
Abstract
Several studies have suggested an association between vitamin D in childhood and autism spectrum disorder. No prospective studies have evaluated whether lower vitamin D levels precede ASD diagnoses – a necessary condition for causality. The objective of this study was to prospectively evaluate whether vitamin D serum levels in early childhood was associated with incident physician diagnosed ASD. A prospective cohort study was conducted using data from preschool-aged children in the TARGet Kids! practice-based research network in Toronto, Canada, from June 2008 to July 2015. 25-hydroxyvitamin D concentration was measured through blood samples and vitamin D supplementation from parent report. Autism spectrum disorder diagnosis was determined from medical records at follow-up visits. Covariates included age, sex, family history of autism spectrum disorder, maternal ethnicity, and neighborhood household income. Unadjusted and adjusted relative risks and 95% confidence intervals were estimated using Poisson regression with a robust error variance. In this study, 3852 children were included. Autism spectrum disorder diagnosis was identified in 41 children (incidence = 1.1%) over the observation period (average follow-up time = 2.5 years). An association between 25-hydroxyvitamin D concentration and autism spectrum disorder was not identified in the unadjusted (relative risk = 1.04, 95% confidence interval: 0.97, 1.11 per 10 nmol/L increase in 25-hydroxyvitamin D concentration) or adjusted models (adjusted relative risk = 1.06; 95% confidence interval: 0.95, 1.18). An association between vitamin D supplementation in early childhood and autism spectrum disorder was also not identified (adjusted relative risk = 0.86, 95% confidence interval: 0.46, 1.62). Vitamin D in early childhood may not be associated with incident physician diagnoses of autism spectrum disorder.
Autism spectrum disorder (ASD) is a complex neurodevelopmental condition characterized by impairment in social interaction and communication, as well as restricted and repetitive behaviors and interests (American Psychiatric Association, 2013). ASD affects more than 1% of children in North America (1 in 94 in Canada and 1 in 68 in United States) (Ouellette-Kuntz et al., 2014; Wingate et al., 2014). Factors associated with ASD, or its diagnosis are mostly non-modifiable such as male sex, preterm birth, ethnicity, socioeconomic status, older parental age, genetic factors, and a family history of ASD (Anagnostou et al., 2014; Becerra et al., 2014; Bhasin and Schendel, 2007; Croen et al., 2002, 2007; Durkin et al., 2010; Huguet et al., 2013; Keen et al., 2010; Kolevzon et al., 2007; Sandin et al., 2014; Williams et al., 2008; Wingate et al., 2014).
There has been interest in vitamin D as a possible modifiable risk factor for ASD because of its hypothesized role in the development and function of the brain (Gentile et al., 2013; Kočovská et al., 2012; McGrath et al., 2004). Vitamin D is known to affect neurotransmitter expression, neuronal cell differentiation, axonal growth, and calcium signaling as well as the production of neurotrophic factors important to the developing brain (Brewer et al., 2001; Cui et al., 2007; Eyles et al., 2013; Ibi et al., 2001; Marini et al., 2010).
Results from cross-sectional and case-control studies, in addition to a systematic review and meta-analysis, have identified lower serum 25-hydroxyvitamin D (25(OH)D) concentration among children with ASD raising the possibility that low vitamin D levels in early childhood may be related to ASD diagnosis (Adams et al., 2011; Bakare et al., 2011; Bener et al., 2014; Du et al., 2015; Fernell et al., 2010, 2015; Gong et al., 2014; Grant and Cannell, 2013; Grant and Soles, 2009; Humble et al., 2010; Kočovská et al., 2014; Lips, 2004; Meguid et al., 2010; Molloy et al., 2010; Mostafa and Al-Ayadhi, 2012; Neumeyer et al., 2013; Saad et al., 2015; Tostes et al., 2012; Ugur and Gurkan, 2014; Wang et al., 2015; Whitehouse et al., 2013). However, these findings may be a consequence of ASD rather than a cause. For example, children with ASD may have lower vitamin D dietary intake given that dietary restriction is common among children with ASD (Bandini et al., 2010; Graf-Myles et al., 2013). A double-blinded randomized controlled trial which evaluated vitamin D supplementation of 300 IU vitamin D3/kg/day in children diagnosed with ASD found that ASD symptoms were reduced following supplementation (Saad et al., 2018). However, this study was not able to evaluate whether vitamin D supplementation resulted in reduced incidence of ASD or its diagnoses.
