
Abstract
Functional outcomes in autism spectrum disorder can be highly variable given the heterogeneous nature of autism spectrum disorder and its interaction with environmental factors. We set out to compare parent/caregiver perceptions of functioning in two divergent countries that participated in the International Classification of Functioning Disability and Health (ICF) Core Set for Autism Spectrum Disorder development study. We focused on the frequency and content of items reported, and hypothesized that environmental factors would most frequently be reported as barriers to functioning in low-resource settings. Using frequency and qualitative content analysis, we compared data from South Africa (n = 22) and Sweden (n = 13). Frequency agreement was seen in three activities and participation categories, and one environmental factor. Obvious frequency differences were observed in one environmental factors category, six body functions categories and three activities and participation categories. Only three ICF categories (immediate family, attention functions, products and technology for personal use) differed in content. Contrary to our hypotheses, few differences in perspectives about environmental factors emerged. The universality of our findings supports the global usefulness of the recently developed ICF Core Sets for Autism Spectrum Disorder. We recommend that more comparative studies on autism spectrum disorder and functioning should be conducted, and that similar comparisons in other disorders where Core Sets have been developed may be valuable.
Keywords
Introduction
Autism spectrum disorder (ASD) is recognized by the World Health Organization (WHO; 2013) as a global public health concern with a global prevalence rate in excess of 1% (Baxter et al., 2015; Christensen et al., 2016; Elsabbagh et al., 2012). Importantly, approximately 90% of individuals with ASD live in low/middle-income countries (LMICs; de Vries, 2016; Franz, Chambers, von Isenburg, & de Vries, 2017; Kieling et al., 2011). Although the clinical characteristics of ASD present the same in individuals who live in high-income countries (HICs) and LMICs (Abubakar, Ssewanyana, de Vries, & Newton, 2016; de Vries, 2016; Newton & Chugani, 2013), the significant contextual differences between HICs and LMICs may result in very different consequences in functioning (Daley, 2002). For example, stigma surrounding ASD is common in many LMICs and often attributed to lack of knowledge regarding ASD (Gilligan, 2013; Gona et al., 2016; Minhas et al., 2015). Stigma can have a restricting impact on the lives of individuals with ASD and their families resulting in lack of support and services, mistreatment and even abuse (Minhas et al., 2015; Qian, Chle, & Bogenschutz, 2012). Another example is the impact that infrastructure and public services can have on functioning. One can expect that public transport services in HICs might be better sign-posted, more punctual and better organized than in an LMIC, which could impact an individual’s ability to make use of these services, either independently or assisted by a caregiver.
Little is currently known about the possible role of sociocultural factors, race and ethnicity on the manifestation, treatment and outcomes of ASD (Daley, 2002; Wallis & Pinto-Martin, 2008). Even in HICs racial/ethnic minority families are significantly underrepresented in research (Wallis & Pinto-Martin, 2008). This may limit the generalizability of findings (Ratto et al., 2016) and our understanding of the complex interplay between genetic, environmental, sociocultural and other factors (Sotgiu et al., 2011). A better understanding of ASD across different environments/settings may help determine the suitability of clinical tools and strategies in low-resource settings and may indicate the need for specific adaptations or particular programmes in specific settings. In contemporary ASD interventions, the principles of naturalistic developmental behavioural approaches (NDBI) implies the need to understand the environment and customs in a specific community setting, in order to make the required environmental arrangement and to use suitable behaviour principles to address and improve outcomes (Daley, Singhal, & Krishnamurthy, 2013; Guler, de Vries, Seris, Shabalala, & Franz, 2018; Schreibman et al., 2015).
In this study, we were particularly interested in the functional impact of ASD as preceived by parents/caregivers on children from different socioeconomic settings. Parents/caregivers are arguably the most important people in the life of a child with ASD as they directly influence the social setting, support, relationships, stimulation and services that are accessed in the crucial first few years, as well as throughout childhood and teenage years. Parents are most likely to notice the first signs of ASD and have the responsibility to seek assessment and intervention for their child. In some countries, especially low-income countries with fewer resources, the burden of care falls almost entirely on parents (Minhas et al., 2015; Qian et al., 2012). The functional impact of ASD is most often the first sign to parents/caregivers, and therefore the motivating factor in starting the diagnostic and intervention process. For example, functional delays in speech and language development, or in communication, and challenging behaviours are often the functional markers that will motivate parents to seek access to assessment and treatment (Azad & Mandell, 2016; Baker-Ericzén, Brookman-Frazee, & Stahmer, 2005; Coonrod & Stone, 2004; Guinchat et al., 2012). The functional ability/disability of the child with ASD are also the key determinants of parental stress and quality of life (Azad, Blacher, & Marcoulides, 2013; Baker-Ericzén et al., 2005; Chiang & Wineman, 2014; Coonrod & Stone, 2004; Estes et al., 2009; Ikeda, Hinckson, & Krageloh, 2014; Tomanik, Harris, & Hawkins, 2004). Given the above, there is a strong rationale to focus on parent/caregiver perceptions of ability and disability in order to examine to what extent ASD may have universal versus differential functional impact in differing socioeconomic and cultural settings. The majority of evidence and research to describe and define ‘functional’ impairment has typically come from professionals who work with children and young people. In a systematic review on ASD and functioning as part of the ICF Core Set for Autism Spectrum Disorder development process, de Schipper and colleagues (2015) identified only 17 out of a total of 71 studies where information was obtained from either parents or peers. All the identified studies in the de Schipper review came from HICs. These findings highlight the lack of knowledge on parent/caregiver perceptions, and, in particular, about parental perceptions from LMICs.
To investigate the difference in perceptions about functioning in LMICs and HICs in ASD, for the purpose of this study, we used Berry, Poortinga, Segall and Dasen’s (2002) ‘universal viewpoint’, which assumes that basic underlying characteristics (and causes) are similar to all individuals with a particular condition, but that these characteristics may be subject to culture and the environment in its development and presentation (Daley, 2002). In light of this ‘universal viewpoint’, the limited literature regarding ASD in LMICs has suggested some similarities with and differences from the HIC literature. Similarities that have been reported were mainly concerned with the basic underlying characteristics of ASD. Some examples include higher prevalence among males, associated genetic disorders such as tuberous sclerosis complex, Rett syndrome and Fragile X, as well as associated comorbidities such as intellectual disability and epilepsy (Newton & Chugani, 2013). A UK-developed parent intervention programme that has been culturally adapted and implemented in Pakistan and India showed similar treatment effects in India/Pakistan as it did in the United Kingdom. Rahman et al. (2016) argued that this suggests some universality as it points to the same developmental processes in ASD within the very different cultural contexts of South-East Asia and the United Kingdom. Differences between high- and low-socioeconomic status (SES) communities relating to ASD include later diagnosis, inadequate referral from primary health care workers, poor access and availability of diagnostic and intervention services and lack of trained health care workers (de Vries, 2016; Franz et al., 2017; Malcolm-Smith, Hoogenhout, Ing, Thomas, & de Vries, 2013) in LMICs.
