
Abstract
This study investigated the comorbid conditions in a whole country population of children/young people aged 0–24 years with and without autism. Data were drawn from Scotland’s Census 2011. We calculated the percentage with autism, their extent of comorbid conditions, odds ratio (with 95% confidence intervals) of autism predicting comorbidities, adjusted for age and gender, and odds ratio for age and gender predicting comorbidities within the cohort with autism. A total of 25,063/1,548,819 (1.6%) had autism: 19,880 (79.3%) males and 5183 (20.7%) females. Autism had an odds ratio of 5.4 (5.1–5.6) for predicting deafness/partial hearing loss, odds ratio of 8.9 (8.1–9.7) for blindness/partial sight loss, odds ratio of 49.7 (38.1–64.9) for intellectual disabilities, odds ratio of 15.7 (13.4–18.5) for mental health conditions, odds ratio of 15.8 (14.1–17.8) for physical disability and odds ratio of 3.9 (3.8–4.0) for other conditions. Females with autism were more likely to have each additional condition than males, including intellectual disabilities, suggesting they may have more severe autism than males and adding evidence that autism may be currently underdiagnosed in more intellectually able females. These conditions are disabling and have a significant impact on long-term quality of life; their coexistence with autism adds extra complexity. It is important to raise clinicians’ awareness of this extent of comorbidity, and to have accurate prevalence data to plan prevention and intervention measures, and to follow health inequality trends.
Introduction
Children and young people with autism can have additional comorbidities. While some health conditions appear to be more common, such as epilepsy, intellectual disabilities and gastrointestinal conditions, there is a general dearth of research on other long-term conditions such as hearing, visual impairments and physical disabilities (Kannabiran and McCarthy, 2009; Kohane et al., 2012; Matson and Goldin, 2013). This may add to the likelihood of comorbid conditions being misdiagnosed or overlooked and is particularly important with regards to long-term conditions due to the impact they may have over time. If individual long-term conditions are indeed more common in children and young people with autism, then a greater awareness of them would be important.
Inconsistent findings were reported in a systematic review on hearing impairments in children and young people with autism (Beers et al., 2014). Only five studies were included, none were recent and all had small samples of only 22–199 children and adolescents with autism. Two studies reported normal peripheral hearing (Gravel et al., 2006; Tharpe et al., 2006), two reported possible increased peripheral hearing loss, but no prevalence estimates (Jure et al., 1991; Tas et al., 2007), and one reported mild to moderate permanent hearing loss or isolated high frequency hearing loss in 7.9%, pronounced unilateral hearing loss and mild hearing loss in the contralateral ear in 1.6%, and pronounced to profound bilateral hearing loss or deafness in 3.5% (Rosenhall et al., 1999). A review of studies on the epidemiology of autism reported a 1.7% median prevalence (range = 0%–5.9%) for hearing deficits and 1.3% (range = 0%–11.1%) for visual deficits (Fombonne, 2003) from 7 and 5 studies between 1966 and 2001. These did not include the studies reported by Beers et al. (2014) and no further information was provided. Subsequent to these reviews, a study of 8-year-old children in Atlanta, USA, 1996–2010, reported hearing loss in 1%, and vision impairment in 1% of children with autism (Van Naarden Braun et al., 2015). We have not identified any studies examining the prevalence of physical disability in children or young people with autism.
There are more studies on intellectual disabilities and mental health than for sensory impairments and physical disabilities, but changing definitions of autism over time render some findings less relevant today. Review of epidemiological surveys of autism shows that intellectual disabilities are more common than in other people, with estimates in the region of 50%–70% (Fombonne, 2003). However, the reviewed studies included only 6–241 people with autism and were of variable methodology. Only five were drawn from a wide population-base (Fombonne, 2003). The studies are further limited by their reporting timespan, which ranged from 1966 to 2001. This is important as concepts have moved from a stricter ‘Kanner syndrome’ definition of autism to that of an autism spectrum condition in recent years, so while the reported prevalence rates of autism have increased, the proportion of those with autism identified with comorbid intellectual disabilities is likely to have fallen. This decrease can be seen in the records of 8-year-old children in Atlanta, USA, in whom the prevalence of recorded autism increased from 4.2/1000 in 1996 to 15.5/1000 in 2010, while the proportion with autism who also had a record of intellectual disabilities fell from 59% to 37% in this same period (Van Naarden Braun et al., 2015). Subsequent to the review, there have been further reports. The Stockholm Youth Cohort, aged 0–17 years resided in Stockholm County, Sweden between 2001 and 2007 (n = 444,154) had a prevalence of autism in 2007 of 11.5/1000, of whom 42.6% had comorbid intellectual disabilities (Idring et al., 2012). Medical records were scrutinised of children aged 8 years between 2003 and 2012, according to the childhood disability registry of Haute-Garonne, south-western France, which supports education. Autism was recorded in 3.6/1000, of whom 51.2% also had intellectual disabilities (Delobel-Ayoub et al., 2015); the authors comment that their reported rate of autism is lower than in other studies. For 1993–2005, Western Australian data from combined education and Disability Services Commission recorded 5.1/1000 to have autism, of whom 74.5% were also recorded to have intellectual disabilities (Bourke et al., 2016). This rate for autism is also lower than that reported recently from other countries, which may account for the higher proportion recorded as also having intellectual disabilities. Overall, there are few contemporary studies that have reported the prevalence of intellectual disabilities in children and young people with autism, and estimates vary due to differing population sampling and methodological designs; hence, accurate prevalence rates are unclear.
