
Abstract
Social support can buffer against stressors often associated with having family members with autism spectrum disorder. This study included 112 parents and typically developing siblings of children with autism spectrum disorder. Relations between self-reported typically developing sibling emotional and behavioral problems and discrepancy between social support frequency and importance were examined via polynomial regression with response surface analysis. Typically developing siblings who described social support as frequent and important reported relatively few problems. Typically developing siblings who reported social support as highly important but infrequent exhibited the highest emotional and behavioral difficulties. Thus, typically developing siblings with little support who view support as highly important may be particularly responsive to social support improvement efforts.
According to the most recent reports from the Centers for Disease Control and Prevention (CDC) and the Autism and Developmental Disabilities Monitoring Network (ADDM), autism spectrum disorder (ASD) diagnostic rates have increased more than 100% since 2002 (Christensen et al., 2016). It is also important to consider the increase in individuals who interact with children with ASD, including parents and siblings. Children with ASD present a variety of challenges that may impact the members of their family and how their families function (Cridland et al., 2014; Reichman et al., 2008). Families of children with ASD experience higher levels of parental stress and increased difficulties in family functioning compared to families of typically developing (TD) children and compared to families of children with many other disabilities or disorders (Altiere and Von Kluge, 2009; Johnson et al., 2011; Miodrag and Hodapp, 2010; Rao and Beidel, 2009).
This increased stress is thought to be due, at least in part, to the unique challenges that accompany ASD (Davis and Carter, 2008), such as insistence on routines, sudden mood changes, restricted/repetitive behaviors, and frequent challenges in social interactions (Attwood, 2007; Heiman and Berger, 2008; Macks and Reeve, 2007; Pakenham et al., 2005). Additionally, aggression, self-injurious behavior, and severe tantrums are common features that impair children with ASD and impact family stress (Adler et al., 2015; Dumas et al., 1991; Ingersoll and Hambrick, 2011). Having a child with ASD often results in a significant financial burden, with medical expenditures 4.1–6.2 times greater for children with ASD than TD children (CDC, 2016). These challenges may often lead to other negative outcomes in family functioning, such as greater family conflict and less frequent use of problem-focused coping strategies (Meadan et al., 2010; Phelps et al., 2009), including among TD siblings.
Sibling outcomes
Much of the previous research on functioning among families with children with ASD has focused heavily on parental outcomes; however, more recently, increased attention has been given to the functioning of TD siblings of children with ASD (Meadan et al., 2010; Smith and Elder, 2010). The research on TD sibling outcomes is mixed (e.g. Green, 2013; Meadan et al., 2010). Some previous literature suggests that a portion of siblings experience significant emotional and behavioral adjustment problems (Smith and Elder, 2010), including depression, anxiety, and externalizing behavior problems (Bitsika et al., 2015; Gold, 1993; Hastings, 2003b; Verté et al., 2003). However, other studies indicate that siblings of children with ASD do not experience emotional and behavioral problems at a greater rate than other siblings (Dempsey et al., 2012; Hastings and Petalas, 2014; Tomeny et al., 2012). Still, other research has found positive outcomes for TD siblings of children with ASD, such as positive self-concept (Macks and Reeve, 2007; Mates, 1990; Verté et al., 2003).
Given this variability, researchers have sought to examine risk and protective factors for TD siblings (e.g. Walton and Ingersoll, 2015). Factors such as gender (Hastings, 2003b; Macks and Reeve, 2007), birth order (Tomeny et al., 2014), and age (Rodrigue et al., 1993) have been identified as third variables involved in the relation between characteristics of children with ASD and adjustment in siblings. Unfortunately, these particular demographic factors are not amenable to intervention. As such, research may be better suited to focus on potentially amenable intervention targets that may aid in more favorable TD sibling development. One variable that may help ameliorate some of the potentially negative effects on TD sibling adjustment (Hastings, 2003a) is social support (Gottlieb, 1985).
Social support
An expansive literature illustrates that social support, in general, can ameliorate the effects of many stressors on childhood adjustment (Cohen, 2004). Social support can be informal, unstructured, and/or spontaneous responses to the needs of a child by those close to that child (e.g. family, friends, and community members), or it can be formal, highly organized resources designed to enhance the well-being of a child (Caplan, 1974). Specifically, recent research suggests that informal social support is beneficial for TD siblings’ psychological adjustment (Cebula, 2012) and that formal supports may act as a buffer between a child’s ASD and the adjustment of their TD siblings (Hastings, 2003a). Considering these findings, as well as the burden for families of youth with ASD often associated with engaging in formal support resources, informal social support may be an avenue in which many TD siblings receive the help they need to cope with the stressors they may face. Formal programs such as Sibshops, which partially aim to increase available informal social support for siblings through interaction with similar peers (Conway and Meyer, 2008), have garnered interest and utilization (D’Arcy et al., 2005). Yet, these programs often have mixed findings regarding sibling outcomes (D’Arcy et al., 2005; Tudor and Lerner, 2015). While these lackluster results may be explained by a host of issues (e.g. poor treatment fidelity and differences in research methodology), these findings may also be related to less than optimal assessment and measurement of informal social support.
