
Abstract
Compared to the social communication domain, considerably less is known about the cause, development, and impact of restricted, repetitive behaviors interests and activities in children with autism spectrum disorder, including possible sex differences. This study examined sex differences in clinically identified (Autism Diagnostic Observation Schedule) restricted and repetitive behavior symptoms using the largest known sample (N = 1024) of age-matched and intelligence quotient–matched female and male children with autism spectrum disorder. More similarities than differences were observed; however, younger higher functioning and older lower functioning females presented reduced rates on the Autism Diagnostic Observation Schedule restricted and repetitive behavior subcategory unusually repetitive/excessive, stereotyped behaviors compared to similar males. These findings identify key restricted and repetitive behavior similarities and differences among young females and males with autism spectrum disorder and emphasize the need for a deeper understanding of the female autism phenotype.
Introduction
Autism spectrum disorder (ASD), one of the most commonly diagnosed childhood developmental disorders, affects approximately 1 in 59 children (Centers for Disease Control and Prevention (CDC), 2018). Diagnosis comes from review of a child’s current behavior and developmental history, with core criteria including social communication impairments and restricted, repetitive behaviors, interests and activities (American Psychiatric Association (APA), 2013). Males are more likely than females to be diagnosed with ASD with mean prevalence ratios at approximately 4:1 (CDC, 2018), with a lower male:female ratio among lower cognitively functioning individuals with intellectual disability (ID) and a higher male:female ratio among higher cognitively functioning individuals without ID (e.g. Nicholas et al., 2008; or see Rivet and Matson, 2011 for review). However, recent studies including a systematic review and meta-analysis of 54 prevalence studies in ASD suggest that the male:female ratio may be lower than current estimates (Jensen et al., 2014; Kim et al., 2011; Lai et al., 2012; Loomes et al., 2017), in part given (1) the likely underreporting of female cases (Giarelli et al., 2010; Russell et al., 2011) and (2) females continue to be underrepresented in research compared to males (Mandy et al., 2012). A result of suspected female underrepresentation and underreporting is a significant gap in our understanding of possible sex differences in the ASD phenotype. Compared to the social communicative domain, far less is known about sex differences in the restricted, repetitive behaviors, interests and activities domain (RRBs; see Lai et al., 2015 for review).
RRBs represent a heterogeneous cluster of behavioral symptoms that include restricted interests, preoccupation with parts of objects, repetitive motor mannerisms, insistence on sameness, sensory behaviors, and strict adherence to specific routines or rituals (APA, 2013). They occur in typically developing children (Çevikaslan et al., 2014; Leekam et al., 2007) and in children with various developmental disabilities including ASD (e.g. Boyd et al., 2010; Hepburn and MacLean, 2009). However, compared to these other populations, RRBs in ASD occur more often, with greater severity, persist across development, and interfere with knowledge transfer, social development, behavioral flexibility, and general adaptive abilities (D’Cruz et al., 2013; Leekam et al., 2011; Matson et al., 2009; Yerys et al., 2009).
Previous research on whether there are sex differences in RRBs yields equivocal findings (e.g. Andersson et al., 2013; Banach et al., 2009; Carter et al., 2007; Hiller et al., 2014; McLennan et al., 1993; Mandic-Maravic et al., 2015; Mandy et al., 2012; Pilowsky et al., 1998; Reinhardt et al., 2015; Zwaigenbaum et al., 2012). Much of the inconsistency though may be due to widespread methodological variation across studies, including participant age, symptom measurement, sample size, and intellectual ability as measured by intelligence quotient (IQ). For example, Andersson et al. (2013) found no differences in RRBs between a group of young higher functioning boys and girls with ASD, while Hartley and Sikora (2009) reported differences in RRBs among similarly aged higher and lower functioning young boys and girls with ASD. The diverse sampling characteristics make it difficult to determine whether discrepancies are driven by methodological variance, or if findings reflect real differences influenced by core developmental factors like age and cognitive ability. Three recent large studies address many of these limitations in examining sex differences in RRBs (Beggiatio et al., 2017; Frazier et al., 2014; Supekar and Menon, 2015).
Two large ASD datasets, the Simons Simplex Collection (SSC; Frazier et al., 2014) and the National Database for Autism Research (NDAR; Supekar and Menon, 2015), have been used to examine differences in overall RRB rates between females and males on the Autism Diagnostic Interview–Revised (ADI-R; Lord et al., 1994). Frazier et al. (2014) found reduced rates in females compared to males on the ADI-R RRB total score and no differences on the Autism Diagnostic Observation Schedule (ADOS) total score (Lord et al., 2002). The sample comprised children aged 4–18 years, with females having significantly lower average IQ than males; however, RRB rates were not moderated by age and were independent of IQ. Focusing on a narrower age range, Supekar and Menon (2015) compared age- and IQ-matched higher functioning females and males (IQ > 70, aged 7–13 years) on the ADI-R RRB domain score and similarly observed reduced rates in females compared to males. Although findings from both studies showed that females present lower overall RRB rates than males, neither the SSC nor the NDAR analyses included RRB subcategory item comparisons.