Most studies of mental ill-health in children and young people with autism have investigated small, often highly selective clinical samples. An exception to this finding is as many as 70% of children with autism may have at least one comorbid psychiatric disorder (Simonoff et al., 2008). This study had the strengths of being population based (with a reported prevalence rate of autism spectrum disorder of 11.2/1000) and conducting detailed assessments but was small in size, including 112 pupils aged 10–14 years identified to have autism spectrum disorder, and did not have direct general population comparisons. As it was conducted in the early 2000s, it pre-dates the further broadening of criteria currently in use for autism spectrum disorders (Simonoff et al., 2008). Reviews of studies of prevalence rates of depression (Stewart et al., 2006) and anxiety (Van Steensel et al., 2011; White et al., 2009) show that rates vary considerably between included studies (4.0%–34.0% for depression; 11.0%–84.0% and 34.8%–39.6% for anxiety) and studied population sizes were small (12–85, 7–487 and 7–301 children and young people, respectively), but these conditions seem to be more common in child and youth populations with autism, particularly girls. Reviews of studies investigating suicidal attempts, ideation and behaviour in children and adolescents also show higher prevalence for people with autism, but reviewed studies differ significantly in study period, age of individuals, diagnostic criteria and sampling methods (Hannon and Taylor, 2013; Segers and Rawana, 2014). It has been shown in child and youth populations aged 5–18 years with autism that bipolar disorder is more common in Asperger syndrome than autism spectrum disorder (8.6% vs 3.0%) and the prevalence increases with age (2.3% at age 5 and 10.4% at age 18) (Rosenberg et al., 2011).
In summary, existing studies are mostly small, and few are contemporary with regards to the prevalence of intellectual disabilities and mental health conditions in children and young people with autism; results are particularly limited with regards to visual and hearing impairments, and we found no studies on physical disabilities. The current study therefore aimed to investigate the prevalence of the specific long-term comorbid conditions of deafness or partial hearing loss, blindness or partial sight loss, intellectual disabilities, mental health conditions, physical disability, and other conditions, in children and young people with autism, compared with their peers without autism. We hypothesised that these conditions would be more prevalent in those with autism.
Methods
Data source
The data source was Scotland’s Census, 2011. This provides information on the number and characteristics of Scotland’s population and households on the census day, 27 March 2011. The census is undertaken every 10 years. It includes the whole Scottish population: people living in communal establishments (such as care homes and student halls of residence) as well as people living in private households. Scotland’s Census is probably one of few country censuses, which identifies people with autism.
In 2011, the census in Scotland was estimated to have achieved a 94% response rate (National Records of Scotland (NRS), 2013). The Census requires the form to be completed by the head of household or joint head of household on behalf of all occupants in private households, and the manager on behalf of all occupants in communal dwellings. It is a legal requirement to complete the Census: the Census form clearly states this, and that a head of household not completing it, or supplying false information can be fined £1000. The Census team follows up non-responders and also provides help to respond when that is needed, hence the high 94% completion rate.