Overall, the comparative literature between HICs and LMICs has been limited, but most of the differences identified in the literature to date have related to environmental factors. A scoping review conducted in preparation for this study (Viljoen, 2018) identified 33 peer-reviewed articles addressing parent/caregiver perceptions on functioning in ASD. Most of the articles identified in the review were from HICs (25/33), six were from LMICs and two studies compared perceptions from a mix of HICs and LMICs. Functional themes from HICs included a range across the International Classification of Functioning, Disability and Health (ICF) biopsychosocial framework components, with body functions, activities and participation, environmental factors and personal factors all represented, while functional themes from LMICs were more typically focused on environmental and personal factors. Perceptions around environmental factors from LMICs were mostly negative, for example, stigma and lack of resources (Viljoen, 2018).
We therefore set out to do a deliberate comparison of parent/caregiver perceptions from HIC and LMIC settings, using identical interview guides for qualitative data collection.
ICF
The ICF is universally accepted by all 191 WHO member states as a classification and description of functioning, disability and health. The ICF uses a biopsychosocial framework that classifies information into four components, namely, (1) body functions and body structures, (2) activities and participation, (3) environmental factors and (4) personal factors. These factors interact with each other to influence functioning and are classified and described in the ICF manual (WHO, 2007). The ICF defines body structures as the anatomical parts of the body such as organs, limbs and their components. Body functions are defined as the physiological functions of body systems and include psychological functions. Activities and participation are grouped together as one ICF component with nine chapters (see Figure 1). Activities can be described as the execution of tasks or action by an individual, while participation is the involvement in a life situation. Activity limitations are difficulties an individual may have in executing activities, while participation restrictions are problems an individual experiences in their involvement in life situations (WHO, 2007). Environmental factors can be defined as ‘the physical, social and attitudinal environment in which people live and conduct their lives’ (WHO, 2007, p. 9). These factors are external to individuals and can have a positive or negative influence on the individual’s performance as a member of society, or on the individual’s capacity to execute actions or tasks (WHO, 2007). Personal factors are not coded in the ICF given the high cultural variability in these.
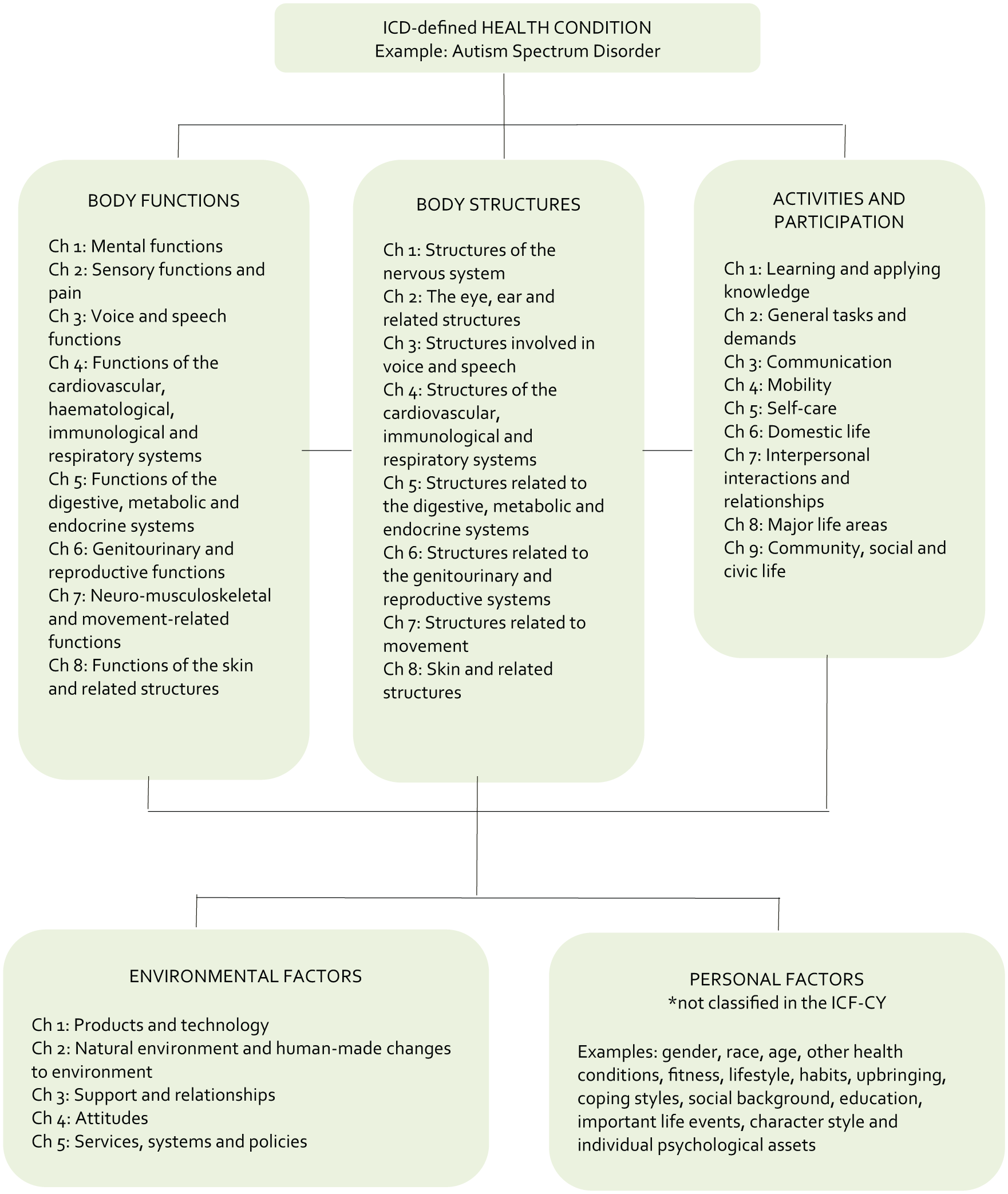
The key components of the ICF and its chapters.
Each of the core components are described in four different levels of depth. As demonstrated in Figure 2, the first level consists of chapters which give an overview of the area of functioning. Chapters are then classified into three hierarchical categories or levels which describe the area of functioning in increasing detail.
