
Abstract
Although the number of Syrians affected by the civil war rises, little work has been done to address the needs of Syrian refugee children with autism spectrum disorder. This research aimed to test the feasibility and acceptability of a culturally sensitive intervention developed specifically for children with autism spectrum disorder affected by trauma. Local partners advised the program team on cultural norms. Nine parents and 11 teachers were recruited to participate in 12-week parent–teacher cooperatives in a large Turkish city. We used qualitative methods to analyze interviews with each participant after intervention completion. A total of 14 participants completed the program (70%). All interviewees were women and Syrian refugees. Local political events, transportation costs and safety, and illnesses impacted attrition and attendance. All participants were satisfied with program content, including gains in autism knowledge, behavior management skills, and social support. Program-related challenges included applying skills to nonverbal children. The majority of participants made recommendations for program improvement, including a need for services outside urban areas. Flexible program delivery methods, including online options, might better accommodate participants unable to travel due to distance, political unrest, or safety. More research is needed to rigorously test program outcomes and to evaluate efforts to train local program leaders.
Challenges related to raising a child with autism spectrum disorder (ASD) have significant impacts on parents and other caregivers, including elevated stress, more depressive symptoms, and lower levels of well-being, compared to those raising children without ASD (Estes et al., 2009; Phetrasuwan and Shandor Miles, 2009; Schieve et al., 2007). Some major sources of stress experienced by parents with children with ASD are challenging child behaviors, limited information about ASD, poor access to services, transportation, and financial burden (Tehee et al., 2009). ASD and related family functioning in non-Western countries, such as those in the Middle East, have been relatively overlooked in the academic literature. Yet, ASD is vastly heterogeneous (Habayeb et al., 2017) and the clinical presentation and identification of the disorder are influenced by cultural and socioeconomic factors (El-Ghoroury and Krackow, 2012; Elsabbagh et al., 2012; Mandell et al., 2002; Mandell and Novak, 2005).
Documented rates of ASD in the Middle East are lower than those found in Western countries, potentially due to decreased awareness (Elsabbagh et al., 2012) and some Middle Eastern families remaining secretive about having a child with a disability (Dardas and Ahmad, 2014). Thus, it is likely that rates of identified cases of ASD are underestimates of the true prevalence of the disorder. Like their Western counterparts, Middle Eastern parents of children with ASD and other disabilities experience greater levels of stress, depression, and anxiety compared to parents raising typically developing children (Al-Farsi et al., 2016; Almansour et al., 2013). Poor service availability and access, as well as limited education about ASD, have also been cited as significant stressors to families of children with ASD in the Middle East (Dababnah and Bulson, 2015; Rayan and Ahmad, 2017). Some research has suggested maternal caregiving burden in Arab communities is higher than for fathers, due to cultural parenting norms (Fido and Saad, 2013). Middle Eastern parents, particularly mothers, have reported experiencing blame, shame, and guilt for bearing a child with ASD (Dababnah and Parish, 2013; Fido and Saad, 2013). In the Middle Eastern cultural context, stigma against individuals with ASD is often experienced by the entire family, for example, resulting in diminished marriage prospects for siblings (Dababnah and Parish, 2013; Dardas and Ahmad, 2014). Stigma places parents at risk for low subjective well-being (Werner and Shulman, 2013) and poor parental self-efficacy (Rosenblum-Fishman, 2013), further exacerbating family burden.
The emerging ASD research in the Middle East primarily comes from wealthy and relatively politically stable countries, including Oman, the United Arab Emirates (Salhia et al., 2014), and Saudi Arabia (Al-Salehi et al., 2009). However, a substantial portion of the region is facing protracted humanitarian emergencies resulting from political unrest, including the refugee crisis stemming from the ongoing Syrian civil war (World Health Organization, 2017). Between the beginning of the war in 2011 through 2015, 7.6 million people were internally displaced from their homes, while another 3.7 million fled the country, mainly into neighboring countries including Lebanon, Jordan, Iraq, and Turkey (Ostrand, 2015). In 2016, Turkey accepted almost 3 million refugees and asylum seekers, of whom 2.7 million were Syrian and 125,000 were Iraqi (UNHCR, 2016). Services and research focused on non-refugee children with ASD in Turkey are scarce (Rakap et al., 2016), while services and research regarding children with ASD and their families in Syria and other regions hosting large refugee populations are nearly nonexistent.