The Census team adjusted for the missing 6%. This imputation process was conducted using a Census Coverage Survey (including around 40,000 households) to estimate numbers and characteristics. The Coverage Survey and Census records were matched using automated and clerical matching. All Census individuals, including individuals reporting long-term health conditions, were deterministically matched to check if any records were duplicated. Individuals estimated to have been missed from the Census were then imputed, using a subset of characteristics from real individuals, including information on their health. The process of development of the Scotland’s Census 2011 Edit and Imputation Methodology was adapted from the Office for National Statistics rigorous and systematic guidelines, which are available here:
http://webarchive.nationalarchives.gov.uk/20160108193745/ http://www.ons.gov.uk/ons/guide-method/method-quality/survey-methodology-bulletin/smb-69/index.html
Further details on how the Census population estimates were arrived at are also available here:
http://www.scotlandscensus.gov.uk/documents/censusresults/release1b/rel1bmethodology.pdf
Approval was gained from the Scottish Government for secondary analysis of the Census data. Full details of the methodology and other background information on Scotland’s Census 2011 are available at:
Census variables
Self-/proxy reporting was used to identify people with autism from the individual Census questionnaire, where Question 20 was as follows: ‘Do you have any of the following conditions which have lasted, or are expected to last, at least 12 months? Tick all that apply’. Respondents were given a choice of 10 response options: (1) deafness or partial hearing loss, (2) blindness or partial sight loss, (3) learning disability (e.g. Down’s syndrome), (4) learning difficulty (e.g. dyslexia), (5) developmental disorder (e.g. autistic spectrum disorder or Asperger’s syndrome), (6) physical disability, (7) mental health condition, (8) long-term illness, disease or condition, (9) other condition and (10) no condition. A write-in box was also included for the respondents to report types of ‘other’ condition. The Census team combined the ‘long-term illness, disease or condition’ and ‘other condition’ data into one category henceforth referred to as ‘other condition’. The Census team also used imputation for the 14.7% who did not tick any of the boxes in Question 20, based on their free text answers for this question and answers to other health questions in the Census, which increased the completion rate to 97.4%. For the remaining 2.6%, the Census team assumed the most plausible explanation was that the person had no long-term condition but did not see the ‘no condition’ check box at the end of the question.
Importantly, while the question included the broad term developmental disorder, it only prompted respondents to reply with regards to autistic spectrum disorder or Asperger’s syndrome. We therefore interpret responses to this question as relating to people who know they have autism/Asperger’s syndrome, henceforth referred to as autism. In addition, the question distinguished autism from learning disability (which in the United Kingdom is synonymous to the international term ‘intellectual disabilities’), learning difficulties such as dyslexia and mental health condition.
Data analysis
We calculated the number and percentage of children and young people with and without autism by gender. We then calculated the number and percentage of children and young people with and without autism reporting deafness or partial hearing loss, blindness or partial sight loss, intellectual disabilities (referred to as learning disability in the Census), mental health conditions, physical disability, and other conditions. Within the whole population, we then used six logistic regressions to calculate odds ratio (OR; with 95% confidence interval (CI)) of autism predicting the binary response of having each of the six specific types of additional health conditions, adjusted for age and gender. Age was categorised into groups of 0–15 years and 16–24 years, with the group of 0–15 year olds being the reference group. Gender was a binary variable; the reference group was male. We calculated cluster robust standard errors, given the likelihood of some related family members in the data. We then calculated the ORs for age and gender in predicting each of the six comorbidities within the population with autism.
Due to the imputation process by the Census team, the dataset had 100% completeness; hence no exclusions were made in the analyses.
Analyses were conducted with STATA/SE software version 12.
Participant characteristics
Scotland’s Census 2011 includes records on 5,295,403 people; of whom 916,331 are children aged 0–15 years and 632,488 are young people aged 16–24 years. A total of 17,348/916,331 (1.9%) of children and 7,715/632,488 (1.2%) of young people were recorded to have autism. Hence, overall, 25,063/1,548,819 (1.6%) of the total population of children and young people in Scotland were recorded to have autism. Of children and young people with self/proxy-reported autism, 19,880 (79.3%) were males and 5183 (20.7%) were females, compared with 766,109 (50.3%) males and 757,647 (49.7%) females in the population without autism. A total of 138 (0.8%) children and 362 (4.7%) young people with autism lived in communal establishments as opposed to private households. Children and young people with autism were more likely to have Caucasian ethnicity (χ2 = 194.59; df = 1; p < 0.001 for children; χ2 = 202.92; df = 1; p < 0.001 for young people) and to live in the most deprived neighbourhoods (χ2 = 196.68; df = 1; p < 0.001 for children; χ2 = 24.00; df = 1; p < 0.001 for young people) than those without autism. Tables 1 and 2 present demographics.
Demographic characteristics of children and young people with and without self/proxy-reported autism in Scotland.