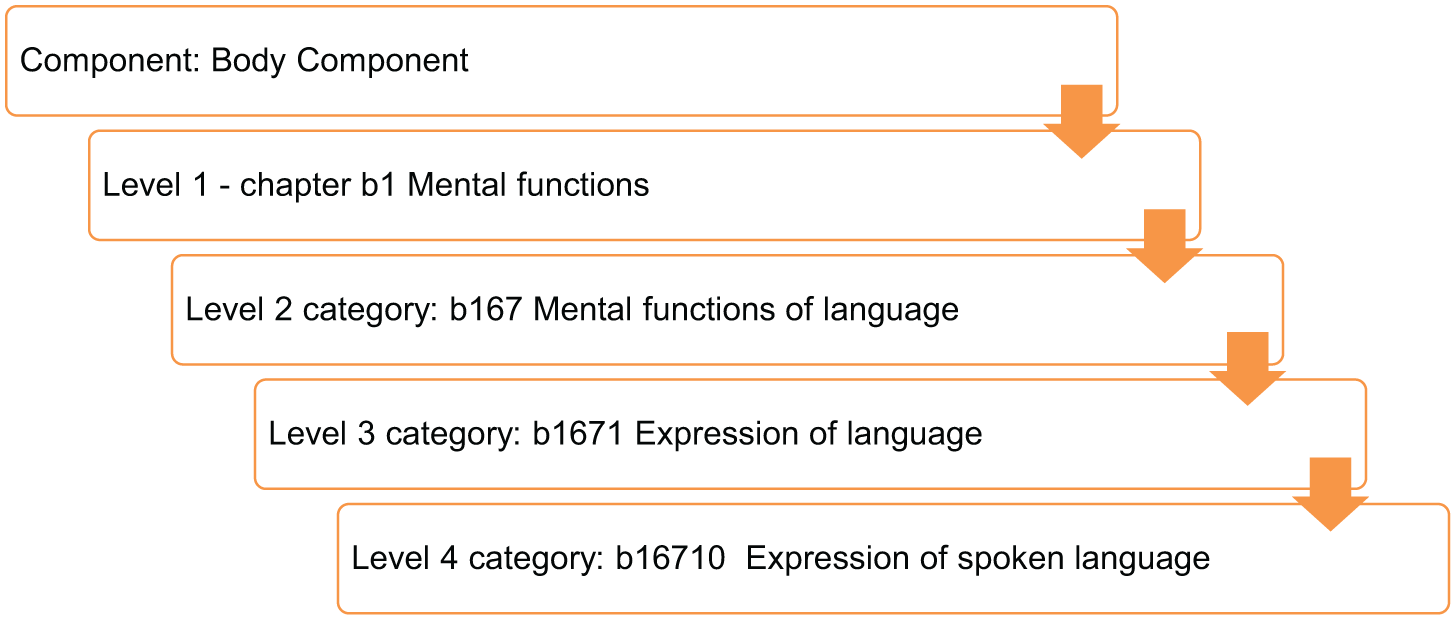
A schematic representation of the ICF process of functioning and disability showing the increase of detail in each level from the most general (component level) to the most detailed (level 4 category).
Recent efforts have been made to develop ICF Core Sets for Autism Spectrum Disorder (Bölte, Mahdi, de Vries, et al., 2018) as well as other childhood-onset disabilities such as attention deficit hyperactivity disorder (ADHD; Bölte, Mahdi, Coghill, et al., 2018) and cerebral palsy (Schiariti, Selb, Cieza, & O’Donnell, 2015). This process included a systematic review of the existing literature, an expert survey and a clinical cross-sectional study (de Schipper et al., 2015, 2016; Mahdi, Albertowski, et al., 2018). Appropriately, the process also had a deliberate step to include parent/caregiver perceptions of functioning (Bölte, Mahdi, de Vries, et al., 2018; Mahdi, Viljoen, et al., 2018), during which focus group discussions and individual interviews were conducted in a range of HICs and LMICs. Focus group and individual interview discussions were facilitated by asking all participants the same questions as specified by the standardized WHO ICF branch Core Set Development Protocol (Bölte, Mahdi, de Vries, et al., 2018).
The overarching aim of this study was to examine the universality of functioning ability and disability in ASD. That is, we were interested to know whether functional themes raised in different contexts would be similar or different. We selected to use the ICF Core Set for Autism Spectrum Disorder development process to determine whether items identified in the qualitative phase of the ICF Core Set for Autism Spectrum Disorder were universally reported across HICs and LMICs, or whether there may have been uniquely different profiles of functional ability and disability associated with different settings.
During the Core Set for the ASD development process, data from the five participating countries (South Africa, Sweden, Saudi Arabia, India and Canada) were pooled. While it was extremely important and valuable that a range of global data were incorporated into the process and decision-making around ICF Core Sets for Autism Spectrum Disorder, we expressed concern that pooling data from across the globe, including African data, may have led to an ‘averaging out’ of the functional consequences of ASD in different regions of the world, particularly given the fact that functioning, ability and disability are highly influenced by context (Mahdi, Viljoen, et al., 2018).
The purpose of this study was therefore to examine the impact of contextual factors on functional ability and/or disability in children with ASD, based on parent/caregiver perceptions of functioning by deliberately comparing and contrasting two of the most divergent countries who participated in the ICF Core Set for Autism Spectrum Disorder development project.
Sweden and South Africa as examples of HIC and LMIC
For this study, we used World Bank income groupings where member states are grouped into LMICs or HICs (The World Bank, 2017c). For the purposes of this study, Sweden was selected as an example of an HIC and South Africa as an example of an LMIC. Sweden and South Africa differ vastly not only in SES, but also in terms of health and education services, systems and policies, as discussed below.
Sweden has an estimated population of 10.16 million (Statistics Sweden, 2018) and a GDP per capita in USD 55,442 (The World Bank, 2017a), hence its HIC classification. A 2011 study found the prevalence of ASD in Sweden to be 0.40%, 1.74% and 2.46% for ages 0–5, 6–12 and 13–17, respectively (Idring et al., 2015). Child and adolescent psychiatry, paediatrics and the habilitation and health centres on the county council side, preschool, schools and social services on the municipality level, as well as federal authorities are obliged to provide a broad array of support to autistic individuals and their relatives. Regional guidelines have been established for the assessment and treatment of ASD (Stockholm County Council, 2010).
For instance, children diagnosed with ASD in Sweden have access to free Early Intensive Behavioural Intervention (EIBI) services until the age of 6 years. These services are provided in collaboration between the county-based habilitation centres’ health care systems and municipality-based education systems. The intensity, duration and content of treatment vary from child to child depending on their needs (Långh, Hammar, Klintwall, & Bölte, 2017). Interestingly, despite the availability of intervention services in Sweden, parents reportedly do not necessarily feel supported and satisfied with the services they receive (Carlsson, Miniscalco, Kadesjo, & Laakso, 2016).
The Swedish school system is regulated through the Education Act (Stockholm Ministry of Education and Research, 2010). The act states that it is compulsory for all children to attend school for 9 years from age 7 to 16. Upper secondary schooling (16–19 years) is not mandatory, but is reportedly attended by most students. Compulsory schooling is free and students also have free access to one preschool year before they commence their compulsory schooling. Preschool for children aged 1–5 years is subsidized depending on the family’s financial situation (Stockholm Ministry of Education and Research, 2010).
The Education Act also states that special support measures should be provided within the existing schooling system embracing inclusion to accommodate learners with special needs. However, there are no clear guidelines in this regard, and the inclusion of children with ASD is far from being accomplished (Bartonek, Borg, Berggren, & Bölte, 2018; Pellicano, Bölte, & Stahmer, 2018). Special schools or ‘särskola’ are available for children with severe intellectual or learning disabilities, but support for learners with difficulties are commonly provided outside the general classroom (Bolic Baric, Hellberg, Kjellberg, & Hemmingsson, 2016). There are a growing number of independent schools in Sweden, of which some are ASD specific.
South Africa has an estimated population of 54.9 million and is classified by The World Bank (2017c) as an upper-middle-income country. The majority of the South African population depends on the public health care system, which has limited physical, financial and human resources (Bloom & McIntyre, 1998; Kon & Lackan, 2008). South Africa also has some of the greatest health disparities of all countries in the world and has a Gini coefficient of 0.65, which is higher than the average (0.45–0.63) for upper-middle-income countries (The World Bank, 2017a).
