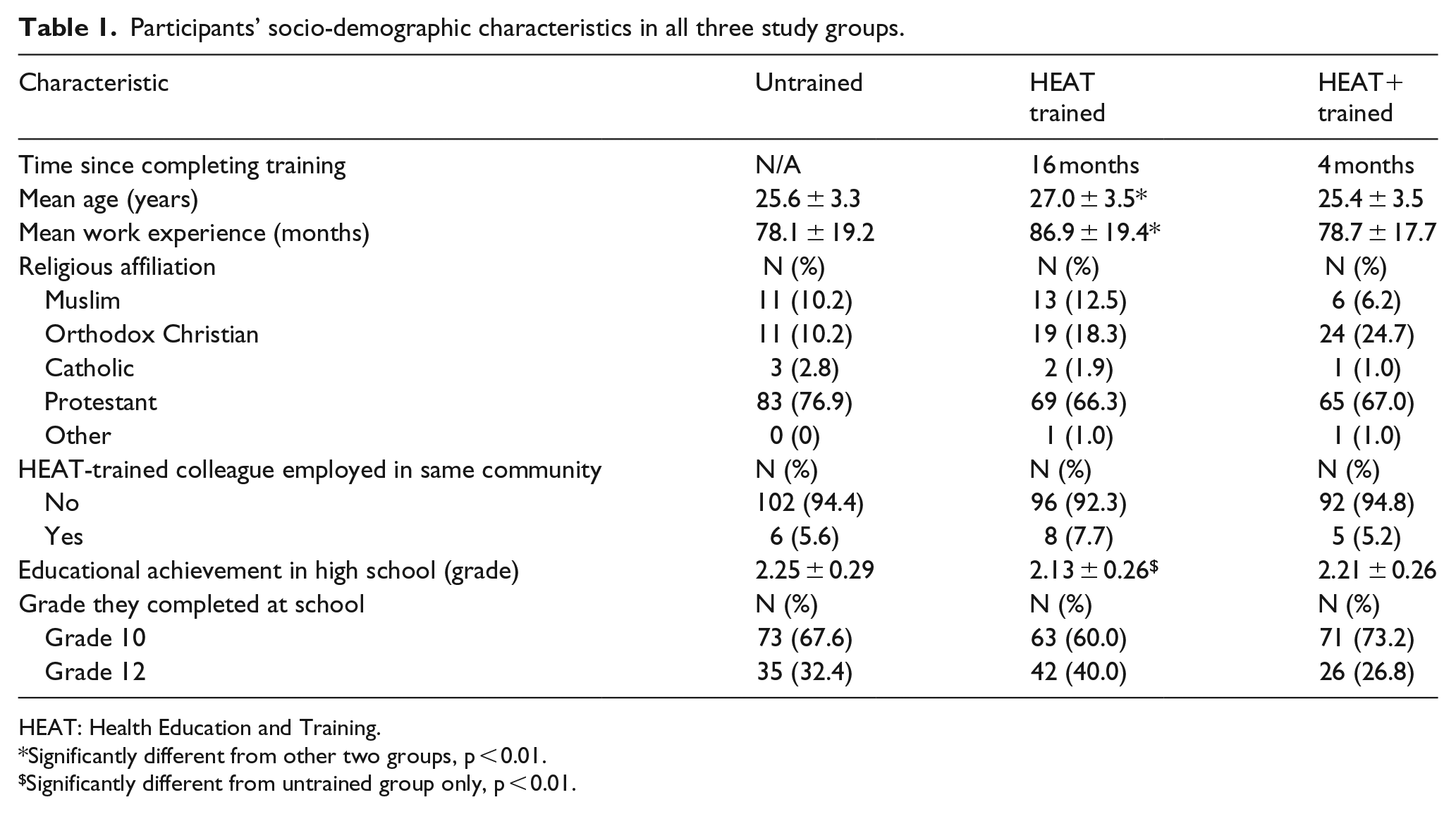
HEAT: Health Education and Training.
Significantly different from other two groups, p < 0.01.
Significantly different from untrained group only, p < 0.01.
Training
Two types of educational interventions were provided as briefly described above: (1) the basic mental health module (HEAT) and (2) the enhanced HEAT mental health module (HEAT+) of the upgrading programme for Ethiopia’s HEWs. The basic HEAT mental health training materials comprise 10 sessions, equivalent to 2 weeks of full-time study, and include a focus on mental health management, assessment and mental illness prevention strategies. One session focuses on child development and child mental health, including a discussion of developmental problems. Autism is described only very briefly, in two sentences. The HEAT training was provided through class teaching using printed module materials written in English, following the language policy of the Federal Ministry of Education; most students had access to their personal copy of the training materials (Tilahun et al., 2017).