Perceptions of unmet needs for informal social support
Literature indicates that the actual amount of informal support available to someone may not be as meaningful as how much support that individual perceives that he or she receives (Bolger et al., 1996; Gable et al., 2012). According to Norris and Kaniasty (1996), “received support refers to naturally occurring helping behaviors that are being provided, whereas perceived support refers to the belief that such helping behaviors would be provided when needed” (p. 489). In their study, Norris and Kaniasty (1996) found that perceptions of social support mediate the relation between the actual receipt of support and some forms of distress. Additionally, perceptions of received support and desired support (i.e. the types of support that an individual would like to be receiving) are believed to be critically different from one another (Picard et al., 1997), and the mismatch between the two is thought to provide more evidence of a lack of overall support than considering generally lower levels of received support alone (Song et al., 2012). Therefore, given the complex nature of social support, simply examining the amount of support one explicitly receives may be less than ideal. Instead, it is important to consider both how much support the individual perceives that he or she receives and, similar to one’s desires for support, the individual’s perceptions of the importance of this support (i.e. is the support perceived as significant and/or meaningful?).
Given that perceptions of received social support and the importance of this support may vary among siblings, comparing across the two constructs may be difficult. However, examining these complex variables together could provide greater insight into the relation between social support and sibling outcomes. Although investigation into support in this manner is common in the marital support literature (e.g. Barry et al., 2009; Brock et al., 2012), it is nearly absent in the literature on siblings. These dynamics are of particular interest among TD siblings of youth with ASD, as families affected by ASD (compared to other families) tend to receive less support but may indeed require more support (e.g. Boyd, 2002; Bromley et al., 2004; Weiss, 2002).
This study
This study aimed to better understand the relation between social support and TD sibling outcomes by examining discrepancies between perceived frequency (i.e. amount) of social support and the level of importance assigned to that support. Specifically, polynomial regression and surface response analysis was used to examine the relations between TD sibling emotional and behavioral difficulties and social support at differing levels of agreement between social support frequency and importance.
First, we expected that TD siblings would report the lowest levels of emotional and behavioral difficulties when social support frequency and importance were high in amount and highly congruent (Hypothesis 1). Next, we expected the level of discrepancy between frequency of social support and social support importance would predict TD sibling emotional and behavioral difficulties (i.e. higher discrepancy would predict more difficulties; Hypothesis 2). Finally, we expected that TD siblings who report social support importance as greater than frequency would also report greater levels of difficulties compared to TD siblings who report frequency as greater than importance and compared to TD siblings who do not report a discrepancy between frequency and importance (Hypothesis 3).
Method
Participants
Respondents were 112 parents of at least two children (one child with an ASD and one TD sibling) and TD siblings of children with ASD (parents and TD siblings were recruited as dyads). TD siblings, those confirmed by parents as not having an ASD diagnosis, included 57 male and 55 female children between the ages of 11 and 17 years (M = 13.31 years, standard deviation (SD) = 1.82 years). Each child with ASD was independently diagnosed prior to this study, as confirmed by parents. Children with ASD included 87 males and 25 females between the ages of 3 and 17 years (M = 11.99 years, SD = 3.30 years), and 55% were diagnosed with autistic disorder, 21% with Asperger’s, and 24% with pervasive developmental disorder–not otherwise specified (PDD-NOS). Caregivers who served as respondents ranged in age from 31 to 60 years (M = 44.07 years, SD = 5.24 years), 98.2% were female, 93.8% were identified as Caucasian, 76.8% were married, and 41.1% were described having a total annual family income over US$100,000. See Table 1 for additional sample characteristics.
Sample characteristics.
SD: standard deviation; ASD: autism spectrum disorder; TD: typically developing.
Procedure
Institutional review board approval, informed consent from each parent, and assent from each TD sibling were obtained prior to any data collection. Families were recruited as part of a larger study through posted flyers, contacts with ASD organizations, and a referral sampling technique. Parents who expressed interest in the study were sent a link to a secure survey website via Qualtrics (2016), and parent and sibling responses were linked via the survey portal. Parents received detailed instructions outlining which child to consider when completing each of the questionnaires. Parents completed the demographic and diagnostic form as well as the Children’s Social Behavior Questionnaire (CSBQ) and the Strengths and Difficulties Questionnaire (SDQ) on their child with ASD (measures are described below in the “Measures” section). TD siblings then completed the SDQ and Child and Adolescent Social Support Scale (CASSS) about themselves (either directly following the parents or at a later time, as participants could return to complete unfinished questionnaires at a later time if needed). Only participants who were sent links but never began the study or who did not complete study measures (i.e. participants who withdrew before finishing measures and participants who skipped sections of measures) were not retained for final analyses. Of the families sent study links, 63% completed the study and were retained in the sample. Following study completion, participating families were entered into a random drawing for 1 of 10 US$30 gift cards to a national retailer.
Measures
Demographic and diagnostic questionnaire
Parents completed this form on their child with ASD, the TD sibling, themselves, and the overall family. This form requested basic demographic information such as age, gender, race, diagnosis of child with ASD, family income, and parent education. Parents confirmed ASD diagnoses using this form, along with age of diagnosis and profession/affiliation of the person who made the diagnosis (i.e. to rule out parents self-reporting that they think their child has an ASD diagnosis).
