
Abstract
The current study assessed whether reactions to diagnosis are associated with health status for mothers of children with autism spectrum disorder at the time of diagnosis, and whether such diagnostic-reaction resolution status is associated with changes in health status over time. A total of 84 mothers of children newly diagnosed with autism spectrum disorder, with stable reactions to diagnosis over a year, participated. Their perceptions of their physical and psychological functioning, and quality of life, were taken at the time of diagnosis and 1 year later. The mothers were also given the Reaction to Diagnosis Interview. Mothers who had an unresolved reaction to diagnosis had a worse health status in terms of their perception of the physical symptoms at the time of the diagnosis, and showed worsening levels of health over the period of a year, relative to mothers who had a resolved diagnostic status. These relationships were independent of other potential predictors of ill health in this sample. The findings point to the potential of the diagnostic process to negatively impact parental health. Given that this can have negative consequences for child prognosis, as well as parental health, there is a need to develop better understanding of the impacts of diagnostic practices.
Keywords
The physical health of carers for people on the autism spectrum is relatively poor, as measured by self-perceived health status (Allik et al., 2006; Benson, 2017) and self-reports of specific illnesses (Reed et al., 2016b), which is thought to be connected to a compromised immune function (Dykens and Lambert, 2013; Gallagher et al., 2009). It is also known that the mental health of this group is relatively poor (Stewart et al., 2017), especially in terms of experienced stress (Dawson et al., 2016; Osborne and Reed, 2009), anxiety (Bitsika and Sharpley, 2004), and depression (Cohrs and Leslie, 2017). The latter psychological factors mediate between external stressors and physical health (Benson, 2017). Other factors implicated in the physical and mental health of carers include the perceived strength of their social support networks (Lovell et al., 2012; Zaidman-Zait et al., 2017), their physical and financial environment (Barrington et al., 2014), and the severity of the condition of the person for whom they care (McStay et al., 2014).
One key external stressor that has been shown to be pivotal in the development of both psychological (Reed and Osborne, 2012) and physical (Reed et al., 2016a) problems is the diagnostic process for autism spectrum disorder (ASD). Many parents of children undergoing this process believe it to be a major contributor to their stress (Keenan et al., 2010; Osborne and Reed, 2008), and it has been found to be associated with their ability to accept or show “resolution” of the diagnosis (Reed et al., 2018).
Parental “diagnostic resolution” status, across many child conditions, is often assessed by the Reaction to Diagnosis Interview (RDI) that classifies reactions as “resolved” or “unresolved” (Marvin and Pianta, 1996). Resolved reactions reflect parental control over their emotions, and being able to adapt to their child’s condition and the demands placed on their parenthood (Marvin and Pianta, 1996; Poslawsky et al., 2014). Unresolved reactions imply difficulty changing hopes and beliefs about their child and are associated with prolonged “grieving” (Marvin and Pianta, 1996; Poslawsky et al., 2014). Levels of resolved reaction to diagnosis in groups of parents of children with ASD vary across studies from 36% for mothers (Milshtein et al., 2010) to 75% for a mixed group of mothers and fathers (Milshtein et al., 2010; Poslawsky et al., 2014), and these reactions are often quite stable over time (Barnett et al., 2006; Poslawsky et al., 2014).
Parental reaction to a child’s diagnosis of ASD is associated with a range of outcomes for both parent and child; unresolved or unaccepted ASD diagnoses predict poorer mental health in parents (Marvin and Pianta, 1996; Reed et al., 2016a; Sheeran et al., 1997) and poorer child outcomes (Fraiberg et al., 1983; Milshtein et al., 2010). Critically, it is not known whether unresolved reaction to diagnosis will impact parental physical health. This is important to establish, as alterations to the diagnostic process, to improve acceptance, are one of the few things in the control of medical professionals, and there are findings suggestive of a relationship between unresolved reactions and poor health. A lack of diagnostic acceptance or resolution is associated with parental depression (Reed et al., 2016a), and depression mediates between external stressors and health (Benson, 2017). In addition, factors predicting unresolved reactions, such as aspects of the diagnostic procedures (Reed et al., 2016a) and severity of the child’s ASD (Reed et al., 2018), are also known to influence parental health (McStay et al., 2014; Reed et al., 2016b).