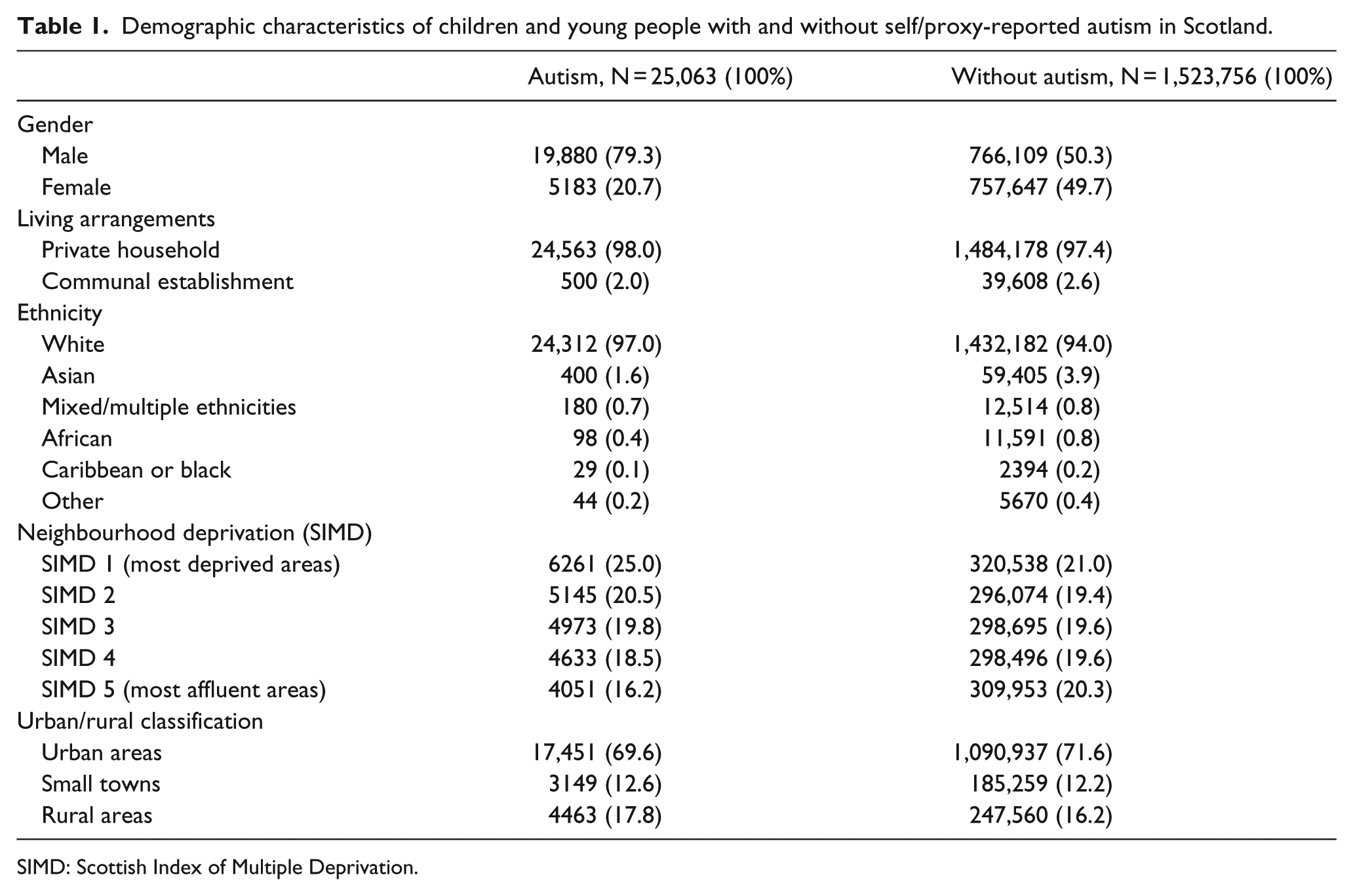
SIMD: Scottish Index of Multiple Deprivation.
Number and proportion of children and young people with and without self/proxy-reported autism in Scotland by age and gender.

Results
Prevalence of comorbid health conditions
Table 3 shows the proportion of the children and young people with and without autism who had each of the additional health conditions.
Prevalence of comorbidities in children and young people with and without self/proxy-reported autism by age and gender.