While not ASD-specific, a large body of research exists on the effect of refugeeism on child development and families in general. In their home countries, children may be exposed to a range of traumatic experiences (Mollica et al., 1987), which can significantly affect social, emotional, and behavioral outcomes (Trickey et al., 2012). The journey to safety following war and conflict often exposes children to additional violence and abuse (Bemak and Chung, 2014). Once resettled in a host country, refugees often face acculturative stress, including language barriers (Bemak and Chung, 2014) and experiences of racism and xenophobia (Montgomery, 2008). Finally, refugee family dynamics can change as a result of acculturation and resettlement, due to separation; altered roles, and child-rearing strategies; unemployment and poor financial support; and parent mental health issues (Bemak and Chung, 2014; Fazel and Stein, 2002; Reed et al., 2012; Tol et al., 2013). Recent research on Syrian refugees has documented high rates of mental health disorders, especially major depressive disorder, with rates increasing when needing to stop and live elsewhere on the journey to safety (Tekeli-Yesil et al., 2018).
Children with disabilities are among the most vulnerable individuals in war settings (HelpAge International and Handicap International, 2014), and those with preexisting mental health issues are more negatively impacted by war and forced migration than those without these preexisting issues (Fazel and Stein, 2002; Murthy and Lakshminarayana, 2006). A study of Somali refugee families raising children with ASD in the United States reported mothers were not familiar with ASD, had difficulties communicating with healthcare professionals, and attributed ASD etiology to non-biological factors such as processed foods and vaccinations (Miller-Gairy and Mofya, 2015). Other unique challenges might face refugee children with ASD. For example, schools and appropriate interventions are abruptly halted when families are forced to flee from war; transitions which can be particularly challenging for individuals with ASD (Battle, 2015; Jabri, 2015). Furthermore, fear caused by conflict can exacerbate many of the challenging behaviors children with ASD can exhibit, resulting in amplified social withdrawal, intense repetitive behaviors, and aggression (Battle, 2015).
Given family functioning post-trauma is associated with child mental health outcomes (Trickey et al., 2012), interventions in other fields have been successfully adapted to incorporate families (Chung and Bemak, 2012). In non-refugee-specific ASD interventions, inclusion of parents is increasingly recognized as beneficial (Matson et al., 2012). Parent-implemented ASD interventions, including behavioral approaches such as applied behavior analysis, can improve children’s challenging behaviors, boost parent–child interactions, reduce parent stress, and increase knowledge of ASD (McConachie and Diggle, 2007; McConachie et al., 2005; Oono et al., 2013). Other researchers have highlighted the need to train teachers in empirically supported ASD practices, especially those teachers who are working to integrate children with ASD into inclusive classrooms (Leblanc et al., 2009). Finally, interventions which include general information about ASD may be particularly needed in low-resources areas (Schultz et al., 2011). For these reasons, a parent–teacher program that incorporates psychoeducation and behavior management skills building components has promise for refugee children with ASD.
This study
In light of the lack of research focused on Middle Eastern children with ASD and their families in general, and refugee children in particular, this article describes a culturally sensitive, community-based intervention developed specifically for children and their families affected by trauma. Parent–teacher cooperatives (PTCs) have been implemented in other Arab and Muslim communities in the Middle East and United States; yet, they have not been described in the academic literature. Thus, this study aimed to explore the feasibility and acceptability of PTCs for Syrian refugee parents and teachers of children with ASD in a large Turkish city.
Method
PTCs were developed by A Global Voice for Autism, a non-profit organization with the mission to support children with ASD in conflict-affected communities. In partnership with local agencies serving children with special needs, this organization works with a team of board-certified behavior analysts (BCBAs), board-certified assistant behavior analysts (BCaBAs), other ASD service professionals, trauma specialists, and community liaisons to deliver parent and teacher training programs, parent and sibling support groups, and community education sessions. The BCBAs and BCaBAs are from the United Kingdom, the United States, and Saudi Arabia and are internationally certified by the Behavior Analyst Certification Board. For this study, A Global Voice for Autism collaborated with the researchers at the University of Maryland, Baltimore to examine the feasibility and acceptability of their PTCs in a specific refugee community in Turkey. Given the data provided by A Global Voice for Autism to the research team were deidentified, the Institutional Review Board at the University of Maryland, Baltimore determined the protocol did not require review.
Intervention
See Table 1 for a brief description of each week’s topic. In the 12-week PTCs, BCBAs teach parents and teacher skills in promoting communication, social interaction, and adaptive behavior skills within a child’s natural environment. Each session module is manualized and available through A Global Voice for Autism. Program modules were developed based on the recommended list of evidence-based practices for children with ASD by the National Professional Developmental Center on Autism Spectrum Disorder at the University of North Carolina at Chapel Hill (http://autismpdc.fpg.unc.edu/evidence-based-practices), with a particular focus on applied behavior analysis teaching strategies.
Weekly topics (22 sessions).