CASSS
The CASSS, completed by TD siblings, is a 40-item self-report measure of child and adolescent perceived social support (Malecki and Demaray, 2002). The CASSS measures support from five sources: parents, teachers, classmates, close friends, and people in school. TD siblings rated frequency, using a 6-point Likert scale from 1 (never) to 6 (always), and importance, using a 3-point Likert scale from 1 (not important) to 3 (very important). According to Malecki and Demaray (2002), the CASSS has displayed good internal consistency, test–retest reliability, and concurrent validity with other childhood measures of social support. The current sample yielded Cronbach’s alphas of 0.97 for each of the scales (both frequency and importance).
SDQ
The SDQ is a 30-item measure of child emotional and behavioral functioning (Goodman, 1997). TD siblings completed the self-report version and parents completed the parent-report version on their child with ASD, rating each item as not true, somewhat true, or certainly true (Goodman, 1997). The SDQ is composed of four problem scales (Emotional Symptoms, Conduct Problems, Hyperactivity/Inattention, and Peer Relationship Problems) and a Prosocial Behavior Scale (Goodman, 1997). The sum of the four problem scales generates a total difficulties score, which served as the measure of TD sibling emotional and behavioral functioning and as the measure of emotional and behavioral symptoms (i.e. indicators of difficulties not specific to ASD) in children with ASD for this study. The SDQ has shown sufficient internal consistency and concurrent validity with other measures of child psychopathology (Goodman, 1997, 2001). The current sample yielded a Cronbach’s alpha of 0.82 for the SDQ total difficulties scale.
CSBQ
As a measure of ASD symptoms, parents completed the 49-item CSBQ on their child with ASD using a 3-point Likert scale: 0 (it does not describe the child), 1 (infrequently describes the child), or 2 (clearly applies to the child; Luteijn et al., 2000). The CSBQ is composed of six subscales that map onto different domains of ASD and a total score (Luteijn et al., 2000). The six domains include “Behavior/emotions not optimally tuned to the social situation/aggressive behavior,” “reduced contact and social interest/withdrawn,” “difficulties understanding social information,” “orientation problems in time, place, or activity,” “stereotyped behavior,” and “fear of and resistance to change” (Hartman et al., 2006). The CSBQ has shown high internal consistency, test–retest reliability, interrater reliability, and concurrent validity with other ASD measures (Hartman et al., 2006). The current sample yielded a Cronbach’s alpha of 0.91 for the CSBQ total score, which served as a measure of overall ASD symptom severity for this study. Moreover, the current sample yielded a mean CSBQ score of 45.62 (SD = 15.32) for the children with ASD, which is consistent with previous clinical samples with ASD (e.g. PDD-NOS; high-functioning autism; means ranging from 33.64 to 47.22; SD = 14.51–15.94; Hartman et al., 2006).
Data analytic approach
Interrelations of the variables of interest were examined by computing Pearson’s correlation coefficients. As suggested by Laird and De Los Reyes (2013), polynomial multiple regression with response surface analysis (for a detailed description of this technique, see Shanock et al., 2010) was used to examine the three hypotheses. Following Shanock et al. (2010), Edwards (2002), and Parker et al. (2016), the sample was first examined to determine whether a discrepancy indeed existed between social support importance and frequency as outlined by Fleenor et al. (1996): z-scores of social support frequency were subtracted from z-scores of social support importance, and those with greater than one-half a SD difference were separated into two groups depending on which support scale (i.e. frequency or importance) was higher. Those with a frequency–importance difference less than one-half SD were placed into a third group. Then, polynomial regression analysis was conducted via ordinary least squares regression (Ostertagová, 2012) on the criterion variable (i.e. TD sibling emotional and behavioral problems) to determine whether response surface analysis was appropriate and to compute the regression coefficients needed to plot the three-dimensional response surface. This analytic procedure was used (a) because linear relations cannot be automatically assumed (Laird and De Los Reyes, 2013) and (b) to avoid the documented shortcomings of other techniques, such as difference score approaches (Edwards, 2001, 2002) Similar to Parker et al. (2016), the analysis was conducted stepwise to allow control variables to be entered and to allow tests of specific components to model hypotheses.
Control variables were entered in the first step; the linear and quadratic social support frequency terms, the linear and quadratic social support importance terms, and the cross product of social support frequency and importance term were added in the second step. Prior to the creation of polynomial terms, the perceived social support frequency scale was transformed to be on the same 1–3 scale as social support importance scale. Next, scores on both social support scales (i.e. transformed frequency and original importance) were centered around their scale mid-point (i.e. 2) to facilitate interpretation and reduce potential multicollinearity (Cohen et al., 2003; Edwards, 2002) and were averaged. Quadratic terms and cross products were then computed using the centered, averaged scores in preparation for polynomial regression analysis. The increase in R2 was examined to determine level of variance explained by including both frequency and importance as predictors.