No prospective cohort studies or randomized controlled trials have evaluated the hypothesis that lower 25(OH)D concentration or absence of vitamin D supplementation in childhood precedes ASD diagnoses—a necessary condition for a causal relationship (Kočovská et al., 2012). The primary objective of this study was to prospectively evaluate the magnitude of the association between serum 25(OH)D concentration in early childhood and incident physician diagnoses of ASD. The secondary objective was to evaluate the association between vitamin D supplementation in early childhood and incident physician diagnoses of ASD.
Methods
Study design and participants
We conducted a prospective cohort study through The Applied Research Group for Kids (TARGet Kids!), a primary care practice-based research network in Toronto, Canada (latitude 43°N). TARGet Kids! is a network of nine pediatric and family practices, which aims to assess the effect of early life exposures on children’s health (Carsley et al., 2015). TARGet Kids! represents an ethnically diverse sample of urban Canadian children with one-third of children of non-European ethnicity (see published TARGet Kids! cohort profile) (Carsley et al., 2015). Healthy children younger than 6 years of age were recruited between June 2008 and November 2014 during routine primary healthcare visits with baseline 25(OH)D measurement and followed during primary healthcare visits until July 2015.
Children were excluded from this study if they were 6 years of age or older at their first visit; younger than 12 months of age at study completion; had health conditions affecting growth, chronic illness (excluding asthma), severe developmental delay, or ASD at baseline; or if they did not have any subsequent TARGet Kids! follow-up visits (Carsley et al., 2015). These criteria ensured that measurement of serum 25(OH)D concentration occurred before ASD diagnoses. The baseline visit was defined as the first TARGet Kids! visit. The follow-up visit was defined as the most recent TARGet Kids! visit.
Informed consent was provided by parents of all the children and approval was obtained from the Research Ethics Boards of St. Michael’s Hospital and The Hospital for Sick Children, Toronto, Canada.
Exposure variables
Exposure variables were measured at the baseline visit. The primary exposure variable, serum 25(OH)D concentration, was obtained from venous blood samples collected by trained phlebotomists. Serum samples were sent daily to the Mount Sinai Services Laboratory (http://www.mountsinaiservices.com). Total 25(OH)D was analyzed on fresh samples using a two-step chemiluminescence assay (LIAISON 25(OH)D TOTAL Assay; DiaSorin). This assay has been extensively tested and found to have an intra-assay imprecision of 7.2% at 213 nmol/L and inter-assay imprecision of 4.9%, 8.9%, and 17.4% at concentrations of 32, 77, and 213 nmol/L, respectively (Carter et al., 2004; Maunsell et al., 2005; Singh et al., 2006).
The secondary exposure was vitamin D supplementation at baseline, which was measured using a standardized parent-completed questionnaire adapted from the Canadian Community Health Survey using the following question “Does your child take a vitamin D containing supplement regularly?” (Statistics Canada, 2013). One binary variable for vitamin D supplementation was derived, either yes or no. Use of vitamin D supplementation included single nutrient vitamin D supplements as well as multivitamins containing vitamin D. Vitamin D containing supplements and multivitamins marketed to children in Canada contain a daily dose of 400 IU (Health Canada, 2007).
Outcome variable
The primary outcome variable was physician diagnoses of ASD, which was measured at the follow-up visit. A two-step process was used to obtain physician-diagnosed ASD. First, children with “possible ASD” were identified, and second, physician diagnoses of ASD were confirmed from the medical record for children with possible ASD. Children with possible ASD were identified by parent report of ASD using the following question, “Has your child been diagnosed with autism or autism spectrum disorder” from the standardized parent-completed questionnaire. There were 74 parents that indicated their child had been diagnosed with ASD; these children were included as possible ASD. In addition, for children 6–24 months of age, the Infant-Toddler Checklist (ITC) was used to identify children with possible ASD. The ITC is a validated developmental screening questionnaire which measures three composite indicators of language development: social, symbolic, and speech and is completed by the child’s caregiver for children 6–24 months of age (Wetherby et al., 2003, 2008). ITC score below the 10th percentile of the age-standardized norms in the social, symbolic, and total score has been suggested to indicate a referral for a developmental evaluation (Wetherby et al., 2003, 2008). The sensitivity and specificity for the ITC in identifying children with ASD and other developmental delay is 88.9% for both (Wetherby et al., 2008). In our study, children who scored below the 10th percentile of age-standardized norms in the social, symbolic, or speech composite scores or total score was identified as possible ASD, in keeping with the intent of the instrument (Wetherby et al., 2003, 2008). As the ITC was conducted for research purposes, it did not influence the diagnosis of ASD in clinical practice. The ITC was measured on 857 children, of which 101 (11%) scored below the 10th percentile on any composite or the total score and were included as possible ASD. In total, using both parent reports and ITC, 171 children were identified with possible ASD.