Examining subcategory item comparisons may help capture potential sex differences across various RRB behaviors and help to narrow the gap in understanding possible RRB sex differences between females and males with autism. Considering this gap, Beggiatio et al. (2017) examined sex differences for each of the ADI-R items in a large group of 129 higher and lower functioning females (Mage 11.3 years; Min 3, Max 42 years) and 465 higher and lower functioning males (Mage 10.5; Min 2, Max 40 years) from the Paris Autism Research International Sibpair (PARIS) Study. Females presented lower rates than males on two ADI-R RRB individual items, circumscribed interests and unusual preoccupations; however, rates were independent of IQ and included individuals with and without ID. The sample included females and males across a large age range; however, consistent with a previous study that examined the circumscribed interests/unusual preoccupations RRB subdomain of the ADI-R in a large group of males and females from multiple affected families with ASD (Szatmari et al., 2012), the finding offers evidence for unique RRB sex differences that an overall RRB score cannot capture and suggest separate RRB profiles present between females and males with ASD.
Together, results from these datasets indicate that compared to males, females may have reduced RRBs overall and among specific RRB subcategories. However, the findings are based on caregiver report, not direct clinical observation. Females and males could differ on RRB subcategories based on standardized clinical observation-based instruments rather than parent-interview data. The ADI-R and the ADOS are considered the two “gold standard” assessments of ASD (De Bildt et al., 2004). However, low agreement has been found between caregiver report and clinical observation in the RRB domain (Stone et al., 1994; Ventola et al., 2006). Questions remain about what specific domains or types of RRBs (if any) differ and whether clinician-based diagnostic instruments at the individual item level differ between females and males. Large-scale studies that use age and IQ matching criteria to examine possible sex differences in the core diagnostic symptoms of RRBs, in particular, how clinical RRB subcategories manifest in females with ASD compared to similar males with ASD, will help provide a first step toward answering these questions. To our knowledge, no studies have examined sex differences in individual subcategories of RRBs on the ADOS nor have studies examined these subcategory comparisons among individual groups of age- and IQ-matched females and males.
The aim of this study is to provide a comprehensive analysis of the ADOS RRB domain, focusing on the RRB subcategories among four individual groups of female and male children with ASD matched on age and IQ. Following recent findings (Frazier et al., 2014; Reinhardt et al., 2015), we anticipate no significant sex differences in ADOS RRB overall rates in our overall population of children with ASD. However, we expect total score differences across our sample of four stratified preschool/primary school age and higher/lower IQ groups. Among the two higher functioning groups, following findings from Andersson et al. (2013) and Harrop et al. (2015), we predict no differences in overall RRB rates for the preschool-aged group; however, considering findings from Supekar and Menon (2015), we anticipate lower overall RRB rates in females compared to males for the primary school-aged group. We also expect differences among our lower functioning age groups (Szatmari et al., 2012). Our primary area of interest is ADOS RRB individual item comparisons. Following the above PARIS database findings, we anticipate higher functioning females will have lower RRB rates in the ADOS RRB item repetitive/excessive interests-stereotyped behaviors, but no differences on all other RRB individual items. We are not aware of RRB individual item sex differences for lower functioning individuals with ASD; analyses for our lower functioning groups are therefore exploratory.
Methods
Participants
Participants for the current sample were selected from the Autism Treatment Network (ATN) registry. The ATN registry is the first and one of the largest autism data registries in North America, with over 7000 enrolled children. The registry is designed as a multi-center observational study that has collected data on children with ASD aged 2–17 years across 17 clinical sites in the United States and Canada. All enrolled subjects in the database meet the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnostic criteria for autistic disorder, Asperger syndrome, or pervasive developmental disorder not otherwise specified (PDD-NOS), or Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) diagnostic criteria for ASD based on a clinical assessment including the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; see Murray et al., 2016 for additional registry details).
All data for the current sample were collected and entered into the registry at the time of initial patient enrollment (baseline). Parent provided demographic information included age at informed consent, sex, ethnicity, race, and primary caregiver education level.
Matching
Our sample was derived from a matching procedure that involved a selection of all female participants enrolled in the ATN registry between 2008 and 2016 for whom age, ASD diagnosis on the DSM-IV of non-PDD-NOS or DSM-5, overall composite IQ score, and ADOS-2 RRB domain and subcategory score information was available. Of the 1141 females in the registry, 512 aged 2–<12 years met full selection criteria. The registry includes children aged 2–17 years; however, given the purpose of the analysis was to differentiate ASD symptomatology between males and females, including all females with data on each variable was important to accurately characterizing them. We therefore restricted our sample to only include females for whom data from the full selection criteria were available. Selected females were then individually matched 1:1 to selected males of the same inclusion criteria on age and IQ. Age in 24-month intervals and IQ stratified by ID cutoff score (⩾70 and <70) were used in matching. The final matched sample included 1024 children (512 females, 512 males) aged 2–<12 years.
Data were analyzed under an institutional review board umbrella protocol used by the ATN/Autism Intervention Research Network on Physical Health’s Data Coordinating Center at Massachusetts General Hospital.