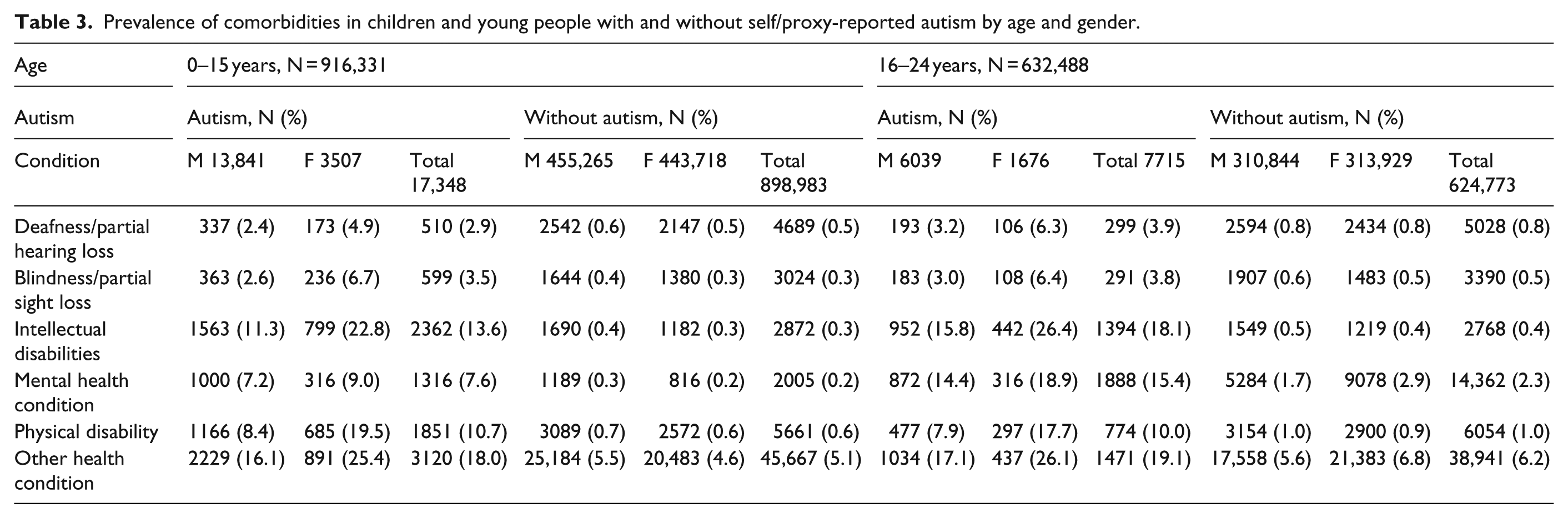
Table 4 shows the OR (with 95% CI) of autism predicting each of the six specific health conditions, having adjusted for age and gender: OR = 5.4 (5.1–5.6) for deafness/partial hearing loss, OR = 8.9 (8.1–9.7) for blindness/partial sight loss, OR = 49.7 (38.1–64.9) for intellectual disabilities, OR = 15.7 (13.4–18.5) for mental health conditions, OR = 15.8 (14.1–17.8) for physical disability and OR = 3.9 (3.8–4.0) for other conditions. As expected, each of the comorbidities were more likely to have been reported for young people aged 16–24 years rather than children (Table 4: ORs ranged from 1.2 to 7.6 for the six conditions). Mental health conditions were more common in females (OR = 1.5; 1.4–1.6).
The odds ratios of autism, age and gender in predicting each of six comorbid conditions in the whole population of children and young people.
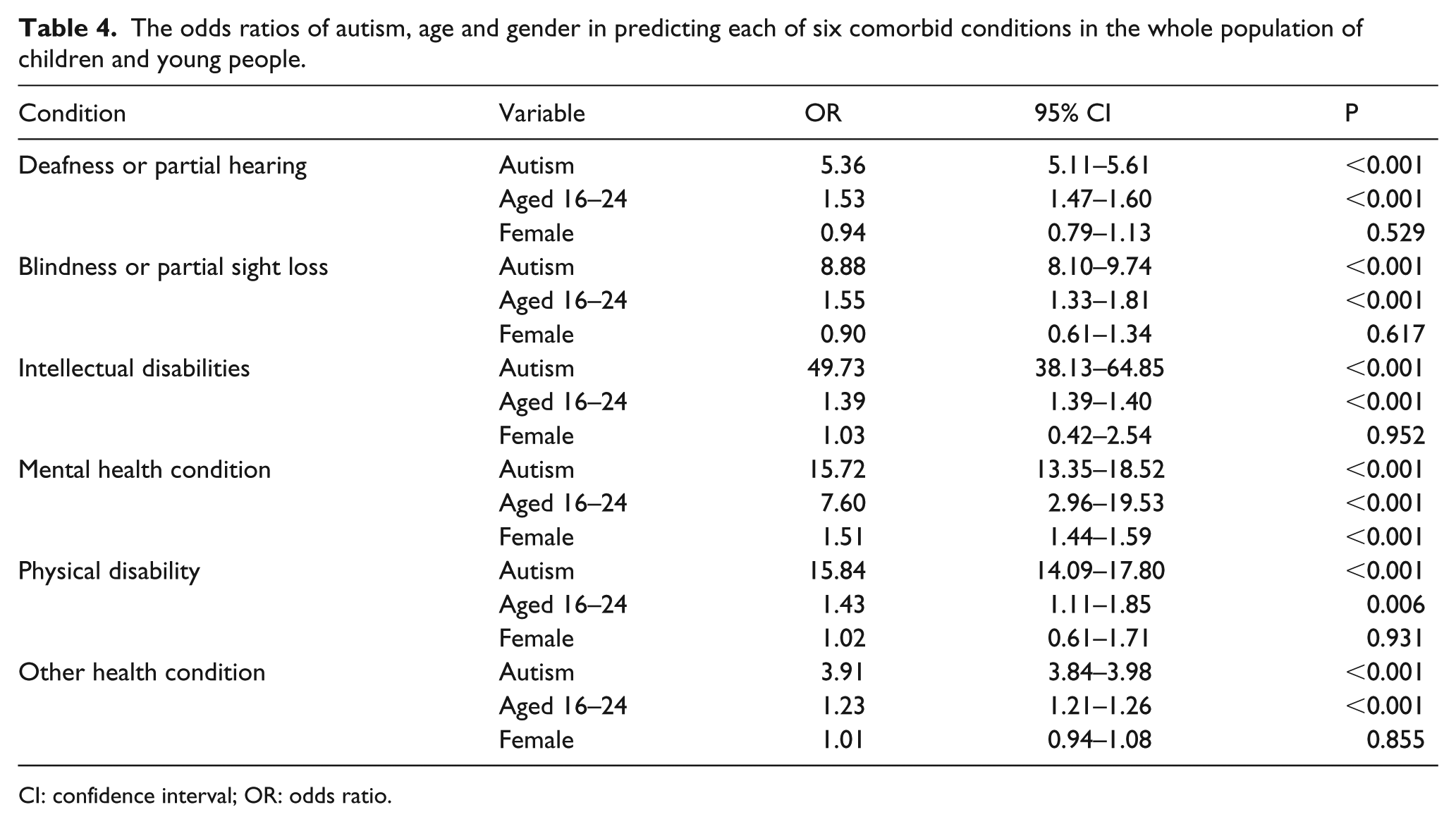
CI: confidence interval; OR: odds ratio.
Table 5 shows the OR (with 95% CI) of age and gender in predicting each of the comorbidities within the population of children and young people with autism. Unlike in the whole population, females with autism were more likely to report each of the comorbid conditions, including intellectual disabilities, than were males with autism.
The odds ratios of age and gender in predicting each of six comorbid conditions in children and young people with self/proxy-reported autism.
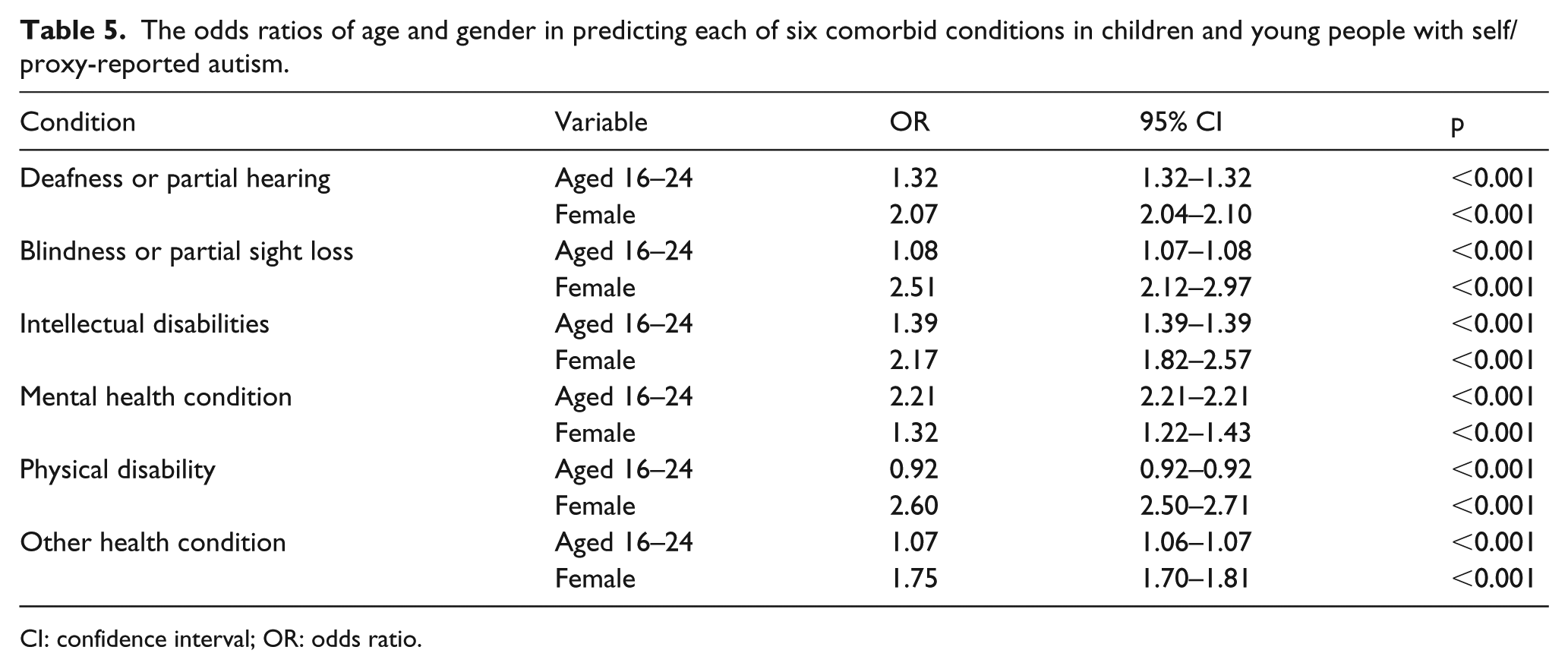
CI: confidence interval; OR: odds ratio.
Discussion
Each of the long-term conditions we investigated was substantially more common in the population with autism than in other people. We found deafness/partial hearing loss, blindness/partial sight loss and physical disability to be, respectively, 5, 9 and 16 times more prevalent in the children