There are currently very little data on the incidence, prevalence and impact of ASD in Africa in general and in South Africa specifically. No epidemiological data of ASD in South Africa are available (Franz et al., 2017; Van Schalkwyk, Beyer, & de Vries, 2016). In a recent database study, Pillay, Duncan and de Vries (2017) found that ASD was under-identified in South Africa, that there are long waiting lists for ASD schools, and that comorbidities associated with ASD are also highly under-identified.
There are no legal mandates for ASD-specific services in South Africa. Nine schools in the country are specifically set up for learners with ASD, of which four are private and the remaining five government funded. Six of these schools are located in the Western Cape province and the remaining three in Gauteng and Eastern Cape (Van Schalkwyk et al., 2016). Children with ASD may also have access to regular schools with special ASD programmes or special needs schools not specific to learners with ASD. Children under the age of 6 or 7 do not have access to public service early intervention or educational programmes due to the fact that no governmental preschools exist and no early intervention programmes are in place. The capacity to diagnose ASD in the public sector is limited due to the limited number of qualified specialists, and the availability of accurate diagnostic services in the private sector is not clear. Intervention services are also limited and often provided within the non-governmental organization (NGO) sector (Van Schalkwyk et al., 2016).
Table 1 shows a socioeconomic comparison between Sweden and South Africa as reported by the Organization for Economic Co-operation and Development (OECD; 2017).
Comparison of socioeconomic factors in South Africa and Sweden (OECD, 2017).
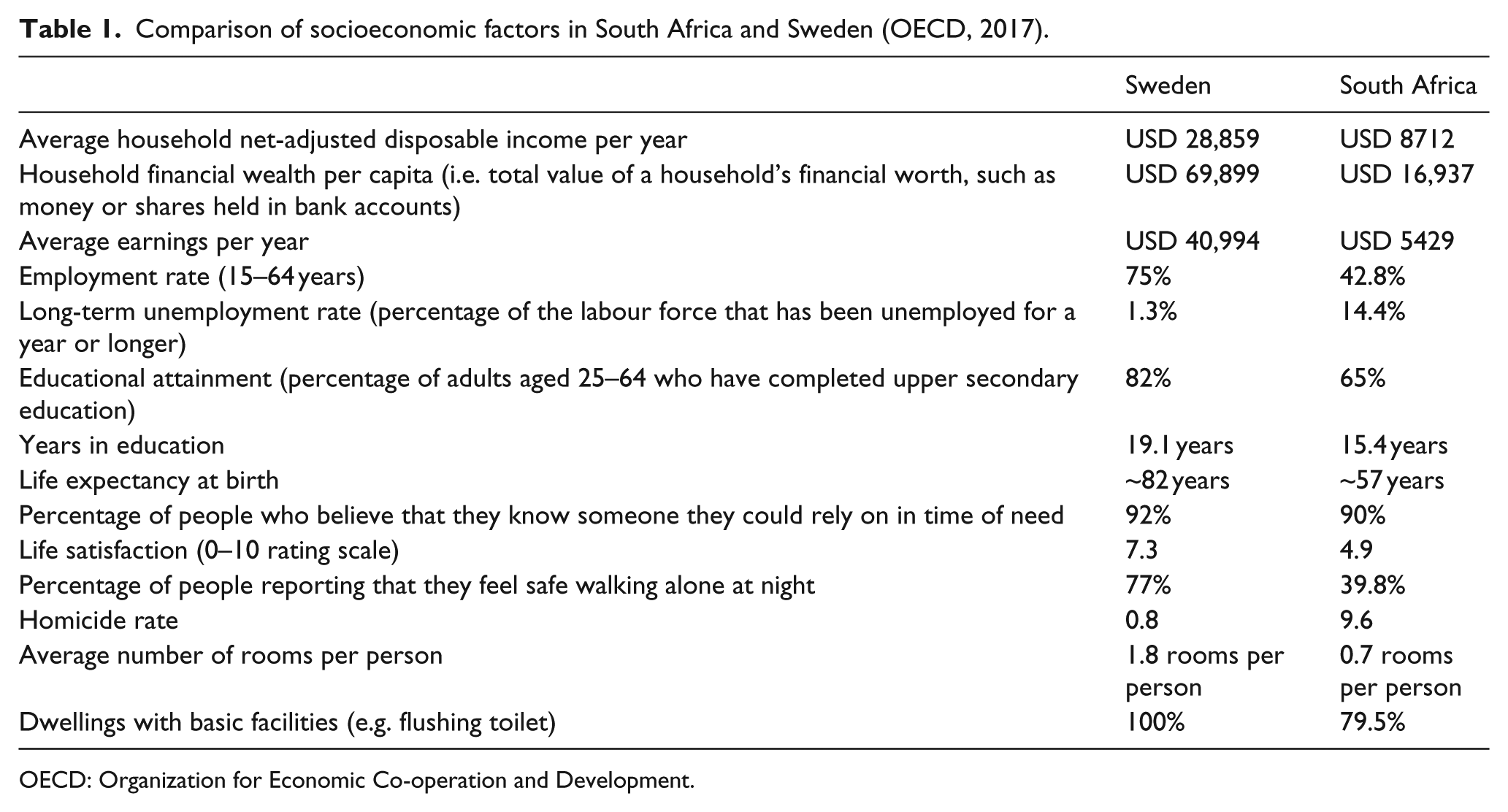
OECD: Organization for Economic Co-operation and Development.
Study rationale and hypotheses
Given the stark socioeconomic differences between Sweden and South Africa, as outlined above, we set out to compare and contrast the functional impact of ASD in the two countries. We were interested in two related but distinct aspects of parent/caregiver perspectives in relation to functioning:
Comparing and contrasting the frequency of functional themes reported by parents/caregivers between Sweden (as HIC) and South Africa (as LMIC);
Comparing and contrasting the content of the functional themes reported by parents/caregivers between an HIC and an LMIC setting.
We hypothesized that:
(a) Body structures and body functions (ICF categories from components 1 and 2) would show similar frequency of reporting by parents in LMIC and HIC settings given that body structures and functions describe the absolute or universal elements of ASD.
(b) Environmental factors (ICF categories from component 4) would be more frequently reported by parents in relation to functional impairment in LMIC settings (as seen in the formative scoping review) than in HIC settings where environmental factors were hypothesized to be more facilitatory to functioning in ASD.
(c) The content of themes from body structures and body functions (ICF categories from components 1 and 2) would be similar in direction (either not impaired or impaired) in LMIC and HIC settings.
(d) The content of themes from environmental factors (ICF categories from component 4) would be different in direction (either facilitator or barrier) in LMIC and HIC settings.
Methods
For the purpose of this study, we performed secondary analysis of data collected during the qualitative phase of the ICF Core Set for Autism Spectrum Disorder development process (Mahdi, Viljoen, et al., 2018). Methodological details are outlined below.
Participants
Inclusion criteria for the original ICF Core Sets for Autism Spectrum Disorder development study were that participants had to be a caregiver, immediate family member or individual involved in the everyday life of someone with a diagnosis of ASD. The original study also involved individuals with a diagnosis of ASD, but, given our interest in parent/carer perspectives, data from this group were not included in this study. For details about the original study recruitment, consent and participants, please see Mahdi, Viljoen, et al. (2018). South African participants were recruited mainly through health professionals and systems who had regular contact with the families. Swedish participants were recruited using a broader range of procedures, including contacting different health care services and ASD interest organizations to disseminate information about our study across different municipalities in Stockholm. Participants were divided into stakeholder groups to ensure a balanced comparison between countries. Participants were therefore divided into four South African and three Swedish Stakeholder groups. For details and rationale for stakeholder grouping, please see Mahdi, Viljoen, et al. (2018).