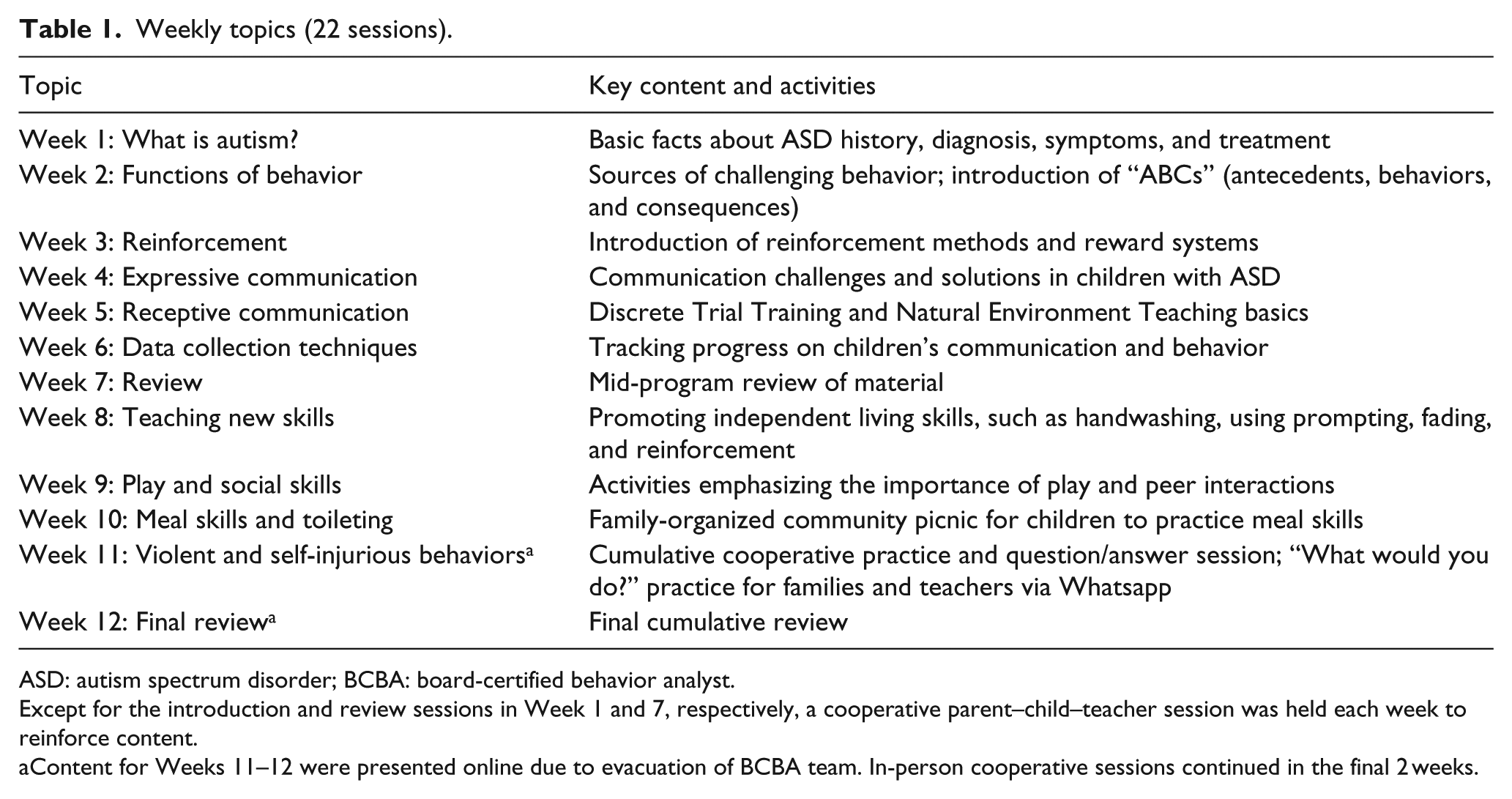
ASD: autism spectrum disorder; BCBA: board-certified behavior analyst.
Except for the introduction and review sessions in Week 1 and 7, respectively, a cooperative parent–child–teacher session was held each week to reinforce content.
Content for Weeks 11–12 were presented online due to evacuation of BCBA team. In-person cooperative sessions continued in the final 2 weeks.
The program was designed for conflict-affected communities and is thus guided by six principles outlined by the National Center for Trauma-Informed Care: safety; trustworthiness and transparency; peer support; collaboration and mutuality; empowerment (voice and choice); and cultural, historical, and gender issues (Substance Abuse and Mental Health Services Administration, 2014). Program team members work with local partners at each site to identify community needs and offer cultural insights before beginning the program. Local partners review program modules for cultural compatibility, in terms of both program content and social images. For example, local partners advised the “meal skills” module be slightly adapted to table norms in the Syrian community in Turkey. Due to financial constraints on families and schools, local partners also advised the program team to ensure that none of the modules were dependent on high-cost materials such as electronic tablets. Once the program began, program team members worked closely with each participant throughout the program to confirm the program materials were culturally relevant and not an additional financial burden to their family. Finally, the program was delivered in a group format in order to promote peer support, transparency, and a dedicated, confidential space to discuss participants’ experiences.