The HEAT+ training comprised the basic HEAT materials, as well as a DVD and a mental health ‘pocket guide’. The DVD includes five short video scenarios modelling an HEW interviewing mothers of children with autism or intellectual disability, demonstrating skills in early detection, supportive counselling and problem solving. The mental health pocket guide provides a brief introduction to mental health with a main focus on detection, mental health first aid and providing support to affected families. The pocket guide includes a dedicated child section, with substantially more information on autism and intellectual disability than provided in the basic HEAT materials. It outlines the symptoms of intellectual disability and autism, provides guidance on referral, gives advice on how to approach parents and how to talk to a child with a DD, highlights the importance of checking for signs of child abuse and protecting the child from harm, gives advice on what information to provide caregivers of a child with a DD and suggests strategies to help families support their child’s development, managing limitations and challenging behaviours while building on areas of skill and promoting new skills. The pocket guide also advises on how to support integration of children with DD into the community, by giving guidance on how to organise community awareness and school-based awareness meetings. The pocket guide was prepared in English and subsequently translated to Ethiopia’s official language Amharic. The scripts for the video scenarios were written in English and then translated to and filmed in Amharic. In addition to the basic HEAT materials, HEWs in the HEAT+ group viewed the training videos as part of their in-class education and received a personal copy of the pocket guide. The tutors teaching the HEAT+ training were given copies of all HEAT+ materials a month before they delivered the training to students, allowing them to prepare their lessons.
Both the basic HEAT materials and the HEAT+ materials are open educational resources, freely available online on the Open University’s HEAT website (quick link: http://www.tinyurl.com/heatplus). All HEAT and HEAT+ resources were produced by a team of Ethiopian and United Kingdom-based experts in mental health and/or pedagogy, ensuring that the materials were culturally and contextually appropriate. The materials use clear learning outcomes directly linked to the key competencies expected of upgraded HEWs (Federal Democratic Republic of Ethiopia, Ministry of Education, 2016).
Measures
To evaluate the impact of the training, all HEWs consenting to take part in the research evaluation were asked to complete a structured questionnaire, including a written case vignette of a child with autism. The vignette described a mother concerned about her 8-year-old son who shows core symptoms of autism (lack of eye contact, limited speech and play with peers, repetitive activities and difficulty with change). The vignette also highlighted the parental love for their son to avoid any impression of family neglect. Following the presentation of the case vignette, the HEWs were asked to respond to various questions related to autism, including self-rating their general beliefs about autism and their preferred social distance (a measure of what level of intimacy and interaction they would accept) from children with autism. These questions were adapted from the World Psychiatric Association’s programme to reduce stigma and discrimination because of schizophrenia (Stuart and Arboleda-Florez, 2001). A similar questionnaire has been used to assess attitudes towards mental illness in Nigeria (Gureje et al., 2005). Adaptation was carried out through expert consensus meetings to make the questions directly relevant to autism and appropriate for the Ethiopian context. The general beliefs questionnaire comprised 10 items including questions assessing positive beliefs and expectations (e.g. ‘children with autism can make their parents proud’) as well as negative beliefs (e.g. ‘children with autism can bring bad luck on the community’). Items were assessed on a 4-point scale ranging from 0 = ‘never’ to 3 = ‘nearly always’. The social distance questionnaire comprised six items, including, for example, ‘would you feel ashamed to be seen out on the street taking care of a child with autism’. Item responses were recorded on a 4-point scale ranging from 0 = ‘definitely not’ to 3 = ‘definitely’, with higher scores indicating a greater preferred social distance from children with autism, suggesting stronger stigmatising attitudes. The survey was first piloted in five untrained HEWs in the Butajira area of SNNPR. Based on the pilot, final revisions were implemented before the data collection began.
Data collection procedure
The questionnaires were administered to HEWs through a face-to-face interview in Amharic by trained and experienced data collectors. This data collection procedure is commonly used in mental health research in Ethiopia and is appropriate for the cultural setting. Data collectors were all women who completed secondary school (10th grade) and were of similar socio-economic status to the participants to limit social desirability bias in the HEWs’ responses. Data collectors were trained over 5 days; the training focused on good interviewing skills, role plays and observed pilot interviews. The data collection was conducted at the training facilities in Hawassa and Hosanna. All study participants provided their written informed consent prior to participation. Ethical approval was obtained from the Institutional Review Board of Addis Ababa University’s College of Heath Sciences and the Open University’s Human Research Ethics Committee.