Procedures
Focus group discussions and individual semi-structured interviews for the original ICF Core Sets for Autism Spectrum Disorder study were conducted following predetermined ICF guidelines. Six questions covering all components of the ICF biopsychosocial model, and one question regarding strengths, guided the discussions. The same interview questions were read in both countries and moderators were instructed to ask follow-up questions to clarify responses. Member checking was also performed by the moderators during the focus groups and individual interviews to ensure that no important information was missing or misinterpreted. The original study (Mahdi, Viljoen, et al., 2018) presented detail regarding focus group and interview procedures as well as a list of the interview questions used in both countries. Moderators in Sweden and South Africa followed the prescribed steps set out in the interview guide during interview and focus group discussions. The interview guide contained the study questions, instructions for when to ask follow-up questions, instructions for ensuring that everyone in the focus group are actively participating in the discussion and specific rules regarding focus group conductance. The authors led all focus group and individual interviews in South Africa and Sweden.
Focus group discussions and individual interviews were recorded, translated and transcribed following ICF guidelines as described in the original study manuscript (Mahdi, Viljoen, et al., 2018). Meaningful concepts were extracted from the transcripts using deductive qualitative content analysis (Krippendorff, 2013) and linked to ICF categories following ICF linking rules (Cieza et al., 2002, 2005; Mahdi, Viljoen, et al., 2018). Two independent coders, one from South Africa and one from Sweden, did coding and linking of all the South African focus group data. Previously coded Swedish data (for analysis for this study) and anonymous Swedish transcripts (for qualitative analysis) were provided to the South African team via a safe electronic platform, once all ethical approvals were in place.
Ethics
Ethical approval for the original study was granted by the Regional Ethics Committee Stockholm (reference number 2014/53-31/2) and by the University of Cape Town Human Research Ethics Committee (HREC reference 506/2015). In addition, permission was granted by Red Cross War Memorial Children’s Hospital for local data collection and by Dr David Griessel, who led recruitment of participants from the second recruitment site in South Africa. We received written permission from the lead team at the Karolinska Institutet to use anonymized Swedish and global data for this study. This study was conducted in conformity with the ethical principles of the Declaration of Helsinki.
Data analysis
Data analysis phase 1: frequency analysis
For frequency analysis, we identified, ranked and compared similarities and differences in frequency of reporting from the coded South African and Swedish data (see Figure 3). Second-level ICF categories were used to ensure that this study was comparable to the overall ASD ICF qualitative study (Mahdi, Viljoen, et al., 2018).
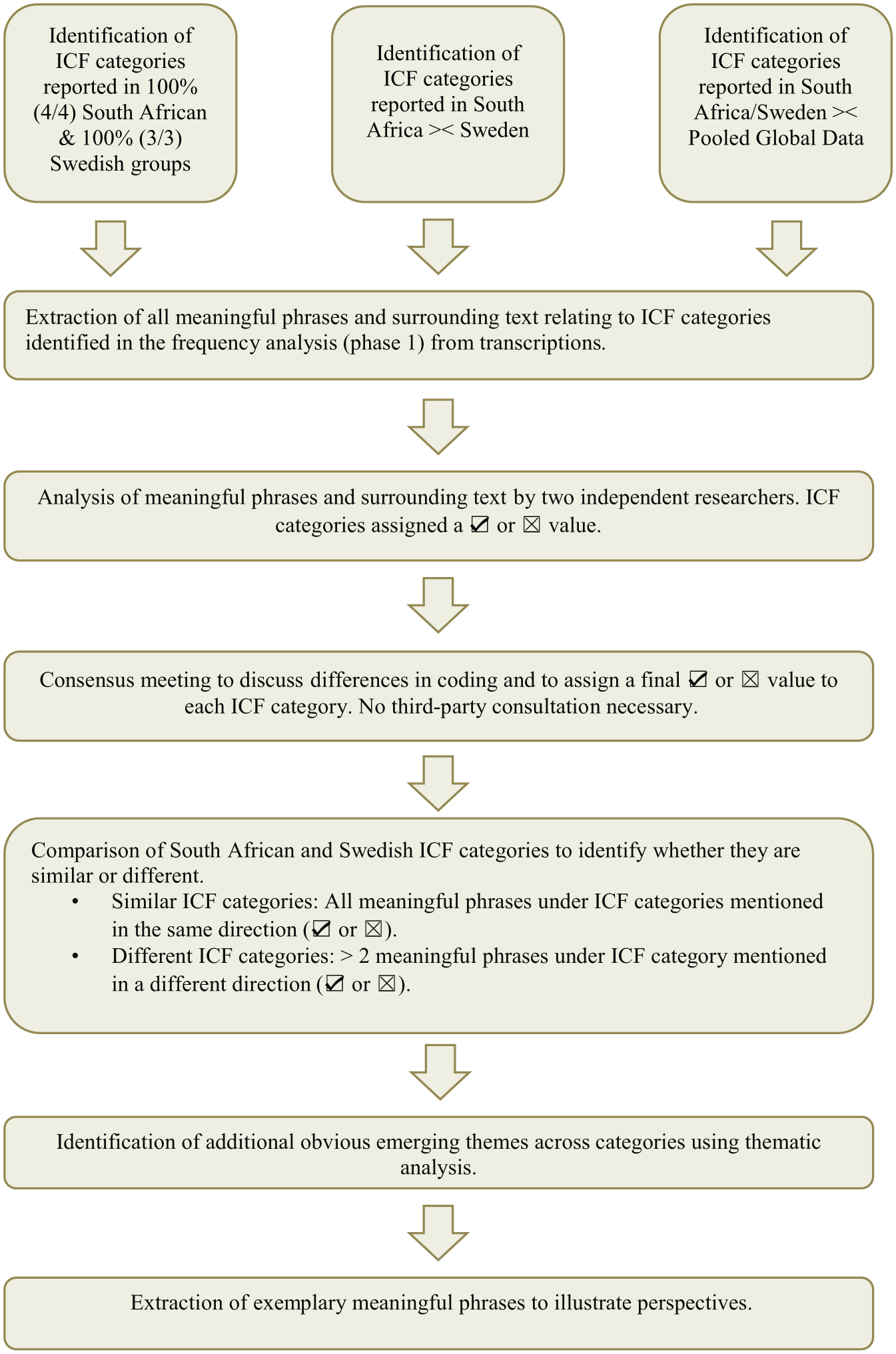
A schematic representation of steps followed in data analysis phase 1 (frequency analysis) and phase 2 (content analysis).
After identifying similarities and differences in frequency of reporting, South African and Swedish data were compared to the ‘pooled global dataset’, referring to data from all the participating countries (Canada, India, Saudi Arabia, South Africa and Sweden). The following steps were followed during the frequency analysis:
South Africa = Sweden: Identification of ICF categories reported in 100% (four of four) South African as well as 100% (three of three) Swedish groups.