The PTCs focus on the application of skills at home, in the community, and in the classroom. In this study, if a child had two primary caregivers (e.g. mother and father), both were invited to attend. Parents and teachers engaged in 60 h of training per participant (total of 5 h over two sessions per week), in which 3.5 h (42 h total) involved lectures, videos, group discussions, and parent/teacher modeling activities. In the remaining 90 min per week, parents and teachers met in cooperative sessions to practice the week’s skills with their children and students. There were no cooperative sessions in Weeks 1 and 7. We note the program is lengthier than some parent training programs (e.g. the EarlyBird and the Incredible Years programs for caregivers of children with ASD are each about 30 h long). However, the program team determined more time should be allotted for Arabic-English interpretation between the BCBAs and participants. The team also recognized that, as is often the case in resource-poor areas, the target population most likely had limited prior or concurrent access to other ASD interventions. Thus, consistent with past PTC participant requests for longer sessions to learn and practice skills, the program team incorporated more time for the psychoeducational and cooperative sessions in particular.
As noted above, A Global Voice for Autism specifically developed the program for Arab and Muslim communities, where ASD is often highly stigmatized. For this reason, the program includes several components to address stigma directly. First, the program team delivered bimonthly community lectures to increase local awareness of ASD. Second, in addition to the psychoeducational and practice training components described above, parents and siblings participated in 18 h of supplemental programming during the 12-week period. This programming included creating a confidential space for parents and siblings to share their experiences, as well as confidence-building and creative-thinking activities to strengthen families’ understanding of ASD. Finally, the team offered families community outings to coach parents through the experiences of taking their children with ASD out in public.
Local partners assisted the program team not only in reviewing modules for cultural relevance but also building community buy-in for program sustainability. Furthermore, the program team offered 12 months of virtual follow-up support and training to PTC graduates, where each participant was matched with a BCBA. These follow-up sessions had two aims. First, the video exchanges allowed the program team to maintain communication and provide ongoing feedback to participants. Second, the sessions aimed to empower parents and teachers to advocate for ASD services and supports in their broader community. As an extension of the second aim, the follow-up program offered the program team opportunities to engage motivated parents and teachers as trainers in future programs. While this study only reports on findings from the in-person, 12-week portion of the program, we will explore the role of the 12-month “train the trainer” and follow-up support program in future studies.
Sample recruitment
Recruitment was coordinated through a local community-based agency targeting the Syrian community in a large city in southern Turkey. Participants were recruited through this agency, as well as through other local agencies and schools predominantly serving the Syrian refugee community. All recruitment materials were in Arabic. Participation was limited to teachers and primary caregivers of children with ASD. There was no age limit. All program sessions except for one were held at the agency coordinating recruitment.
Measures
Staff collected participant attendance at each session. Participants also completed a demographic information form before beginning the program. In addition, one of the program team’s BCBAs and one Arabic-speaking BCaBA conducted a semi-structured interview with each PTC graduate at the end of the program. With participants’ signed permission, the interviews were audio-recorded. Those participants who declined audio-recording were offered the alternative of the interviewer taking detailed notes during the interview. All participants in this study consented to audio-recording, except for one teacher who requested and received the alternative. The interviewers asked each participant 10 open-ended questions about their positive and negative experiences in the program, including any barriers to intervention engagement and completion. Interviewers also questioned participants about the role of the program in promoting their children’s social communication skills and addressing challenging behaviors. Each interview lasted approximately 30 min. A professional translated the interview data from Arabic to English. A Global Voice for Autism team member removed identifying information before sharing secure files via Accellion with researchers at the University of Maryland, Baltimore.
Data analyses
The research team at the University of Maryland, Baltimore managed and analyzed participant attendance and demographic data using descriptive statistics in SPSS (IBM Corp, 2017). We then analyzed the qualitative data using the constant comparative method in NVivo 11 (QSR International, 2015; Strauss and Corbin, 1990). Before beginning the coding process, the first and third authors each read the interview transcripts twice, maintaining memos of key ideas and potential relationships. Subsequently, we collaboratively developed an initial codebook, based on our preliminary readings and memos. Then, each researcher independently open coded relevant segments of the transcripts, adding to the initial codebook when new information emerged. When new codes were added, we reviewed previously coded transcripts to ensure the coding was consistent. After completion of the open coding process, the first author examined both sets of codes for any discrepancies and finalized the codebook after discussion with the third author. The final codebook was used to review all transcripts again to check segments were accurately coded, after which the first author used an axial coding process to identify relationships between codes, as well as emerging themes by subgroups (e.g. teachers vs parents). The first author discussed the final set of themes with the second author and the program team in Turkey, as an additional check on the data analysis findings.
