
Abstract
Developmental approaches to autism treatment aim to establish strong interpersonal relationships through joint play. These approaches have emerging empirical support; however, there is a need for further research documenting the procedures and demonstrating their effectiveness. This pilot study evaluated changes in parent behavior and child autism symptoms following a 12-week Developmental Reciprocity Treatment parent-training program. A total of 22 children with autism spectrum disorder between 2 and 6 years (mean age = 44.6 months, standard deviation = 12.7) and a primary caregiver participated in 12 weekly sessions of Developmental Reciprocity Treatment parent training, covering topics including introduction to developmental approaches, supporting attention and motivation, sensory regulation and sensory-social routines, imitation/building nonverbal communication, functional language development, and turn taking. Results indicated improvement in aspects of parent empowerment and social quality of life. Improvement in core autism symptoms was observed on the Social Responsiveness Scale total score (F(1,19): 5.550, p = 0.029), MacArthur–Bates Communicative Development Inventories number of words produced out of 680 (F(1,18): 18.104, p = 0.000), and two subscales of the Repetitive Behavior Scale, Revised (compulsive, p = 0.046 and restricted, p = 0.025). No differences in sensory sensitivity were observed on the Short Sensory Profile. Findings from this pilot study indicate that Developmental Reciprocity Treatment shows promise and suggest the need for future controlled trials of this developmentally based intervention.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder with symptoms emerging early in childhood and with many children diagnosed within the first 3 years of life. ASD is characterized by deficits in social reciprocity and repetitive behaviors (American Psychiatric Association, 2013). Early interventions for ASD continue to be an important area of study, as the prevalence rate is estimated at approximately 1 out of 59 children in the United States (Centers for Disease Control, 2018). Parent-implemented intervention has been classified as an evidence-based practice for ASD (Wong et al., 2014) and parent involvement is considered an essential component of effective early intervention (National Research Council (NRC), 2001).
While historically autism treatments have ranged widely from those grounded primarily in developmental theory to those based on behavior analytic principles (Thompson, 2013), in recent years the treatment of very young children has led to increasing integration of developmental science with behavioral interventions (Schreibman et al., 2015; Smith and Iadarola, 2015). This movement has been driven, in part, by the concern that highly structured behaviorally based teaching focused on a narrow range of target skills may not adequately address the fundamental developmental and social difficulties that children with ASD experience (Pajareya and Nopmaneejumruslers, 2011). There is now increasing support for a range of treatments known as Naturalistic Developmental Behavioral Inter-ventions (NDBI), which incorporate naturalistic procedures and developmental strategies within early behavioral intervention programming (Dawson et al., 2010; Kasari et al., 2008; Schreibman et al., 2015; Thompson, 2013).
Despite growing evidence for the NDBI approach, there is a need for more empirical research specifically documenting the procedures and expected outcomes, particularly for the developmental treatment strategies (Mahoney and Perales, 2005). Research documenting skill improvement following intensive behavioral intervention based in Applied Behavior Analysis (ABA) comes from multiple large-scale controlled trials (Reichow, 2012). A growing literature now also supports developmental treatment approaches as potentially effective interventions for individuals with ASD (Mercer, 2017). For instance, the general category of Developmental Relationship-based Treatments has been classified as “emerging” (i.e. one or more studies suggest they may produce favorable outcomes but effectiveness has not been established; National Autism Center, 2015). As a core component of NDBI, further investigation of developmental treatment components could meaningfully inform the larger early intervention literature.
Developmental treatment approaches integrate developmental theory and the social-pragmatic models of language acquisition to address core ASD symptoms (Houghton et al., 2013; Ingersoll, 2011). These treatments are based on the premise that establishing strong interpersonal relationships through natural play can foster developmental progress and have a positive impact on the fundamental symptoms of ASD (NRC, 2001). Treatment procedures are based on typical developmental progressions and aim to capitalize on child-initiated teaching episodes, while using developmentally appropriate materials and activities (Houghton et al., 2013). Well-known developmental approaches include the Developmental, Individual-Difference, Relationship-Based (DIR)/Floortime model (Greenspan and Wieder, 1999), Son-Rise (Kaufman and Kaufman, 1976), and Relationship Development Intervention (RDI; Gutstein et al., 2007). According to developmental theory, it is through establishing positive relationships that children with ASD are expected to learn to engage appropriately with others and build affective reciprocity (Rogers, 2005). In addition, developmental approaches have traditionally taken into consideration biological differences that are thought to interfere with learning for children with ASD, such as sensitivities to sensory stimulation (Sandberg and Spritz, 2012). The combination of tailoring intervention to a child’s developmental level, building a positive relationship based on reciprocity and affective sharing, and accommodation of a child’s potential sensory needs is hypothesized to encourage improvement in autism symptomatology.
Optimism about this approach came in part from a rich history of developmental science documenting the importance of the parent–child relationship in development. In their seminal paper, Siller and Sigman (2002) demonstrated that parental responsiveness was associated with long-term benefit in language ability for children with ASD. There is also some evidence that interventions to improve parental responsiveness (e.g. Responsive Teaching) have been associated with improvements in child cognition, language, and social-emotional functioning (Mahoney and Perales, 2003, 2005). Further support for developmental approaches to treatment of ASD comes from studies which have documented positive effects of treating core developmental deficits in ASD (e.g. joint attention; Kasari et al., 2006).
Studies documenting outcomes from specific developmental treatment programs, including a number of randomized controlled trials (RCTs), have highlighted the need for further evaluation of benefits associated with these interventions. For instance, several studies have reported gains in child functional development on the Functional Emotional Assessment Scale following DIR/Floortime (Pajareya and Nopmaneejumruslers, 2011; Solomon et al., 2007), including two RCTs which showed improvement in several measures of parent–child interaction though not in standardized measures of child language and cognition (Casenhiser et al., 2013; Solomon et al., 2014). In another small study, Houghton et al. (2013) found a significant increase in head orientations, gestures, duration of social interactions and total time spent engaged with the examiner for six children with autism who participated in a 5-day intensive Son-Rise Program compared to a control condition of six other children with autism interacting with their parents. However, a few other studies have shown null or mixed effects (see Smith and Iadarola, 2015 for review), or effects restricted to specific social-communication skills and not broader measures of development (Solomon et al., 2014), highlighting the need for additional research using standardized outcome measures.
