
Abstract
Comparison of oral health status, dental needs and dietary habits of children with autism and their healthy siblings. In this cross-sectional study, oral hygiene measures, sugar consumption and dental examination of 58 Pakistani children with autism spectrum disorder were assessed and compared to 27 of their siblings without autism spectrum disorder. Questionnaires were distributed to their parents regarding oral hygiene measures, dietary habits and past dental experiences. Clinical examination for the presence of dental caries, periodontal disease or parafunctional habits was carried out and findings were associated with the mother’s education. Children with autism had a higher incidence of caries (50%) as compared to their healthy siblings (22.2%). Significant differences were observed between the groups regarding frequency of brushing and independent brushing. Dental plaque was observed on anterior teeth in 24% children with autism spectrum disorder as compared to 14% in the control group. Trauma due to self-injurious behaviour and bruxism was also recorded and compliance during clinical examination was noted in children with autism spectrum disorder. There was no significant difference in sugar consumption between children with autism spectrum disorder and their healthy siblings. Children with autism had greater dental needs and were more prone to developing dental problems as compared to their healthy siblings.
Introduction
Autism spectrum disorder (ASD) is a complex, lifelong neurodevelopmental disorder that is diagnosed in children at a very early age. It primarily affects communication, socialization and cognition of the child (Amaral et al., 2008). The child may have impaired social inter-action, limited interests and repetitive behaviour (Friedlander et al., 2006; Imran et al., 2011). In recent years, ASD has shown an increase in prevalence. The American Academy of Pediatrics has reported a prevalence rate of 1 out of 91 children in the age group of 3–17 years (Kuhaneck and Chisholm, 2012). Although the exact cause of ASD is not known, research has largely supported the claim that it is a combination of developmental, environmental and especially genetic factors (Kuhaneck and Chisholm, 2012).
It has been reported that children with ASD generally prefer sweet, soft and sticky food and therefore are more susceptible to dental caries (Lu et al., 2013). In addition, failure to maintain oral hygiene without assistance can further complicate matters, as the dexterity required for brushing can be lessened due to weakened oral musculature (Klein and Nowak, 1999). Moreover, lack of oral hygiene measures may also predispose these children to periodontal diseases (Gandhi and Klein, 2014).
Though the dental health needs of children with autism are similar to those of other children, it is more challenging to provide them with effective dental treatment (DeMattei et al., 2007). Children with ASD are more likely to feel anxious in an unfamiliar dental environment and may be non-compliant and uncooperative from the start of the dental visit (Gandhi and Klein, 2014). In addition, limited verbal communication, unusual and exaggerated response to sensation, possible avoidance of social contact by these children and inexperience with autism on part of the clinician may make the dental visit unpleasant for a child with autism (Kuhaneck and Chisholm, 2012).
There is no published data on the prevalence of oral health problems in children with autism in Pakistan. This study aims to identify the causative risk factors for developing dental problems in Pakistani children with ASD. Another significant feature of this study is that to exclude the effects of confounding variables like mother’s education and socio-economic status, healthy siblings of the children with autism were included as controls. The hypothesis put forward is that there is a difference in the dental health problems between children with autism and their siblings without autism.
Materials and methods
This cross-sectional comparative study was conducted at the Autism Resource Centre (ARC), Rawalpindi, Pakistan, between September and December 2016. A formal permission to conduct the study was obtained from the director of ARC. Informed consent was obtained from the mothers of the children who were enrolled for the study.
Study sample
Children in the age bracket 2–10 years and whose mothers consented to be included were enrolled. A total of 85 children participated in the study, of which 58 had ASD and 27 were their healthy siblings (control group). Both groups fulfilled the criteria of similarity of age and socio-economic status. Data were collected using the following methods.
Questionnaire
A questionnaire was prepared to inquire about the oral hygiene measures (tooth brushing, frequency and dependency of child for brushing on parents), dietary pattern (frequency of sugar consumption), past dental experience and habits (self-injurious behaviour/oral sensory issues). The level of mother’s education was also recorded. The questionnaire was filled by the mothers when they accompanied the children and were also available for comment. In rest of the cases, the questionnaire was sent to their homes for filling.