South Africa >< Sweden: Identification of ICF categories with obvious differences in frequency of reporting between South Africa and Sweden. ‘Obvious Differences’ were operationalized to include categories that were present in three out of three Swedish groups and zero or one South African group, or in two out of three Swedish groups but zero South African groups. For South African data, it included categories that were present in four of four South African groups and zero or one Swedish group, as well as three of four South African groups and zero Swedish groups.
South Africa/Sweden >< Pooled Global Data: Identification of ICF categories where South African and/or Swedish data were different to pooled global data. To do this, we identified categories that were reported in 100% of groups from other countries, but in 50% (2/4) or less of South African groups or in 33% (1/3) or less of Swedish groups. We also identified categories that were reported only in South Africa and/or Sweden, but not in any group from any other country.
Data analysis phase 2: content analysis
The content of all ICF second-level categories identified in the deductive frequency analysis (phase 1) was analysed to determine if they were mentioned as a facilitator or barrier to functioning.
The process for content analysis is described below and summarised in Figure 3:
All meaningful phrases relating to all the ICF categories identified in the frequency analysis (see above) were extracted from the original South African and Swedish transcriptions. Text surrounding the meaningful concepts that might have enabled the researchers to better understand the context in which the meaningful phrase was mentioned was also extracted.
Meaningful phrases and surrounding text in Swedish were translated to English by the Swedish research team at the Karolinska Institute. Swedish and South African meaningful phrases and surrounding text were independently analysed by two researchers (S.M. and M.V.). Researchers read through transcripts and assigned a value describing the nature in which each meaningful phrase was mentioned in the data. The surrounding text was considered during this process. Where a meaningful phrase was mentioned as a factor that supports or improves the individual with ASD’s functioning, it was assigned a positive value (☑). For a meaningful phrase to be rated as a facilitator or not impaired, it had to have been described by parents/caregivers as unambiguously improving/supporting functioning in the individual with ASD. Where a meaningful phrase described a factor that lowered or had a limiting impact on functioning, it was defined as a barrier or impaired and assigned a negative value (☒). For a meaningful phrase to be rated a barrier/impaired, it had to have been described by parents/caregivers as unambiguously limiting/reducing functioning in the individual with ASD. Where the meaning of a phrase was unclear or where there was uncertainty whether it was positive or negative, a rating of ‘9’ (unable to code) was given. After both researchers independently coded all the meaningful phrases, they met to discuss differences in their coding and reach consensus. It was not necessary to consult a third party to reach consensus.
Once meaningful phrases were coded as barriers/impaired or facilitators/not impaired, the phrases for each ICF category were compared between South Africa and Sweden. ICF categories were defined as similar when all the meaningful phrases coded under that specific ICF category were mentioned in the same direction (facilitator/not impaired or barrier/impaired). ICF categories were defined as different when more than two meaningful phrases coded under the specific ICF category were mentioned in a different direction.
Additional obvious emerging themes across categories were identified using thematic analysis.
Finally, exemplary meaningful phrases were extracted to illustrate perspectives.
Results
Demographic results
The overall study included 11 stakeholder groups (61 participants) from five countries (India, South Africa, Saudi Arabia, Canada and Sweden). Four stakeholder groups were from South Africa (22 participants), three from Sweden (13 participants), two from India (11 participants), one from Saudi Arabia (6 participants) and one from Canada (9 participants).
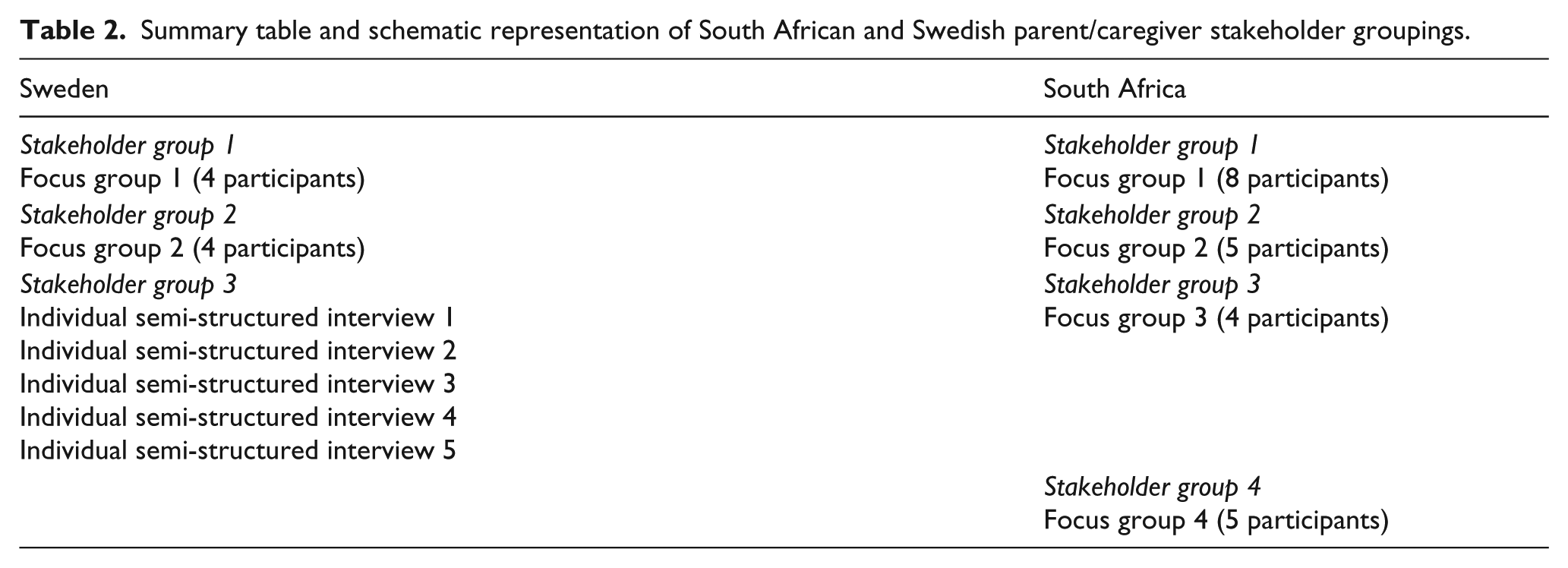
As per Mahdi, Viljoen, et al. (2018), participants were divided in stakeholder groups to avoid favouring the responses of interviewed participants. An ICF code mentioned more than once in a stakeholder group was therefore counted as ‘one’ in the frequency analysis. The three Swedish and four South African stakeholder groups represented 13 Swedish and 22 South African parent/caregivers, respectively. The composition of these is outlined in Table 2. The mean age of South African participants was 40 years. South African participants consisted of 72.7% (16 of 22) female participants and 27.3% (6 of 22) male participants. All participants were caregivers of children between the ages of 3 and 18 years. The mean age of Swedish participants was 48 years. Swedish participants were also mostly female (84.6%, 11 of 13).
Summary table and schematic representation of South African and Swedish parent/caregiver stakeholder groupings.
Frequency of ICF categories reported in Sweden and South Africa
Categories present in 100% of South African and Swedish groups
Four ICF categories were identified that were reported in 100% (four of four) South African as well as 100% (three of three) Swedish groups. These included three categories under activities and participation, namely, carrying out daily routine (d230), dressing (d540) and complex interpersonal interactions (d720), and one category from environmental factors, namely, immediate family (e310). All of the categories, apart from dressing, were also present in all stakeholder groups in the pooled global data. That is, 100% of the groups that were part of the global study mentioned these three categories. Results are summarized in Table 3.