There have also been a number of RCTs focused generally on evaluating parent-implemented developmental approaches (e.g. Carter et al., 2011; Green et al., 2010; Rickards et al., 2007; Siller et al., 2013, 2014) and on parent training in Developmental Social Pragmatic (DSP) intervention, which have been specifically classified as “probably efficacious” based on methodological criteria from the Journal of Clinical Child & Adolescent Psychology for evaluating treatments of childhood behavior disorders (Smith and Iadarola, 2015). Inclusion of a parent coaching component has also been associated with positive developmental progress in a number of trials of NDBI (e.g. Dawson et al., 2010; Ingersoll and Dvortcsak, 2006; Ingersoll et al., 2005; Kasari et al., 2006; Stahmer et al., 2011; Stahmer and Ingersoll, 2004; Wetherby et al., 2014; Yoder and Stone, 2006). Furthermore, parent education has added benefits by improving treatment intensity and generalization (Kaiser et al., 2000; Steiner et al., 2012), and may reduce parent stress and improve empowerment (Minjarez et al., 2013). In addition, the focus on enhancing the quality of the parent–child relationship could result in additional benefits for parent empowerment, stress-reduction, and family quality of life. Based on this collective evidence, it is likely that developmental strategies are an important aspect of treating ASD symptoms in children and that parent training in developmental approaches has particular promise for producing meaningful change in family functioning and in child development.
Given the rich history of developmental treatment approaches and emerging empirical support, more research is needed to better understand the unique contributions of developmentally-based treatments in terms of both the parent and child outcomes. The potential benefit of this line of research would be to build a stronger foundation for empirical investigation of active ingredients, mechanisms of change, and predictors of treatment response for developmental interventions.
This study is a pilot investigation with the primary goal of examining changes following a 12-week Developmental Reciprocity Treatment (DRT) program. A parent-training model was used in this investigation where parents were taught DRT and were asked to implement the procedures at home. Changes in family empowerment, parenting stress, and quality of life were assessed to evaluate the effect of the treatment on the participating parents and family system. Child outcomes were measured by examining changes in core symptom areas, such as social communication, as measured by the Social Responsiveness Scale (SRS) and MacArthur–Bates Communicative Development Inventories (CDI), restricted repetitive behaviors (Repetitive Behavior Scale-Revised), and sensory abnormalities (Short Sensory Profile). Finally, given that ASD has been associated with impairments in other symptom domains, such as executive function (Smithson et al., 2013) and adaptive skills (Kanne et al., 2011), secondary goals included the assessment of benefits as measured by the Behavior Rating Inventory of Executive Function, Preschool Version (BRIEF-P) and the Vineland Adaptive Behavior Scales, 2nd Edition (Vineland-II). The examination of these domains is particularly important in light of the observations that DRT procedures include strategies that aim at improving flexibility and child self-regulation.
Method
Study design
This was a 12-week uncontrolled trial of DRT as implemented by parents for young children with ASD between the ages of 2 and 6 years conducted between September 2010 and January 2014. The study was registered at ClinicalTrials.gov. This investigation was approved by the Institutional Review Board at the authors’ home institution. Informed consent was provided by each child’s legal guardian(s) before subjects were screened, and inclusion and exclusion criteria were assessed. Subjects who met inclusion criteria were enrolled consecutively and no changes in eligibility criteria were applied throughout the study.
Participants
Children with autism were identified from referral to the Autism and Developmental Disabilities Clinic and the Developmental Behavioral Pediatric Clinic within a large academic medical center. Inclusion criteria included children aged 2.0–6.11 years with a Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association, 2000) diagnosis of autism on the basis of clinical evaluation and established diagnostic tools including the Autism Diagnostic Interview—Revised (ADI-R; Lord et al., 1994) and Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2000). Participants who were medically unstable (e.g. more than one seizure a month) or had a medical diagnosis that causes autism-like symptomatology (e.g. Fragile X, Down syndrome, Angelman’s syndrome, tuberous sclerosis, Rett’s disorder) were excluded.
Intervention
The DRT was based on a developmental early intervention program implemented by clinicians within a local community-based autism treatment program. Consistent with developmental treatment approaches documented in the literature (Greenspan and Wieder, 1999; Rogers and Lewis, 1989), this model aims at building emotional reciprocity through joining with the child in his or her interests and using a play-based and responsive approach. The model incorporates developmental strategies commonly employed across DSP treatments including following the child’s interest, responding to preintentional and unconventional communication attempts, emphasizing affective sharing, and scaffolding communication and play (Ingersoll, 2010). Specifically, the adult uses an enthusiastic, affectively rich interactive style to engage the child and respond to the child’s interaction attempts. The adult attempts to clearly demonstrate what is expected from the child (e.g. each learning opportunity is presented with a clear beginning, middle, and end), give adequate response time, and positively acknowledge all forms of child response. The adult is also responsive to the child’s sensory needs and acts in a predictable manner to enhance the child’s sense of control. For the purposes of this study, the DRT procedures were operationalized to include the following treatment components: adjusting sensory environment, responding to child’s sensory seeking behavior, using appropriate energy and style, joining and following child’s lead, manageable/predictable action, responding to interaction attempts, and building on play and language (see Supplemental Material for definitions). The primary goal of the treatment approach is to build a trusting relationship by respecting the child’s choice of activities and joining the child in play. Underlying developmental theory suggests that this trusting relationship forms a foundation from which the adult can then teach appropriate play and communication skills.
Procedures
Participants completed a screening visit which included informed consent, a clinical interview, establishment of inclusion and exclusion criteria, and a psychiatric and medical history. During this visit they also completed screening measures including the ADI-R, ADOS, and a test of developmental abilities (Mullen Scales of Early Learning).
Participants deemed eligible for the study subsequently attended a baseline visit. Baseline assessments included standardized parent questionnaires related to child social communication skills and repetitive behavior/sensory abnormalities, and clinician rating of Clinical Global Impressions: Severity and Improvement (CGI-S and CGI-I). These assessments were repeated at week 12. In addition, parents were oriented to the structure of DRT in this baseline session.
Weekly 90-min parent–child therapy sessions were provided for 12 weeks (weeks 1–12) in a clinic setting. A standard set of toys was used during play sessions, which included duplicates of each toy to ensure that a parent could imitate the child’s play with any toy. The toys used included puzzles, toy cars, train tracks and trains, bubbles, play dough, squishy balls, baby dolls, children’s books, shape sorters, foam blocks, and popup toys. For each visit, parents were requested to provide a home video recording (minimum duration 10 min) of their interactions with their child during the prior week. The therapist reviewed these videos regularly with the parent and provided feedback as a way to support the parent’s transfer of the DRT skills to the home setting.
