
Abstract
Research has shown that individuals with autism spectrum disorder have higher rates of health problems throughout childhood, adolescence, and adulthood, and that this may result in elevated risk of early mortality. This study reported the rate, timing, and causes of death in a large community-based cohort of adolescents and adults with autism spectrum disorder (n = 406) over a 20-year period (1998–2018) and identified predictors of mortality. Over this period, 6.4% of individuals died at an average age of 39 years. Causes of death included chronic conditions (such as cancer and heart disease), accidents (such as choking on food and accidental poisoning), and health complications due to medication side effects. Even after controlling for age and health status, significant predictors of mortality were early childhood levels of impairments in social reciprocity and high levels of functional impairments at the start of the study period. The results suggest the importance of social engagement and functional self-sufficiency across the life course, as well as adequate access to health care for individuals with autism spectrum disorder.
Although studies have shown that there is some abatement of autism symptoms over time (Woodman, Mailick, Anderson, & Esbensen, 2014) many individuals with autism spectrum disorder (ASD) continue to experience significant challenges throughout adulthood. For example, adults with ASD, with and without intellectual disability (ID), have high rates of unemployment and underemployment (Roux, Shattuck, Rast, Rava, & Anderson, 2015; Taylor, Henninger, & Mailick, 2015; Taylor & Seltzer, 2011). Most individuals with ASD continue to have problems with social relationships during adulthood and many do not live independently (Henniger & Taylor, 2013; Howlin & Moss, 2012; Roux et al., 2013).
In addition to these difficulties, individuals with ASD have been shown to have higher rates of health problems across a wide range of health domains than controls (Croen et al., 2015; Fortuna et al., 2016). Individuals with ASD also have limited access to health care (Nicolaidis et al., 2012; Weiss et al., 2018) and are at risk for taking increasing numbers of medications over time (Esbensen, Greenberg, Seltzer, & Aman, 2009). Notably, disparities in health-care access for individuals with ASD that are apparent during childhood (Chiri & Warfield, 2012) persist throughout the transition to adulthood (Cheak-Zamora et al., 2013, 2014). Relatively little is known, however, about mortality risk for this population and what factors might be associated with this risk. To address this gap, this study prospectively examined risk for mortality over a 20-year period in a large, well-characterized sample of adolescents and adults with ASD and predictors of death.
There is a small but growing literature suggesting that individuals with ASD may have an increased risk of mortality than the general population (Woolfenden, Sarkozy, Ridley, Coory, & Williams, 2012). For example, in a Danish cohort of 341 individuals with ASD followed from 1960 to 2006, individuals with ASD died at twice the expected rate of the general population (Mouridsen, Bronnum-Hansen, Rich, & Isager, 2008). In this study, there were no differences in mortality risk between those with ASD and ID compared with those with ASD without ID, with frequent causes of death including epilepsy, infectious diseases, and accidents. More recently, Hirvikoski et al. (2016) conducted a population-based case–control study of Swedish health registries and found an increased mortality for individuals with ASD compared with the population; this risk was found across the range of the autism spectrum and for both males and females, although the risk was highest among females with ASD with the lowest levels of functioning.
In the United States, Bishop-Fitzpatrick and colleagues (2018) recently analyzed diagnostic codes from electronic health records of decedents with ASD and matched decedent community controls. Results from machine learning suggested that there were distinct lifetime diagnostic patterns, with the decedents with ASD having higher rates of most health conditions. The decedents with ASD also died at younger ages (about 20 years earlier than control decedents). Finally, a follow-up of a statewide autism prevalence study in Utah found elevated mortality risk for individuals with ASD (Bilder et al., 2013). Medical comorbidities and ID were related to death. Common causes of death included respiratory, cardiac, and epileptic events. Interestingly, in this study, in addition to community controls, individuals with autism were compared with family controls (i.e., siblings and cousins); findings suggested that some of the mortality risk observed for individuals with ASD may be explained by familial factors (Bilder et al., 2013).