Given this, the current study assessed whether diagnostic reactions are associated with health status for mothers of children with ASD at the time of diagnosis, and whether such diagnostic-reaction resolution status is associated with changes in health status over time. To this end, mothers of children newly diagnosed with ASD, whose reaction to the diagnosis did not alter over time, were assessed in terms of their health status at the time of diagnosis and then 1 year later.
Explorations of physical health have used a variety of self-report measures of perceptions of physical-health status, such as the somatic sub-scale of the General Health Questionnaire (GHQ; Allik et al., 2006), and self-reports of the occurrence of specific illnesses, such as through the Immune Function Questionnaire (IFQ; Reed et al., 2016a). Self-report is a strong method in this context, as symptoms are easy to self-discriminate, are often not reported to health professionals, so not visible through medical record inspection, and are often experienced without any objectively verifiable viral cause (Heikkinen and Järvinen, 2003). However, in addition to assessing physical health through the GHQ and IFQ, the current study also employed the World Health Organization Quality of Life (WHOQOL) scale. This scale was included to provide another measure of perceived physical health, but also as it includes measures of two key potential mediators of physical health—the perceived quality of social relationships and the physical environment. Along with measuring parents’ psychological states, using the Hospital Anxiety and Depression Scale (HADS), these measures also allowed analyses of any mediational impacts of these variables, and of changes in these variables, on the relationship between reactions to diagnosis and physical health.
Methods
Participants
The mothers of 120 children, consecutively diagnosed with ASD, were asked to participate within 3 months of receiving the diagnosis. A power analysis based on detecting a medium sized effect (f′= 0.25), with 80% power at the p < 0.05 level, suggested that 57 participants would be required in an analysis involving six variables. As previous research suggested that it might be expected to have around 80% stability over time in reaction to diagnosis (Barnett et al., 2006; Poslawsky et al., 2014), and attrition rate in such research is around 20% (Reed et al., 2016a), it was thought that asking 120 mothers to participate should be sufficient to guarantee power.
Of the 120 mothers approached, 115 (96%) agreed to participate; of these, 95 (82%) provided both a baseline and follow-up assessment. The diagnostic-reaction resolution status changed for 11 (12%) of these mothers over the period, leaving 84 mothers (70% of the original sample) with a stable reaction to diagnosis over the 12-month period. The mean age of the participating mothers was 41.17 (SD = ±8.56, range = 20–54) years; 54 (64%) were married or civil partnership, 11 (13%) were in another form of relationship, and 19 (23%) were single, divorced, or widowed. In terms of occupation, 8 (10%) were classed as laborers, 2 (2%) as skilled, 46 (55%) as managerial/professional, and 28 (33%) as unemployed or home-makers. The ethnic backgrounds of the mothers were 67 (80%) White, 2 (2%) Mixed/Multiple, 8 (10%) Asian; 3 (4%) Black/African/Caribbean, and 4 (4%) Other.
Of the participants diagnosed with ASD, 71 (85%) were males and 13 (15%) females, and their mean age was 5.41 (±4.00, range = 1–25) years at the time of diagnosis. The ASD severity was assessed using the standardized severity score (Gotham et al., 2009) of the Autism Diagnostic Observation Schedule (ADOS; Lord et al., 1999); this mean was 7.70 (±0.98; range = 5–9).
Ethical approval was given by the Psychology Department Ethics Committee of the University.