The parent training handouts covered five core topics (Supporting Attention and Motivation, Sensory Regulation and Sensory-Social Routines, Imitation Building from Non-Verbal Communication, Functional Language Development, and Turn-Taking). The core features of the treatment taught to parents included being aware of the child’s level of sensory stimulation, responding to the child’s sensory seeking behaviors and adjusting the environment to prevent overstimulation, showing energy and enthusiasm for play with the child, following the child’s lead in the play, being manageable and predictable during interactions through narration and slow movements, responding and praising all interaction attempts, and building on play and language behaviors. See Supplemental Material for a detailed description of each session’s content.
Each topic was presented over the course of two sessions. Upon presentation of each new topic, the therapist reviewed the next handout with the parent, and described the key concepts using examples related to the individual child. The clinician then interacted in play activities with the child for approximately the first half of the session and modeled the skills described while the parent observed. During this modeling, clinicians narrated their use of key skills and described the observed effects of these skills on child behavior. The second half of the session involved parent practice with clinician coaching related to appropriate implementation of techniques relevant to the week’s topic. In the second week for that topic, the clinician began by reviewing the home video and providing comments and feedback on parents’ use of relevant skills at home. Clinicians discussed any areas of difficulty for the parent and answered questions. The remainder of the session was spent jointly playing with the child using the techniques. This play period allowed clinicians to model as well as coach parents on the DRT skills. Parents were encouraged to review learning exercises from the treatment handout to test their own knowledge.
Therapist training
Therapists were trained in the core components of the DRT treatment and provided parent training following the sequence of topics outlined in the parent handouts (see Supplemental Material). The two primary therapists were child psychology doctoral students who received training via didactic instruction, video review, observation of treatment sessions, and in-vivo coaching. These therapists demonstrated greater than 80% DRT fidelity of implementation based on video review of interactions with at least two different children prior to beginning treatment sessions and received regular supervision focused on maintaining DRT fidelity from a clinician with over 5 years of experience implementing and supervising therapists using the DRT model. Assessment of therapist fidelity of DRT implementation was based on the same criteria used to assess parent fidelity which are outlined below.
Measures
Participant characterization
The ADI-R (Lord et al., 1994) and ADOS (Lord et al., 2000) were administered to all study participants and participants were only included if they met the criteria for autism on both measures (including autism spectrum criteria on the ADOS). Developmental functioning was assessed using the Mullen Scales of Early Learning (Mullen, 1995).
Parent questionnaires
A series of parent-report measures were collected to assess social and communication behaviors, repetitive/sensory behaviors, as well as other aspects of child and parent functioning. The Family Empowerment Scale (FES; Koren et al., 1992) is designed to measure empowerment in families with children who have emotional, behavioral, or mental disorders. The Parenting Stress Index, Short Form (PSI/SF; Abidin, 1995) evaluates stress within the parent–child relationship and includes three subscales: Parental Distress, Parent–Child Dysfunctional Interaction, and Difficult Child. The Pediatric Quality of Life Inventory (PEDSQL; Varni et al., 2001) is a measure of health-related quality of life covering both physical and psychosocial aspects of health. The SRS (Constantino and Gruber, 2005) is a parent-report questionnaire which provides a measure of the degree of a child’s social impairment. The MacArthur–Bates CDI (Fenson et al., 2007) Words and Gestures and Words and Sentences versions were also administered to assess the effect of the intervention on communication skills. The Repetitive Behavior Scale-Revised (RBS-R; Bodfish et al., 2000) is a clinical rating scale for measuring the presence and severity of a variety of forms of restricted, repetitive behavior that are characteristic of individuals with autism. The Short Sensory Profile (SSP; Dunn, 1999) is a measure completed by a caregiver that measures the child’s sensory processing abilities and helps determine their effect on daily functioning, including tactile sensitivity, taste/smell sensitivity, movement sensitivity, unresponsive/seeks sensation, auditory filtering, low energy/weak, and visual/auditory sensitivity scales. The Behavior Rating Inventory of Executive Function, Preschool Version (BRIEF-P; Gioia et al., 2002) is a rating scale for measurement of a range of executive functions in preschool-aged children, including inhibitory self-control, flexibility, and emergent metacognition scales. The Vineland Adaptive Behavior Scales, 2nd Edition (Vineland-II; Sparrow et al., 2005) is a measure of adaptive function and includes information across the domains of communication, daily living skills, and socialization.
Clinical ratings of severity and improvement
CGI-S and CGI-I (Guy, 1976) were completed by a clinician with extensive experience in the assessment and treatment of children with developmental disabilities. The clinician obtained information about each child by talking to parents. Given the uncontrolled nature of the trial, the clinician was not blind to treatment assignment or time point. The CGI-S uses a 7-point scale ranging from not at all ill (1) to extremely ill (7). The CGI-I uses a 7-point scale ranging from marked improvement (1) to no change (4) to very much worse (7). In this study, the ratings were specifically focused on social and communication skills.
Parent fidelity of DRT implementation
A structured laboratory observation (SLO) was conducted to assess parent fidelity of implementation of the DRT procedures. The SLO was a video-recorded play session conducted at baseline and 12 weeks. Parents were instructed to encourage their child to play and talk for 10 min using whichever strategies the parent would typically use at home. A standard set of toys was placed in the middle of the room including cars and a car ramp, a train set, dishes, a baby doll, bubbles, books, puzzles, Mr Potato Head set, and a popup toy.
Operational definitions used for observational coding of parent fidelity of implementation of the DRT techniques were based on the components of the parent handout. A rating scale to assess the parents’ correct or incorrect use of the techniques was developed by the authors for this study in consultation with clinicians with experience in the DRT approach being used. Specifically, parent use of the following techniques was assessed: responding to sensory seeking behaviors, appropriate energy/style, joining and following child’s lead, manageable/predictable actions, responding to interaction attempts, building on play, and building on language (see Supplemental Material). After viewing each 2-min segment of video, raters assessed the parent’s overall performance using a 0–4 rating scale: (0—not applicable, implementation of the technique was not appropriate during this interval; 1—adult rarely or never implements the technique appropriately; 2—adult occasionally implements the technique appropriately; 3—adult often implements the technique appropriately; 4—adult always or almost always implements the technique appropriately). Ratings of 3 or 4 were considered correct implementation of that skill area for fidelity summary scoring. Parents who demonstrated at least 80% correct implementation of each of the seven developmental treatment techniques were considered to have met the fidelity criteria. One additional technique, adjusting the sensory environment, was assessed but not included in the calculation of parent fidelity of implementation given that the structure of the SLO was not conducive to parent demonstration of this skill.