Data management and analysis
Double data entry using Epidata version 3 (Lauritsen and Bruus, 2003) was employed to reduce the risk of data entry errors. The data were then exported to SPSS version 23 (IBM SPSS Statistics 23; IBM Corp., 2015) and MPlus version 5.21 (Muthén and Muthén, 2007) for analysis. The factor structure of the adapted questionnaires was assessed in two steps, using exploratory factor analyses (EFA) and confirmatory factor analyses (CFA) in MPlus. The total sample of 309 participants was randomly split in half. Half of the sample was used to conduct the EFA. The factor structure suggested by the EFA was subsequently tested employing CFA using the second half of the sample. Modification indices were used as guidelines to examine whether the fit of the resulting model could be further improved. The overall fit of the models was evaluated using the comparative fit index (CFI) and the root mean square error of approximation (RMSEA). A good model fit is indicated by CFI values above 0.90 and RMSEA below 0.08 (Schermelleh-Engel et al., 2003). Once the best fitting models were identified, further analyses were conducted in SPSS. The internal consistency of the resulting scales was estimated using Cronbach’s alpha. Non-parametric Kruskal–Wallis test and subsequent Mann–Whitney U tests were used to examine group differences in a single item. Analyses of covariance were used to examine group differences in quantitative scales. The following four variables were included as covariates in these analyses: HEW’s age, length of work experience practising as HEW, educational achievement in high school and whether the HEW worked alongside a HEAT-trained colleague.
Results
Participant characteristics
The sample characteristics for each of the three groups are reported in Table 1. The three groups had a similar distribution of religious affiliations; similar proportions in each group had completed high school to 10th or 12th grade level, and similar proportions worked alongside a HEW colleague who had already completed the upgrading programme. The HEAT group was significantly older and had a significantly longer experience working as an HEW compared to the HEAT+ and untrained groups (p < 0.01). Moreover, the untrained group had a slightly higher average grade in high school than the HEAT-trained group (p < 0.01). No other group differences in background characteristics were observed.