Summary table showing the results of the frequency analysis.
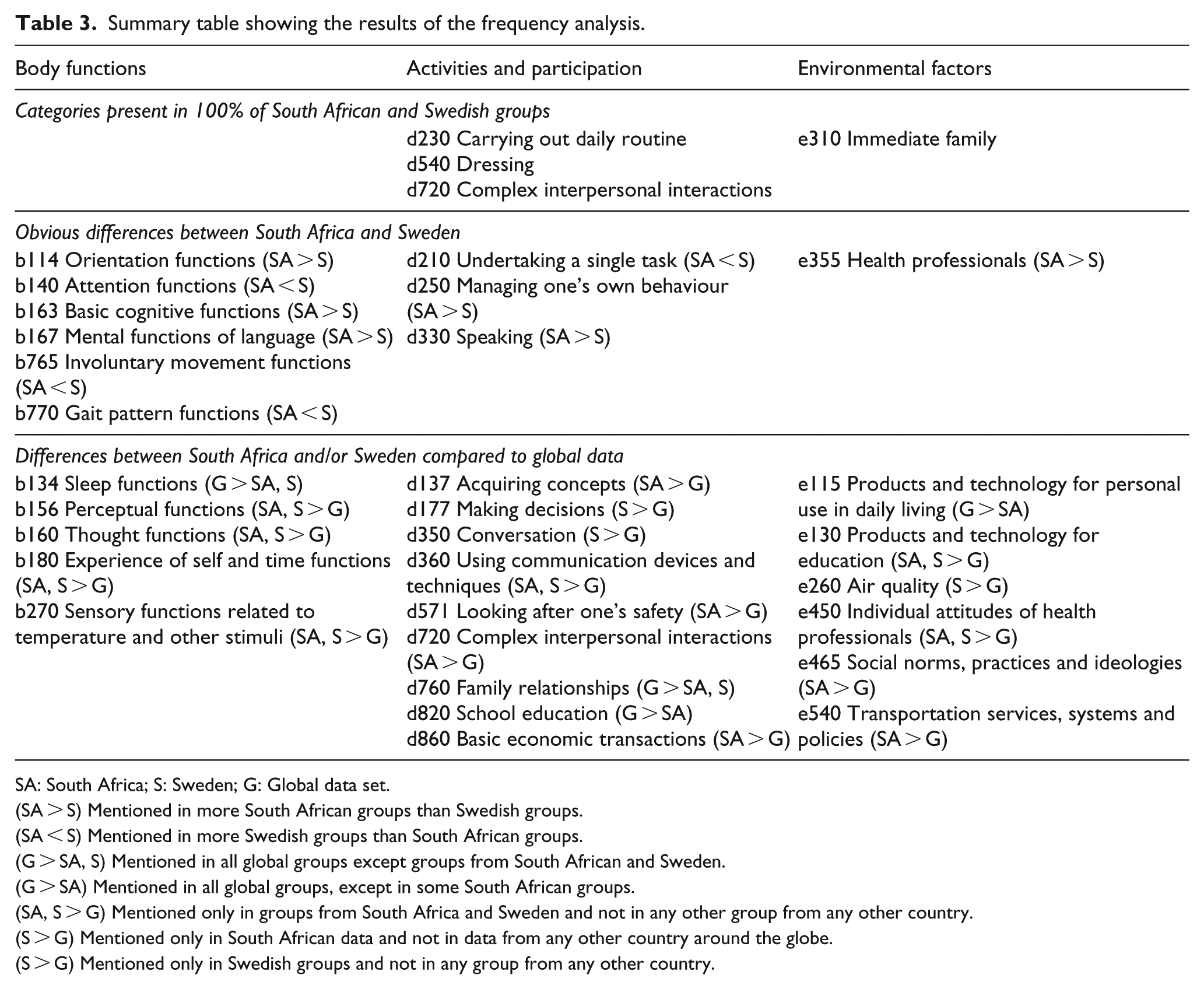
SA: South Africa; S: Sweden; G: Global data set.
(SA > S) Mentioned in more South African groups than Swedish groups.
(SA < S) Mentioned in more Swedish groups than South African groups.
(G > SA, S) Mentioned in all global groups except groups from South African and Sweden.
(G > SA) Mentioned in all global groups, except in some South African groups.
(SA, S > G) Mentioned only in groups from South Africa and Sweden and not in any other group from any other country.
(S > G) Mentioned only in South African data and not in data from any other country around the globe.
(S > G) Mentioned only in Swedish groups and not in any group from any other country.
Obvious differences between South Africa and Sweden
In total, 10 ICF categories with obvious differences in frequency of reporting between South Africa and Sweden were identified. A total of six categories were identified under body functions, three under activities and participation, and one under environmental factors. Obvious differences between South Africa and Sweden are shown in Figure 4. Categories mentioned in more South African than Swedish groups included orientation functions (b114), basic cognitive functions (b163), mental functions of language (b167), managing one’s own behaviour (d250), speaking (d330) and health professionals (e355). Categories mentioned in more Swedish than South African groups included attention functions (b140), involuntary movement functions (b765), gait pattern functions (b770) and undertaking a single task (d210). Results are summarized in Table 3.