Therapists trained in the DRT techniques but blind to treatment time point served as raters and scored videos in random order. Initial training was conducted until raters consistently reached target interobserver agreement (IOA; i.e. 80%). Two raters independently co-scored at least 33% of the videos randomly selected from the total set. IOA was 89% (ranging from 71% to 100% across different video probes scored). Kappa (Cohen, 1960) was also calculated to correct for chance agreement (k = 0.79).
Statistical analyses
Data analysis was conducted with SPSS 23 (SPSS Inc., Chicago, IL). To examine the effects of the 12-week DRT, analyses comparing baseline and 12-week assessments were completed. Repeated measures analysis of variance models were computed with the two time points (time: baseline and week 12) as the repeated measures independent variable. To examine the existence of any predictors of treatment response, Spearman’s correlations were computed to examine relationships between changes in specific outcome measures (SRS and CGI) and baseline characteristics such as age, gender, cognitive, and adaptive functioning.
A type 1 error rate of 0.05 was used for all analyses. Multiple comparison correction was not performed since analyses in this pilot study were exploratory, the sample was small, and preliminary results are intended primarily to guide future research planning. All of the assumptions for analysis of variance (ANOVA) were checked when indicated. In addition, in order to generate more reliable, robust statistics, all of the analyses were performed with 5000 resamples bootstrapping using the bias-corrected accelerated method (Efron and Tibshirani, 1993; Tabachnick and Fidell, 2007).
Results
A total of 48 subjects signed consent to enroll in the study; 12 of these did not meet inclusion/exclusion criteria and 6 decided not to participate. Of the 30 subjects that participated in the trial, 8 subjects did not complete the study. Termination was due to personal/family reasons (e.g. scheduling conflict, family moving, pursuing alternative treatment). Data from 22 subjects were included in the analyses.
The sample of children for whom treatment outcome data are available included 18 males and 4 females with a mean age of 44.6 months (standard deviation (SD) = 12.7 months). Mean Mullen Early Learning Composite Score was 59.6 (SD = 16.0; range: 49–119) indicating that most children in the sample had significant developmental delays; only three children scored above the impaired range (>70). The sample included 3 Caucasian, 15 Asian, 2 Hispanic, and 2 bi-racial participants. Available demographic information for participating children and parents is provided in Table 1. In all, 65% of children were enrolled in a special education preschool or early intervention program at the time of the study and 45% were receiving in-home ABA treatment (mean number of weekly hours = 14). The majority of participating parents were female and married. Parental education level ranged from parents with a high-school diploma as the highest educational degree (15%) to those with a college degree (38%) or graduate degree (46%).
Participant characteristics.
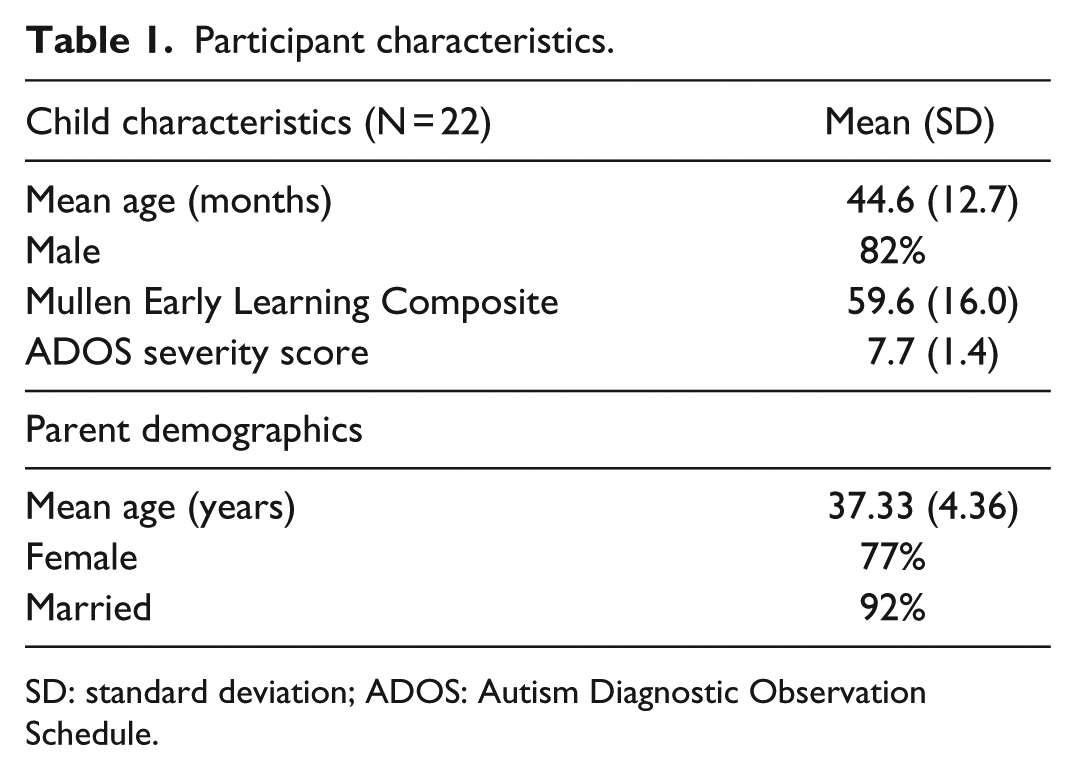
SD: standard deviation; ADOS: Autism Diagnostic Observation Schedule.
Effects on family/parent
Table 2 presents data related to changes in family empowerment, parenting stress, and quality of life following parent training in DRT. The FES total score showed a trend toward significant change between baseline and week 12. Significant changes were specifically observed on the Family subscale (F(1,18): 7.230, p = 0.015) and the Services system subscale (F(1,18): 4.713, p = 0.044). No significant changes in parenting stress were observed on the PSI/SF. Although significant change was not observed in overall quality of life indicators based on the PEDSQL Total Score, significant change was observed between baseline and week 12 on the Social subscale (F(1,18): 5.061, p = 0.037).
Treatment effect on family empowerment, parenting stress, and quality of life.