Measures
The RDI (Marvin and Pianta, 1996; Poslawsky et al., 2014) contains five semi-structured questions asked by a professional to a parent about their feelings and beliefs surrounding the diagnostic process, their child’s condition, and the participant’s reaction to the diagnosis (e.g. “When did you first realize that your child had a medical problem?”). The RDI is analyzed through content analysis, with participant being classified as either “resolved” or “unresolved” based on coding of their responses. There are three sub-types within the “resolved” classification (“feeling-oriented,” “thinking-oriented,” and “action-oriented”) and six sub-types within the unresolved classification (“emotionally overwhelmed,” “angrily preoccupied,” “neutralizing,” “depressive/passive resignation,” “cognitive distortions,” and “disorganized/confused”). Previous studies have noted good inter-coder reliability of RDI classifications and good stability of reactions over time (Poslawsky et al., 2014). In the current study, two coders (blind to the rest of the data relating to the participants) coded the responses according to the RDI manual. Although not specifically certified on use of the RDI, the inter-coder agreement was 100% on the main classifications and 95% on the sub-classifications. Disagreements were settled by discussion.
World Health Organization Quality of Life—Brief (WHOQOL-BREF; WHOQOL Group, 1998) is a 26-item scale measuring participants’ perceptions of their physical health, psychological health, social relationships, and environment over the last 4 weeks, on a 5-point scale (scored 0–4). All questions were given to the participants, but only responses from the Physical, Social Relationships, and Environment sub-scales were employed in the current study, as psychological variables were measured by the HADS. The mean score of items within each domain is multiplied by 4 to give the sub-scale score, varying between 4 and 20, with higher scores denoting higher QoL. In health populations, the mean scores on all domains are typically 15–16 (Hawthorne et al., 2006). The internal reliabilities (α) of the sub-scales in the current study varied between 0.89 for Physical and 0.58 for Social Relationships.
GHQ-28 (Goldberg and Hillier, 1979) measures a range of psychiatric and health problems and is divided into four sub-scales, each with seven items measured on a four-point scale (scored 0–3): somatic symptoms, anxiety and insomnia, social dysfunction, and severe depression. To preserve the reliability of the scale, all questions were asked of the participants, but only the somatic scale was of interest in the current study. The total score on the somatic sub-scale varies between 0 and 21. The internal reliability (α) of the overall scale and the sub-scales for the current study were above 0.70.
IFQ (Reed et al., 2015) assesses the frequency of various symptoms associated with poor immune function. Based on their frequency in the general population, and direct relation to immune deficiencies, the following conditions were selected as a base for the items on the questionnaire: common cold, influenza, cold sores, pneumonia, sepsis, long healing injuries, and skin infections. Following the analysis of the major symptoms of these conditions, 19 symptom items were included on the questionnaire as signs of weakened immune system functioning: sore throat, headaches, flu, runny nose, coughing, cold sores, boils, mild fever, warts/verrucae, pneumonia, bronchitis, sinusitis, sudden high fever, ear infection, diarrhea, meningitis, eye infection, sepsis, and long healing injuries. They were rated on a five-point Likert-type scale (Never, Once or Twice, Occasionally, Regularly, and Frequently with scores from 0 to 4, respectively). A high score reflects worse immune function, with a nonclinical healthy population having a mean of 13.5 (Reed et al., 2015). The internal reliability (α) of the scale for the current study was above 0.70.
HADS (Zigmond and Snaith, 1983) is a self-assessment of levels of anxiety and depression and contains seven items for anxiety and seven for depression. Both scales give scores ranging from 0 to 21; 0–7 = “normal”; 8–11 = “mild”; 12–14 = “moderate”; and 15+ = “severe.” It has a test–retest reliability of 0.86 for anxiety and 0.74 for depression (Hastings and Brown, 2002). The internal reliabilities (α) were 0.78 for anxiety and 0.73 for depression for the current study.
ADOS (Lord et al., 2008) is a semi-structured standardized observation of the child by a professional that measures symptoms of ASD. A standardized calibrated severity score (CSS) can be calculated (Gotham et al., 2009), which has a range of 1–10, with 10 being the most severe symptoms and 4 being the cut-off point for ASD.