Examination
The oral examination was conducted by two trained dentists at ARC. All children (study and control group) were examined by seating them in a comfortable chair under natural light using disposable dental examination kits in the presence of their caregivers. A clinical record sheet was developed to document the findings of the examination. During examination, the ‘Tell-Show-Feel and Do’ technique was used with all children (El Khatib et al., 2014). Examination was done to assess the presence of plaque on the anterior teeth, caries and restorations, signs of bruxism, soft tissue injuries, gingival status and oral defensiveness. Assessment was done on the basis of the absence or presence of an oral condition.
Score 0 indicated the absence and score 1 indicated the presence of the condition. A score of 10 was given for any condition requiring a dental visit and was designated as Urgent Need of Care (UNC). The compliance and level of cooperation of children with ASD was assessed and scored on a level from 0 to 7, depending on the level of cooperation during examination. A score 0 indicated complete compliance with the examiners and 7 represented aggressive refusal (DeMattei et al., 2007). All the examinations were done by the same person to eliminate any error and to ensure consistency of results. Time out was given to the children not willing to be examined and recalled after they had settled down. This study conforms to the Strobe Guidelines.
Data analysis
Statistical analysis was done using Statistical Package for Social Sciences (SPSS) version 21. The p value < 0.05 was taken as significant. The data were described using frequencies and percentages for categorical variables. Pearson Chi-square test was used to compare the differences between the two groups. When the numbers in any category were less than 5, Fisher’s exact test was used.
Results
The study group comprised 58 children with autism including 46 males and 12 females. Their ages ranged from 2 to 10 years with a mean of 5 years and 4 months. In the 27 controls, there were 17 males and 10 females. The ages of the controls also ranged from 2 to 10 years with a mean of 5 years and 6 months.
The results of the responses to questions asked in the survey are given in Table 1. The frequency of brushing and independent brushing in the study and the control group was significantly different (p < 0.005). In the study group, 37/58 (64%) of children with ASD brushed their teeth once and 5/58 (8.6%) brushed twice. Out of those who were brushing, 48/58 (82.7%) of children with ASD were not brushing their teeth independently as compared to 6/27 (22.2%) in the control group (p < 0.001). The majority in both groups (41/58 in the study and 24/27 in the control group) were using toothbrush and toothpastes. The overall sugar exposure was not significantly different between the two groups. An alarming majority of children with ASD (47/58, 81%) had never been to a dentist and out of the 19% who had visited, 54.5% encountered an unpleasant experience.
Frequency of responses given to questions asked in the survey and their associated p value.
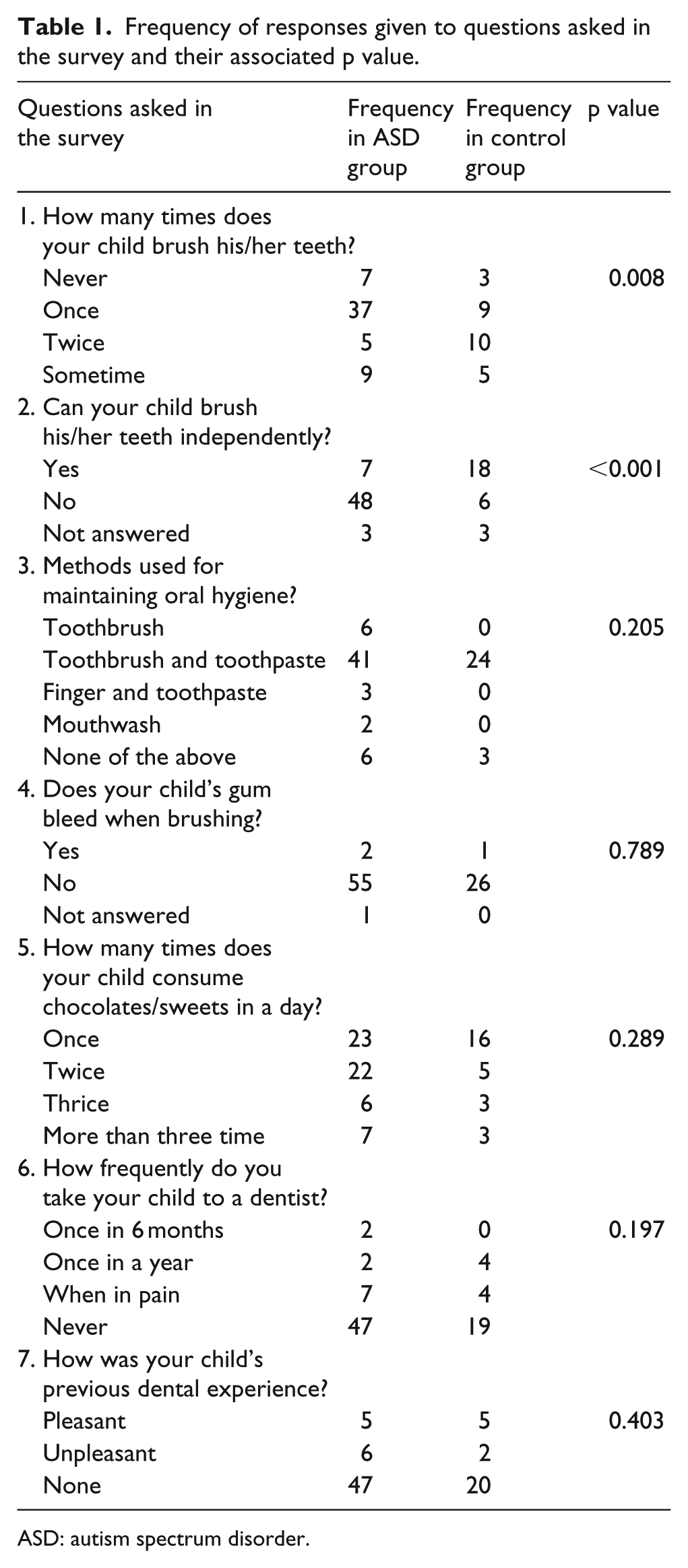
ASD: autism spectrum disorder.