Results
Nine parents and 11 teachers of children with ASD enrolled in the program. Four parents discontinued the program for reasons including the birth of a child, a prolonged child illness, transportation costs and safety, and moving away. One of the parents who left the program was an Iraqi refugee; the remainder were Syrian refugees. One teacher left the program due to being unable to reenter Turkey after she traveled to Syria; and, the other due to a personal illness. Thus, five of the parents (56%) and nine of the teachers (82%) who began the program graduated.
See Table 2 for a summary of participants’ characteristics. All program graduates, including the teachers, were Syrian refugees. Nearly all participants were women, with the exception of one mother–father dyad, and only mothers participated in the final interviews. The majority of the children with ASD were male (60%), and their ages ranged from 2 to 9 years at the beginning of the program (mean = 6.3 years). Parents reported having an average of 2.2 other children without ASD, whose ages ranged from newborn to 13 years old.
Sample characteristics.

SD: standard deviation.
Two significant events occurred during the study period that impacted program implementation. In June 2016, following a wave of previous attacks throughout Turkey that year, a terrorist attack at Istanbul’s main airport killed over 40 people. Then, in July 2016, the Turkish military attempted to stage a government coup, which resulted in part in increased animosity toward the Syrian refugee community. Program participants reported some Syrians were taunted in the streets, and their property destroyed, events verified in the news media (Hansen, 2016). As a result, the participants reported they felt unsafe speaking Arabic in public, or going into the community alone or with their children. Furthermore, while the first 10 weeks of the program were completed in-person, the remaining 2 weeks took place in a virtual classroom, given the core program team was forced to evacuate the country.
Attendance
Among those participants who graduated from the program, parents attended an average of 17.2 and teachers an average of 18.2 of the 22 program sessions (see Table 3 for details). The most common reason for parent absences from weekly sessions were child illnesses. Other reasons included a death in the family, housing-related stressors, domestic disputes, houseguests, and pregnancy-associated illnesses. The teachers’ absences were related primarily to mandatory work training programs. Two teachers also missed sessions due to family or childcare issues.
Average session attendance.

SD: standard deviation.
Interviews
Five mothers and eight teachers participated in an interview after completing the final in-person session in Week 10. (One teacher was unable to participate in the interview due to a family emergency.) Their comments fell into three broad categories: program benefits, challenges, and recommendations. We summarize these themes below.
Program benefits
All participating parents and teachers felt the program was appropriate for the needs of children with ASD. Furthermore, all participants felt they had gained knowledge about ASD itself, as one mother explained, “First, I did not know [ASD] was for life, or that my son is smarter than his siblings in many things, but his behaviors are different.” A teacher said: The most important thing we learned is that we cannot change a child with autism for sure. He will not change, but his behavior will, so we can make him gain skills that will allow him to be active in society.
Another mother said the program helped her to sort out information she had received elsewhere, saying: How long have I known about this situation? A year almost. I read a lot about the disorder. I read books, and communicated with many people, but honestly I benefited the most from [this program] … I used to have very confused information: you take a bit from a person who says this, you listen to people, and to YouTube. I used to hear a lot of contradictory information. But [in this program], I feel I am receiving the appropriate answer.
Participants claimed numerous other program benefits. The most common benefit identified by participants was the acquisition of new skills gained to help children with ASD. Several parents and teachers specifically noted reinforcing positive behaviors was a beneficial skill, as one teacher explained: The reinforcement method had a big impact on the students. For example, when we used to talk to them and ask them to do something, whether they did it or not, it was the same for us. However, when we started reinforcing them, we found that there was a difference in the sessions with several children.
One mother said that her child’s destructive behavior decreased because the mother “stopped reinforcing these behaviors and has made it clear that [child] can only get what she wants if she asks, waits and honors [my] requests.”
Participants also endorsed other skills gained from the program, including prompting positive child behaviors and use of the “ABC” strategy (i.e. identifying the antecedent “A” and consequence “C” of a behavior “B”). Some participants said they enjoyed learning how to encourage children to gesture, as one parent said: [My son] hasn’t learned it fully … but what matters to me most is that as a start he now knows how … What bothered me the most was that he communicated with me only by screaming. But now, he has something else to use other than screaming. Not always, but as a start …
Other parents learned ways with which to deal with challenging behaviors such as hyperactivity, as one parent who began teaching her son with games instead of requiring him to sit. Another parent was pleased with her child’s improvement in social skills, saying her child “no longer takes things that he wants from his peers, and has developed skills to play with peers who approach him.” Finally, some teachers recognized the skills they gained could also be applied to typically developing children, including the teachers’ other students and own children.