Graphical analyses of three-dimensional response surfaces from features of the polynomial models were then conducted (Shanock et al., 2010). Per Edwards and Parry (1993) and Edwards (2001), the coefficients from the regression model are used in response surface analysis to construct four slopes along the response surface. The slope of the line of congruence (a1 = b1 + b2; also called the line of agreement) represents the effect of predictors on the outcome when the two predictors are in agreement (X = Y). For example, a significant positive slope indicates that when both predictors are high, the outcome is at its highest. The curvature of this line (a2 = b3 + b4 + b5) is also examined to determine whether the relation between predictors and the outcome, while predictors are in agreement, is curvilinear. The slope of the line of incongruence (a3 = b1 − b2; also called the line of disagreement) represents the effect of predictors on the outcome when the two predictors are discrepant (X = −Y). For example, a significant positive slope indicates that when the first predictor is higher than the second predictor, the outcome is at its highest. Alternatively, when the second predictor is higher than the first, the outcome is at its lowest. The curvature of this line (a4 = b3 − b4 + b5) indicates if the relation between predictors and the outcome, while predictors are discrepant, is curvilinear (i.e. more discrepancy is related to higher outcomes).
Results
Preliminary analyses
Less than 0.4% of data were missing at the item level (i.e. questions that were skipped at the item level), and the relevant scales were prorated and person mean imputation was implemented, per Roth et al. (1999) and Hawthorne and Elliot (2005). Descriptive statistics and the interrelations of the variables of interest are presented in Table 2. Frequency of social support and social support importance (as measured by the CASSS) were positively correlated. Self-reported TD sibling emotional and behavioral problems (as measured by the SDQ) were negatively correlated with both perceived frequency of social support and social support importance. Furthermore, both ASD symptom severity (as measured by the CSBQ) and emotional and behavioral symptoms (as measured by the SDQ) in siblings with ASD were positively correlated with TD sibling emotional and behavioral problems and were included as covariates in the polynomial regression analysis. The relations between demographic variables and the variables of interest are presented in Table 3. TD sibling age was negatively correlated with social support frequency (older children reported less frequent social support) and also was included as a covariate in the polynomial regression analysis. It should be noted that TD siblings in the current sample, on average, received scores on the SDQ in the normal range (M = 10.04, SD = 5.74, current sample range: 0–25, possible range: 0–40; Goodman et al., 1998), suggesting relatively low levels of emotional and behavioral difficulties.
Intercorrelations and descriptives of variables of interest.

ASD: autism spectrum disorder; CSBQ: Children’s Social Behavior Questionnaire, measuring ASD symptom severity; SDQ: Strengths and Difficulties Questionnaire, measuring emotional and behavioral problems; CASSS: Child and Adolescent Social Support Scale, measuring social support; TD: typically developing; SD: standard deviation.
The mean of social support frequency was calculated using its original 1- to 6-point Likert scale.
p < 0.01; *p < 0.05.
Correlations between variables of interest and possible control variables.

ASD: autism spectrum disorder; TD: typically developing.
Gender coded as 0: male, 1: female; sibling gender match/mismatch coded as 0: gender mismatch, 1: gender match.
Measured by the Strengths and Difficulties Questionnaire (SDQ).
Measured by the Child and Adolescent Social Support Scale (CASSS).
TD sibling race was dichotomized and coded as 0: non-white, 1: white.
Absolute value.
p < 0.01.
Hypothesis testing
Table 4 presents results from the polynomial regression analysis of social support importance and social support frequency predicting self-reported TD sibling emotional and behavioral problems. Greater than half (51.8%) of the sample had “discrepant” predictor variables as outlined by Fleenor et al. (1996; i.e. their scores were greater than one-half SD different from one another). A total of 24.1% of youth reported greater importance than frequency, and 27.7% reported greater frequency than importance. When predicting TD sibling emotional and behavioral problems, the hierarchical polynomial multiple regression revealed a significant Model 1 (control variables), F(3, 108) = 3.26, p = 0.02, R2 = 0.08; however, none of the control variables were significant unique predictors in the model. Inclusion of the polynomial terms yielded a significant Model 2, ΔF(5, 103) = 8.37, p < 0.001, ΔR2 = 0.27. Specifically, social support frequency accounted for unique variance in the model, β = −0.60, p = 0.003. Because the increase in R2 was significant with the addition of the linear and quadratic predictor terms, response surface analysis was explored to provide better understanding of the three-dimensional response surface produced by the polynomial model (addition of the cubic terms did not yield a significant Model 3, thus providing support for a quadratic model; Edwards, 2002; Shanock et al., 2010). A post hoc power analysis conducted with G*Power 3.1 (Faul et al., 2009) revealed that with a sample size of 112, α = 0.05, 8 total predictors (5 tested predictors), and the observed effect size (f 2 = 0.369), achieved power was 0.99 for the above regression analysis.
Results of regression and polynomial response surface analysis of TD sibling emotional and behavioral problems as predicted by social support frequency and importance.

ASD: autism spectrum disorder; CSBQ: Children’s Social Behavior Questionnaire, measuring ASD symptom severity; SDQ: Strengths and Difficulties Questionnaire, measuring emotional and behavioral problems; CASSS: Child and Adolescent Social Support Scale, measuring social support.