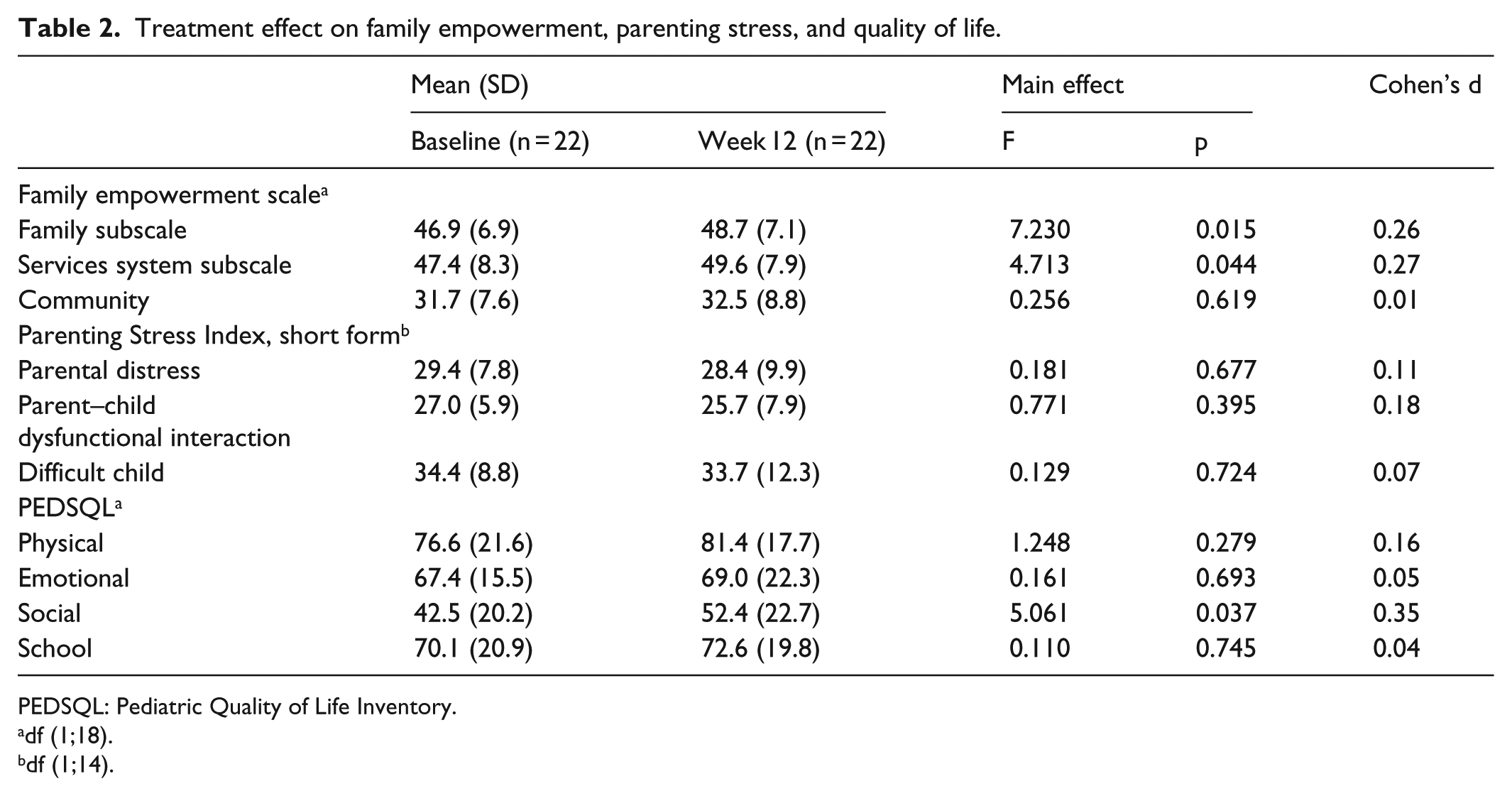
PEDSQL: Pediatric Quality of Life Inventory.
df (1;18).
df (1;14).
DRT fidelity of implementation was also assessed in this pilot trial. By the end of treatment (week 12), 92% of parents demonstrated improvement in fidelity, though only 9 of the 22 (41%) parents who completed the 12-week course of parent training met full fidelity of implementation criteria (80% correct or better) by week 12.
Effects of treatment on core ASD features
Analyses of change in core ASD symptom domains between baseline and week 12 are presented in Table 3. Social behaviors as measured by the total SRS raw score showed significant improvement between baseline and week 12 (F(1, 19): 5.550, p = 0.029). Examination of subscale scores indicated significant improvement primarily in the Social Communication subscale. Effect sizes were small and no significant changes were observed in autistic mannerisms. Communication skills as measured by the CDI Words and Gestures questionnaire showed significant improvement between baseline and week 12 in both number of words understood out of 396 and words produced out of 396, as well as number of words produced out of 680 on the CDI Words and Sentences questionnaire.
Effects of treatment over time on core features.