Factor analyses
The 10 items assessing positive and negative beliefs towards children with autism were examined using EFA. Initial EFA indicated that one item showed little covariance with the other nine items. Item content inspection (‘Can improve their language skills with the right help’) suggested this item mainly assesses a positive belief in efficacy of an intervention, rather than a positive belief towards children with autism directly. The EFA was re-run including the nine remaining items only. The results indicated a two-factor structure: one factor comprising four items assessing positive beliefs and expectations about children with autism, and one factor comprising five negative belief items. This two-factor model was subsequently fitted to the second half of the data. The modification indices suggested that the model fit could be improved if we would allow a small tweak to our specified model: a cross-loading of one of the positive belief items on the negative belief factor (allowing for some covariation of this item with the negative belief factor). Implementing this modification resulted in a good model fit (CFI = 0.927; RMSEA = 0.064). Next, the six items assessing social distance were subjected to EFA. The EFA suggested a one-factor structure; testing this structure using CFA in the second half of the data indicated a very good model fit (CFI = 0.987; RMSEA = 0.063); there were no modification indices above the minimum value. The 4-item positive beliefs scale had moderate internal consistency (Cronbach’s α = 0.54), acceptable when taking into account the low number of items included. The internal consistency of the 5-item negative beliefs scale (α = 0.67) and 6-item social distance scale (α = 0.72) were adequate.
Impact of training on beliefs and attitudes
Tables 2 and 3 show the item-by-item responses of the participants in relation to positive (Table 2) and negative (Table 3) beliefs and stereotypes towards children with autism, while Table 4 presents the responses related to preferred social distance.
