
Abstract
Results of randomized controlled trials have demonstrated significant reductions in anxiety symptoms following cognitive behavior therapy participation. Although promising, the extent to which previous research has included families from low socioeconomic status or racially/ethnically diverse backgrounds is unknown. Aims of this study are as follows: (1) What is the race, ethnicity, and educational attainment of youth with autism spectrum disorder and their families who have participated in research examining the efficacy of cognitive behavior therapy for anxiety? and (2) How do the demographics of these participants compare to that of the United States census? A total of 14 studies were reviewed that included 473 participants. Chi-square analyses indicated that there are significant differences between the race/ethnicity of youth with autism spectrum disorder participating in cognitive behavior therapy research for anxiety and that of youth in the United States. Standard residuals indicated significant overrepresentation of White youth and significant underrepresentation of Black and Latino youth in cognitive behavior therapy research (all p-values <0.001). Similarly, there were significant differences in the educational attainment of caregivers participating in cognitive behavior therapy research, with a significant underrepresentation of caregivers from low socioeconomic status backgrounds (p < 0.001). These findings have implications for the development of cognitive behavior therapy interventions for youth with autism spectrum disorder and anxiety that are both rigorous and inclusive.
Children and adolescents with autism spectrum disorder (ASD) are at high risk for developing co-occurring mental health conditions, and anxiety represents one of the most commonly co-occurring psychiatric conditions (Van Steensel et al., 2011). In response to this significant mental health need, researchers have adapted cognitive behavior therapy (CBT) for youth with ASD. Results of more than a dozen randomized controlled trials examining the impact of individual and group CBT have demonstrated significant reductions in anxiety symptoms following treatment participation (Weston et al., 2016).
Although this burgeoning area of research points to the importance of using CBT approaches for youth with ASD and anxiety, it does not guarantee that these services are accessible in community contexts. Issues related to accessing evidence-based practices (EBPs) are well documented in general pediatric mental health (Reiss, 2013) and are even more pronounced for youth from low socioeconomic status (SES) and racial/ethnic minority backgrounds. That is, low SES and underrepresented racial and ethnic minority (URM 1 ) youth and their families experience notable disparities in accessing a variety of mental health treatments (Reiss, 2013). These disparities are thought to be more significant for anxious youth (Gudiño et al., 2009), and are problematic, as untreated anxiety in childhood is associated with long-term negative outcomes (Essau et al., 2014).
Diagnostic and treatment disparities for children and teens with ASD parallel findings reported for typically developing youth with mental health disorders. That is, a number of research studies have demonstrated that youth from URM and low SES backgrounds are diagnosed with ASD at older ages (Durkin et al., 2017; Parikh et al., 2018) and access fewer services for their child with ASD (Pickard and Ingersoll, 2016; Zuckerman et al., 2017). The treatment disparities reported for URM youth with ASD are thought to be related to a variety of cultural and structural barriers (Burkett et al., 2015; Zuckerman et al., 2015, 2017). For example, URM families may be more likely to seek informal support from community members than from formal health care providers (Ratto et al., 2017). Other cultural factors known to influence access to ASD services include English language proficiency (Amant et al., 2018) and perceived stigma associated with ASD diagnoses and treatment (Zuckerman et al., 2018). Structural barriers also contribute to treatment disparities for low SES and URM youth with ASD. These barriers include limited access to transportation and childcare, as well as the time required to participate in ASD services (Pickard and Ingersoll, 2016).
URM and low SES youth with ASD and co-occurring anxiety may experience additional barriers that further impede access to treatment. Difficulty accurately identifying and assessing anxiety symptoms in youth with ASD has been broadly reported (Kerns et al., 2014). However, the challenges of assessing anxiety are likely increased in URM youth with ASD and anxiety due to differential presentation of anxiety in diverse youth (Kirmayer, 2001) and the potential bias toward identifying externalizing disorders in these youth (Chavira et al., 2004). Additional barriers for URM youth with ASD and anxiety may include stigma associated with seeking out services specific to mental health disorders (Ratto et al., 2017).
The underlying reasons that treatment disparities exist, both broadly and for youth with ASD and anxiety, are likely complex. However, one contributing factor may be that, in general, EBPs are designed and trialed in controlled research environments that may make it difficult to engage diverse families (Barrera et al., 2011; Huey and Polo, 2008). By not fully including low SES and URM youth and families throughout intervention development, it is difficult to know whether EBPs are efficacious for youth and families from low SES and URM backgrounds (Miranda et al., 2005). In addition, limited participation of low SES and URM families leads to missed opportunities to understand their perspectives related to treatment utilization and engagement. This “traditional” process of developing interventions in controlled research settings prior to moving them into the community is common in the development of ASD interventions (Stahmer et al., 2017). Although this process results in the development of rigorous EBPs, it is also thought to exacerbate treatment disparities (Dingfelder and Mandell, 2011).