Citing their new skills, all of the mothers reported increased confidence in managing challenging child behaviors in the community, such as running into traffic, refusing to stay beside the parent, and throwing objects. One parent was pleased that her comfort interacting with her local community members in Turkey improved, as she realized, “I do not feel embarrassed from my daughter or her behavior anymore … I tell [the community members] that she has [ASD] … I find [community members] smiling, meaning there is no problem if she does anything.”
In addition to new skills gained, participants felt the program had other benefits, including a positive impact on their families and themselves. Some parents discussed meaningful improvements in family relationships related to the program, including with in-laws, siblings, and spouses. For example, one mother described the changes in her husband: My husband at first … was trying to evade the notion that, “There’s something wrong with my son,” especially because my son is young … But, frankly when [the program] came along … he started to feel, “As a father, I need to work at it. I also need to help my son.” So truly, he started sitting with me, taking the training material, reading, and asking me about anything he did not understand. For example, when I deal with [my son] in a specific way, he used to blame me before and say “No, why like this?” Now he asks me, “What should I do?”
Furthermore, both parents and teachers explained how the program has benefited them directly, including decreased stress and higher self-confidence. One mother said, “I learned that I have hidden strength. I felt I was weak having this child. I felt stressed. But no, now I feel I have strength.”
Finally, may parents and teachers felt the social support gained from the program was critical, particularly given that many felt isolated prior to the program, with one mother saying, “I enjoyed that everyone who has a child feels the same way I feel, and teachers understand it, too. I am not shy anymore that I am only person who has a child with a difficult condition.” The relationships the participants established often were compared to familial bonds, as one teacher described: We felt we were one family. We felt that the child we were dealing with … from the bottom of my heart I felt as if the child were my own son or daughter. There was a lot of affection and familiarity among us, and the nicest thing was that there was honesty and no artificiality at all.
Several participants mentioned maintaining these social relationships outside of the program, through social media and group outings.
Program challenges
Most participating parents reported having some difficulties in the program. Some mothers reported it was a challenge to ignore negative or attention-seeking behaviors, while only reinforcing positive behaviors, as one explained: [My daughter] needed a little more patience. She started to cry more, especially at bedtime when I did not want to do everything she asks for. For example, I tried to distract her or give her something else to reach the goal I wanted from her. I struggled a bit.
Some mothers also mentioned their child’s inability to focus for long periods as a barrier to properly practicing program skills at home. Parents added they had difficulties reaching the agency where the program was held, particularly as the program meetings were lengthy and partly overlapped with the Islamic holy month of Ramadan. One mother explained: My house is far away … I wasted time, an hour before going in and an hour coming back, [then] two or three hours [in the program]. My whole time was spent on the journey, and it was agony. I neglected my house very much … I would come exhausted, especially during Ramadan. I would reach home tired, barely able to make food … and I am responsible for a house and my children and husband. If I could not attend, it was because of that, I swear.
Many teachers also identified some challenges with the program, all related to application of skills. Some teachers found working with more than one child with ASD at a time difficult, although these teachers also noted they felt more confident by the end of the program. Other participating teachers described the challenge of teaching children with few preexisting communication skills, as one explained: There were children with no capacity to talk, and several children who did not have the ability to respond. So, it was very difficult, even while we were prompting them. They do not … play … It was very difficult for them to interact.
Finally, one teacher noted that collecting data on a child’s behaviors “needs time, high concentration, a lot of precision,” which some teachers felt was difficult when intensely learning new content and working with a child.
Program recommendations
All participants said they would recommend the program to others, including those teachers working with typically developing children. Teachers specifically discussed the prevalence of psychological trauma among children in their schools, as one noted: I recommend [the program] to all parents, whether their children are healthy or suffer from a minor problem, because it might benefit all [children] … There are children who are not in a normal psychological state. This program might help a lot.
Most participants had suggestions to improve the program, while some parents said they would not change the program at all. Many teachers and parents requested more information and follow-up for program graduates and expressed relief that they could have access to a year of virtual follow-up sessions. Some participants also requested additional training sessions, as well as more video and print content, particularly for families in non-urban areas. Regarding the training sessions themselves, participants would have liked longer meeting periods; more application and reinforcement of content from lectures within the cooperative groups; and additional information and skills focused on working with young and/or traumatized children, or those who have limited existing skills. Finally, some participants felt program staff should identify more ways to encourage program attendance and retention.