and young people with autism, i.e. strikingly more common. These conditions have been little studied in children and young people with autism previously, if at all with regards to physical disability. Each of these conditions are disabling and can significantly impact learning, functioning and long-term quality of life when they occur as single conditions; clearly their coexistence with autism adds extra complexity.
Our reported prevalence for deafness/partial hearing loss of 2.9% in 0–15 year olds and 3.9% in 16–24 year olds was higher than previously reported in all studies (Fombonne, 2003; Gravel et al., 2006; Jure et al., 1991; Tas et al., 2007; Tharpe et al., 2006; Van Naarden Braun et al., 2015) except one (Rosenhall et al., 1999). This latter study conducted detailed examinations, but was small in size. Our study supports the view that deafness is likely to be higher than previously recognised in children and young people with autism. Our findings for blindness/partial sight loss of 3.5% in 0–15 year olds and 3.8% in 16–24 year olds were higher than previously reported rates of 1.0% (Van Naarden Braun et al., 2015) and 1.3% (Fombonne, 2003). This also suggests that visual impairment is higher in children and young people with autism than previously recognised.
Physical disabilities, not previously reported in children and young people with autism are also very common, with 10.7% of 0–15 year olds and 10.0% of 16–24 year olds reported to have a physical disability. Clearly, further study is needed to better understand the types of physical disabilities that people with autism are experiencing, their reasons, impact on daily activities and approaches that might improve function.