Taken together, these studies suggest that individuals with ASD may be at a greater risk for early mortality than the general population. However, little is known about the factors that explain this risk. The most consistent finding is that certain co-occurring health conditions, particularly seizures, may be associated with elevated risk (Gillberg, Billstedt, Sundh, & Gillberg, 2010; Pickett, Xiu, Tuchman, Dawson, & Lajonchere, 2011). Evidence is mixed regarding the relative risk for men versus women; some studies have found elevated risk for women (Gillberg et al., 2010; Hirvikoski et al., 2016), whereas others have not (Bilder et al., 2013).
However, to the best of our knowledge, no past research has examined which aspects of the behavioral phenotype of ASD (e.g., severity of autism symptoms, behavior problems, and daily living skills) might signal elevated risk years before the death occurs. While some aspects of the behavioral phenotype may be fixed, others are malleable and hence may be targets for intervention that could reduce early mortality in this population. Some past research (e.g., Bilder et al., 2013; Hirvikoski et al., 2016) has examined whether co-occurring ID increases the risk of mortality, but ID status tends not to be a malleable factor, which is the focus of this research. There is thus a need for more research to explore what aspects of the behavioral phenotype of ASD may contribute to mortality.
Present study
Although factors such as autism symptom severity and daily living skills have been shown to be predictive of adult outcomes such as independence and employment (Eaves & Ho, 2008; Farley et al., 2009; Shattuck et al., 2012; Taylor & Mailick, 2014), these behavioral features of individuals with ASD have not yet been studied as predictors of mortality. This study addressed this gap by examining the timing and cause of death and identified the factors associated with mortality risk in a large, community sample of adolescents and adults with ASD who were prospectively followed over a 20-year period.
Methods
Data and sample
Data for this study were from a large, longitudinal study of families of adolescents and adults with ASD in Massachusetts and Wisconsin (Seltzer et al., 2011). The study began in 1998 with families of 406 adolescents and adults with ASD who were then aged 10 years or older and was carried out over 14 years. Families were recruited via informational packets distributed by agencies, schools, and diagnostic clinics as well as media announcements. All families met three initial inclusion criteria: (a) they had a child aged 10 or older; (b) the parent reported that the child had received a diagnosis of ASD from a medical, psychological, or education professional; and (c) there was a confirmation of parent report of diagnosis based on research-administered Autism Diagnostic Interview-Revised (ADI-R; Lord, Rutter, & Le Couteur, 1994).
Mortality information was collected in three phases. During the 14-year study period, information about the death of adolescents and adults with ASD was reported by the mother (or other family respondents if the mother predeceased the adult with ASD); 19 individuals with ASD were consequently identified as deceased. Second, in December 2017, we contracted with the University of Wisconsin Survey Center (https://uwsc.wisc.edu) to trace all 406 cases to confirm family-reported deaths and to identify additional deceased cases whose death occurred after the study ended. Specifically, the Survey Center traced mortality using LexisNexis and confirmed via obituaries. Identity was triangulated using the names of the adult child, the parent, and the parent’s spouse, along with last known and historical addresses and phone numbers. Five additional cases were thus identified as deceased. Finally, in February 2018, an on-line obituary search on all 406 cases identified two additional deceased adults with ASD. The deaths of these two cases were subsequently confirmed by their family members. Combined, these methods identified 26 deceased individuals with ASD out of the original 406 cases over a 20-year period.
The average household income for families in 1998 (Time 1) was about US$43,000, with an average of 2.8 children per family (including the adolescent or adult with ASD). About two-thirds (65%) of the individuals with ASD were living at home with their parents at Time 1. Nearly half (45.1%) of mothers had college degree or higher level of education. There were no significant differences in these family background variables between those whose son or daughter died and those who remained alive.
Measures
We examined the following predictors of mortality of individuals with ASD: age, sex, ID status, health status, maladaptive behavior, lifetime autism symptomatology, and daily living skills. All predictors were measured at the start of the study (referred to as Time 1) and based on maternal reports unless noted otherwise.