Given the significant interference of anxiety for children and adolescents with ASD, it is crucial to understand whether CBT interventions for youth with ASD and anxiety have actively engaged low SES and URM families. Understanding the demographic background of study participants is pressing given the known treatment disparities for anxious low SES and URM youth in the general pediatric population and the long-term impact of these disparities.
This study
The primary purpose of this article is to characterize a sample of children and adolescents who have participated in the process of developing and trialing CBT for youth with ASD and anxiety. Specific objectives are as follows: (1) describe demographic variables, such as race, ethnicity, and caregiver education for youth with ASD and their families who have participated in clinical research examining the efficacy of CBT for anxiety and (2) compare the demographic background of these participants with those of the US population. We anticipate that URM and low SES youth with ASD and their families will not be represented in CBT research at rates consistent with the US Census.
Methods
Procedure
Article selection and review
Articles were selected using the search terms “autism spectrum disorder,” “cognitive behavior therapy,” and “anxiety” in Google Scholar, PsychInfo, ProQuest, and PubMed. Articles were included in the present review if they met the following criteria: (1) were conducted within the past 15 years (from 2003 to 2018), (2) CBT was used to target anxiety in children and adolescents with ASD, (3) at least one anxiety outcome measure was used, (4) demographic data of study participants was reported, and (5) the study sample was recruited from within the United States. There were no limitations on the basis of sample size. Based on these criteria, 19 studies were selected that included a total of 483 participants. However, of the 19 selected studies, 5 case studies did not report demographic data and were therefore excluded (see Figure 1). Thus, a total of 14 studies were reviewed that included a total of 473 participants (see Table 1). These articles were cross-referenced with recent meta-analyses that have examined the efficacy of CBT for youth with ASD and anxiety.

Study selection process.
Demographic information of participants by reviewed study.
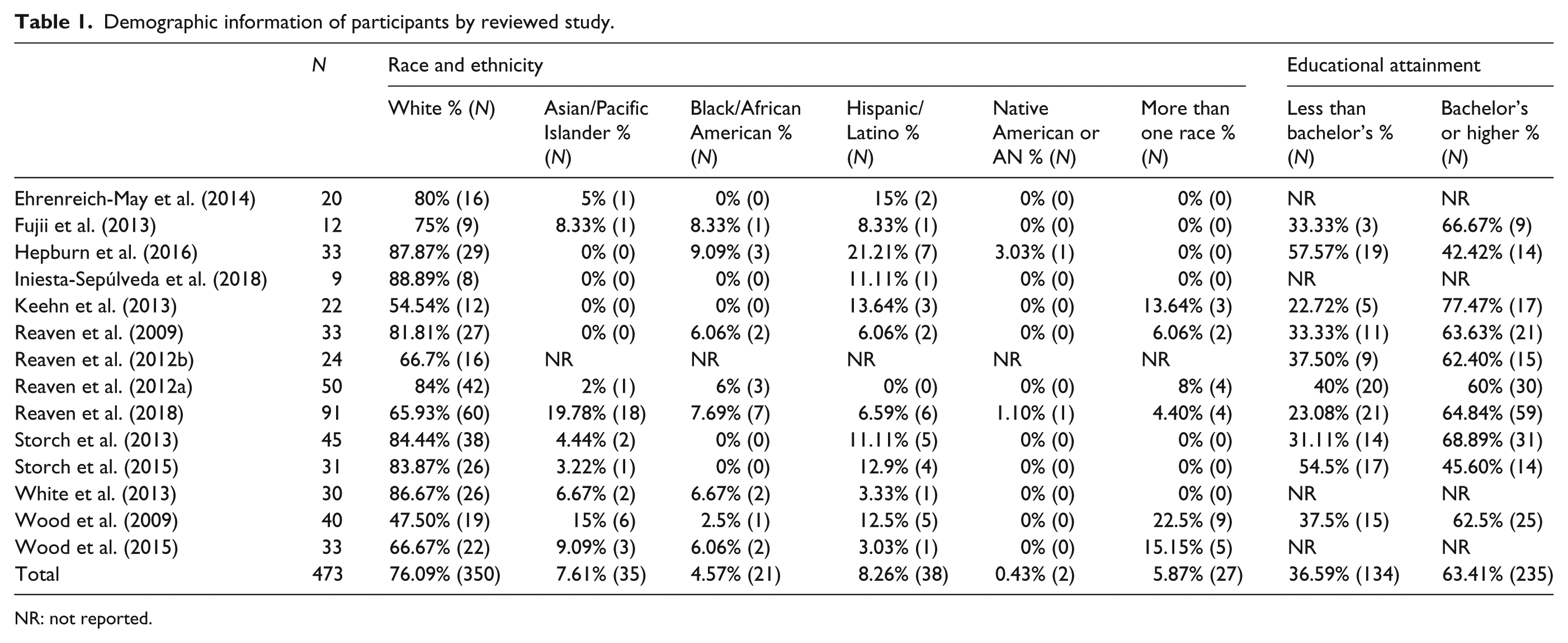
NR: not reported.