Physician diagnoses of ASD was confirmed by retrospective review of the clinic medical record for each child with possible ASD using a standardized data collection form completed by a reviewer (Y.A.) who was blind to possible ASD status. This included review of consultation letters from specialists including developmental pediatricians and psychiatrists. Children were considered to have incident physician diagnoses of ASD if a diagnosis of ASD was indicated in the child’s medical record. All diagnoses were made by physicians using the autism spectrum or autism cutoff in the Autism Diagnostic Observation Schedule-1 (ADOS-1) or ADOS-2, or a Diagnostic Statistical Manual of Mental Disorders (4th ed.; DSM-IV) or Diagnostic Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria diagnosis of ASD, in combination with clinical judgment (American Psychiatric Association, 2000, 2013; Lord et al., 1989, 2000). To ensure blinding, 44 randomly selected children who were not suspected to have ASD were included the medical record review, none of which were identified as having physician-diagnosed ASD. In total, 215 medical records were reviewed—171 were identified as possible ASD and 44 were negative controls. After reviewing charts, 58 children had physician diagnoses of ASD; 17 were diagnosed prior to baseline, and were excluded and 41 were incident ASD diagnoses.
Covariates
Covariates that could be confounders of the association between 25(OH)D concentration and ASD diagnosis were identified a priori through a review of the literature. Covariates were measured at baseline and included child age, sex, family history of ASD (parent or sibling), maternal ethnicity, and median neighborhood household income (Bhasin and Schendel, 2007; Dealberto, 2011; Kolevzon et al., 2007). Family history of ASD was measured through the following question: “Has your child’s biological family been diagnosed with Autism: mother, father or sibling?” This question was combined into a dichotomous variable as either a history of ASD in a parent or sibling or no family history of ASD. Maternal ethnicity was measured through self-report (Omand et al., 2014). Maternal ethnicity was included as a dichotomous variable, European and non-European, as some studies have shown an association between non-European maternal ethnicity and ASD (Hultman et al., 2002; Keen et al., 2010; Kolevzon et al., 2007; Lauritsen et al., 2005). Higher median family income has also been found to be associated with ASD (Bhasin and Schendel, 2007; Durkin et al., 2010). Median neighborhood after-tax household income was used as a proxy for individual level income and was obtained using the Statistics Canada Postal Code Conversion file and 2006 Canadian Census (Mustard et al., 1999; Wilkins, 2009).
Statistical analysis
Descriptive statistics were calculated for the exposures, primary outcome, and covariates. For the primary analysis, modified Poisson regression with a robust error variance was used to provide estimates of relative risks (RRs) and 95% confidence intervals (CIs) (Zou, 2004). Unadjusted Poisson regression was first conducted to determine the unadjusted association between serum 25(OH)D concentration and incident physician diagnoses of ASD. A multiple Poisson regression model was then developed including clinically relevant covariates identified a priori (see covariates above). The number of covariates was limited to five to prevent model overfitting (Babyak, 2004; Vittinghoff and McCulloch, 2007). All covariates were included in the final models regardless of statistical significance to reduce standard error inflation from traditional variable selection techniques (Harrell, 2001). A similar model was used for the secondary analysis, but using child vitamin D supplementation as the secondary exposure variable.