Age was calculated in years based on date of birth and date of the Time 1 interview.
ID status
ID status was determined using various sources including the Wide Range Intelligence Test (WRIT; Glutting, Adams, & Sheslow, 2000), the Vineland Screener (Sparrow, Carter, & Cicchetti, 1993), and a review of available educational records. As noted by Taylor and Seltzer (2010), ID status (0 = no intellectual disability and 1 = intellectual disability) was determined using a variety of sources. Standardized intelligence quotient (IQ) was obtained by administering the WRIT (Glutting et al., 2000) and adaptive behavior was assessed by administering the Vineland Screener (Sparrow et al., 1993). The WRIT is a brief measure with strong psychometric properties and both verbal and non-verbal sections. The 45-item Vineland Screener measures daily living skills in the youth with ASD and correlates well with the full-scale Vineland score (r = 0.87 to 0.98). It has high inter-rater reliability (r = 0.98) and good external validity (Sparrow et al., 1993). Individuals with standard scores of 70 or below on both IQ and adaptive behavior measures were classified as having an ID, consistent with diagnostic guidelines (Luckasson et al., 2002). For cases where the individual with ASD scored above 70 on either measure, or for whom either of the measures was missing, a review of records by three psychologists, combined with a clinical consensus procedure, was used to determine ID status.
Physical health status of individuals with ASD was rated by mothers on a 4-point scale: 0 = poor, 1 = fair, 2 = good, and 3 = excellent. Considerable previous research has provided evidence of the validity of such health ratings in predicting mortality (Idler & Benyamini, 1997). For this study, due to the small number in the “poor” category, the “poor” and “fair” categories were combined to create a three-category variable: poor/fair health, good health, and excellent health. Criterion validity of health ratings in this sample is indicated by the significant association with worsening health during the past 12 months (chi-square = 123.50, p < 0.001) and with number of prescription medications (F = 4.42, p < 0.05).
Maladaptive behaviors were measured by the Problem Behavior subscale of the Scales of Independent Behavior-Revised (Bruininks, Woodcock, Weatherman, & Hill, 1996). Respondents indicated whether eight categories of behavior problems were manifested during the past 6 months: hurtful to self, unusual or repetitive habits, withdrawal or inattentive behavior, hurtful to others, destructive to property, disruptive behavior, socially offensive behavior, and uncooperative behavior. The summary score was a count of the number of behavior problems manifested, ranging from 0 to 8. Reliability and validity have been established by Bruininks et al. (1996).
Autism symptomatology
Autism symptoms were assessed using the ADI-R (Lord et al., 1994), a standardized diagnostic interview administered to the parent. The ADI-R yields two ratings: the “lifetime” rating and the “current” rating. This analysis focused primarily on the “lifetime ratings,” which reflected the severity of symptoms when the individual with ASD was aged 4–5 or the most severe level of impairment ever exhibited by the individual. Summary scores are computed that reflect lifetime impairments in non-verbal communication, lifetime impairments in reciprocal social interaction, and repetitive behaviors and interests. We also measured “current” ratings on these same symptoms, reflecting severity of autism symptoms at Time 1.
Daily living skills
To measure the degree of independence in activities of daily living, the Waisman-Activities of Daily Living scale (W-ADL; Maenner et al., 2013) was used. The W-ADL consists 17 items assessing the level of independence in typical daily activities such as self-care, meal preparation, household tasks, and community activities such as running errands. Each item was rated on a 3-point scale (0 = does not do at all, 1 = does with help, and 2 = independent) and summed up to create a total score. The internal consistency (Cronbach’s α) of the W-ADL was 0.903. Criterion validity of the W-ADL for adults with ASD was previously established (Maenner et al., 2013). Specifically, Maenner et al. (2013) reported how the W-ADL differentiated among individuals with mild, moderate, severe, and profound ID. Of the 34-point scale, those with mild ID scored 24.9 on average, those with moderate ID scored 21.8 on average, those with severe ID scored 16.1 on average, and those with profound ID scored 5.8 on average. Although these benchmarks were generated by data on individuals with Down syndrome, other research has shown that the scale works similarly for adults with ASD (Smith et al., 2012).