While intellectual disabilities and mental health conditions have previously been reported to be more prevalent in children and young people with autism, the size of our study and the direct comparison with the general population provides credibility to the findings. While we found that intellectual disabilities were 50 times more prevalent in the children and young people with autism than in other children and young people, the actual prevalence was 13.6%–18.1% compared with 0.3%–0.4% in the other children/young people (more in young people than the children, as some intellectual disabilities are not confirmed until school age). This is much lower than previously reported, in view of the broadening out of criteria for autism spectrum condition in recent years. Interestingly, a recent large Swedish study focussed on familial co-aggregation of autism, and attention deficit hyperactivity disorder has reported a prevalence of autism of 1.5%; 1.2% without intellectual disabilities and 0.3% with intellectual disabilities, suggesting only 20% of the people with autism also had intellectual disabilities (Ghirardi et al., 2018).
We found mental health conditions to be 16 times more common in the children/young people with autism than in the general population. This finding is in keeping with other studies of higher rates of mental health conditions, having now extended such study to a much larger population.
We consider that practitioners need a heightened response to the possibilities of comorbidities, particularly of hearing and visual impairments and physical disabilities, given our conclusions that these were under-reported in previous studies. This might suggest a level of ‘diagnostic overshadowing’, although of course it is possible that in our study, there is a correlated detection whereby the children and young people with autism had more contact with healthcare and may thus have been more likely to receive an additional diagnosis.