Multicollinearity was assessed using the variance inflation factor (O’Brien, 2007). All variance inflation factors were below five, which suggested that multicollinearity was unlikely. Children with missing 25(OH)D or vitamin D supplementation data were excluded from the primary or secondary analyses to prevent misclassification of the exposures. Similarly, children with missing primary outcome data were excluded from the analyses to prevent misclassification of the primary outcome—this included children who were awaiting evaluation for ASD. All covariates had less than 15% missing data. To reduce the potential for bias, missing data (except for the exposures and primary outcome) were imputed using multiple imputation with 50 imputed datasets and using all identified covariates (Little and Rubin, 2002). All statistical analyses were conducted with SAS statistical software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
A total of 3852 children met inclusion criteria, of which 41 were identified with incident physician diagnoses of ASD (incidence = 1.1%) (Figure 1). The primary analysis included 2526 children with 25(OH)D data, of which 26 were cases (1.0%). All children that had vitamin D supplementation data were included in secondary analysis which included 3825 children, of which 39 were cases (1.0%).
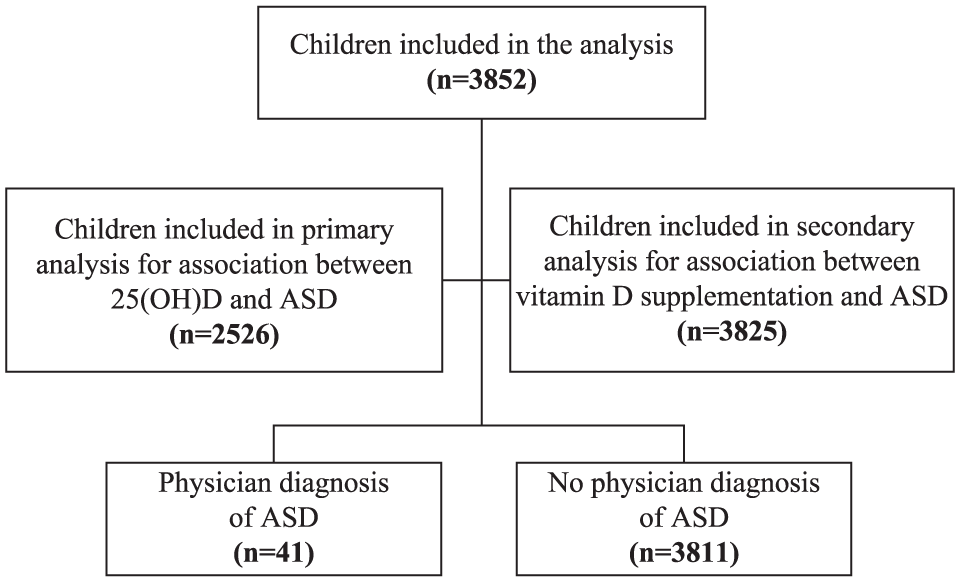
Study participants and ASD diagnosis.
The mean age of children at baseline was 2.5 years (standard deviation (SD) = 1.6) and 5.1 years at follow-up (SD = 2.3) with a mean follow-up duration of 2.5 years (SD = 1.4) (Table 1). Average age at the time of diagnosis was 4 years (SD = 1.8). Of the children included in the analysis, 52% of the children were male, 1% had a family history of ASD, 29% had non-European maternal ethnicity, and 52% were receiving a vitamin D supplement. Mean 25(OH)D measurement at baseline was 87.2 nmol/L (SD = 31.6 nmol/L, range: 11–355 nmol/L), and 38% of the children had 25(OH)D concentration less than 75 nmol/L.
Baseline characteristics of study population (n = 3852).

SD: standard deviation; ASD: autism spectrum disorder; 25(OH)D: 25-hydroxyvitamin D; n: number of subjects.
Numbers may not add to the total due to missing values.
Family history includes history of ASD in mother, father, or sibling.
Non-European consists of 169 East-Asian (7.2%), 123 South Asian (5.2%), 122 Mixed (5.2%), 89 African (3.8%), 88 Southeast Asian (3.7%), 68 Latin (2.9%), and 52 other ethnicities (2.2%).
Median after-tax household income based on postal code.
2526 children had children had 25(OH)D measurement and were included in the primary analysis for the association between 25(OH)D and ASD. About 3825 children with vitamin D supplement data were included in the secondary analysis.