Positive beliefs and expectations about children with autism in untrained, HEAT-trained and HEAT+ trained HEWs.
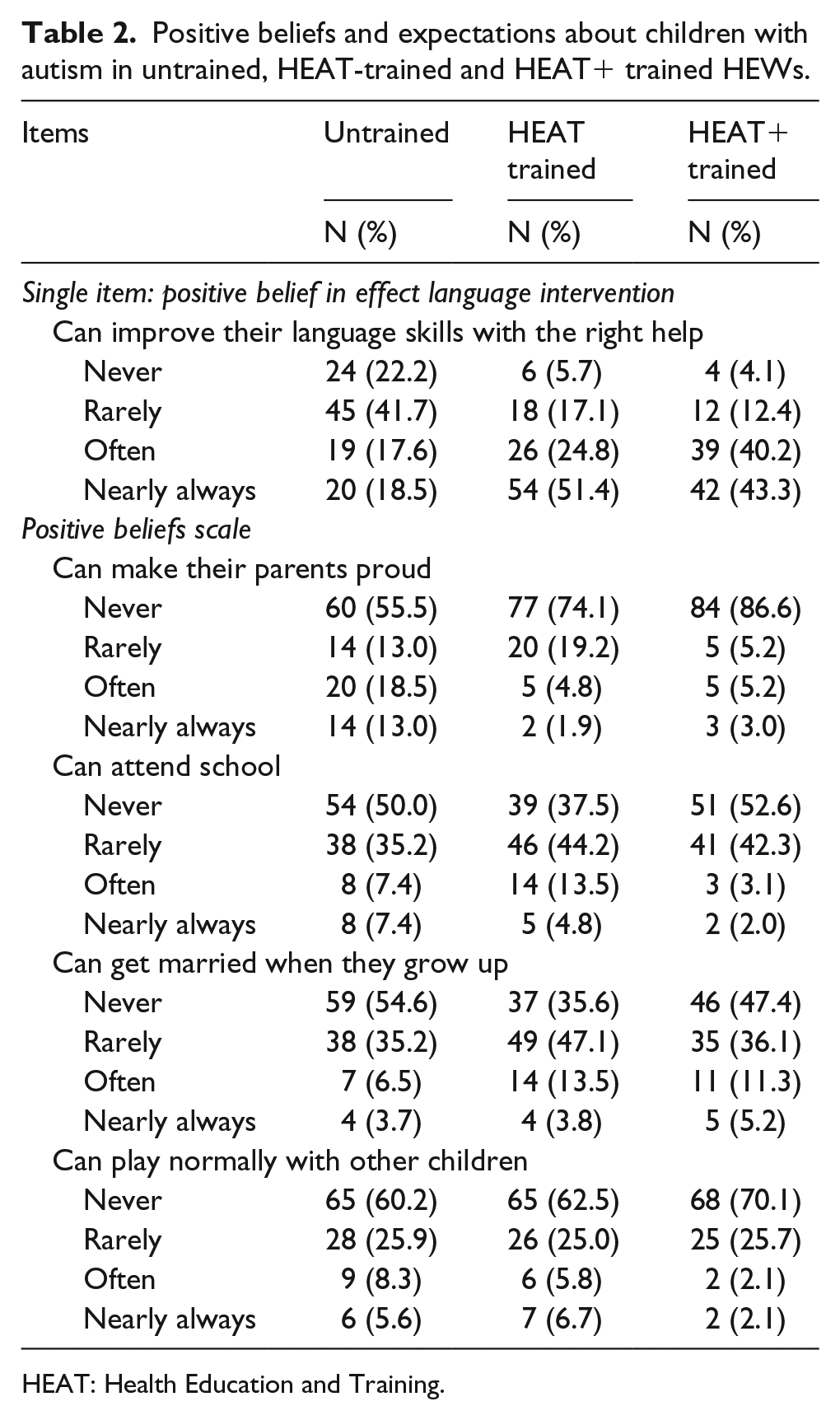
HEAT: Health Education and Training.
Negative beliefs towards children with autism in untrained, HEAT-trained and HEAT+ trained HEWs.

HEAT: Health Education and Training; HEWs: health extension workers.
Social distance towards children with autism in untrained, HEAT-trained and HEAT+ trained HEWs.
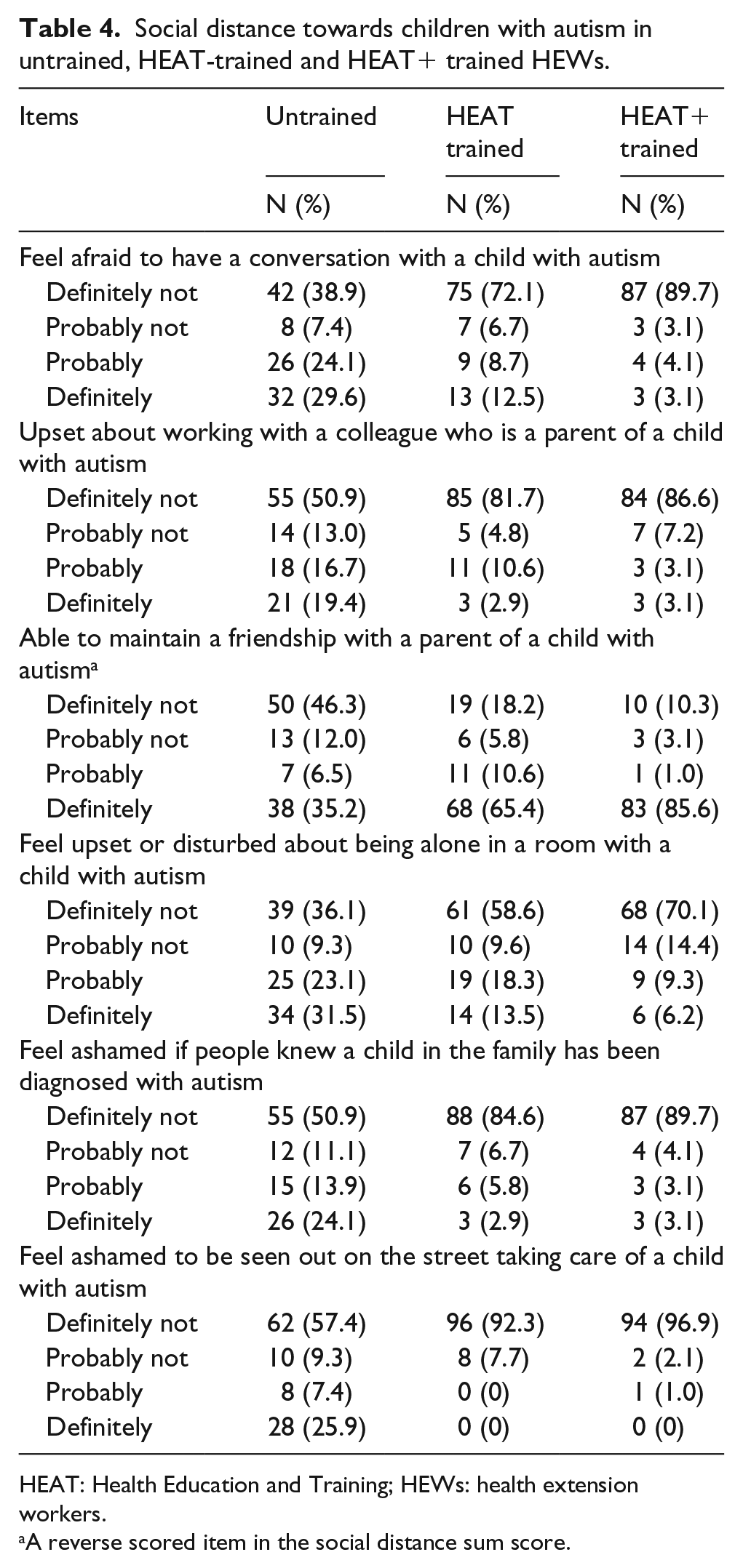
HEAT: Health Education and Training; HEWs: health extension workers.
A reverse scored item in the social distance sum score.
The groups differed significantly in their belief that a child with autism can improve their language skills with the right help (H (2) = 52.371, p < 0.001). Subsequent Mann–Whitney U tests indicated that HEAT+ trained (Z = –6.24, p < 0.001, r = –0.44) and basic HEAT-trained (Z = –6.14, p < 0.001, r = –0.42) HEWs were more likely to believe that children with autism can improve their language skills compared to untrained HEWs (Table 2). The HEAT and HEAT+ groups did not differ from each other (Z = –0.46, p > 0.05).
Figure 1 shows the mean scores and distributions of the positive beliefs (Figure 1(a)), negative beliefs (Figure 1(b)) and social distance (Figure 1(c)) scales in each of the three groups. There was a significant group effect on the positive beliefs scale (F (2, 301) = 4.57, p = 0.01, partial η2 = 0.03). Planned contrasts using Bonferroni correction for multiple comparisons revealed that the HEAT+ group had significantly lower positive beliefs scores than the untrained group (p = 0.01); none of the other group comparisons were significant. None of the included covariates had a significant effect on positive beliefs (all p > 0.05).
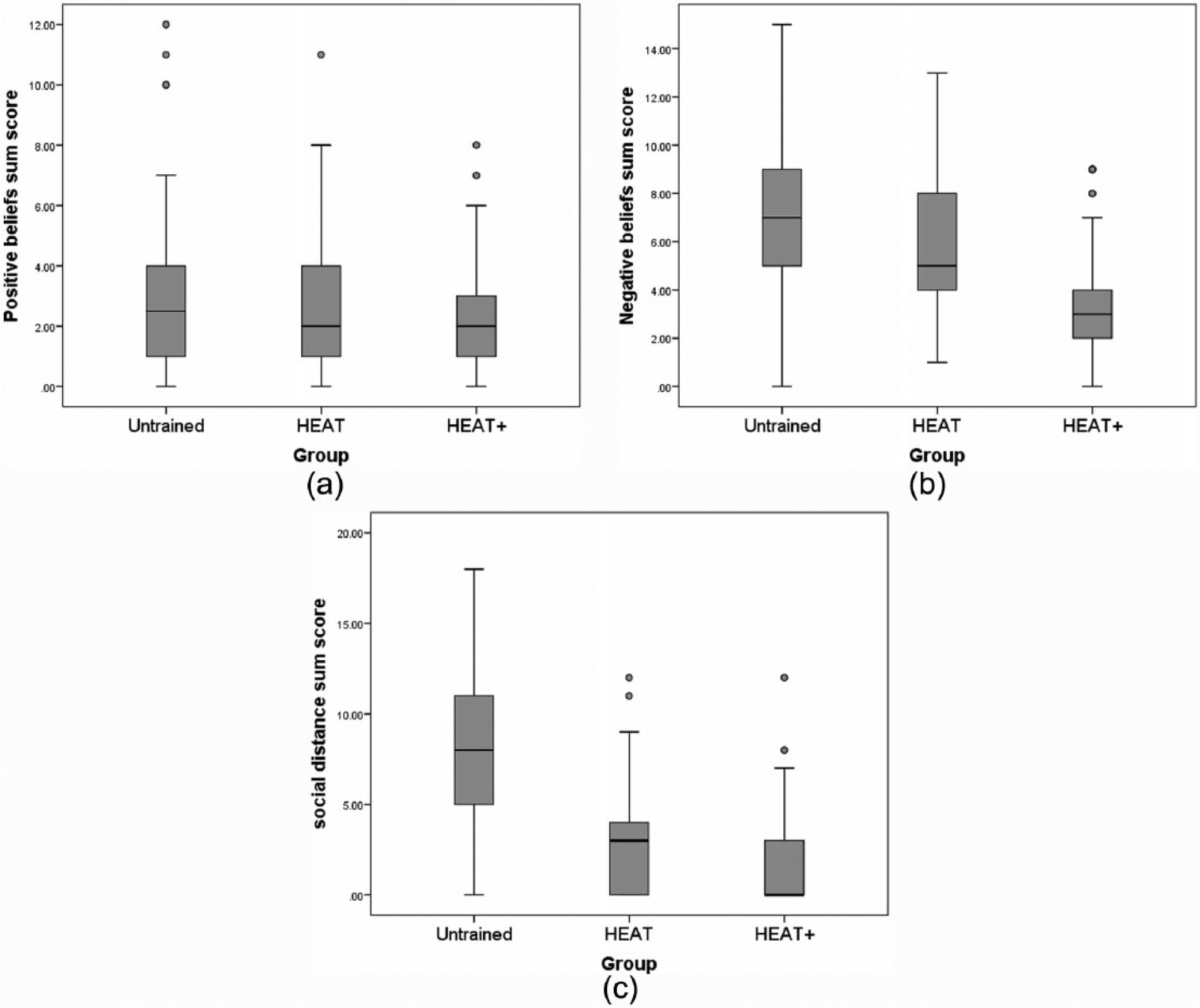
(a) Positive and (b) negative beliefs and (c) social distance towards children with autism in untrained, HEAT-trained and HEAT+ trained HEWs.