Measures
The ADOS-2, one of two primary diagnostic instruments for ASD, is the second edition of a clinician-based semi-structured standardized assessment of communication, social interaction, play, and restricted, repetitive behaviors interests and activities (Gotham et al., 2007; Lord et al., 2012). The ADOS-2 comprises five modules used for individuals with differing developmental and language abilities. The Toddler Module is used with children aged 12–30 months who do not consistently use phrase speech; Modules 1–3 are used with pre-verbal to verbally fluent children aged 31 months and older; and Module 4 is used with verbally fluent adults. Behaviors during ADOS administration are coded and rated based on categories including language and communication, reciprocal social interaction, play and imagination, and restricted interests and stereotyped behaviors. Associated behaviors are scored on a 4-point severity scale ranging from 0 to 3, with 0 (no abnormality) to 3 (moderate to severe abnormality). The ADOS-2 provides a domain score based on a behavioral algorithm of these categories for each of the two core ASD symptom domains: social communication impairments, and restricted, repetitive behaviors interests and activities (RRBs). Table 1 shows the RRB domain subcategory items by module for Modules 1–3 given to children in this study. Between-item categories are heterogeneous while item content remains similar and consistent across modules allowing for within-item cross module comparability (Gotham et al., 2007, 2008; Kim and Lord, 2010).
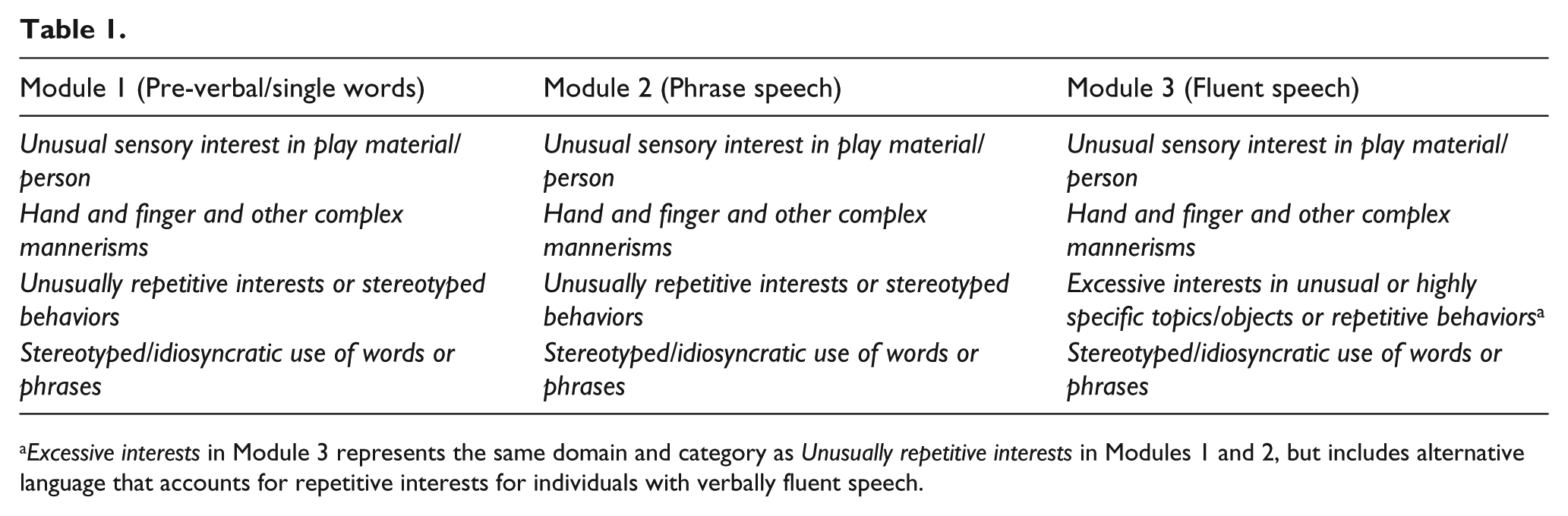
Excessive interests in Module 3 represents the same domain and category as Unusually repetitive interests in Modules 1 and 2, but includes alternative language that accounts for repetitive interests for individuals with verbally fluent speech.
Cognitive data for the majority of participants are available in the form of an overall composite IQ score derived from two well-known standardized IQ instruments: the Stanford–Binet Edition, Fifth Edition (Roid, 2003); and Mullen Scales of Early Learning (Mullen, 1995). Overall IQ for a minority of participants are derived from the following additional commonly used standardized IQ measures: Differential Ability Scales, Second Edition (DAS-II; Elliott, 1990); Wechsler Intelligence Scales (Third, Fourth, and Preschool Eds; Wechsler, 1991, 2002, 2003); and Bayley Scales of Infant Development (Bayley, 1993).
Analysis
Sample characteristics including age group, race, ethnicity, IQ stratified at 70, primary caregiver education level, and autism diagnoses were tabulated overall and by sex in the matched sample. All demographic variables were analyzed as categorical variables. Because males were individually matched to females, we used statistical tests which take this matching into account: McNemar’s tests for dichotomous variables or Bowker’s tests of symmetry for variables with more than two categories were used to examine whether the distributions of each of these characteristics differ significantly by sex.