Unstandardized regression coefficients reported for each predictor; standard error reported in parentheses following each regression coefficient. Degrees of freedom reported in parentheses following each R2 value. a1 = (b1 + b2), where b1 is beta coefficient for social support importance and b2 is beta coefficient for social support frequency. a2 = (b3 + b4 + b5), where b3 is beta coefficient for social support importance squared, b4 is beta coefficient for the cross product of social support importance and social support frequency, and b5 is beta coefficient for social support frequency squared. a3 = (b1 − b2). a4 = (b3 − b4 + b5).
Measured by the Strengths and Difficulties Questionnaire (SDQ).
p < 0.001; **p < 0.01; *p < 0.05.
The slope and curvature of both the line of congruence (slope: a1, curvature: a2) and the line of incongruence (slope: a3, curvature: a4) are displayed in Figures 1 and 2 (Panels a through d; Cohen et al., 2003; Edwards, 2002). Response surface analysis revealed a significant and negative slope of the line of congruence (a1; X = Y) when predicting TD sibling emotional and behavioral problems (a1 = −9.06, standard error (SE) = 3.08; t = −2.94, p = 0.004; Table 4), indicating that TD sibling problems decrease as both social support importance and perceived social support frequency increase. This significant negative slope along the line of congruence supports Hypothesis 1. Furthermore, response surface analysis revealed a significant and positive line of incongruence (a3; X = −Y) with TD sibling emotional and behavioral problems as the criterion (a3 = 12.28, SE = 4.56, t = 2.69, p = 0.008; Table 4). That is, sibling problems are relatively low when social support importance and perceived social support frequency are in agreement or when perceived frequency is high and importance is low. Alternatively, TD sibling difficulties are higher when social support importance is high and perceived social support frequency is low. This significant positive slope along the line of incongruence supports Hypothesis 3. However, because the curvature of the line of incongruence is nonsignificant, Hypothesis 2 was not supported; that is, the relation between social support discrepancy and TD sibling emotional and behavioral difficulties does not vary as a function of the amount of discrepancy present.
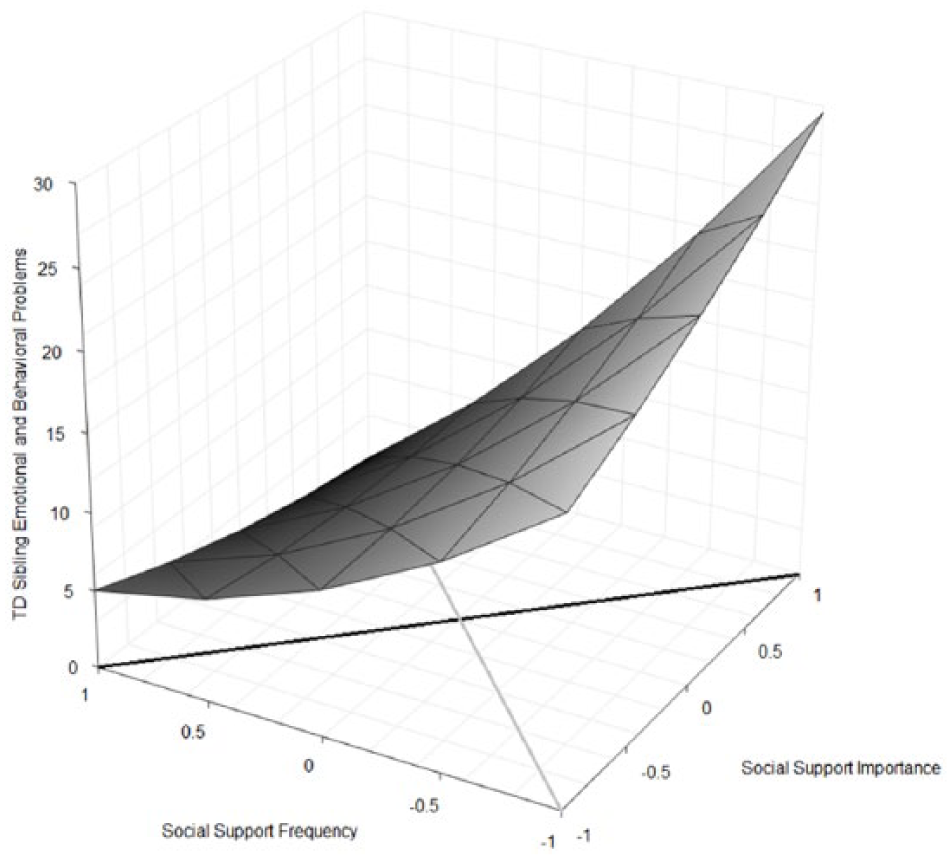
Response surface of the relation between social support importance and social support frequency in predicting TD sibling emotional and behavioral problems. The black line represents the line of incongruence, and the gray line represents the line of congruence.