Plan for data analysis
Descriptive data were computed comparing those adults with ASD who died during the study period and those who survived using chi-squares and analyses of covariance (controlling for age of the individual with ASD). “Premature death” was computed based on age at Time 1, using sex-specific life tables (Centers for Disease Control and Prevention (CDC)—National Center for Health Statistics, n.d.) and was defined as the number of years between age at death of an individual and his or her life expectancy at Time 1. Causes of death were enumerated, with the sex of the decedent noted as well as whether the decedent had ID. Cox proportional hazard modeling was used to predict survival versus mortality over the 20-year period, with all predictors measured at Time 1.
Results
Descriptive findings
Table 1 presents a comparison of the characteristics of individuals with ASD who died between 1998 and 2018 and those who remained alive. In 1998, at the beginning of the study period, the sample members ranged in age from 10 to 52 years of age. Those who died during the next 20 years averaged nearly 9 years older at Time 1 than those who survived. In addition, those who died were in significantly poorer health at Time 1, with half as many rated as being in excellent health and more than twice as many rated as being in fair or poor health at Time 1 as those adults who survived over the next 20 years. However, the two groups did not differ in sex or ID status, with the majority of both groups classified as having ID.
Descriptive statistics of individuals with ASD and family background (all measured at Time 1).
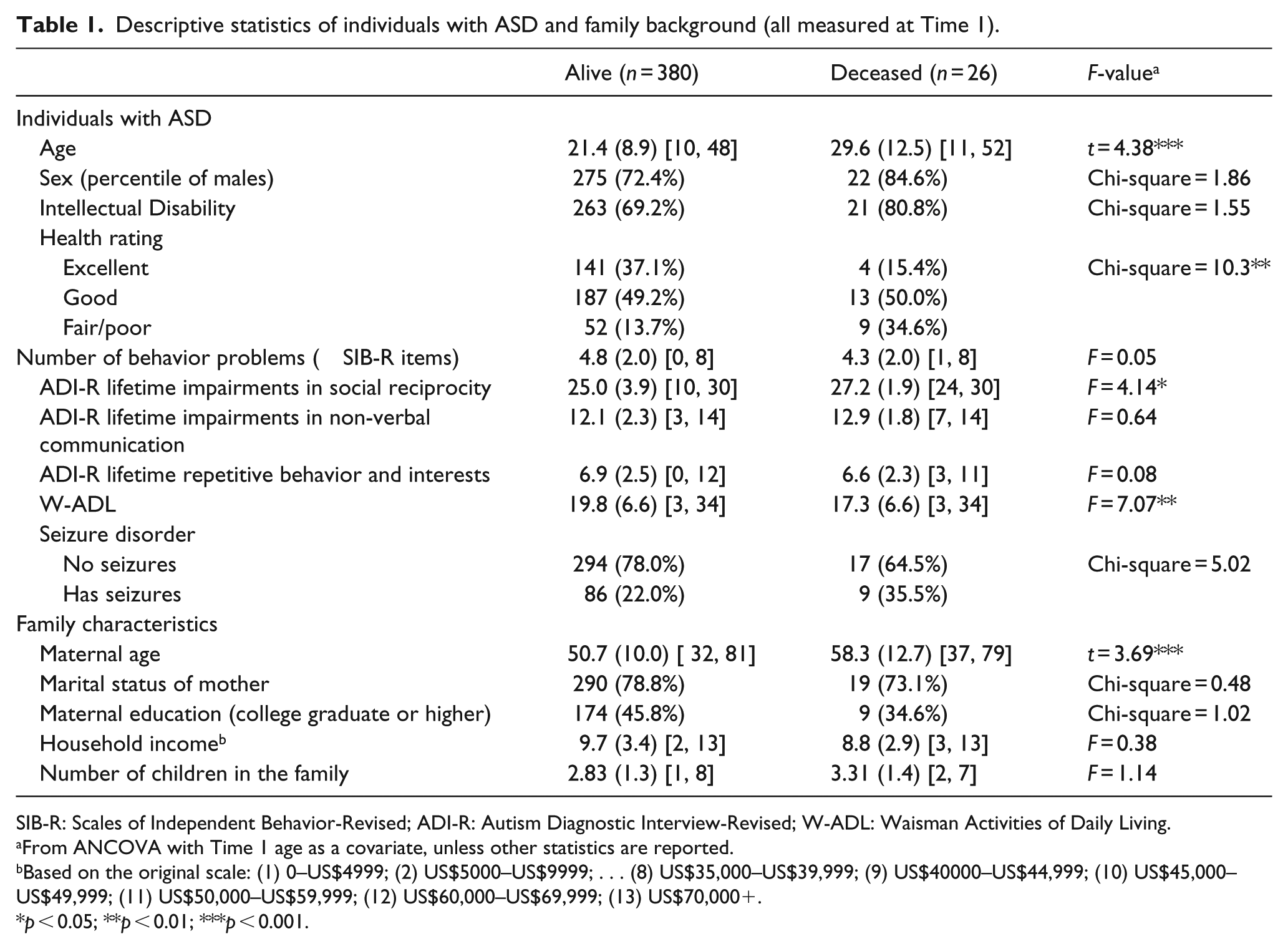
SIB-R: Scales of Independent Behavior-Revised; ADI-R: Autism Diagnostic Interview-Revised; W-ADL: Waisman Activities of Daily Living.
From ANCOVA with Time 1 age as a covariate, unless other statistics are reported.
Based on the original scale: (1) 0–US$4999; (2) US$5000–US$9999; . . . (8) US$35,000–US$39,999; (9) US$40000–US$44,999; (10) US$45,000–US$49,999; (11) US$50,000–US$59,999; (12) US$60,000–US$69,999; (13) US$70,000+.
p < 0.05; **p < 0.01; ***p < 0.001.