Procedure
On diagnosis, mothers were approached by letter, given information about the study, and asked if they, and their child, would like to participate. Once consent had been given, a time was arranged to complete the assessments in the participants’ home. A psychologist administered the HADS, WHO-QUOL-BREF, IFQ, and RDI to the mothers, and the ADOS to the child. All assessments on a particular mother and child were conducted on the same day as one another. After a 12-month period, the mothers were tested again, as noted above. Any missing data were handled by mean substitution, although there were only three instances of this (at the level of a single question) in the current data.
Results
There were 52 (62%) mothers classified as “resolved” in their reaction to diagnosis: 18 “feeling-oriented,” 18 “thinking-oriented,” 22 “action-oriented,” and 12 “feeling-oriented.” Of the 32 (38%) mothers with an “unresolved” reaction to diagnosis, 10 were classed “depressed/passive resignation,” 4 “neutralizing,” 6 “angrily preoccupied,” 8 “emotionally overwhelmed,” and 4 “cognitive distortions.”
Table 1 shows the group-mean scores for the resolved and unresolved sets of mothers on the other variables measured in this study at the point of diagnosis, and the results of the t-tests conducted on these variables. Inspection of these data shows that, at the time of diagnosis, the resolved mothers had significantly less anxiety and depression, but better perceptions of their social relationships, than the unresolved mothers. The resolved mothers also reported significantly better perceptions of their physical health (WHOQOL), and less problems with immune function (IFQ), than the unresolved mothers.