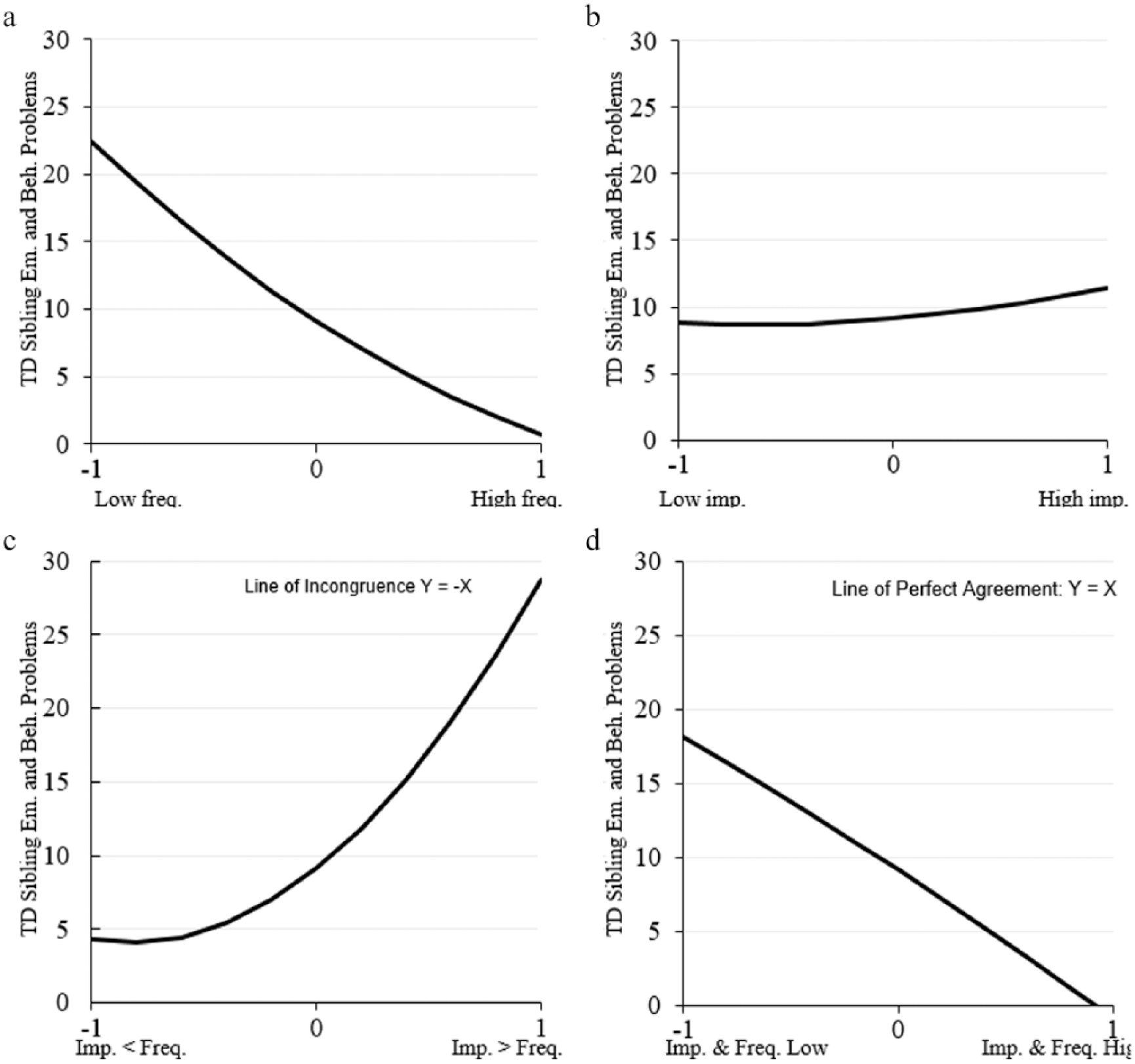
Panels a–d: TD sibling emotional and behavioral problems are featured on the Y-axis of each panel. Panel a: the relation between frequency of social support and TD sibling emotional and behavioral problems while importance is held constant at 0. Panel b: the relation between importance of social support and TD sibling emotional and behavioral problems while frequency is held constant at 0. Panel c: the line of incongruence (Y = −X) as it relates to TD sibling emotional and behavioral problems (1 represents when importance is high and frequency is low, and −1 represents when frequency is high and importance is low). Panel d: the line of congruence in relation to TD sibling emotional and behavioral problems (1 represents when both frequency and importance are high, and −1 represents when both are low).
Comparisons were then conducted to examine differences between points of interest along the line of incongruence. Specifically, we wanted to determine whether there were significant differences in TD sibling emotional and behavioral difficulties at different points along the line of incongruence: when importance > frequency (i.e. at 1 in Figure 2, Panel c), when there is no discrepancy (i.e. at 0 in Figure 2, Panel c), and when frequency > importance (i.e. at −1 in Figure 2, Panel c). Considering that the line of incongruence had nonsignificant curvature, these comparisons examined linear relations only. As previously mentioned, three groups were calculated based on Fleenor et al. (1996) and Shanock et al. (2010): individuals with greater frequency than importance (−1), individuals with greater importance than frequency (1), and those with no difference (0). A one-way analysis of variance (ANOVA) predicting TD sibling emotional and behavioral problems with a Bonferroni correction was conducted to test the difference in TD sibling problems between each group. A significant omnibus ANOVA was present, F(2, 109) = 4.87, p = 0.009. Post hoc Bonferroni comparisons revealed that those who had higher social support importance than frequency (M = 12.94, SD = 5.52) experienced significantly greater emotional and behavioral problems than either those with no discrepancy (M = 9.02, SD = 5.42) or those with higher frequency than importance (M = 9.29, SD = 5.82), providing further support for Hypothesis 3. Moreover, there was no significant difference between those with no discrepancy and those with higher frequency than importance.