ADOS RRB domain score was described overall and by gender, and subcategory item scores were described by gender only in the following four individual age- and IQ-matched groups: (1) IQ ⩾ 70 and 2–<6 years, (2) IQ ⩾ 70 and 6–<12 years, (3) IQ < 70 and 2–<6 years, and (4) IQ < 70 and 6–<12 years. The two groups with ID (<70) are considered lower functioning and the two without ID (⩾70) are considered higher functioning (Volkmar et al., 2004). Per ADOS-2 algorithm scoring conventions for calculation of ADOS subcategory item severity scores, item scores of 3 were converted to scores of 2 (Gotham et al., 2007). Means and standard deviations were reported for the RRB total and subscale severity scores. Paired t-tests were used to assess whether total score differed significantly by sex and were selected as the most appropriate method for examining differences, because this method takes advantage of the power afforded by the rigorous individual matching. ADOS RRB subcategory item scores (1 or 2 vs 0) were tabulated, and McNemar’s tests were used to test if the distributions of the dichotomized variables differed significantly by sex. Confidence intervals were set at 95% and significance reported at p < 0.05. Findings are based on specific planned comparisons of two matched groups (males and females) on ADOS total score and ADOS RRB individual item scores (see above); therefore, multiple comparison adjustments were not used for the total score or individual item comparisons (Sokal, 2009).
Results
Sample characteristics
Descriptive demographic and clinical characteristics for our matched sample of 1024 children with ASD (512 female, 512 male; age range 2–<12 years) are shown in Table 2. None of these characteristics differed significantly by sex. Bivariate analyses were used for all RRB domain score and individual item sample comparisons. Table 2 also provides the total number of participants by age, sex, and ADOS Module among those who completed Modules 1, 2, or 3.
Autism Treatment Network study sample demographics and clinical characteristics.
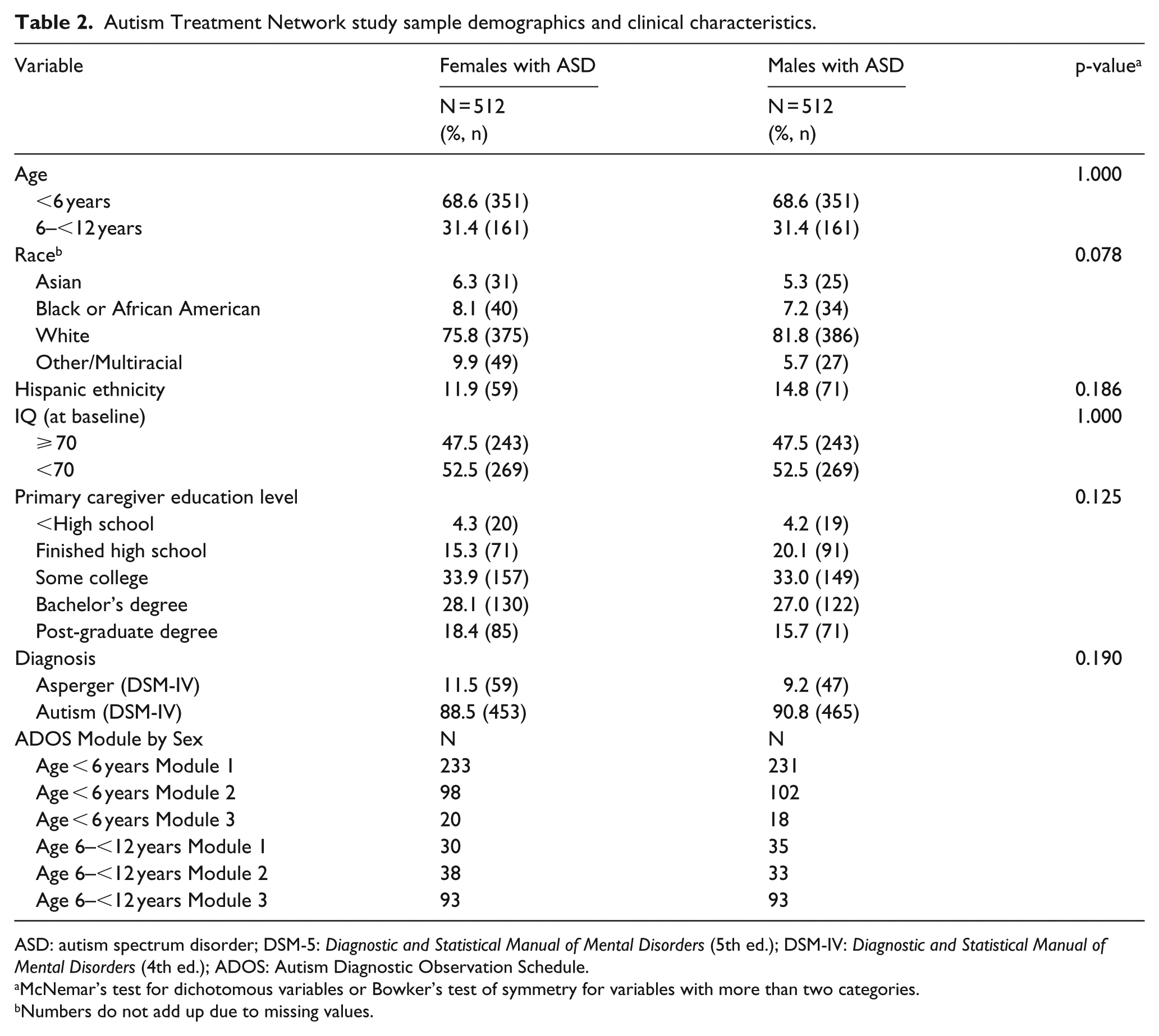
ASD: autism spectrum disorder; DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.); DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.); ADOS: Autism Diagnostic Observation Schedule.