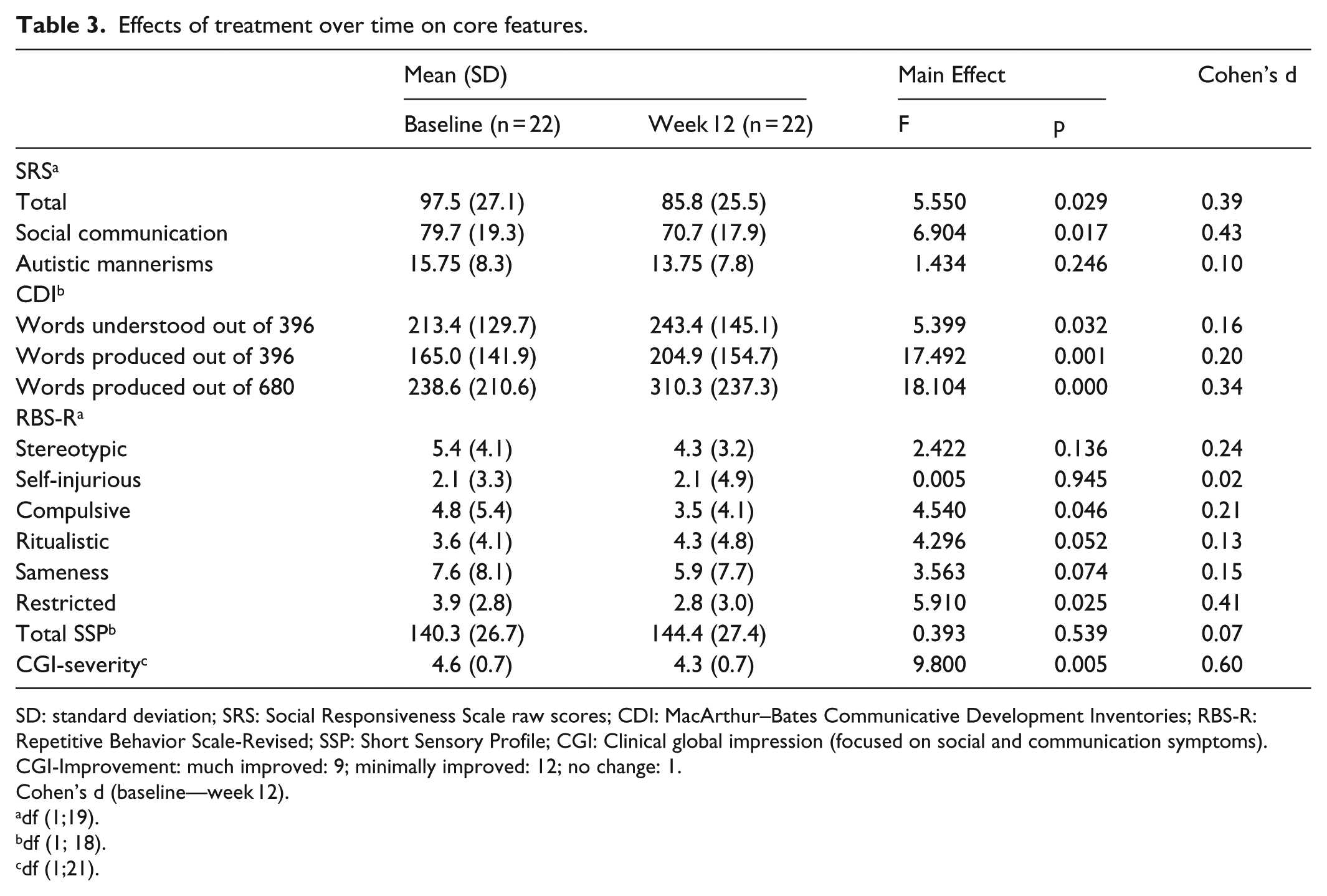
SD: standard deviation; SRS: Social Responsiveness Scale raw scores; CDI: MacArthur–Bates Communicative Development Inventories; RBS-R: Repetitive Behavior Scale-Revised; SSP: Short Sensory Profile; CGI: Clinical global impression (focused on social and communication symptoms).
CGI-Improvement: much improved: 9; minimally improved: 12; no change: 1.
Cohen’s d (baseline—week 12).
df (1;19).
df (1; 18).
df (1;21).
Limited improvement was observed in repetitive behaviors and sensory abnormalities. The overall RBS-R score showed a trend toward significant improvement between baseline and week 12. The Compulsive Behavior subscale scores were statistically improved from baseline to week 12 (F(1,19): 4.54, p = 0.046), as were the Restricted Behavior subscale scores (F(1,19): 5.910, p = 0.025). None of the other RBS-R subscales reached significance. No significant changes with treatment were observed on the SSP, which measures tactile, taste, smell, movement sensitivities as well as under-responsiveness, sensory seeking, auditory filtering, low energy/weakness, and visual and/or auditory sensitivity.
Finally, the severity of social interaction and communication deficits as measured by the CGI severity subscale showed improvement from baseline to week 12 (F(1, 21): 9.800, p = 0.005) with a medium effect size (Cohen’s d = 0.60). Improvements in social interaction and communication were also reported on the CGI-Improvement subscale at week 12. Nine children were rated as much improved, twelve as minimally improved, and one had no apparent change.
In addition, baseline predictors of response including age, gender, Mullen Early Learning Composite Score, and Vineland-II Adaptive Behavior Composite were assessed for the SRS Total Raw Score, SRS Social Communication subscale, and CGI Improvement Scale. Age, gender, and baseline Vineland-II performance were not found to be predictors of treatment response on the SRS or CGI-I. Higher baseline Mullen Composite was significantly associated with greater CGI Improvement (R:−0.460, p = 0.031) but not with SRS ratings at week 12.
Effects on executive function and adaptive abilities
Table 4 presents data related to changes in executive function and adaptive behaviors based on parent report on the BRIEF Preschool version and Vineland-II. Significant change was observed on the BRIEF-P Global Executive Composite (F(1,18): 6.342, p = 0.021) and Emergent Metacognition Index (F(1,18): 8.164, p = 0.010). No significant changes were observed on the Flexibility or Inhibitory Self-control Indexes. The Vineland-II Overall Adaptive Composite Score trended toward significance. The Communication subscale Standard Score improved significantly between baseline and week 12 (F (1,16): 6.251, p = 0.024) as well as the Vineland Receptive V-Scale (F(1,18): 12.2, p = 0.003). The Vineland Expressive V-Scale trended toward significance. However, several Vineland domains such as socialization and daily living did not improve significantly.
Improvement in executive functioning and adaptive abilities.