Demographics: aggregation and comparison
Demographic data from each study was categorized based on those used in the race, ethnicity, and caregiver education data from the 2012–2016 American Community Survey 5-year Estimates. Caregiver educational attainment was used as a proxy for SES. After categorizing the demographic data, the total number of participants was aggregated within each demographic category and divided by the total number of participants from whom race (N = 460) and caregiver education (N = 369) were reported. The race and ethnicity percentages were then compared to those reported in the 2012–2016 American Community Survey for youth under 18 years (United States Census Bureau, 2016a), while the educational attainment percentages were compared to educational attainment data from the same survey (United States Census Bureau, 2016b). The 2012–2016 American Community Survey was used as a comparison given that it reflected the demographic make-up of the US population during a time period when 11 of the 14 reviewed studies were published.
Inter-rater reliability
Demographic data was independently categorized by two of the authors (N.R. and K.P.) on the basis of pre-established categories from the US Census. Percent agreement (90.9%) was calculated based on this initial categorization. Consensus coding involving the senior author was used for disagreements. The majority of disagreements occurred when demographic data did not align with the categories used by the US Census. For example, maternal education was often reported in general terms or not reported at all. Therefore, in order to collapse maternal education across studies, we chose to present it as the percent of participating caregivers with a college degree or higher. Similarly, the majority of research studies combined their reporting of race and ethnicity such that participants were reported as either “White” or “Latino.” Therefore, the percentage of White youth included in research was compared to the US Census data for White and Non-Latino children.
Analytic plan
Chi-square analyses were used to compare percentages of the US population to the actual counts and percentages of youth and caregivers participating in CBT research. Chi-square goodness-of-fit analyses were completed for race/ethnicity data, as well as maternal education data. Youth and caregiver percentages were based on participants for whom demographic data was reported and could be mapped onto the United States Census categories. For example, participants listed as “unknown” or “other than White” were not included in the analysis. A significant chi-square in our analyses indicated that the two populations being compared were significantly different. Follow-up standard residuals using two-sided Fisher’s exact tests were used to calculate p-values for each demographic category.
Results
Table 2 compares aggregated demographic information from research participants to population-level demographic information drawn from the 2012–2016 American Community Survey. A total of 473 youth, ages 7–19 years, were included across the 14 reviewed studies. Across studies, the race/ethnicity was reported for 95.24% of participating youth (N = 460) and the educational attainment was reported for 76.40% of participating caregivers (N = 369).
Race, ethnicity, and educational attainment of youth and families participating in CBT research compared to US Census.