Significant group differences were observed for the negative beliefs scores (F (2, 301) = 45.91, p < 0.001, partial η2 = 0.23). This comparison took into account the effect of whether the surveyed HEW had a co-worker trained in mental health (F (1, 301) = 4.08, p = 0.04, partial η2 = 0.01); none of the other three covariates was significant (all p > 0.05). Considering all three groups together, HEWs with a HEAT-trained co-worker (N = 19) reported fewer negative beliefs. Both the HEAT (p = 0.004) and HEAT+ group (p < 0.001) showed fewer negative beliefs towards children with autism than the untrained group. The HEAT+ group in turn displayed fewer negative beliefs than the HEAT group (p < 0.001).
Significant differences were also observed between the groups’ social distance scores (F (2, 301) = 103.14, p < 0.001, partial η2 = 0.41), taking into account the effect of having a trained or untrained HEW co-worker (F (1, 301) = 4.99, p = 0.03, partial η2 = 0.02). None of the other covariates was significant (all p > 0.05). Overall, HEWs with a trained co-worker reported greater social distance. Considering this covariate separately for each group revealed that this effect was only significant in the group of HEWs untrained in mental health (p = 0.033). Taking the effect of this covariate into account, both the HEAT (p < 0.001) and the HEAT+ group (p < 0.001) showed decreased social distance towards children with autism compared to the untrained group; the HEAT+ group displayed a smaller preferred social distance than the HEAT group (p = 0.017).
Discussion
To our knowledge, this is the first study in Africa that provides evidence of the impact of both a basic and enhanced educational intervention on the beliefs and attitudes of community health workers towards children with autism. We find that both educational approaches have a significant impact in improving attitudes and negative beliefs, with more mixed findings regarding positive beliefs about children with autism.
Impact of training on positive beliefs and expectations
Compared to untrained HEWs, both the HEAT+ and the HEAT-trained groups of HEWs were more likely to think that children with autism can improve their language skills with the right help. While two-thirds of the HEWs not yet trained in mental health and DD thought children with autism will never or rarely improve their language with the right help, only a minority of HEAT (23%) and HEAT+ (16%) trained HEWs had such low expectations of the efficacy of a language intervention.