Mean (standard deviation) of scores at baseline for the resolved and unresolved reaction to diagnosis groups.
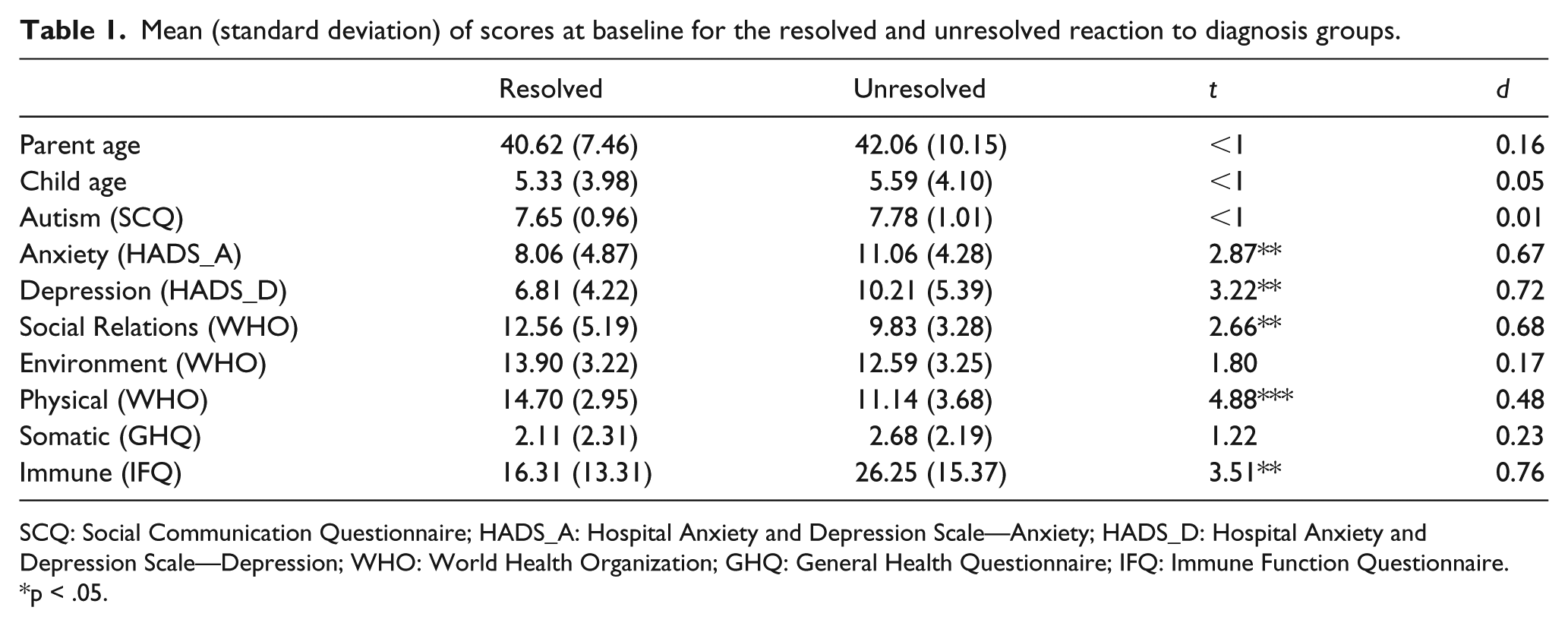
SCQ: Social Communication Questionnaire; HADS_A: Hospital Anxiety and Depression Scale—Anxiety; HADS_D: Hospital Anxiety and Depression Scale—Depression; WHO: World Health Organization; GHQ: General Health Questionnaire; IFQ: Immune Function Questionnaire.
p < .05.
Figure 1 shows the change in the mothers’ scores on the three health-related variables over 12 months. To make these figures easier to interpret positive scores on the figures are improvements in health, and the change scores are expressed as a percentage of the baseline scores, so that the three measures can be compared more directly with one another (the measures having different scales) as a percentage of their baseline health (follow-up minus baseline). Inspection of these data shows that there were increases across all three measures of self-perceived health for the resolved mothers over the 12-month period, but decreases across all three measures of health for the unresolved mothers.
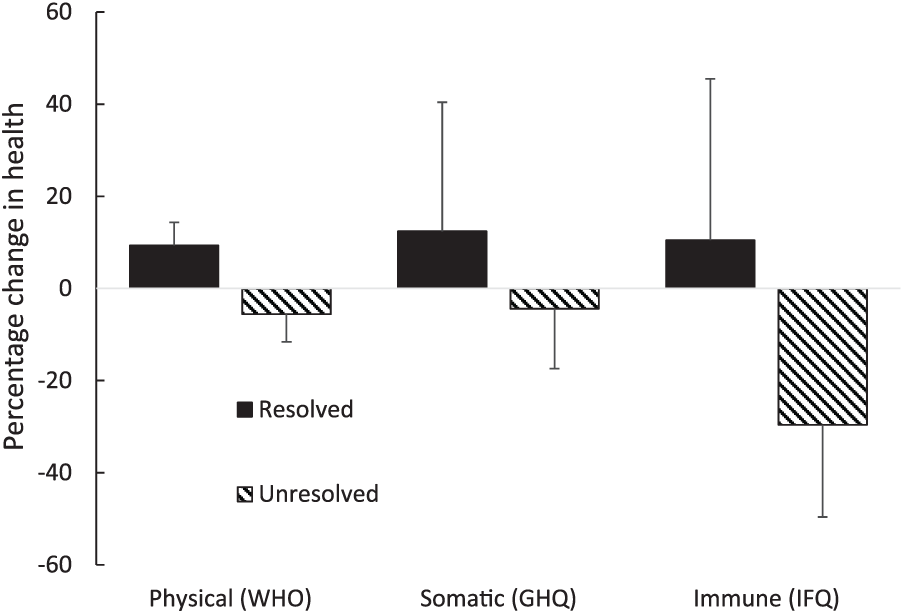
Percentage change in health scores for the two groups (change/baseline score) for perceived physical symptoms (WHOQOL), perceived somatic symptoms (GHQ), and immune function (IFQ). Error bars = 95% confidence limits.