In the future, several parents emphasized the need to open more centers or meeting locations for families to participate in the program. Teachers also stressed this point, with one noting the need for more school resources: We hope and we aspire to have … a room specialized for providing support for children with autism, meaning to have specialists. Even if we can contribute to that since we now have … training and some skills acquired during the training … Unfortunately, we do not have any rooms, nor training, nor program that cares for children with autism.
Participants discussed the importance of expanding the program to more families and teachers, both because there is a need in the community, and for teachers to gain more experience working with children with ASD. Accordingly, several parents and teachers recommended increased program advertising, including through brochures, public meetings, and past participant word-of-mouth referrals. One teacher also noted financial support is needed to support families and ASD programs. Finally, some participants felt the program should have an even greater role in increasing local community awareness of ASD. A mother asserted, “I would like [the program] to assist in creating understanding in the community so that it changes. In our surrounding community, no one knows what autism means … I wish that society becomes aware of this disorder.”
Discussion
This article examined the acceptability and feasibility of PTCs in a large Turkish city, which aimed to provide skills to parents and teachers to help meet the needs of children with ASD. To our knowledge, this study is the first to examine services for Syrian refugee children with ASD in the academic literature. Furthermore, it adds to the limited bodies of knowledge on both Middle Eastern and refugee families of children with ASD, respectively.
The program was generally acceptable to participants. All participants reported gaining knowledge and learning new skills to manage child behavior from the PTCs, which past research has cited as methods to improve parent stress (Tehee et al., 2009). The parents also identified benefits such as increased confidence in managing child behavior and taking children into community settings. The latter benefit of including children with ASD in community activities is particularly notable, given previous research has found this is difficult for some Middle Eastern parents due to perceived stigma (Dababnah and Parish, 2013; Dardas and Ahmad, 2014). The participating mothers’ reports of improved family relationships and decreased isolation are also important to consider within the context of previous research. Such research has found that shame, guilt, and social isolation related to raising a child with ASD particularly impact Middle Eastern mothers negatively (Dababnah and Parish, 2013). Furthermore, the cooperative parent–teacher–child sessions seemed to serve not only an instructional purpose, but also to build social support between participants. While parents’ need for social support related to ASD has been extensively documented (Boyd, 2002), the benefits for teachers are less well understood. In this study, the teachers themselves were Syrian refugees and thus also at risk for social isolation and other stressors. Future research should continue to explore the potential benefits of creating collaborative parent–teacher partnerships to address child behavior and build support.
Participants also outlined some challenges specific to the PTCs, such as parents’ reported difficulties ignoring challenging child behavior and engaging children with short attention spans. The teachers likewise struggled with using intervention skills with some children with limited communication abilities, or with more than one child with ASD at a time. While these are common challenges experienced by both parents and teachers working with children with ASD across settings (Tehee et al., 2009), future researchers will need to collect more data on participants’ use of the skills in order to better assist them in using these strategies. Furthermore, follow-up support for PTC graduates to continue to receive advice on the use of the skills is likely a vital program component, although this hypothesis will need to be tested in subsequent studies.
The study revealed some of the logistical challenges delivering services to Syrian refugee parents of children with ASD in Turkey, which could impact the feasibility of scaling up the intervention. While Turkey is relatively stable compared to Syria, the attempted government coup and terrorist attacks that occurred during the program period highlighted the uncertainty these families continue to face. These events impacted participants’ feelings of personal safety and comfort in their communities and on public transportation. The security of the non-Turkish program team was also in question, which led to shifting the final 2 weeks of the program to an online format. Furthermore, 40% of the participants who began the program did not finish. The reasons for their discontinuation included unsafe and/or costly transportation to reach the service agency, family emergencies, and trouble reentering Turkey. Those who graduated from the program had fairly high attendance (78% and 83% attendance in sessions for parents and teachers, respectively), yet, their reasons for missed sessions were also primarily family-, housing-, and work-related.
Together, these challenges and barriers have several critical implications for future use of PTCs in high-conflict and/or refugee communities. First, flexible program delivery is crucial. In this study, the program team used online program modules when the international members evacuated Turkey prior to Week 11, which appeared to work well under the circumstances. Only a future study can ascertain if online modules are an appropriate substitute for in-person delivery. Another method to create flexible delivery is to identify “core” and “optional” program modules, such as in the World Health Organization’s Caregiver Skills Training Programme for children with developmental disabilities (World Health Organization, 2018). With this method, the program can be abridged if needed to ensure participants are exposed to essential program components. Then, given past participants often requested more time in the program, the optional modules can be appended if appropriate.