HEAT+ trained HEWs were less likely to have positive expectations about children with autism, for example, that they can make their parents proud, can attend school, can get married when they grow up and can play normally with other children. This unexpected finding may perhaps be explained by the exposure of HEWs in rural Ethiopia to predominantly severe cases of autism, as well as the direction of our training materials towards cases with severe symptoms of DD. The training materials were developed based on our previous research and clinical experience in Ethiopia. Identified children with autism in Ethiopia nearly always have comorbid intellectual disability (Tilahun et al., 2016), and tend to have a classic form of autism, with no or limited speech, and frequent additional challenging behaviours such as aggression (Hoekstra et al., 2017). To make the training directly relevant to rural Ethiopian context, the HEAT+ materials primarily characterised the difficulties of children with classic autism. Although areas of skill were mentioned, the predominant emphasis on problems may have somewhat limited the scope for HEAT+ trained HEWs to formulate more positive expectations of outcomes, especially given the context in which the HEWs work, in rural settings where intervention services are unavailable (Tekola et al., 2016). The limited positive expectations of HEAT+ trained HEWs may reflect not only their improved knowledge about autism (compared to the other two groups who received little or no autism-specific training) but also the practical reality that severely affected children are unlikely to get married later, and unlikely to fit in mainstream education, in the absence of specialised autism education or behavioural intervention services (Tekola et al., 2016). Our finding of no difference between the HEAT and untrained group is consistent with a number of previous mental health education studies that observed no significant change in positive attitudes or beliefs in a positive outcome for mental health patients in community health workers (Armstrong et al., 2011; Makanjuola et al., 2012) and occupational health students (Penny et al., 2001) after training.
Impact of training on negative beliefs
Compared to HEWs untrained in mental health, both HEAT and HEAT+ trained HEWs were less likely to endorse negative beliefs relating to children with autism. The HEAT+ trained group in turn endorsed fewer negative beliefs than the HEAT-trained group. HEWs who had a HEAT-trained co-worker (irrespective of group) were also less likely to report negative beliefs. Importantly, HEAT or HEAT+ trained HEWs were unlikely to believe that children with autism ‘need to be chained up at home’, while 18% of untrained HEWs thought this would ‘often’ or ‘nearly always’ be needed. Chaining and beating children with DD is still common in Ethiopia (Tilahun et al., 2016); it is thus encouraging to see that a brief training appears to reduce the belief in this practice.
The effectiveness of the HEAT and HEAT+ programme to change negative beliefs is in keeping with previous mental health education intervention studies in health workers (Li et al., 2014, 2015; Liu et al., 2016; Mansouri et al., 2009), occupational health students (Penny et al., 2001) and young people (Yamaguchi et al., 2011). One explanation of the greater impact of HEAT+ compared to basic HEAT may be the use of videos in the training. Previous mental health intervention education studies suggest that video-based education is more effective in changing attitudes than lecture-only education (Clement et al., 2012; Yamaguchi et al., 2013). An alternative explanation may be that the effect of basic HEAT training is reduced in this study as the training was provided 16 months prior to data collection (in contrast to HEAT+, which was provided 4 months prior). Previous studies suggest that positive effects of mental health training may decline over time (Baxter et al., 2001; Yamaguchi et al., 2011).
Impact of training on social distance
Both the HEAT and the HEAT+ group showed reduced preferred social distance towards children with autism compared to the untrained group, suggesting decreased stigmatising attitudes. The HEAT+ group displayed a lower preferred social distance than the HEAT group. In total, 50% of the HEAT+ HEWs obtained a score of zero on the social distance scale, suggesting they have no need for social distance towards children with autism. The effect of the intervention is in keeping with previous reports that examined changes in the social distance towards people with mental health problems in community health workers (Li et al., 2014, 2015), police officers (Hansson and Markström, 2014) and young people (Yamaguchi et al., 2011). The results are also consistent with previous reports that video-based training is more effective in reducing social distance than lecture-only methods (Clement et al., 2012; Yamaguchi et al., 2013).
Somewhat counterintuitively, HEWs who had a HEAT-trained co-worker reported greater preferred social distance. Further analyses exploring the effect of this covariate per group showed that the effect was only significant in the untrained group: HEWs untrained in mental health who had a HEAT-trained co-worker indicated a preference for greater social distance towards children with autism. This finding may suggest that gaining some limited mental health insights through working with a trained colleague, in the absence of personal education on this topic, may increase awareness of some mental health-related issues (e.g. the importance of personal safety) without providing a full picture of mental health and DD. It also illustrates the complex trajectory of learning that HEWs embark upon when they start to learn about autism. There is not a straightforward linear acquisition of knowledge and understanding, but a ‘bumpy’ trajectory in which some attitudes go backwards before they can go forward. It is important to note that only a small subsample of HEWs had a HEAT-trained colleague, therefore these covariate results should be interpreted with care.