While the majority of the autism population aged 0–24 was male (N=19,880; 79.3%), females with autism reported having more of each of the additional health conditions than did males, whereas this was only true for mental health conditions for the whole population. In particular, females with autism were more than twice as likely than males to have intellectual disabilities. This suggests that the females self/proxy-reported autism may actually have had more severe autism than the males, adding to the body of evidence reflecting the view that autism is currently underdiagnosed in more intellectually able females. Since autism is more prevalent in males, some clinicians may discount autism symptoms in girls and young people unless they present during the assessment of comorbidities, such as intellectual disabilities (Rubenstein et al., 2015).
The children and young people with autism were more likely to be of Caucasian ethnicity and to live in most deprived neighbourhoods. The extent to whether this impacts on their other characteristics warrants further study.
Strengths and limitations
This study investigates the whole population of children and young people in Scotland, and hence also is one of the biggest population sizes to date. The study is also strong in view that Scotland’s Census, 2011 had a very high level of coverage (94%) and enquired about comorbidities in all people living in Scotland, allowing direct comparisons between the children and young people with autism and the rest of the population. While the whole population coverage is a strength of the study, it used a broad-brush measure to identify conditions, based on the population self/proxy-reporting conditions. Limitations include the use of the term of ‘developmental disorders’ in the Census. However, it prompted responses only for the examples of autistic spectrum disorder or Asperger’s syndrome. Furthermore, the developmental disorders category was distinguished from intellectual disabilities, learning difficulties and mental health conditions, which are important distinctions. Hence, we consider that respondents will have replied accordingly, that is, responded regarding autism. However, we have no means to check this. While the term ‘mental health condition’ is imprecise; in Scotland, it is typically used to describe emotional disorders such as depression, anxiety and eating disorders. We consider it very unlikely to have been used for neurodevelopmental disorders, given the other categories provided for them in the Census. Respondents reported whether or not each person had autism and each of the long-term conditions, rather than each person receiving a clinical research assessment for these conditions. This lack of validation means that some reporting error is possible, and has not been quantified. We also do not know the extent to which proxy-reports would concur with self-reports. We report the numbers and proportion of children and young people living in communal establishments and private households but did not have access to their health needs by residential type. Imputation of zero by the Census team on the 2.6% with missing data on long-term conditions was not tested, though considered by the Census team to be the most plausible explanation. Despite these limitations, we believe that the results of this study are generalisable to other high-income countries, as well as filling a significant gap in existing research on the prevalence of long-term health conditions in children and young people with autism.
Implications
This study has provided information about the number and type of additional health conditions among children and young people with and without autism in a whole population. Clinicians, parents and teachers need an awareness of the higher risk of these conditions in children and young people with autism to improve identification in a timely fashion, so that the appropriate additional support for learning can be provided to reduce their impact and suitable health interventions can be sought and provided. It is also essential to have accurate information on the prevalence of comorbid health conditions in the population with autism in order to accurately plan for appropriate allocation and funding of resources, as well as implementing policies focussed on tackling health inequalities.
This is particularly so, given the changing prevalence rates of disorders in view of changes in practice in diagnosing autism. The higher rates of additional health conditions observed in children and young people with autism demonstrate a clear need to focus on improving understanding of provision of healthcare and the wider determinants of health in this population, which differ from the general population. People with autism may be at particularly high risk for poor health outcomes, which has been highlighted in relevant policies in the United Kingdom (National Institute for Health and Care Excellence (NICE), 2012; Scottish Government, 2008, 2011, 2013), but research in this area is still lacking, and reports from older studies are of lesser relevance due to diagnostic changes for autism spectrum disorders. Despite their young age, children and young people with autism experience considerably poorer health compared with the general population. More evidence is needed to determine relationships between specific health conditions and associated factors among children and young people with autism to help influence the development of appropriate interventions, public health strategy and health and social care policy.
Supplemental Material
AUT791279_Lay_Abstract – Supplemental material for Prevalence of sensory impairments, physical and intellectual disabilities, and mental health in children and young people with self/proxy-reported autism: Observational study of a whole country population
Supplemental material, AUT791279_Lay_Abstract for Prevalence of sensory impairments, physical and intellectual disabilities, and mental health in children and young people with self/proxy-reported autism: Observational study of a whole country population by Ewelina Rydzewska, Laura A Hughes-McCormack, Christopher Gillberg, Angela Henderson, Cecilia MacIntyre, Julie Rintoul and Sally-Ann Cooper in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by the Scottish Government via the Scottish Learning Disabilities Observatory.
Ethical approval
Permission to access data was granted by the National Records of Scotland, Scottish Government.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.