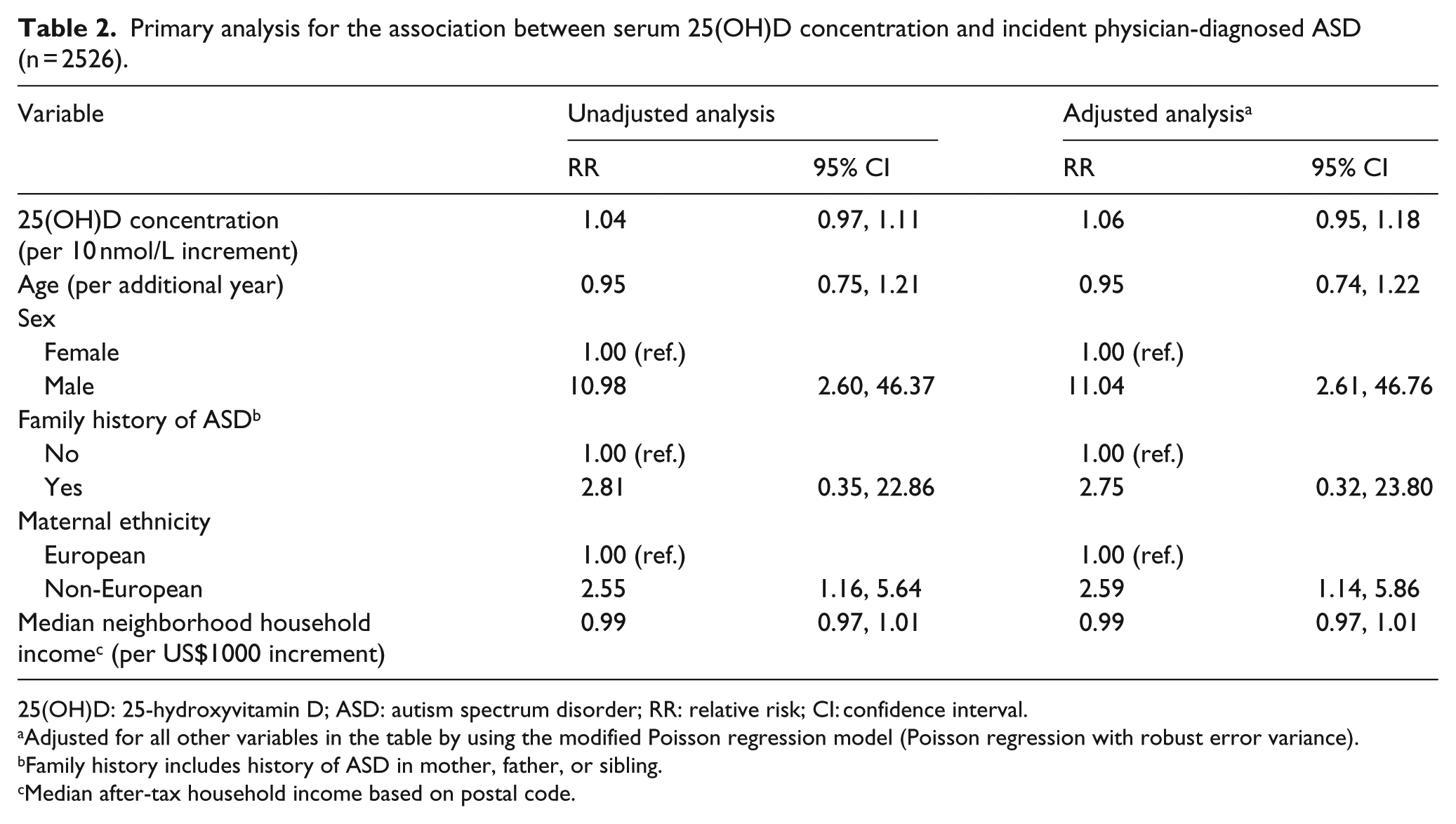
In the unadjusted primary analysis, a statistically significant association between serum 25(OH)D concentration at baseline and incident physician diagnoses of ASD was not identified (RR = 1.04; 95% CI: 0.97, 1.11 per 10 nmol/L increase in 25(OH)D concentration) (Table 2). Results of the adjusted primary analysis were similar (adjusted RR = 1.06; 95% CI: 0.95, 1.18 per 10 nmol/L increase in 25(OH)D concentration). Covariates which were significantly associated with increased risk of ASD diagnosis were male sex (adjusted RR = 11.04; 95% CI: 2.61, 46.76), and non-European maternal ethnicity (adjusted RR = 2.59; 95% CI: 1.14, 5.86).