Adults who later died were significantly less independent in their activities of daily living at Time 1 than those who remained alive over the next 20 years. The specific Time 1 W-ADL items that significantly differentiated those who later died from those who remained alive (controlling for age) were independence in toileting; making one’s bed; doing household tasks (including picking up around the house, putting things away, light housecleaning, etc.); doing home repairs (including simple repairs around the house, non-technical in nature, for example, changing light bulbs or repairing a loose screw); and preparing complete meals (all p < 0.05), and at a trend level, running errands (including shopping in stores) and banking and managing daily finances (including keeping track of cash, checking account, paying bills, etc. (all p < 0.10)).
In addition, adults who later died had significantly greater lifetime impairments in social reciprocity. However, they did not differ in other core domains of autism symptoms (lifetime impairments in non-verbal communication, lifetime restricted repetitive behaviors and interests). They also did not differ in the severity of their behavior problems at the start of the study period.
Table 2 presents data on the age at death and causes of death of the 26 individuals with ASD who died during the 20-year study period. The youngest death was at age 18 and the oldest was at age 65, with the average age at death being 39. Decade by decade, most deaths occurred during the 40s (n = 8) but nearly that many died in their 20s (n = 6) or 30s (n = 6).
Age and causes of death of individuals with ASD.

Premature death defined as the number of years the individual died before his or her life expectancy.
Female.
Does not have ID.
We calculated the extent of “premature death,” defined as the number of years the individual died before his or her life expectancy (life expectancy was calculated at Time 1 for each individual). The average number of years of premature death in the current sample was 38.5 years (range = 16.8–57.7 years before the individual’s life expectancy).
Also shown in Table 2 are causes of death. The most common causes of death were cardiac arrest and cancer, each reported for five adults. Cancers included breast, colon/liver, rectal, and spine, as well as one unspecified type of cancer. Three adults died due to seizures, three from respiratory failure or pneumonia, two died from choking on food, and two others died following health complications due to medication side effects (Thorazine and Depakote). The causes of death of five adults were unknown.