The results of oral examination are summarized in Figure 1. The overall prevalence of dental caries among children with ASD was 50% (29/58) as compared to 22.2% (6/27) in their siblings (p < 0.05). The presence of plaque was seen in 15/58 (25.9%) of children with ASD as compared to 4/27 (14.8%) in the control group. Bruxism was observed in 6/58 (10.3%) of the children with ASD and none in the control group. Soft tissue injuries including mouth ulcers were recorded in only 2/58 of the children with ASD.

Frequency of various dental pathologies in the ASD and the control groups.
Out of the 58 mothers surveyed, 24 (41%) had a professional degree, 26 (45%) were graduates, 7 (12%) had primary-level education and 1 (1.7%) were uneducated. In the 24 most educated mothers, 19 (77%) had children who were brushing once or twice a day and only 5 (18%) were allowing sugary diet thrice or more in a day. Likewise, caries was seen in only 13/39 (33.3%) children in this group. Caries was seen in the children of 13/34 (38%) graduate mothers, 7/9 (78%) mothers with primary education and 2/3 (67%) uneducated mothers. Level of compliance encountered during examination of children with autism as assessed by the examiners is given in Figure 2.

Level of compliance as assessed by the examiners in children with ASD.
Discussion
ASD is now considered as one of the most rapidly increasing disabilities in children (Imran et al., 2011). However, it is not yet known whether this increase in ASD is attributed to improved awareness or whether there is a real increase in the number of children with autism. The literature shows that children with autism may have difficulty in brushing their teeth in addition to poor oral hygiene (DeMattei et al., 2007). This study was conducted at the ARC on a group of children with ASD and their healthy siblings to assess the dental health status and dental needs of children with ASD. The 2- to 10-year age bracket was chosen to allow assessment of dental problems at different developmental stages and also represented all the children in the Early Intervention Programme in the centre.
Autism being a behavioural disorder is often associated as being a risk factor for dental caries (Namal et al., 2007). Although there is no published data on caries prevalence in children with autism in Pakistan, the general consensus is that they have many unmet dental needs. Children with ASD may have difficulty in brushing their teeth independently leading to compromised oral hygiene (DeMattei et al., 2007). In addition, these children prefer food which is sweet and sticky (Lu et al., 2013). Our results clearly show that caries was more common in children with ASD as compared to their normal sibling controls. We used normal siblings as controls to exclude the confounding variables like mother’s education and socio-economic status. It appears that the main reason for the increased frequency of caries in our children with ASD is the lack of frequent brushing and second the child’s inability to perform brushing independently and adequately. The children with ASD may have a strong reaction (hypersensitivity) to the odour, taste and texture of toothpastes during brushing (Gandhi and Klein, 2014). This view is in line with a number of studies done to understand sensory processing in children with ASD (Gandhi and Klein, 2014; Kuhaneck and Chisholm, 2012).