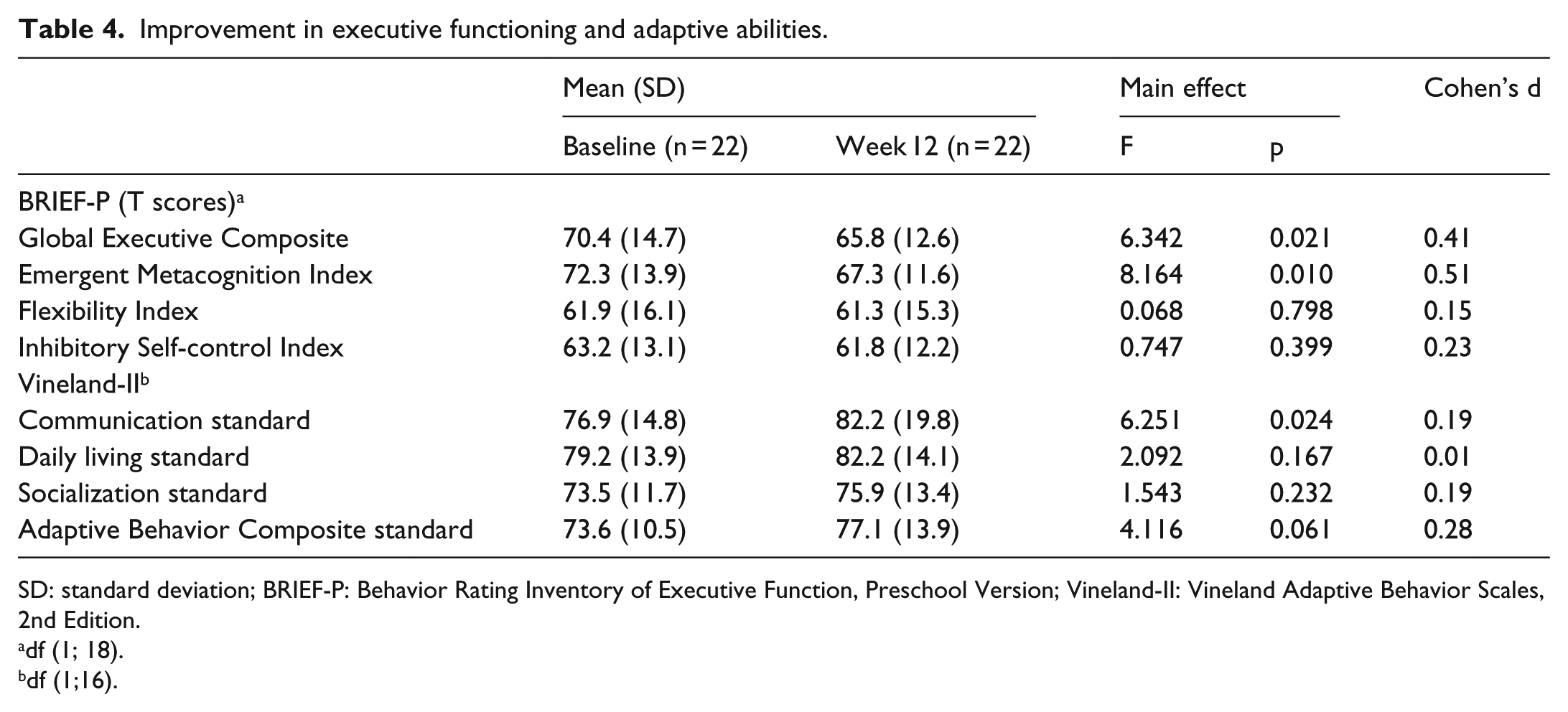
SD: standard deviation; BRIEF-P: Behavior Rating Inventory of Executive Function, Preschool Version; Vineland-II: Vineland Adaptive Behavior Scales, 2nd Edition.
df (1; 18).
df (1;16).
Discussion
This pilot study explored the effects of a 12-week parent training in a developmental treatment for children with ASD. Parent questionnaires following treatment indicated improvement in aspects of family empowerment and social quality of life. Developmental treatment approaches are notoriously more difficult to operationalize and quantify than behavioral approaches (Rogers, 2000; Solomon et al., 2007); nevertheless, this study also measured parent fidelity of implementation of the DRT procedures and child performance on standardized outcome variables. In spite of the fact that many of the participating parents did not meet full fidelity of the implementation criteria by the end of the 12 weeks, results indicate improvements in social deficits, vocabulary, compulsions, and restricted repetitive behaviors, as well as reduced severity of social interaction and communication deficits following DRT. In addition, there was evidence of benefits in some aspects of executive function skills and adaptive communication.
This study provides support for using parent-delivered treatment models to empower parents and provide them with the tools to implement treatment throughout the day in a variety of interactions with their child. Following participation in DRT, parents reported feeling more empowered within the family context and in navigating service systems. Parents also reported improvements in social aspects of child quality of life. These findings provide further support for the parent training approach employed in this study. Parent-training models across treatment types have shown efficacy while reducing cost (e.g. time and money). In addition, parent delivered treatment can lead to better generalization, maintenance of skills, and increased self-efficacy (Dawson and Burner, 2011; Rogers et al., 2012). Beaudoin and colleagues conducted a review of parent training programs in young children with ASD to study the outcomes of the parent training model on child development, parent well-being and parent–child interactions. Outcomes included child gains in receptive and expressive language, frequency of communication, imitative behaviors, joint attention, eye contact; and parent outcomes including high parent satisfaction with the model, meeting fidelity of implementation, and an increase in parent–child interactions (Beaudoin et al., 2014). Although there have been mixed results across studies, evidence of improvement following parent training supports the utility of further research to clarify the effects of parent-training.
While the majority of parents in this study made improvements in fidelity of implementation of the DRT procedures following parent training, less than half of the sample met full fidelity criteria at the conclusion of the 12-week parent-training program. While studies of naturalistic behavioral interventions have shown high levels of parent fidelity after only 12 weeks of training (Hardan et al., 2015), 12 weeks was not sufficient for the majority of the parents in this study to master the DRT strategies. Additional research investigation will be necessary to determine whether modifications to the parent training procedures, greater intensity of training, or longer duration of the trial would be necessary to boost parent fidelity. Improvements in child behavior were nonetheless significant by the end of the study. While several studies have shown that reported parent use of developmental treatment techniques was associated with greater gains in child behaviors (Casenhiser et al., 2015; Solomon et al., 2014), this pattern of child improvement even without full parent implementation has been observed in other research. For instance, Mahoney and Perales (2005) found that while approximately two-thirds of their sample of parents increased their use of responsive interaction techniques following 1 year of weekly parent training, approximately three-quarters of the children improved in language skills. These observations highlight the need for further investigation of the different variables affecting fidelity with the goal of implementing strategies to achieve optimal outcomes.
Improvement in social skills in children with ASD with the 12-week DRT, as measured by the SRS, is promising. Within the measure, the subscale measuring social communication skills improved significantly over the course of the trial. Evidence of more sophisticated social abilities and more thorough understanding of social situations is consistent with other research on developmental treatment models (Rogers, 2005; Sandberg and Spritz, 2012). Other studies have similarly suggested an association between adults imitating a child’s behavior and increases in child social responsiveness, eye gaze, and functional play (Dawson and Adams, 1984; Dawson and Galpert, 1990; Ingersoll, 2012; Tiegerman and Primavera, 1984). As this was an uncontrolled trial, effect sizes were small, and an additional measure of social skills, the Vineland-II Socialization scale, showed only a trend toward improvement at week 12, clinical significance of results must be confirmed with further study. For instance, future research will be needed to determine whether a more intensive or longer-term treatment could yield more widespread social improvements.