McNemar’s test for dichotomous variables or Bowker’s test of symmetry for variables with more than two categories.
Numbers do not add up due to missing values.
Restricted and repetitive behaviors
ADOS RRB domain score was analyzed by sex overall and for the four age/IQ groups. Table 3 displays the means and standard deviations for the ADOS RRB domain score overall by sex and stratified into four independent groups based on age and IQ. No differences were observed for the domain score overall or in the four groups.
ADOS RRB domain score overall and by group for female versus male children with ASD.
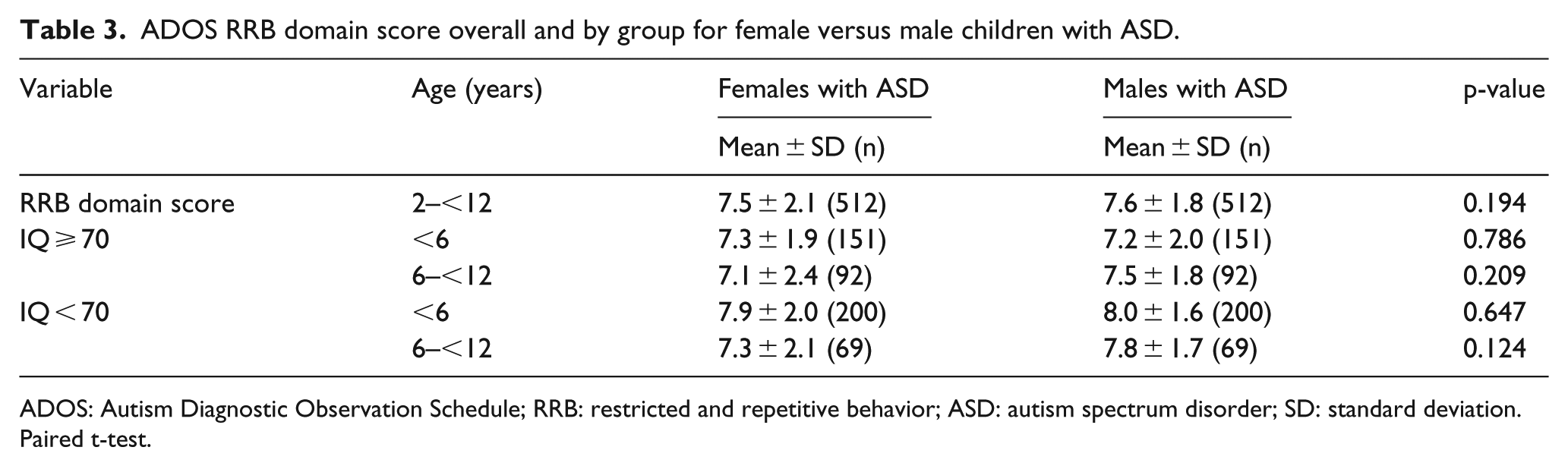
ADOS: Autism Diagnostic Observation Schedule; RRB: restricted and repetitive behavior; ASD: autism spectrum disorder; SD: standard deviation.
Paired t-test.
Table 4 displays the means and standard deviations for the ADOS RRB subcategory item scores by sex. We found differences for the unusually repetitive interest or stereotyped behaviors subcategory in two groups: (1) younger higher functioning females (IQ ⩾ 70) had less (about half the odds) repetitive interests/behaviors than males (McNemar S = 4.17, odds ratio (OR) = 0.45, p = 0.04); and (2) older lower functioning females (IQ < 70) also had less (about 70% less odds) repetitive interests/behavior than males (McNemar S = 4.57, OR = 0.27, p = 0.03). No differences were observed for stereotyped/idiosyncratic use of words or phrases, unusual sensory interest in play material/person, or hand and finger and other complex mannerisms.