Primary analysis for the association between serum 25(OH)D concentration and incident physician-diagnosed ASD (n = 2526).
25(OH)D: 25-hydroxyvitamin D; ASD: autism spectrum disorder; RR: relative risk; CI: confidence interval.
Adjusted for all other variables in the table by using the modified Poisson regression model (Poisson regression with robust error variance).
Family history includes history of ASD in mother, father, or sibling.
Median after-tax household income based on postal code.
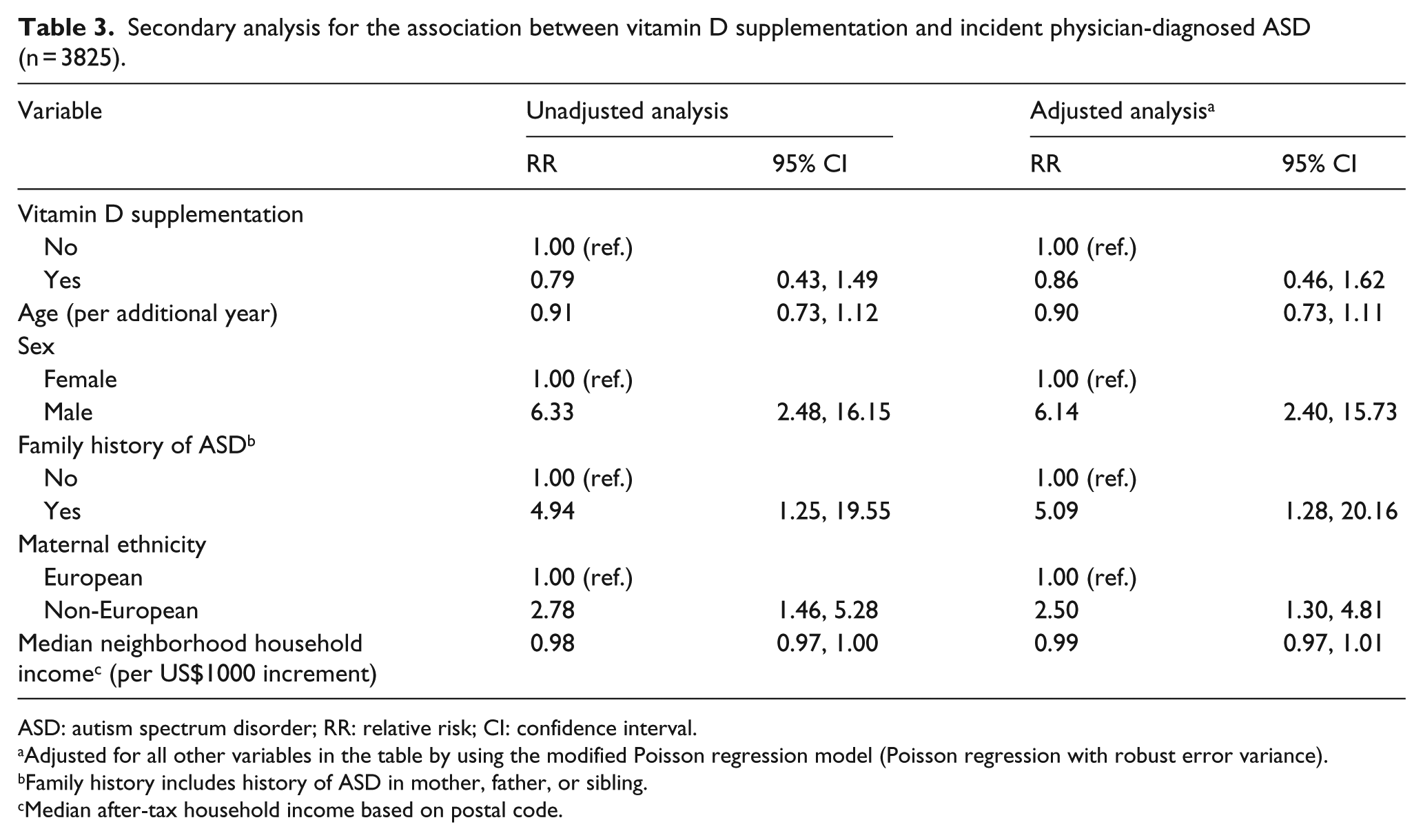
Similar results were observed for the secondary analysis. A statistically significant association was not observed between vitamin D supplementation and incident physician-diagnosed ASD in either the unadjusted (RR = 0.79; 95% CI: 0.43, 1.49) or adjusted models (adjusted RR = 0.86; 95% CI: 0.46, 1.62) (Table 3). In addition to male sex and non-European maternal ethnicity, family history of ASD was also associated with an increased risk of ASD in this adjusted model (RR = 5.09; 95% CI: 1.28, 20.16).