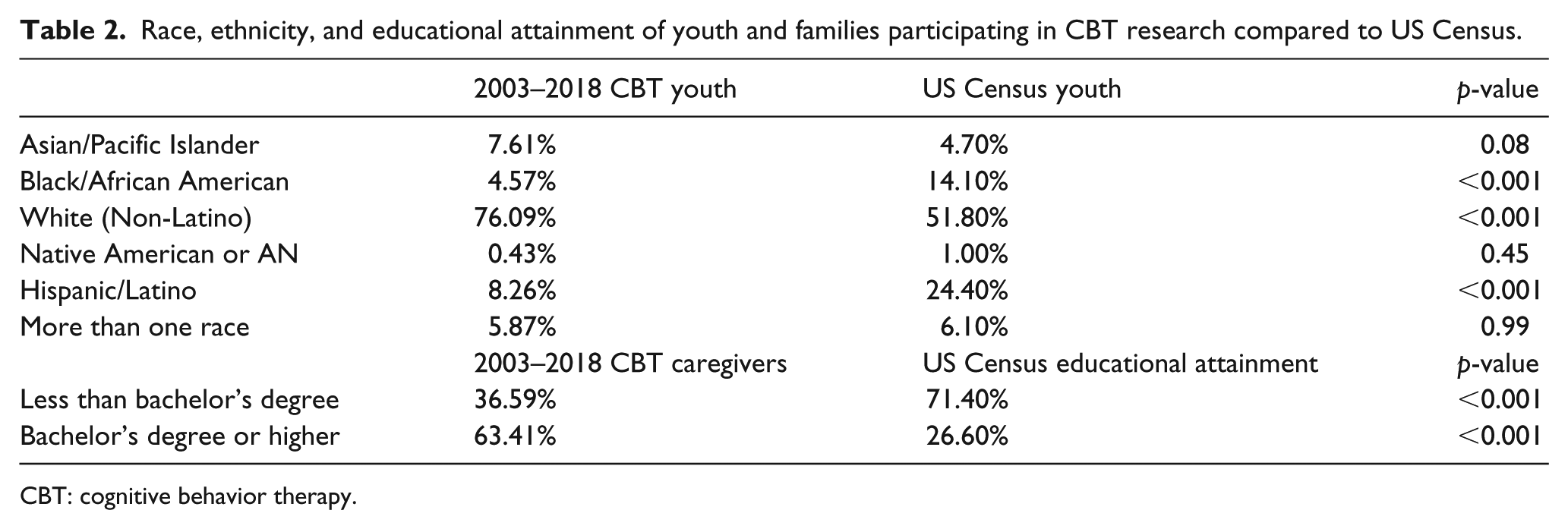
CBT: cognitive behavior therapy.
Overall, the demographic composition of youth and families who participated in clinical trials examining CBT for youth with ASD and anxiety is not reflective of the US population. With regard to race and ethnicity, significant differences were observed between that of youth participating in CBT research and youth in the US population χ2(5, N = 460) = 84.61, p < 0.001. Standard residuals using Fisher’s exact test indicated significant overrepresentation of White youth and significant underrepresentation of Black and Latino youth. There were also significant differences in the educational attainment of caregivers participating in CBT research, χ2(2, N = 369) = 80.99, p < 0.001. For example, only 28.60% of mothers in the US census have a Bachelor’s or graduate-level degree. However, mothers with a college education or above comprise a significant majority of those included in CBT research.
Discussion
The goals of this study were to understand the demographic composition of youth with ASD and their families who have participated in research examining the efficacy of CBT for anxiety and to compare the demographic information of participants to the US census. The 14 reviewed studies varied greatly in the level of detail with which they reported demographic information. The majority of the reviewed studies conflated race and ethnicity, and maternal education or other markers of SES were not reported for 20% of participants. In spite of these challenges, results indicated a significant overrepresentation of White youth and significant underrepresentation of Black and Latino youth in CBT research. Similarly, caregivers who participated in CBT research were significantly more educated than those represented in the US census.
Results of this study highlight that CBT interventions for youth with ASD and anxiety have been developed and trialed with youth and families who are not fully representative of the US population. This finding is consistent with research examining the efficacy of CBT in neurotypical adults, which has been shown to have an underrepresentation of racial and ethnic minority participants (Waheed et al., 2015). Although recent literature has also argued that it is critically important to determine whether rates of research participation vary by race, ethnicity, and SES for neurotypical anxious youth, this research has yet to be conducted (Huey and Polo, 2017). Taken together, the results from this study reflect a long-standing history of intervention development that has prioritized the development of rigorous, high-quality interventions at the expense of actively including low SES and URM families. The limited inclusion of diverse communities in the early stages of treatment development hinders the translation of these interventions to heterogeneous populations (Barrera et al., 2011) and is particularly problematic given the shifting demographics within the United States. It is estimated that racial and ethnic minority groups will make up more than 50% of the US population by 2050 (Passel and Cohen, 2008). Without proactive efforts to represent low SES and URM families in research, we are at risk to develop interventions that further exacerbate treatment disparities for a growing number of youth and families.
Developing interventions for youth with ASD and anxiety without diverse community engagement may be both inequitable and inefficient. Limited participation from diverse families is inequitable in that it inadvertently ignores the beliefs that these families might hold regarding mental health causes and ASD treatment, in addition to structural barriers and facilitators to treatment engagement, thus, perpetuating the presence of cultural/structural barriers. Inadvertently ignoring these perspectives may also lead to higher rates of attrition once CBT interventions are moved to community settings (Stahmer and Pellecchia, 2015). In addition to being inequitable, not adequately including low SES and URM families in intervention research is inefficient in that, once interventions are developed, additional research may be required to understand the applicability of the intervention to diverse community settings (Miranda et al., 2005).