Prediction of mortality in adults with ASD
We used Cox proportional hazard models to predict the factors associated with the mortality of individuals with ASD over 20 years (Table 3). The predictors, all measured at Time 1, were evaluated in three blocks. The first block included age, sex, and ID status. The second block added health status. The third block included behavior problems, lifetime autism symptomatology, and daily living skills. As shown in Model 1, the age of the individual with ASD in 1998 was a significant predictor of mortality. For every 1 year older age at the start of the study period, the individual had a 7% greater risk of dying over the next 20 years. Sex and ID status were not predictive of mortality.
Predictors of mortality for individuals with ASD (Cox proportional hazard models).
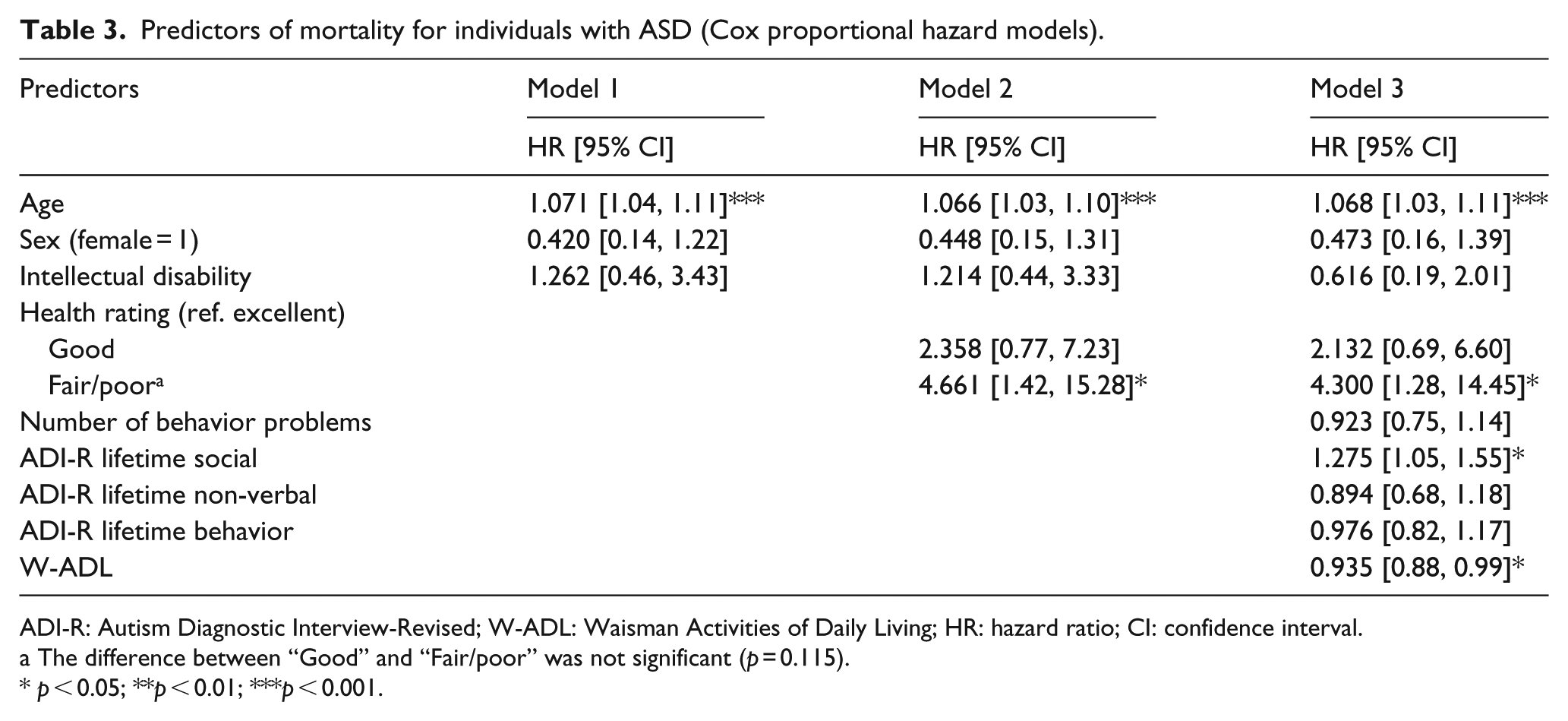
ADI-R: Autism Diagnostic Interview-Revised; W-ADL: Waisman Activities of Daily Living; HR: hazard ratio; CI: confidence interval.