A multivariate analysis of covariance (MANCOVA) was conducted on these data, with the actual change (follow-up minus baseline) in physical (WHO), somatic (GHQ), and immune (IFQ) scores as the dependent variables, resolution of diagnosis (resolved versus unresolved) as the independent variable, and baseline parent age, child age, autism severity (ADOS), anxiety (HADS_A), depression (HADS_D), social relationships (WHOQOL), and environment (WHOQOL) as covariates. This analysis revealed a significant effect of resolution: Wilk’s lambda = 0.500, F(3,73) = 24.32, p < 0.001,
Table 2 shows the results of three separate mediation analyses aimed to establish if there is a direct relationship between reaction to diagnosis and change in each of the three health measures (physical, somatic, and immune) when examining the impact of the change in anxiety, depression, social relationships, and environment, over the 12-month period. A mediation analysis was conducted using the bootstrap method with bias-corrected confidence estimates (Mackinnon et al., 2004; Preacher and Hayes, 2004). In this study, the 95% CI of the indirect effects was obtained with 5000 bootstrap samples (Preacher and Hayes, 2004). Inspection of the top panel shows the relationship between reaction to diagnosis and the change in the mediators. These data revealed only a significant relationship between reaction to diagnosis and a change in anxiety—with resolved mothers showing reduced anxiety over time, relative to the unresolved mothers. The second panel shows the relationship between the change in the mediators and the change in the three health scales, separately. These data show that none of these relationships were significant. The third panel shows the mediation effect of each of the mediators on the relationship between reaction to diagnosis and the change in the health score, separately. All of the confidence limits on these relationships contain zero, meaning that none of these mediated relationships were statistically reliable. The bottom panel shows the direct relationship between reaction to diagnosis and health for each of the three health scores, separately, when the mediating effect is taken into account, and, as none of these confidence limits contain zero, all of these direct relationships remain significant when taking into account the effect of change in the potential mediating variables.