Limitations
There are a few important limitations to consider for this study. First, it was difficult to aggregate demographic data given the conflation of race and ethnicity, and the limited report of maternal education. Accurately categorizing race and ethnicity while also capturing the growing diversity within each category has been a national topic of interest given the increasing number of racially diverse Latino families living in the United States (Gonzalez-Barrera and Lopez, 2015). In addition, we chose caregiver educational attainment as a marker of SES. Although educational attainment is used as a proxy for SES in health disparities research (Shavers, 2007), it does not reflect family income and size. Another limitation was that the 14 reviewed studies spanned a larger time frame than the US Census comparison. We chose to use the 2012–2016 American Community Survey given that 11 of the 14 reviewed studies were published within this time frame. Comparing the reviewed studies to Census data from an earlier time period did not change the study results. We did not compare studies on a state-by-state basis, which may have yielded somewhat different results.
Finally, this review included only studies from the United States. Although a number of other studies have examined the impact of CBT for youth with ASD and anxiety in other high-income countries (i.e. Australia, United Kingdom, Singapore), very few that we are aware of have been conducted in low- and middle-income countries. For example, an identical search in Spanish to find studies that examined CBT for youth with ASD and anxiety yielded only two case studies conducted in Spain and Ecuador (Garzón Jurado, 2015; Martínez-González and López Gil, 2017). This gap reflects a broader, international tendency to design interventions in areas of greater resource prior to moving them to geographical areas of need. Although there has been greater initiative for global research partnerships, it may be the case that these initiatives have primarily focused on the epidemiology of ASD or on translating early intervention internationally (Rahman et al., 2016). CBT for youth with ASD and anxiety is still a burgeoning area of research within the United States and, therefore, may lag behind other well-established and/or priority research areas.
Future directions
The results of this study suggest a number of next steps aimed at reducing mental health disparities for youth with ASD and anxiety. First, when conducting CBT research for youth with ASD and anxiety, it will be important to thoroughly document the race, ethnicity, and SES of participants, as well as those of the clinicians delivering treatment. In addition to improved reporting practices, it is essential to develop strategies to recruit and engage URM families in CBT research. In order to do so, CBT researchers will need to address the structural barriers to research participation, as well as cultural and attitudinal barriers. Strategies to address these barriers may include partnering with trusted family advocates to support recruitment efforts and reduce mental health stigma; recruiting within community settings such as primary care settings, churches, and schools; making recruitment materials available in other languages; and providing childcare and transportation supports when possible.
The need for proactive recruitment of low SES and URM families in CBT research highlights a broader need for increased use of research conducted within diverse community settings. Community-based research is not typically a defining feature of the “traditional” intervention development process (Wandersman, 2003), but it is one method to actively engage low SES and URM families in research, with the understanding that interventions can be strengthened if informed by community insight (Strand et al., 2003). Community-based models of research have been of increasing interest in the ASD field and are crucial in creating interventions that are both rigorous and culturally responsive (Stahmer et al., 2017).
The importance of developing interventions in partnership with communities and reducing barriers to research participation is without question. However, one challenge that ASD researchers are faced with is that many CBT interventions for youth with ASD and anxiety have already been developed in controlled research settings. Although it is not feasible to restart the intervention development process, it is of critical importance to retroactively understand the fit of these services in diverse settings. Utilizing known frameworks designed to assess the culturally sensitive elements of treatments may be helpful in this regard (Bernal et al., 1995).
Conclusion
Youth with ASD and their families who have participated in CBT research for anxiety are a primarily White and educated sample and are not reflective of the race, ethnicity, and SES of youth and families living in the United States. This finding is consistent with prior research documenting the tendency for EBPs to be designed and trialed without full representation of diverse families. Limited representation of low SES and URM youth and families during intervention development and efficacy trials limits the generalizability of the interventions, fosters treatment disparities, and is particularly problematic given the growing numbers of URM youth and families living in the United States. Increased use of recruitment and research conducted in partnership with diverse communities is essential to engage low SES and URM families in CBT research.
Supplemental Material
AUT795678_Lay_Abstract – Supplemental material for Examining the inclusion of diverse participants in cognitive behavior therapy research for youth with autism spectrum disorder and anxiety
Supplemental material, AUT795678_Lay_Abstract for Examining the inclusion of diverse participants in cognitive behavior therapy research for youth with autism spectrum disorder and anxiety by Katherine Pickard, Nuri Reyes and Judy Reaven in Autism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.