Secondary analysis for the association between vitamin D supplementation and incident physician-diagnosed ASD (n = 3825).
ASD: autism spectrum disorder; RR: relative risk; CI: confidence interval.
Adjusted for all other variables in the table by using the modified Poisson regression model (Poisson regression with robust error variance).
Family history includes history of ASD in mother, father, or sibling.
Median after-tax household income based on postal code.
Discussion
In this study, we used prospectively collected data from a large cohort of healthy, urban, preschool-aged children to evaluate whether early childhood 25(OH)D concentration or vitamin D supplementation was associated with incident physician diagnoses of ASD. We did not find a statistically significant association between either serum 25(OH)D concentration or vitamin D supplementation and incident physician diagnoses of ASD. However, other covariates known to be associated with ASD, such as male sex and family history of ASD, were associated with increased risk of ASD diagnosis.
To the best of our knowledge, no other prospective cohort study has evaluated 25(OH)D concentration in early childhood and incident ASD. Findings from our study differ from existing cross-sectional and case-control studies which have suggested an inverse association between 25(OH)D concentration in early childhood and ASD. A recent systematic review and meta-analysis of 11 cross-sectional and case-control studies found lower levels of 25(OH)D in children with ASD relative to children without ASD (pooled weighted mean difference = −8.63 ng/mL; 95% CI: −13.17, −4.09) (Wang et al., 2015). Of these studies, nine found statistically significant results, while two did not. Recent double-blind randomized controlled trials evaluating effects of vitamin D supplementation on ASD symptoms showed conflicting results. One trial with 300 IU vitamin D3/kg/day showed a significant improvement in ASD symptoms from supplementation and another trial with 2000 IU vitamin D3/day showed no improvement (Kerley et al., 2017; Saad et al., 2018).
None of these studies measured 25(OH)D prior to ASD diagnosis leaving open the possibility of reverse causality—ASD may have led to lower 25(OH)D levels. A plausible scenario for reverse causality could be through dietary restriction which is a common issue for children with ASD (Wang et al., 2015). In one study, children with ASD had more food refusal, more restricted dietary variety, and lower intake of vitamin D, as measured by 3-day food record (Bandini et al., 2010).
The mechanisms by which vitamin D has been hypothesized to lead to ASD have largely been based on in vitro evidence and animal models of ASD. Such research has identified changes in gene regulation, brain development, neuronal proliferation, and differentiation (Courchesne et al., 2007; Eyles et al., 2006; Ramagopalan et al., 2010). In rats, vitamin D-deplete diets during prenatal and early life have been associated with changes in brain morphology and genetic expression (Cui et al., 2007; Féron et al., 2005). One sibling-control study in Sweden reported lower in utero levels of 25(OH)D among children with ASD relative to their siblings suggesting that 25(OH)D during pregnancy may be a sensitive window for vitamin D to influence ASD (Fernell et al., 2015). Although we studied the association between vitamin D and ASD in pre-school aged children, the effect of vitamin D on ASD could potentially happen earlier in life, such as during prenatal development, which was not investigated in this study. Prospective studies assessing prenatal vitamin D exposure may help identify whether vitamin D sensitive windows exist in the development of ASD.
Strengths of our study included a relatively large sample size with 25(OH)D measurement in early childhood and subsequent prospective evaluation of incident physician diagnoses of ASD which allowed evaluation of the temporality of the association, a necessary condition for causality (Hill, 2015). Furthermore, clinically rich baseline data allowed for adjustment for multiple possible confounders. The mean follow-up duration of 2.5 years in children less than 6 years of age allowed for accrual of 41 cases with an incidence consistent with population-based estimates, suggesting generalizability of our findings (Ouellette-Kuntz et al., 2014; Wingate et al., 2014). In addition, outcome ascertainment included confirmation of physician diagnosis of ASD making misclassification unlikely.