Results (coefficients) of three separate mediation analyses relating RtD to change in health symptoms—physical (WHOQOL), somatic (GHQ), and immune (IFQ)—with change in anxiety (HADS_A), depression (HADS_D), social relationships (WHOQOL), and environment (WHOQOL) as potential mediators.
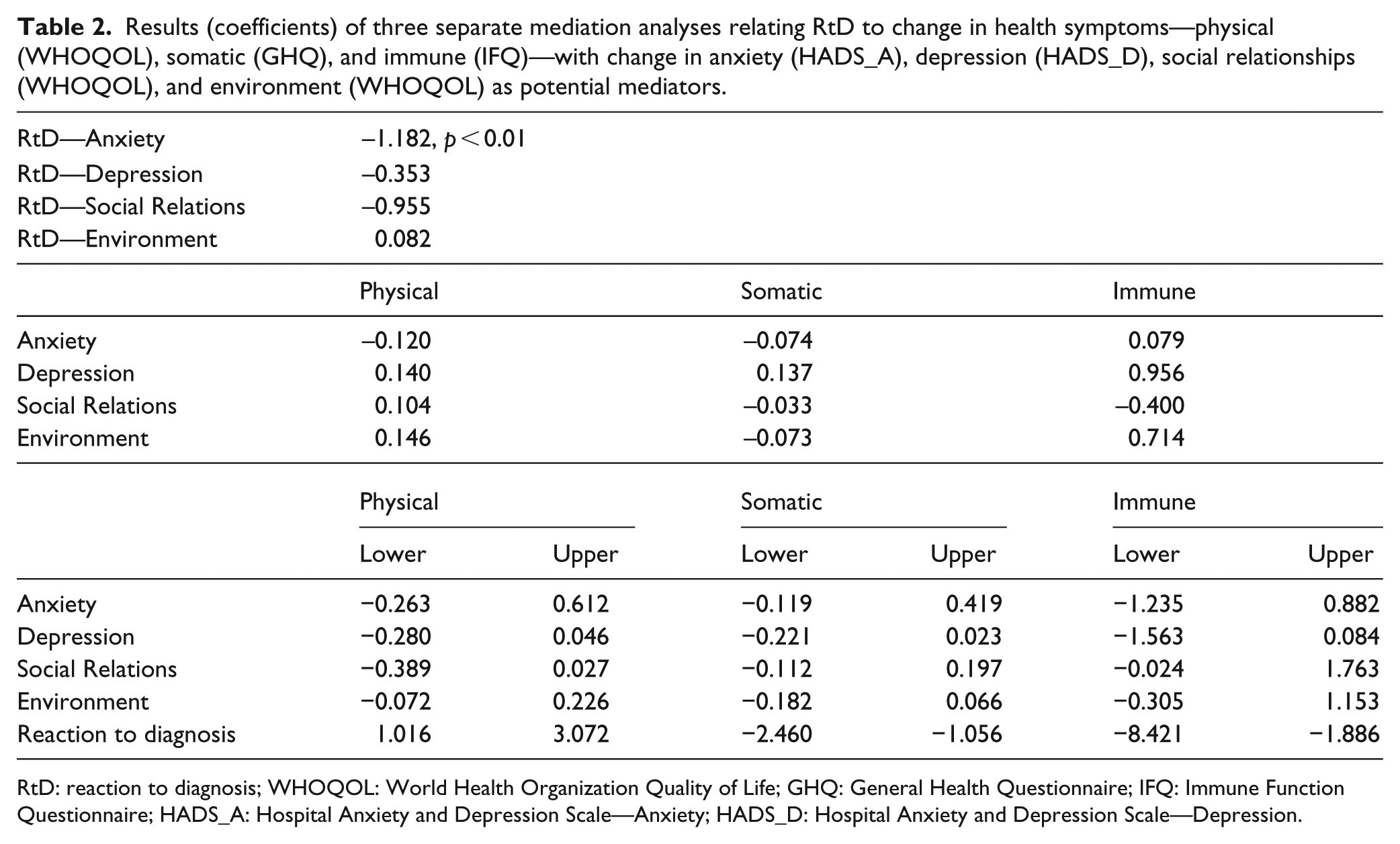
RtD: reaction to diagnosis; WHOQOL: World Health Organization Quality of Life; GHQ: General Health Questionnaire; IFQ: Immune Function Questionnaire; HADS_A: Hospital Anxiety and Depression Scale—Anxiety; HADS_D: Hospital Anxiety and Depression Scale—Depression.
Discussion
The current study examined the relationship between the resolution of a diagnosis for a mother of a child with ASD and their health status at the time of the diagnosis and a year later. It also examined the extent to which the relationship between the resolved or unresolved diagnostic status and the mothers’ health was mediated by a range of predictors also known to be important. The results demonstrated that mothers who had an unresolved reaction to diagnosis had a worse health status in terms of their perception of the physical symptoms (WHOQOL) and their self-report of illnesses (IFQ) at the time of the diagnosis. They also showed worsening levels of health over the period of a year relative to mothers who had a resolved diagnostic status. These relationships were independent of other potential predictors of ill health in this sample, such as their psychological state, or perception of their social relationships and environment.
These findings are the first to show that physical-health status declines over a year if the reaction to diagnosis is not resolved, although they do add to the literature that shows resolution of diagnosis is related to psychological wellbeing at the time of diagnosis (Marvin and Pianta, 1996; Reed et al., 2016a; Sheeran et al., 1997). They also show that, while resolution of diagnosis is related to a range of variables at the time of diagnosis (Barrington et al., 2014; McStay et al., 2014; Reed et al., 2016a; Zaidman-Zait et al., 2017), that these variables do not, in themselves, fully explain the association between diagnostic reaction and later self-reported physical health.