These three groups also differed in mean levels of both social support frequency, F(2, 109) = 10.99, p < 0.001, and social support importance, F(2, 109) = 8.01, p = 0.001. Specifically, TD siblings who reported more importance than frequency reported lower social support frequency (M = 223.74, SD = 39.25) than those who reported more frequency than importance (M = 277.00, SD = 51.88) and those with no difference (M = 259.58, SD = 41.14). Furthermore, those who reported more frequency than importance reported significantly lower social support importance (M = 120.87, SD = 27.09) than both of the other groups (no difference: M = 135.72, SD = 19.82; more importance than frequency: M = 143.12, SD = 19.24).
Discussion
To our knowledge, this is the first study to explore the role of social support discrepancy (i.e. the difference between how important one views social support and how much support one perceives that he or she receives) in the emotional and behavioral adjustment of TD siblings of youth with ASD. As expected, greater perceived social support frequency and greater social support importance were both related to fewer emotional and behavioral problems for TD siblings of youth with ASD. Furthermore, when TD siblings did not exhibit a discrepancy between how much support they receive and how important they view such support, greater importance and frequency were related to fewer TD sibling emotional and behavioral problems, over and above the variance explained by ASD symptom severity and emotional and behavioral problems in children with ASD. However, results also suggest that many TD siblings reported a discrepancy between frequency and importance of support. Data suggest that just under a quarter of these TD siblings may view support as highly important, but they perceive receiving less frequent support. Additionally, a separate quarter of these youth may perceive receiving high levels of support, but they view social support as less important. Polynomial multiple regression with surface response analysis revealed that those who view support as highly important but who perceive receiving little support report greater levels of emotional and behavioral problems compared to those who exhibit congruence between social support importance and frequency or compared to those who report high frequency and low importance. Although TD siblings who viewed social support as highly important but perceived a low frequency of support exhibited the highest problems, the relation between TD sibling emotional and behavioral problems and social support discrepancy did not vary as a function of the amount of social support discrepancy.
Additionally, social support was found to be negatively related to TD sibling emotional and behavioral difficulties at the bivariate level, consistent with past studies of youth in general (e.g. Auerbach et al., 2011) and in TD siblings of youth with ASD specifically (Cebula, 2012; Wolf et al., 1998). Social support has long been considered an important factor in buffering the effects of negative stressors and in improving outcomes, such as lower levels of interpersonal stress (Auerbach et al., 2011), depressive symptoms (Vaughan et al., 2010), and overall adjustment difficulties (Wolf et al., 1998). Programs to enhance informal support for TD siblings (e.g. Sibshops) have begun to increase in recent years (Conway and Meyer, 2008); however, programs’ abilities to improve sibling outcomes have often been met with mixed results (D’Arcy et al., 2005; Tudor and Lerner, 2015).
Similarly, the pattern of results suggests that there may not be a difference in the amount of support received between TD siblings who perceive having their social support needs met and those who perceive receiving support that is more frequent than important. Alternatively, TD siblings who report social support discrepancies with importance greater than frequency may receive less frequent support while also viewing support as more important. This pattern suggests that it is not only that these TD siblings view support as very important but also that they perceive receiving less support that drives social support discrepancies. It may be that these siblings view support as more important because they have lacked support in the past. These findings highlight the need for clinicians who work with TD siblings to be keenly aware of the siblings’ perceptions of both the availability and importance of social support.
Overall, our results suggested that difficulties in TD siblings were highest when they expressed perceptions of unmet social support needs (i.e. frequency was lower than importance ratings). Generally, increasing informal social support resources for TD siblings remains a potential target of interventions for TD siblings of youth with ASD (Conway and Meyer, 2008; D’Arcy et al., 2005). However, this finding suggests that considering instances of unmet support may be more useful than a simple examination of how much support one perceives that they receive. This result is consistent with marital/spousal support literature (Dehle et al., 2001; Picard et al., 1997) and parent-support literature (Boothe et al., 2011; Fonseca et al., 2014; Lee and Choi, 2013) but had previously been unexamined in terms of broadly stated social support, particularly among TD siblings of children with ASD.