The difference between “Good” and “Fair/poor” was not significant (p = 0.115).
p < 0.05; **p < 0.01; ***p < 0.001.
Model 2 shows the incremental effect of health status at Time 1 in predicting mortality, net of age, sex, and ID status. Being in fair or poor heath at Time 1 conferred a 46% greater risk of dying over the next 20 years than being in excellent health at Time 1.
Model 3 indicates that even controlling for initial age and health status (both of which remained significant predictors), two additional factors predicted mortality over the next 20 years: independence in activities of daily living and lifetime impairments of social reciprocity. For every one point higher score on the measure of activities of daily living in 1998 (signifying higher levels of independence), individuals with ASD had a 6.5% lower risk of mortality over the next 20 years. For every one point higher score on the measure of lifetime impairments in social reciprocity (signifying greater levels of impairment at age 4–5), there was a 27% higher risk of mortality during the 20-year study period. The other two “lifetime” measures of autism symptoms (lifetime impairments in non-verbal communication and restricted repetitive behaviors and interests) were not significant predictors of mortality.
In follow-up analyses (data not shown), we examined whether each of these lifetime measures of autism symptoms would be predictive of mortality if the other two lifetime measures were not included in the Cox regression model. The only one that was a significant predictor was lifetime impairments in social reciprocity. Notably, none of the ADI-R measures that reflect current functioning at Time 1 was a predictor of mortality.
Discussion
This study reports on predictors of mortality over a 20-year period in a large community-based cohort of adolescents and adults with ASD. In this cohort, 6.4% died during the 20-year follow-up period, and the average age at death was 39 years. These individuals died an average of 38.5 years prior to their life expectancy. Causes of death were diverse, including chronic conditions (such as cancer and seizures), accidents (such as choking on food and accidental poisoning), and health complications due to medication side effects. Our results build on previous research that has indicated that individuals with ASD have a higher risk for mortality than the general population (Hirvikoski et al., 2016; Mouridsen et al., 2008; Woolfenden et al., 2012) and have health risks that could contribute to earlier death (Croen et al., 2015; Fortuna et al., 2016). Specifically, our results confirm prior research showing that seizures and accidents are common causes of death for individuals with ASD (e.g., Hirvikoski et al., 2016; Mouridsen et al., 2008). However, our study differs from past research in that we investigated behavioral factors that predict mortality as well as causes of death.
Not surprisingly, age and health were major factors that predicted death in this study. Being in fair or poor health was the strongest predictor of mortality, increasing the risk of dying over the next 20 years by 46% (compared to being in excellent health). In a review of 27 US and international studies of representative community samples, the validity of self-reported heath ratings in predicting subsequent mortality was firmly established, above and beyond other indicators of health such as physicians’ ratings and biomarkers (Idler & Benyamini, 1997). The review concluded that health ratings are valuable because they are holistic, capturing the “full array of illnesses a person has and possibly even symptoms of disease as yet undiagnosed but present in preclinical or prodromal stages” (p. 27). In this study, the health ratings were made by mothers of the adolescents and adults with ASD, and the findings reported here underscore the importance and predictive validity of parent-reported health ratings for individuals who have compromised ability to communicate on their own behalf.