The prime implication of such findings is that the diagnostic process needs to be sensitive to the impact that such a diagnosis will have on the parent. Negatively impacting parental health will, ultimately, produce worse child outcomes (Fraiberg et al., 1983; Milshtein et al., 2010; Osborne et al., 2008). The diagnostic process has long been perceived as a source of parental stress (Goin-Kochel et al., 2006; Keenan et al., 2010; Osborne and Reed, 2008), but there are a number of findings that point to ways in which the process might be improved to reduce the currently found problems. For example, it is suggested that a more measured approach to giving a diagnosis, rather than just a speedy one, will reduce levels of parental psychological problems (Reed et al., 2018). As well as taking the time necessary to reach a diagnosis, such a “measured” approach, might include ensuring greater consistency in the number, and communication, of the professionals who the parents see (Goin-Kochel et al., 2006; Reed et al., 2016a). The current findings clearly point to the need to further develop understanding of the relationships between aspects of diagnostic practices and the impact on parents.
In addition to these principle findings, the current results broadly replicate a number of previously established findings, such as the slightly worse self-reported health of mothers of children with ASD, relative to individuals without this responsibility. Many of the measures of physical health were lower for the sample (both unresolved and resolved), than they have been noted in healthy groups (Allik et al., 2006; Benson, 2017; Reed et al., 2016b). The results also show poorer reports of psychological wellbeing in the current sample than might be expected in a general population, and worse perceptions of their social relationships (Barrington et al., 2014; McStay et al., 2014; Zaidman-Zait et al., 2017). The level of resolution of diagnosis in the current sample was over 60%, which is within the range typically found for this population (c.f. Milshtein et al., 2010; Poslawsky et al., 2014), and the stability of these reactions, over time, was quite high in this sample, but similar to that noted in other studies (Barnett et al., 2006; Poslawsky et al., 2014).
There are limitations to the current findings that need to be acknowledged. It is important to note that the current findings were obtained from a single clinic, and it may be that practices in other clinics would produce different results. Although this remains a possibility, the children were assessed by a multidisciplinary team, employing standard diagnostic practices. The representativeness of a sample of mothers who volunteered for such research needs to be highlighted. Although, as the majority of mothers approached agreed to participate, this may mitigate concerns about representativeness. The low number of females with ASD included, and the lack of information on mental and physical-health status prior to inclusion in the study, might have implications for the generalizability of the results, and these factors could be studied in future work. Although this study confirmed an important association between RDI for mothers and their health perceptions, a causal link between health perception and diagnostic-reaction resolution status could be possible. Therefore, previous health status of the mothers could be an influencing factor/predictor of reaction to ASD diagnosis and could be of interest in future research. Neither is it known if the findings would replicate with fathers.
In addition, it might have been useful to collect data on the proportion of parents in each group (resolved and unresolved), who had other children with ASD and related disabilities. In a larger sample, where diagnostic-reaction resolution status changed over the course of the study, it could be instructive to determine the directions of change occurring. Similarly, examining the relationship between outcomes and the various sub-classifications of the RDI might also be useful. Exploration of these issues needs to be conducted with a larger sample size. Finally, the subjective rating scales used for assessing physical health need to be acknowledged, and replication with objective measures would support the findings.
Notwithstanding these caveats, the current results demonstrate that mothers who had an unresolved reaction to diagnosis had poor health at the time of the diagnosis, which got worse over the period of a year. This association was independent of a range of other predictors of ill health. Given the importance of parental functioning to the child’s prognosis, these findings point to the need to further develop understanding of optimal diagnostic procedures in this field.
Supplemental Material
AUT815641_Lay_Abstract – Supplemental material for Reaction to diagnosis and subsequent health in mothers of children with autism spectrum disorder
Supplemental material, AUT815641_Lay_Abstract for Reaction to diagnosis and subsequent health in mothers of children with autism spectrum disorder by Phil Reed and Lisa A Osborne in Autism
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.