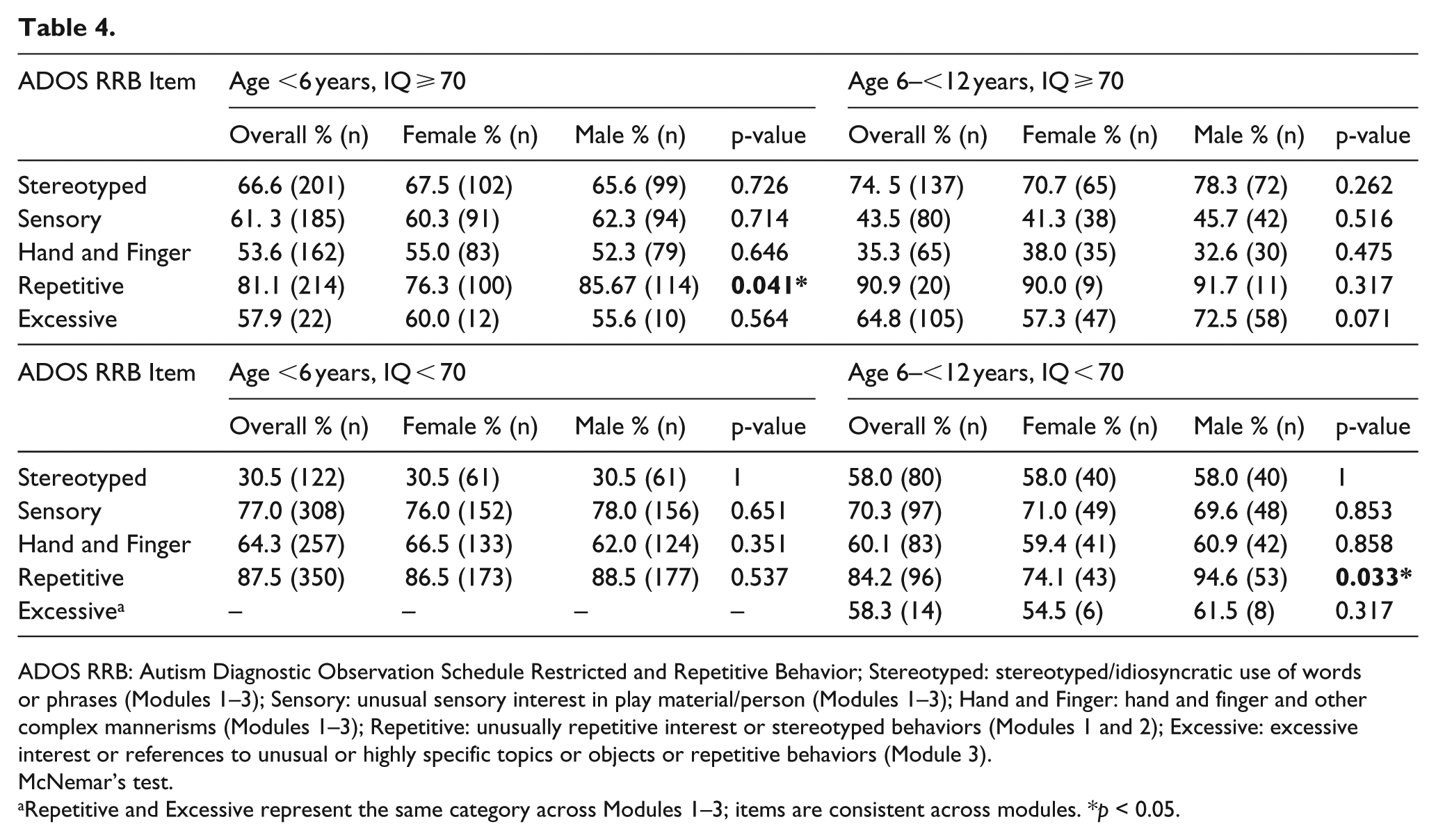
ADOS RRB: Autism Diagnostic Observation Schedule Restricted and Repetitive Behavior; Stereotyped: stereotyped/idiosyncratic use of words or phrases (Modules 1–3); Sensory: unusual sensory interest in play material/person (Modules 1–3); Hand and Finger: hand and finger and other complex mannerisms (Modules 1–3); Repetitive: unusually repetitive interest or stereotyped behaviors (Modules 1 and 2); Excessive: excessive interest or references to unusual or highly specific topics or objects or repetitive behaviors (Module 3).
McNemar’s test.
Repetitive and Excessive represent the same category across Modules 1–3; items are consistent across modules. *p < 0.05.
Discussion
This study uses the largest known sample to date of 1024 individually matched female and male children with ASD to investigate sex differences in the core diagnostic domain of restricted, repetitive behaviors interests and activities (RRBs) based on clinician observation. Our key finding of decreased repetitive interests/stereotyped behaviors in younger higher functioning females and in older lower functioning females compared to similar males demonstrates RRB domain individual item sex differences for young children with ASD (see Table 4). This study provides novel information about the clinical identification of differentiated RRB subdomains between females and males with ASD and lends further insight to the female autism phenotype.
The results from this study identified more RRB similarities than differences between females and males. We observed no sex differences on the ADOS RRB domain score across the full sample and for each of the stratified age/IQ groups. We also observed no differences for three of the four subcategory individual item analyses for each group. Our finding of no overall effect on the RRB domain score contrasts with a meta-analysis by Van Wijngaarden-Cremers et al. (2014) who observed lower rates of RRBs in females than males aged 6–12 years. However, the meta-analysis included findings from both clinician (ADOS) and caregiver (ADI-R) report, whereas this study only included a clinical sample based on direct clinical observation (ADOS). The inherent bias in our sample that only included children referred to an ATN site and the potential differences between direct clinician observation versus historical report (see below) may also account for this discrepancy. Taken together, our findings do not show enough evidence to reject our hypotheses of no differences overall and for the higher functioning preschool-aged group. These results support previous studies showing similar RRB domain scores on clinician-reported diagnostic measures between female and male children with ASD (Andersson et al., 2013; Frazier et al., 2014; Harrop et al., 2015; Reinhardt et al., 2015). We did not confirm our expectation that RRB domain differences emerge among primary school-aged higher or lower functioning groups (Supekar and Menon, 2015; Szatmari et al., 2012). However, the discrepancy may reflect instrument use; these studies used parent report data, whereas this study used clinical observation data. Clinical and caregiver perspectives of RRBs may differ. Previous studies show discordance and moderate to low associations in the RRB domain between the ADI-R and the ADOS in mixed sex samples (Le Couteur et al., 2008; Lemler, 2012; Ventola et al., 2006) and in exclusively female samples (Kopp et al., 2010).