We did not see any significant difference in sugar consumption between the children with ASD and their healthy siblings. Similar results have also been reported in a study done in Egypt (El Khatib et al., 2014). Higher caries rate was also seen in another study done for children attending autism centres in Dubai and Sharjah (Jaber, 2011). Desai et al. (2001) also stated that caries experience was higher in children with autism in a study done in Melbourne. However, children with autism are more likely to be ‘searching for food’ to comfort themselves when anxious or confused (O’Brien and Whitehouse, 1990). Moreover, these children tend to ‘pouch’ food in their mouth instead of swallowing (Jaber, 2011). This can lower the salivary pH and increases their susceptibility to dental caries (Stookey, 2008).
Parents, especially mothers, were an integral part of this study. Not only did they complete the questionnaires, but they also gave insight into the problems their children with ASD experienced due to neglected dental care. A significant association between mother’s education and frequency of brushing was observed. The majority (86%) of mothers were professionals or graduates; 77% of professional mothers regularly brushed their children’s teeth at least once or twice regardless of whether or not their child had ASD, compared to the less-educated mothers.
The responses given by educated mothers also showed that they recognized the importance of regular tooth brushing combined with lower frequency of sugar intake as a prerequisite for controlling caries (Harris et al., 2004). This was also shown by the lack of any significant difference in sugar consumption between the children with ASD and their normal siblings. The use of refined sugars in the form of chocolates and candies are less popular in the typical Pakistani culture as the staple diet of people of this region includes rice and wheat.
Bruxism is also one of the oral health problems experienced by children with ASD (Gandhi and Klein, 2014; Muthu and Prathibha, 2008). A similar concern is soft tissue injury, which may be due to self-injurious behaviour of some children (Cooper et al., 2009). Data suggest that 10% of children with ASD had bruxism compared to none in the control group. Moreover, no self-inflicted behaviour was reported by parents of children with ASD in this study. However, lip ulcers were still observed in 3% of children with ASD. A low prevalence of behavioural problems in these children could be attributed to the early intervention therapy provided to them at the centre. The results clearly reflect the widely documented fact that early and integrated therapeutic programmes can help manage behaviour in autistic children (Gandhi and Klein, 2014).
This study also assessed the level of cooperation of children with ASD during the dental examination. Interestingly, children who had been enrolled in the centre for the longest duration were the most compliant. The majority (45%) of the children opened their mouth only and 17% allowed the clinician to lift the lip; 17% refused the dental examination passively and 2% refused aggressively. In the end, it was observed that of all the children with ASD, only 19% had visited a dentist, after experiencing pain. Those who visited had to face many difficulties either due to the child’s poor cooperation, lack of awareness and attitude of dentist or a long waiting time. This was alarming as they had many unmet dental needs as compared to their siblings who had also seldom visited the dentist.
The limitation of this study was that it was conducted at only one centre and therefore the sample size was small, so results cannot be extrapolated for the entire population. Therefore, it is recommended to conduct similar studies nationwide. It is also recommended to provide professional oral health care services in special schools at subsidized rates to these children to enable early detection of oral health problems. In addition, we recommend the development of educational workshops for the dentist, parents and caregivers to improve their skills in handling these individuals.
Conclusion
Carries and dental plaque were significantly more common in children with ASD as compared to their healthy sibling controls. The main reason for the higher incidence of dental problems in ASD may be the lack of brushing and failure to do adequate teeth brushing independently. There was no significant difference in sugar consumption between the children with ASD and their healthy siblings. Mother’s education was important in implementing frequent and adequate teeth brushing in children with ASD and preventing dental caries and plaque formation. With the increase in number of children with ASD being diagnosed, dental surgeons must be aware of ASD in order to give proper treatment to their patients.
Supplemental Material
AUT730299_Lay_Abstract – Supplemental material for Oral assessment of children with autism spectrum disorder in Rawalpindi, Pakistan
Supplemental material, AUT730299_Lay_Abstract for Oral assessment of children with autism spectrum disorder in Rawalpindi, Pakistan by Fatima Suhaib, Asfia Saeed, Hashmat Gul and Muhammad Kaleem in Autism
Footnotes
Acknowledgements
The authors would like to thank the children and parents who participated in this study. They are also obliged to Ghazal Nadeem and Maria Iftikhar of Autism Resource Centre Rawalpindi for facilitation in data collection. The help of Dr Suhaib Ahmed for useful suggestions in study design and preparation of manuscript is also greatly acknowledged. Dr Shahreen Zahid Khan is also acknowledged for her suggestions in statistical analysis. There is no funding to be reported for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.