Even after controlling for age and health status, we found that limited self-sufficiency in activities of daily living was an important predictor of mortality for adults with ASD. Past research has indicated that children with ASD show poorer adaptive functioning than typically developing children (Franchini et al., 2018) and that adolescents and adults with ASD have greater impairments in ADL self-sufficiency than individuals with other developmental disabilities, such as those with Down syndrome (Esbensen, Seltzer, & Krauss, 2008; Esbensen, Bishop, Seltzer, Greenberg, & Taylor, 2010; Smith et al., 2012). Furthermore, it has been shown that ADL skills that are acquired by adults with ASD are not maintained over time to the same extent as those with Down syndrome (Smith et al., 2012). Importantly, ADL self-sufficiency by adults with ASD has been shown to be responsive to environmental influences (Taylor et al., 2014). For example, employed adults with ASD are more likely to improve their ADL skills over time than unemployed adults with ASD, perhaps due to expectations set by the workplace for personal hygiene and related ADL skills (Taylor et al., 2014). ADL skills are malleable and dynamic, and hence, interventions aimed at building self-sufficiency in daily living skills are important to provide to children, adolescents, and adults with ASD. In addition, setting high expectations for maintaining such skills during the life course may have implications for health maintenance and even survival.
Perhaps the most intriguing finding of this study concerns the extent to which impairments in social reciprocity, as evidenced in early childhood, are predictive of mortality that occurs decades later in adulthood. Confirmation of this finding in future research is needed, but the magnitude of the effect in our sample is notable. Examples of impairments in social reciprocity include abnormalities in joint attention, social smiling, responsivity to the approaches of others, interest in people, exhibiting a range of appropriate facial expressions to communicate, and social overtures. Early intervention has been shown to ameliorate the core symptoms of autism, including social reciprocity impairments (Kasari & Patterson, 2012; Kasari et al., 2015; Schreibman et al., 2015; Tachibana et al., 2017), and reduction in the severity of symptoms early in childhood has been shown to have long-term effects on later adaptive behavior and autism symptoms (Kasari et al., 2012; Klintwall et al., 2015; Perry et al., 2017). Our findings suggest that these effects may extend into adulthood, potentially influencing mortality. Future research that elucidates the mechanism by which impairments in social reciprocity may directly or indirectly affect survival in adulthood is needed to understand this finding fully, but the findings point to the importance of lifelong social engagement.
This study is not without methodological limitations. The analysis suffers from both right and left censoring, as only individuals who survived to age 10 were eligible to participate in the longitudinal study, and 75% of the members of the study cohort are still alive. Although this research was based on a volunteer community sample, the adults were largely Caucasians and hence the results may not be representative of a more diverse population of adults with ASD. Furthermore, compared to children diagnosed today, a larger proportion of adults with ASD in this generation had co-occurring ID; they also experienced a different service landscape. For this reason, generalizability of findings may be limited. Finally, knowing the cause of death is informative, but it does not fully capture the sequence of health problems that may have led to deaths. Juxtaposed against these limitations are strengths of the research, including the long follow-up period, the large-sized sample, and the utilization of measures of risk factors that are commonly available on children and adults with ASD. For these reasons, clinical screening for these risk factors would potentially be feasible.
Taken together, the findings of this study suggest that the risk of mortality in adults with ASD might be reduced by identification of individuals judged by their parents to be in fair or poor health and attending to any unmet health-care needs, participating in early intervention to reduce impairments in social reciprocity symptoms, and receiving interventions across the life course to support acquisition and maintenance of self-sufficiency in ADL skills. Studies of the effects of these population health approaches are needed to confirm the findings of this research and to enhance the survival of adults with ASD.
Supplemental Material
AUT827412_Lay_Abstract – Supplemental material for Mortality in individuals with autism spectrum disorder: Predictors over a 20-year period
Supplemental material, AUT827412_Lay_Abstract for Mortality in individuals with autism spectrum disorder: Predictors over a 20-year period by Leann Smith DaWalt, Jinkuk Hong, Jan S Greenberg and Marsha R Mailick in Autism
Footnotes
Funding
This study was supported by the National Institute on Aging (grant/award no.: R01AG08768), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (grant/award no.: P03HD03352), and Autism Speaks (grant/award No.: 7724).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.