Planned comparisons for our individual item analyses suggested that females in the higher functioning group (IQ ⩾ 70) present reduced rates for the repetitive/excessive interests—stereotyped behaviors category. We did find a reduced rate in females in both age groups, but only the results in the younger age group for Modules 1 and 2 were statistically significant. Note, however, that relatively few children were analyzed in the older age group for this item for Modules 1 or 2 and in the younger age group for this item for Module 3. The sparse data in these analyses are reasonable given verbal fluency abilities among higher functioning children across these two age groups (e.g. Charman, 2004; Corbett et al., 2009). The difference between females and males for the older lower functioning age group for the repetitive/excessive interests—stereotyped behavior item in Modules 1 and 2 was also statistically significant. However, this result was exploratory; therefore, additional studies using planned hypotheses are needed to confirm the finding. This item was also less frequent in older lower functioning females than males for Module 3 (and not measured in the younger age group).
The effect sizes for our two discordant groups indicate that compared to younger higher functioning females, younger higher functioning males were about twice as likely, and older lower functioning males were about four times as likely, to engage in repetitive/excessive interests—stereotyped behaviors. However, findings should be interpreted with caution as the differences observed account for approximately 25% of the females among the discordant groups. A majority of females (76%) in the younger higher functioning group and a majority of females (74%) in the older lower functioning group presented with repetitive/excessive interests—stereotyped behaviors (Table 4). Overall, these results seem to suggest that there are more similarities than differences across the ADOS RRB subcategory items between females and males; however, repetitive/excessive interests—stereotyped behavior is less frequent in preschool-aged higher functioning females than preschool-aged higher functioning males and is less frequent in primary school-aged lower functioning females than primary school-aged lower functioning males.
Findings from our higher functioning groups on the repetitive/excessive interests—stereotyped behaviors item support the phenomenon observed in higher functioning females with ASD to be more motivated or more effective at concealing or camouflaging certain autism symptoms than higher functioning males with ASD (Attwood, 2006; Gould and Ashton-Smith, 2011; Rynkiewicz et al., 2016; Rynkiewicz and Łucka, 2015). In addition, our findings could indicate that lower functioning primary school-aged females are able to camouflage repetitive interests/stereotyped behaviors, although this finding was exploratory (see above). To be clear, no evidence from this study indicates that our sample of females (or males) endeavored to mask or conceal RRBs, and our findings showed that two female groups presented with lower rates of repetitive interests/stereotyped behaviors. However, concealing autism symptoms such as social communication difficulties have been described or reported in primary and secondary school-aged girls and adult women, but not in younger preschool-aged girls (Cook et al., 2017; Dean et al., 2016; Hull et al., 2017). Higher functioning girls who conceal social communication difficulties may appear less functionally impaired. Therefore, other ASD-related developmental concerns such as RRBs may be required to get evaluated by a clinician for ASD. This may, in theory, explain why higher functioning older girls in our sample did not show lower rates compared to boys, but younger preschool-aged girls and older lower functioning girls did show lower rates compared to boys: preschool-aged higher functioning girls may not be old enough to mask social communication difficulties; however, primary school-aged girls are known to conceal these behaviors (e.g. Cook et al., 2017), and suggests why we might be seeing the observed pattern of findings.
Moreover, compared to higher functioning individuals with ASD, lower functioning individuals with ASD have poorer adaptive behavior and social skills, and increased challenging behaviors (see Matson and Shoemaker, 2009 for review). ID impairs language and social cognition, which tend to be core areas of concern for children diagnosed with ASD. Therefore, associated communication and social skills abilities that support social skills impairment coping strategies in higher functioning females with ASD are thus further compromised in lower functioning females. Lower functioning primary school-aged females exhibiting fewer RRBs than their male counterparts would still be evaluated for ASD as their social communication impairments are more likely to be displayed and thus more likely to contribute to a diagnosis.
Recent studies investigating RRB sex differences in ASD offer further theoretical support to our explanation of this study’s results. In an examination of clinician-reported autism diagnostic criteria and teacher-reported autism-related behavioral concerns among higher functioning young girls and boys with ASD, Hiller et al. (2014) showed that the types of restricted and repetitive interests demonstrated by a majority of girls younger than 7 years of age were “random,” whereas a majority of males’ restrictive and repetitive interests in this age group focused on “wheeled toys.” Compared to males, the restricted and repetitive interests among females were thus more difficult to categorize and “identify as atypical” (Hiller et al., 2014: 1391). These results provide additional support for this study’s findings, given that if the types of restricted and repetitive interests in young higher functioning females with ASD are more difficult to categorize, they may be less likely to identify and therefore in theory captured less often than males who engage in more easily identifiable RRB interest type categories. Hull et al. (2017) recently reported that higher functioning adults with ASD express the ability to use compensatory strategies to camouflage their RRBs. However, the reported techniques are rather sophisticated and include recognizing their RRBs, developing a strategy to hide or conceal repetitive/excessive behaviors, and performing these compensatory behaviors in the appropriate context. This type of self-referential behavioral recognition, understanding of behaviors in others, systematic planning, and behavioral execution is unlikely to occur in young preschool-aged females (or males) with ASD (e.g. Pellicano, 2012). Studies examining the development of the ability to camouflage RRBs in females with ASD, however, will further inform both our understanding of this domain and our understanding of the female autism phenotype.