Limitations
Our study has some limitations. First, the study only included HEWs from SNNPR; views expressed by our participants may not reflect views of HEWs working in other regions. However, stigma and misconceptions about autism are widespread in sub-Saharan Africa (Bakare et al., 2009; Gona et al., 2016; Ruparelia et al., 2016), suggesting that our findings may apply more widely across Ethiopia and be relevant to settings elsewhere in Africa. Second, although we tried to limit social desirability bias by employing independent data collectors of similar socio-economic status to the participants, it is conceivable that socially desirable responding may have played a role. Against this interpretation, the HEWs who took part in our initial evaluation of HEAT (Tilahun et al., 2017) appeared open to share their opinion on what they did not like about the programme (e.g. dissatisfaction that the original HEAT materials were only available in English, rather than Amharic). A third limitation is that our groups were not perfectly matched: the HEAT group was significantly older and had longer work experience as HEW compared to the other two groups, and the untrained group had a slightly higher mark in high school compared to the HEAT group. Moreover, the time lag in between the survey and the HEAT and HEAT+ training was different: the HEAT group had completed their training 16 months prior, while the HEAT+ group had completed their training only 4 months prior. Differences between the HEAT and HEAT+ group may thus also be explained by this time lag difference. Fourth, the HEAT+ materials included both a DVD and a mental health pocket guide. From our study, we cannot deduce whether it was the exposure to video materials or access to the pocket guide or both that generated the impact in the HEAT+ group. Fifth, this study did not include a comparison in beliefs and attitudes pre- and post-training. Sixth, this study did not consider whether the training had a direct impact on children with autism and their families. Our study is limited to self-reported beliefs and attitudes; future studies are warranted to examine whether these self-reported changes in beliefs and attitudes translate into tangible differences for families with children with autism, for example, in terms of increased identification of children with autism, and decreased stigma experienced by families. Moreover, it would be useful for future studies to explore in more detail how the training tools were used in practice and which aspects of the training were most important in affecting change. Finally, the training evaluated in this study was brief and primarily focused on identification of children with DD, raising awareness in the community, decreasing stigma and promoting community rehabilitation. The 2-week-long training did not allow for inclusion of comprehensive guidance on the use of social communication intervention strategies to support the child’s development. In an ongoing project, we are piloting the feasibility and acceptability of a parent skills training programme for caregivers of children with DD; if evaluated positively, this training could help address the lack of available intervention services for children with DD in rural Ethiopia.
Implications
Our finding that a brief training on mental health and DD is associated with decreased negative beliefs and an increased willingness to have contact with children with autism and their parents bodes well for the role community health workers could play in decreasing stigma in the community and in community rehabilitation for children with DD. Apart from health prevention and treatment activities, a main responsibility of Ethiopian HEWs concerns outreach services, including home visits and raising health awareness in their local community. Decreased negative beliefs among HEWs may contribute to decreased stigma and negative beliefs in the community as a whole; decreased social distance from HEWs to families with a child with autism is likely to facilitate community rehabilitation, for example, through the use of non-specialist workers to administer psychosocial interventions in the community (Patel et al., 2013).
The mixed effects of the HEAT+ training on positive expectations about children with autism highlights the need for carefully designed educational interventions, taking into account the local practical and sociocultural context. The finding of a stronger effect of HEAT+ compared to HEAT training (with the caveat of the greater time lag in the HEAT group) echoes the emerging finding in mental health education research that different forms of training do not all create the same effect, and video presentations may be an especially powerful training method to reduce stigma, especially in training situations where direct social contact is not feasible (Clement et al., 2012; Yamaguchi et al., 2013).
The HEAT and HEAT+ study materials are open educational resources that are free to be adapted and used elsewhere. Given that similar challenges related to autism and mental health are reported elsewhere, the lessons learned in this study are likely to have relevance for training community health workers in other low-resource settings. A recent review highlighted the lack of evidence for interventions to reduce mental health-related stigma conducted in LMIC (Thornicroft et al., 2016). Our findings are thus likely to be relevant to addressing stigma relating to a broader range of mental health and developmental conditions too.
Conclusion
This study suggests that a 2-week training course on mental health and DD has a significant impact on decreasing community health workers’ negative beliefs and social distance towards children with autism and their parents. Training delivered in a widely used Ethiopian language, including video materials and a pocket guide, proved especially effective in decreasing negative attitudes and social distance, though was unsuccessful in increasing positive attitudes. Future research needs to investigate how beliefs in a positive outcome can be preserved while developing an increasing awareness about autism in challenging low-resource settings. The findings presented here are likely to be relevant for task-sharing and scale up of services for children with DD in low-resource settings worldwide.
Supplemental Material
AUT730298_Lay_Abstract – Supplemental material for Ethiopian community health workers’ beliefs and attitudes towards children with autism: Impact of a brief training intervention
Supplemental material, AUT730298_Lay_Abstract for Ethiopian community health workers’ beliefs and attitudes towards children with autism: Impact of a brief training intervention by Dejene Tilahun, Abebaw Fekadu, Bethlehem Tekola, Mesfin Araya, Ilona Roth, Basiro Davey, Charlotte Hanlon and Rosa A Hoekstra in Autism
Footnotes
Acknowledgements
The authors gratefully acknowledge Addis Ababa University and The Open University for technical support. We are also thankful to the study participants for their voluntary participation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by an Autism Speaks GAPH grant (#7770).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.