Assessment of the children’s language skills found improvements in communication over the course of the 12-week intervention. Specifically, on the CDI, the children showed improvement both in number of words understood and number of words produced. Similarly on the Vineland-II Communication domain, overall communication was significantly improved at week 12. Within the Communication domain, the subsection measuring receptive language was significantly improved and expressive language trended toward significant improvement. These findings are consistent with other studies which have found improvements in functional language use following developmental treatment (Casenhiser et al., 2015). Several investigations have also documented that children with autism show improvement in spontaneous social communication when adults join their focus of activity (Ingersoll and Schreibman, 2006; Lewy and Dawson, 1992). In addition, the severity of social interaction and communication deficits as measured by the CGI severity subscale showed improvement. On the CGI improvement scale, nine of the children were rated as much improved in their social communication symptoms and only one child demonstrated no apparent change. These findings suggest that the DRT intervention may help children to improve their communication abilities, though there may have been some variability in which children had greater success in improving communication. For instance, and consistent with other studies which have indicated that pretreatment developmental levels (i.e. developmental quotient scores) were a significant predictor of language change (Casenhiser et al., 2015), this study found that baseline developmental level on the Mullen predicted greater improvement in social communication skills on the CGI. Future study will be necessary to replicate this pattern and identify other relevant predictors of positive treatment response.
There were also behavioral improvements seen after 12 weeks of DRT. There was a significant decrease in the RBS-R compulsion and restricted subscale scores, however, no improvement was observed on the other subscales (stereotypic, self-injurious, ritualistic, and sameness). The decrease in compulsions and restricted behaviors is promising, as the DRT model stressed the importance of creating a strong relationship as the foundation for expanding the child’s play skills, thus building their ability to be flexible and tolerate new routines or experiences. However, there were no improvements in sensory symptoms overall or in any of the subdomains. Through the DRT model, parents were taught about their child’s sensitivity to sensory stimuli, and instructed to be “sensory detectives” to identify and adapt the child’s environment to suit the needs of the child. Although the concept behind this training is to have the child perceive the caregiver as understanding and safe, it also removes sensory stimuli from the child’s environment that are difficult for the child to manage, consequently reducing their exposure and habituation to those stimuli. Further research will be necessary to better evaluate the importance and effect of this approach.
Improvement in executive functions as measured by the BRIEF-P was also observed, particularly in the area of emergent metacognition. This indicates improvement in the ability to sustain an activity or an idea in working memory and the ability to problem-solve using planning and organizational strategies. Improvement was not observed in the areas of flexibility or inhibitory self-control. Similarly, benefits in adaptive behaviors as related to play and leisure, coping skills, and daily living skills were not observed. There is limited information from the published literature regarding the effect of developmental treatments on executive and adaptive functioning. While some behavioral treatments based on ABA have shown efficacy in increasing adaptive functioning (Carr and Durand, 1985; Cohen et al., 2006; Howard et al., 2005; Lovaas, 1987; Remington et al., 2007), concerns surrounding the spontaneity and generalizability of skills have been raised (Prizant and Wetherby, 1998). Although developmental treatments were developed to target adaptive skills by using everyday play as opportunities for communication and language development, the lack of clear improvement in this study suggests that additional research will be needed to further specify treatment components necessary for improving daily living skills.
There are several limitations of this study. As this was a pilot study, the small sample size and lack of a control group are major weaknesses. A subsequent RCT could provide an important control for maturation effects, as well as the effects of concomitant interventions which, though maintained stable during this trial, could also have affected child outcomes in this sample. A subsequent larger trial could also provide information about potential predictors of treatment response. For instance, given that a relatively small number of parents met fidelity of treatment implementation at post-treatment, it would be informative to investigate the relationship between parent fidelity and child progress in a larger sample. In addition, this sample was demographically unique and included a high number of Asian American families. Further research will be necessary to determine the extent to which parent and child outcomes are similar for a demographically different group. Future research should also focus on how this DRT model compares with other evidence-based treatments. For instance, while DRT incorporated treatment strategies similar to other developmental treatments for ASD (e.g. joining with the child, using an affectively rich interactive style, responding to sensory needs), the model did not include detailed developmental assessment to facilitate specific goal-setting the way other behavioral and developmental models have (e.g. Early Start Denver Model (ESDM); Rogers and Dawson, 2010). In addition, the reliance on unblinded clinician ratings and parent-report measures is still vulnerable to bias, particularly in an uncontrolled trial. Future controlled studies will help provide more objective evidence of improvement. Direct measurement of nonverbal communication, such as eye contact and gestures, which are important deficits in children with ASD, would also be important as these skills are targeted specifically during this intervention but improvement on these domains can be difficult to capture on questionnaires.
Consistent with other studies of early intervention using developmental treatment approaches, this study showed improvement in social deficits and communication following developmental intervention (Houghton et al., 2013; Kasari et al., 2006; Rogers, 2005). Findings also indicated improvements in family empowerment and social quality of life, as well as possible improvement in repetitive behaviors and executive function, suggesting preliminary efficacy of developmental treatment in targeting these important areas of functioning. Controlled trials will be needed to further analyze the degree of benefit and understand any relative advantages of a developmental approach when compared with established treatment models.
Supplementary Material
Lay_Abstract, AUT775538_Lay_Abstract – Effects of a parent-implemented Developmental Reciprocity Treatment Program for children with autism spectrum disorder
Lay_Abstract, AUT775538_Lay_Abstract for Effects of a parent-implemented Developmental Reciprocity Treatment Program for children with autism spectrum disorder by Grace W Gengoux, Salena Schapp, Sarah Burton, Christina M Ardel, Robin A Libove, Gina Baldi, Kari L Berquist, Jennifer M Phillips and Antonio Y Hardan in Autism
Supplementary Material
Supplementary Material, AUT775538_Supplementary_material – Effects of a parent-implemented Developmental Reciprocity Treatment Program for children with autism spectrum disorder
Supplementary Material, AUT775538_Supplementary_material for Effects of a parent-implemented Developmental Reciprocity Treatment Program for children with autism spectrum disorder by Grace W Gengoux, Salena Schapp, Sarah Burton, Christina M Ardel, Robin A Libove, Gina Baldi, Kari L Berquist, Jennifer M Phillips and Antonio Y Hardan in Autism
Footnotes
Acknowledgements
The authors gratefully acknowledge the study therapists and participating families. ClinicalTrials.gov Identifier: NCT0-2037022.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Mosbacher Family Fund for Autism Research, the Teresa and Charles Michael Fund for Autism Research and an anonymous donor. Data management was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1 RR025744.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.