Limitations and future directions
Data for this study were derived from children with ASD who participated in ATN clinical sites. Findings are thus based on a sample of convenience and therefore may not be generalizable to the full population of individuals with ASD. Moreover, it is important to recognize the potential for sampling bias in this study as females with more muted or distinct RRBs are less likely to be identified and diagnosed with ASD and therefore more likely to be excluded from this study. This challenge relates to the broader issue of whether the DSM autism diagnostic criteria is potentially gender-biased and unable to capture the subtleties of the female autism phenotype (Haney, 2016). Sampling bias could also result from the ATN registry participants who did not meet full inclusion criteria (see section “Matching”). The registry data does not ascertain the reason participant data was missing and therefore cannot inform whether findings resulted in systematic bias.
We also analyzed autism symptomatology using the ADOS-2, a direct observation measure. Designed for clinical settings, the ADOS-2 does not provide a comprehensive assessment of RRBs. And it remains unknown the extent to which clinical settings favor a full expression of RRBs (Gardenier et al., 2004). However, the Repetitive Behavior Scale–Revised (RBS-R; Lam and Aman, 2007) and Repetitive Behavior Scale for Early Childhood (RBS-EC; Wolff et al., 2016) target a broad range of RRBs. Large-scale studies should investigate potentially female-specific RRBs using comprehensive RRB measures like these in addition to the ADOS and ADI-R to assess a more complete range of RRBs. Studies show that the combination of direct clinical observation and parent report yields a more accurate representation of an individual’s ASD phenotype (e.g. Kim and Lord, 2012; Risi et al., 2006); large-scale studies should also look to examine sex differences using well-matched samples that include fine-grained analyses of RRB subdomains that include both clinical observation and in-depth historical report. Furthermore, although our results were significant at the 0.05 level, we did not adjust for multiple comparisons, decreasing our ability to control for type I error for our pre-specified hypotheses; therefore, small differences may have resulted by chance. Future studies using pre-specified hypotheses with larger samples are necessary to confirm these findings. Finally, this study identified similarities and differences in the rates of RRBs between females and males. However, future research should consider investigating sex differences in the quality and nature of RRBs. This may help to better understand the results of this study, advance knowledge of the female autism phenotype, and inform diagnostic testing.
Conclusion
This study provides the largest examination to date of individually matched females and males with ASD on the core diagnostic domain of restricted and repetitive behaviors (RRBs). Our study adds novel information about the female ASD phenotype, specifying sex similarities and differences in RRBs based on age and cognitive functioning. To our knowledge, this study is the first to describe the similarities and differences in RRBs based on clinical observation at the individual item level between a large sample of individually matched females and males. Findings suggest that females and males exhibit many similarities and important differences in clinically measured RRBs. For the most part, there were no differences by sex. Notably, though, a unique pattern did emerge: preschool-aged higher functioning females and primary school-aged lower functioning females presented decreased rates of repetitive interests/stereotyped behaviors compared to similar males. Future studies should investigate individual item RRB differences in large scale similarly age- and IQ-matched groups of females and males using other diagnostic tools for ASD.
The limited evidence, mixed results, and overall lack of knowledge about the female autism phenotype increase the challenges in detection and diagnosis and make it more difficult for clinicians to recommend effective treatment strategies (Van Wijngaarden-Cremers et al., 2014). Narrowing the gap in understanding the phenotypic sex differences in ASD may help to prevent possible delayed diagnoses, missed diagnoses, or missed referrals in females with autism (Halladay et al., 2015; Rivet and Matson, 2011). Finally, deepening the understanding of the female autism phenotype and thus the possible sex differences in core domains that define autism may help to determine (1) why females are diagnosed with ASD at disproportionately lower rates than males and in what ways might the autism phenotype present differently in females and males and (2) will help identify potential early developmental markers that can be used to help improve treatment and thus functional outcomes for both females and males with ASD.
Supplemental Material
AUT786490_Lay_Abstract – Supplemental material for Sex differences in restricted repetitive behaviors and interests in children with autism spectrum disorder: An Autism Treatment Network study
Supplemental material, AUT786490_Lay_Abstract for Sex differences in restricted repetitive behaviors and interests in children with autism spectrum disorder: An Autism Treatment Network study by John Knutsen, Morgan Crossman, James Perrin, Amy Shui and Karen Kuhlthau in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This Network activity was supported by Autism Speaks and cooperative agreement UA3 MC11054 through the US Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Research Program to the Massachusetts General Hospital. This work was conducted through the Autism Speaks Autism Treatment Network. This project was supported by grant numbers T32HS000063 and K12HS022986 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.