A second implication from this study is the urgent need to train local professionals to deliver ASD interventions. While training on ASD for teachers in Turkey in general is weak (Rakap et al., 2016), task-shifting approaches, in which local non-specialist providers are trained to deliver ASD interventions, have been successfully implemented in other low-resource countries (Divan et al., 2015) and could be considered in this context. The use of local trainers would also obviate the extra time allotted for Arabic-English interpretation in this study. The follow-up support offered to PTC graduates is partly intended to train future parent and teacher program leaders. However, more work is needed to determine the best method to deliver the mix of program training and follow-up support, and identify which participants are well-suited to be program trainers.
The third implication to improve program feasibility and sustainability is to continue to engage community partners, which can include individuals with ASD, parents and other family members, service providers, policymakers, and other community leaders. In this study, the local partners’ input to the program team on cultural norms were valuable in tailoring the PTCs in Turkey, and their continued involvement helped the team to understand some of the obstacles encountered during program delivery. Nonetheless, the choice of local partners must be made with care, as politics, financial interests, and other factors might influence program delivery and participant recruitment and engagement. Nonetheless, we believe the wide array of benefits associated with community stakeholder involvement to improve scale up activities and program sustainability outweigh the possible drawbacks (Hoekstra et al., 2018).
Program graduates made several recommendations for future program implementation, which overlapped with some of the implications we outlined above. They recommended expanding the quantity and type of resources (e.g. print, video) for parents living outside of urban areas. Similarly, participants wished to identify ways to offer the program to more families and teachers, as well as to improve the attendance and retention of participants. Several participants emphasized the limited capacity of schools and other centers to serve children with ASD, which is consistent with recent research finding limited ASD knowledge among Turkish teachers (Rakap et al., 2016). Others advocated for greater awareness of ASD and more financial and social support for families, common challenges reported in other studies of both Middle Eastern caregivers (Dardas and Ahmad, 2014) and providers (Dababnah, 2018). Finally, despite the literature on the prevalence of trauma-related behaviors in refugee families, only some of the teachers (and none of the parents) specifically addressed their students’ trauma exposure. Teachers observed that trauma exposure was high among the general student population, which was predominantly composed of Syrian refugees. Thus, program graduates suggested the program could be appropriate for teachers and parents of typically developing children as well. More studies are needed to explore these participants’ recommendations for future PTCs.
Limitations
This study is limited by a small sample size, composed solely of Syrian mothers and female teachers living in a city in southern Turkey. Other studies should investigate the broader needs of refugee children with ASD, their caregivers (including fathers and other non-maternal caregivers), and teachers. Furthermore, program team members conducted the interviews described in this article in Week 10 of the intervention, due to the evacuation. Participants possibly would have responded differently if interviewers were not part of the program team, or if the interviews would have been conducted after the final session in Week 12. Future studies should utilize independent interviewers when possible, in order to minimize social desirability bias. Furthermore, we were only able to collect data from those who completed the program. The perspectives of those who discontinued the program would have been valuable to our feasibility and acceptability analyses. Finally, this study only describes one type of data (qualitative interviews). Subsequent research should collect standardized measures on key outcomes, such as parenting stress and child behavior, to assess intervention effects.
Conclusion
This study presented findings from a pilot investigation of a trauma-informed program for caregivers and teachers of children with ASD. The children, caregivers, and teachers were all part of a hard-to-reach and particularly vulnerable population, due to their status as Syrian refugees in Turkey. This study provided initial evidence that a PTC training program to better meet the needs of children with ASD is acceptable. However, challenges to program implementation, including recruitment, attrition, attendance, political events, and limited local research and training capacity, should be expected in future trials. Moving forward, researchers will need to investigate methods to increase the capacity of local non-specialist providers to deliver ASD interventions, to address inherent challenges in sustaining interventions led by international program teams. Future studies will also need to rigorously test the impact of PTC participation on key child, parent, family, and teacher outcomes. Despite these challenges, this research offers important insights on delivering ASD services to support children, caregivers, and teachers in refugee communities.
Supplemental Material
AUT805368_Lay_Abstract – Supplemental material for Feasibility of a trauma-informed parent–teacher cooperative training program for Syrian refugee children with autism
Supplemental material, AUT805368_Lay_Abstract for Feasibility of a trauma-informed parent–teacher cooperative training program for Syrian refugee children with autism by Sarah Dababnah, Serene Habayeb, Benjamin J Bear and Dana Hussein in Autism
Footnotes
Acknowledgements
We are grateful to the families and teachers who participated in this project, as well as Syrian Social Gathering—Mezitli for their support. We thank Melissa Diamond, Kitti Robinson, and other A Global Voice for Autism staff for their critical role in implementing the program.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the support of the Open Society Foundations in funding A Global Voice for Autism for the implementation of Parent-Teacher Cooperatives. The program funder had no role in any aspects of the research, including the data collection, analyses, or manuscript preparation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.