Limitations of this study included statistical power to detect a weak association. Even with a large prospective cohort study, the relatively low incidence of ASD makes prospective evaluation of ASD risk factors challenging. However, the magnitude of the observed effect estimates were close to 1.0, suggesting that a clinically meaningful association is unlikely. In addition, 8% of children included in the analysis were between the age of 1 and 2 years old at follow-up, and some of these children may have yet to be diagnosed with ASD (Wingate et al., 2014). Despite our best efforts to confirm ASD diagnosis, we may have missed some cases since medical records were reviewed only for children with suspected ASD. Children with ASD that did not have the ITC completed or did not have a parent report of ASD could have been missed as cases. Also, reliability of chart abstraction could not be obtained for those whose charts were reviewed since there was only a single data abstractor.
Also, there may be the possibility of selection bias since not all children with a baseline 25(OH)D measurement had follow-up visits. Furthermore, the time of ASD diagnosis may not have reflected the initiation of ASD symptoms which, while undiagnosed, may have occurred prior to baseline 25(OH)D measurement. Also, due to data limitations, we were unable to capture the age at which supplementation was started and thus supplementation measurement may not reflect the time period when it was administered. In addition, while 25(OH)D concentration is believed to be stable over time, only one 25(OH)D measurement was available in this study (Berger et al., 2012). This study was also limited in the number of covariates that could be included in the models due to limited power and to avoid overfitting (Peduzzi et al., 1996). For example, maternal ethnicity was collapsed into two categories limiting adjustment for other ethnicities and few children diagnosed with ASD were female. Non-European maternal ethnicity was found to be associated with ASD diagnosis, which differs from US population-based surveillance and survey data where a higher prevalence of ASD was identified in non-Hispanic white children, relative to non-Hispanic black or Hispanic children suggesting that our population may not be representative of all North American children (Durkin et al., 2017; Mandell et al., 2002). Other covariates which were considered for inclusion, but not incorporated because of limited power included skin pigmentation and season of birth. However, these factors were unlikely to have a large effect on vitamin D levels in early childhood (Maguire et al., 2013). While residual confounding is a possibility, the unadjusted and adjusted results had similar effect estimates suggesting that this is unlikely. Also, baseline 25(OH)D concentration was relatively high with 52% of subjects consuming a vitamin D containing supplement and this may not be generalizable to other populations with lower supplementation and 25(OH)D concentrations.
Conclusion
Findings from previous cross-sectional and case-control studies have suggested an association between low serum 25(OH)D concentration in early childhood and ASD. In this prospective cohort study where vitamin D was measured prior to ASD diagnosis, a statistically significant association between serum 25(OH)D concentration or vitamin D supplementation in early childhood and incident physician diagnoses of ASD was not identified with effect estimates close to null. Low serum 25(OH)D concentration in early childhood may not be associated with ASD diagnoses. Prospective studies assessing prenatal vitamin D exposure may provide further insights into whether vitamin D sensitive windows exist in the development of ASD.
Supplemental Material
AUT756787_Lay_Abstract – Supplemental material for Prospective cohort study of vitamin D and autism spectrum disorder diagnoses in early childhood
Supplemental material, AUT756787_Lay_Abstract for Prospective cohort study of vitamin D and autism spectrum disorder diagnoses in early childhood by Yamna Ali, Laura N Anderson, Sharon Smile, Yang Chen, Cornelia M Borkhoff, Christine Koroshegyi, Gerald Lebovic, Patricia C Parkin, Catherine S Birken, Peter Szatmari and Jonathon L Maguire; on behalf of the TARGet Kids! Collaboration in Autism
Footnotes
Acknowledgements
We thank all of the participating families for their time and involvement in TARGet Kids! and are grateful to all practitioners who are currently involved in the TARGet Kids! practice-based research network.
*
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JLM received an unrestricted research grant for a completed investigator-initiated study from the Dairy Farmers of Canada (2011–2012) and D-drops provided non-financial support (vitamin D supplements) for an investigator initiated study on vitamin D and respiratory tract infections (2011–2015).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes for Health Research (MOP-106532). Funding agencies had no role in the design, collection, analyses, or interpretation of the results of this study or in the preparation, review, or approval of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.