More importantly, these findings provide valuable information for interventions that aim to either increase the availability of informal social support to siblings or that attempt to reframe siblings’ opinions of the support they already receive. Although increasing the overall amount of support received by TD siblings can be important in many cases, clinicians must be cautious when prescribing additional intervention to families who often are already overburdened by treatments sought for their child with ASD as suggested by Tudor and Lerner (2015). Increasing supports for siblings who desire little support or who do not view support as important may not be nearly as critical as increasing available support for siblings who view social support as highly important (Picard et al., 1997). Moreover, the wide variability in TD sibling outcome research suggests that simply being a sibling of a child with ASD does not appear to be reason enough for TD siblings to need treatment for themselves (Tudor and Lerner, 2015), particularly given the limited resources possessed by many families. However, the current results indicate that TD siblings of individuals with severe ASD symptomatology may benefit from intervention, particularly when they believe that they are not receiving the informal supports that they perceive as important.
Limitations and future research
The results should be considered in light of several limitations. The sample was relatively small and homogeneous. Data were cross-sectional and collected using a technique that could have led to sampling bias. Similarly, TD siblings’ mean SDQ scores fell within the normal range based on normative data (e.g. Goodman et al., 1998), indicating that most of the TD siblings were relatively well adjusted. Nevertheless, we argue that examination of the variability in sibling adjustment is an important step in differentiating those TD siblings who may be in need of services. Although a primary goal of this study was to improve on past research by examining self-report data from TD siblings and to establish a relation between social support discrepancy and functioning in TD siblings, the direction of the current results cannot be confirmed. Specifically, it is just as possible that TD siblings with more emotional and behavioral problems wish for more support than they are receiving, rather than discrepancy in support predicting problems in TD siblings. For example, TD siblings with more emotional and behavioral problems may recognize their own distress and hope for relief in the form of additional support. These remaining questions indicate that future research is needed on the mechanisms by which social support relates to better outcomes, on the types of support that are most beneficial and at which developmental periods, and on why some TD siblings receive (or at least perceive that they receive) more or less support. Moreover, data from a larger, more diverse sample that documents the amount and type of social support received across time would likely provide a more comprehensive, generalizable view of the variables and would allow for examination of changes over time to better understand relations temporally.
Although the mean CSBQ score of the children with ASD in the current sample (M = 45.62) was similar to previous clinical samples with ASD (i.e. PDD-NOS; high-functioning autism; Ms ranged from 33.64 to 47.22; Hartman et al., 2006), the research team did not independently verify ASD diagnoses. Direct assessment of family members would offer a more thorough picture of each individual and would permit more pointed examination of the variables. Similarly, having participants complete study questionnaires in a controlled environment (rather than online) would allow for data collection to be more closely monitored and would help to reduce any extraneous error. Although data were collected from multiple informants (i.e. parents and TD siblings), future research would benefit from collecting data from additional sources, such as from the second parent or from teachers, as this would help to correct for any biases, allow assessment of younger TD siblings who are not able to provide self-report, and provide a more comprehensive assessment of child and family functioning.
Although this study helps to address gaps in the literature, additional research on TD siblings remains sorely needed. A variety of other individual and contextual factors not included in the current models likely account for additional variance in TD sibling outcomes. Specifically, future research should investigate distinct traits possessed by TD siblings (e.g. personality characteristics), along with coping styles, and whether these characteristics influence functional outcomes in TD siblings. For example, might TD siblings with certain personality traits who also display a specific pattern of coping styles handle stress more effectively, even if they possess feelings of unmet support? Future studies should more thoroughly examine the neurodiversity common among families. Similarly, future research could build on the current findings by examining different types of social support more closely, particularly how support subtypes may differentially relate to outcomes for TD siblings in certain age groups and/or developmental periods. Similarly, in addition to examining traits among TD siblings and their family members, a systematic examination of techniques aimed at improving support for TD siblings, as well as the availability of this support, is an important next step. Finally, the variability in study outcomes remains a significant concern. As such, efforts to improve the consistency of methodology used by different research groups who study TD siblings and studies meant to differentiate variance attributed to differences in methodology would be of great benefit.
Conclusion
The variety of challenges associated with ASD, along with its genetic predisposition, may result in TD siblings experiencing their own challenges. However, support from others may serve as a buffer against any present stressors and vulnerabilities. This study supports this notion; however, our results suggest that the relation between social support and difficulties in TD siblings may be multifaceted and likely requires precise assessment that incorporates TD siblings’ direct points of view. Specifically, our data indicate that siblings who described social support as both frequent and important reported relatively low levels of emotional and behavioral problems. However, a considerable number of siblings reported a discrepancy in frequency and importance of social support, and TD siblings who reported social support as being highly important but low in frequency exhibited the highest levels of emotional and behavioral problems. Overall, these results underscore the importance of capturing the nuances of perceptions of support received by adolescent TD siblings. Thus, when considering which TD siblings may benefit from intervention, TD siblings who describe receiving little informal social support but who also view social support as highly important may be particularly responsive to efforts aimed at improving social support.
Supplemental Material
AUT763973_Lay_Abstract – Supplemental material for Discrepancy in perceived social support among typically developing siblings of youth with autism spectrum disorder
Supplemental material, AUT763973_Lay_Abstract for Discrepancy in perceived social support among typically developing siblings of youth with autism spectrum disorder by Theodore S Tomeny, James A Rankin, Lorien K Baker, Sophia W Eldred and Tammy D Barry in Autism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.