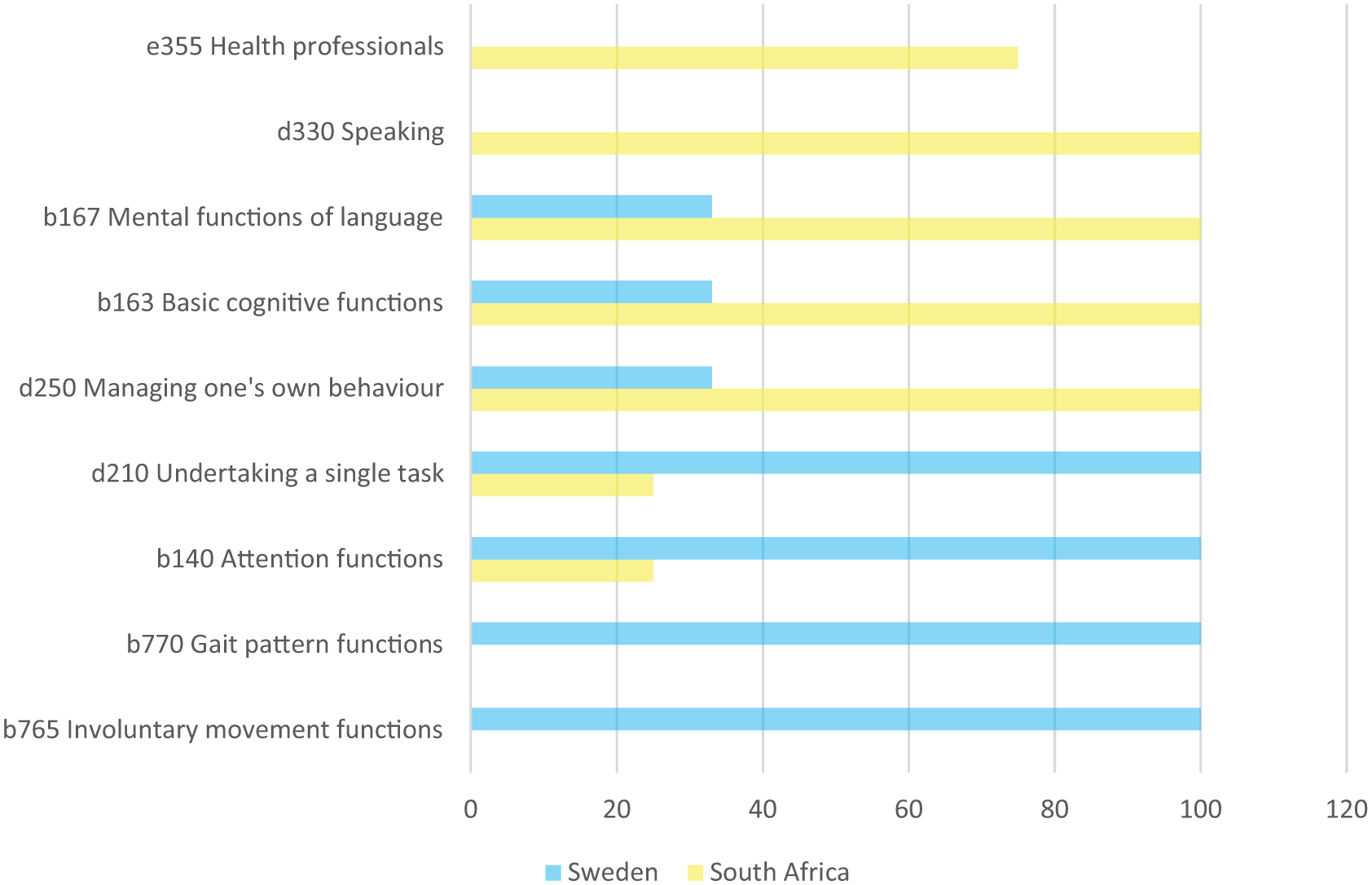
Obvious differences in frequency of reporting between South Africa and Sweden.
Differences between South Africa and/or Sweden compared to global data
In total, 20 categories were identified where South African and/or Swedish data were very different to pooled global data. These categories are shown in Figure 5. Five categories were identified under body functions, nine under activities and participation, and six under environmental factors.
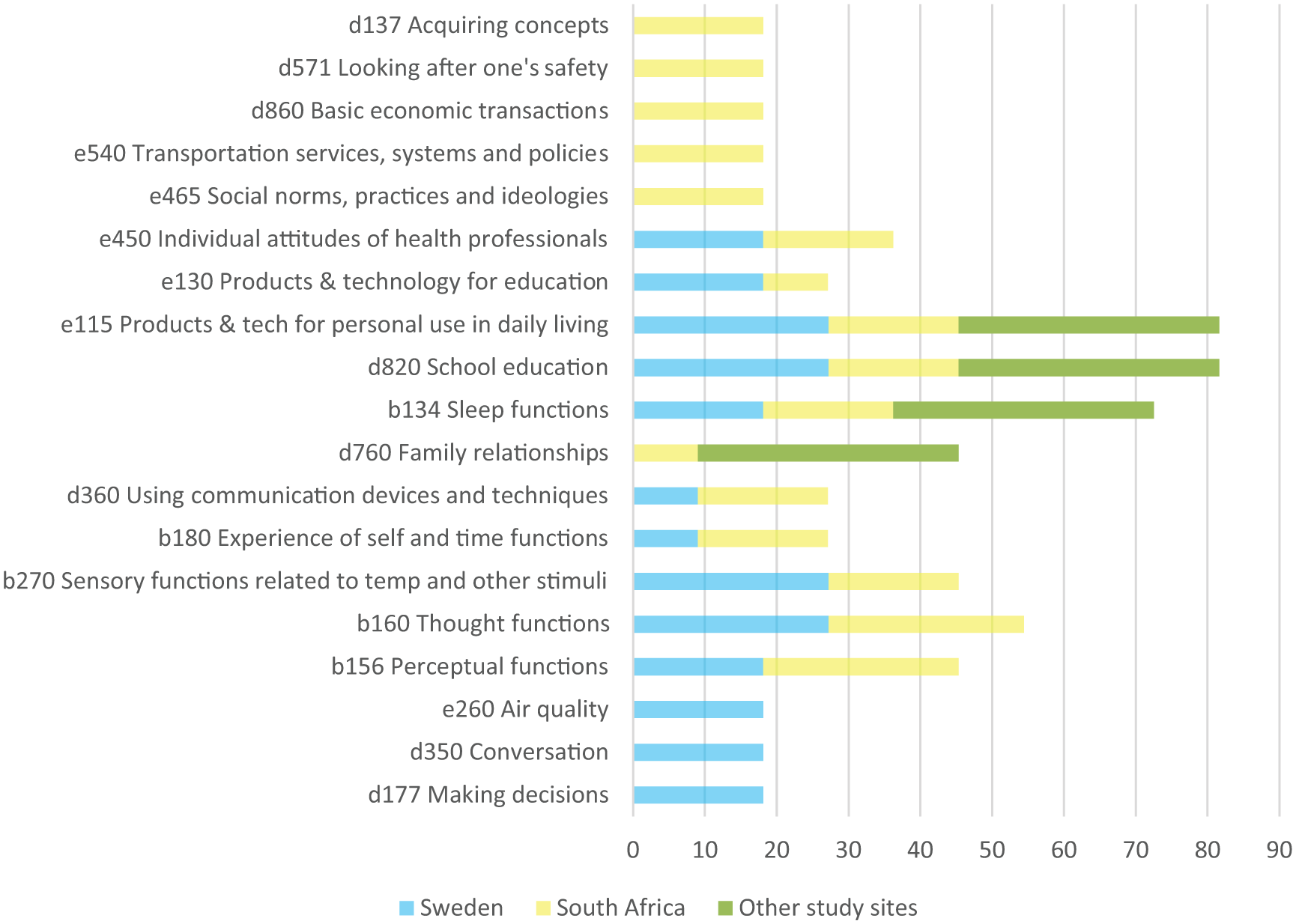
Differences in frequency of reporting between South African and/or Sweden and pooled global data.
Categories mentioned in all global groups except South Africa and Sweden were sleep functions (b134) and family relationships (d760). Categories mentioned in all global groups, except in some South African groups, were school education (d820) and products and technology for personal use in daily living (e115).
Categories mentioned only in groups from South Africa and Sweden but not in any other countries were perceptual functions (b156), thought functions (b160), experience of self and time functions (b180), sensory functions related to temperature and other stimuli (b270), using communication devices and techniques (d360), products and technology for education (e130) and individual attitudes of health professionals (e450).
Categories mentioned only in South African data and not in data from any other country were acquiring concepts (d137), looking after one’s safety (d571), basic economic transactions (d860), social norms, practices and ideologies (e465) and transportation services, systems and policies (e540). Categories mentioned only in Swedish groups and not in any group from any other country were making decisions (d177), conversation (d350) and air quality (e260). Results are summarized in Table 3.
Content of ICF categories reported in Sweden and South Africa
Only three categories differed qualitatively between South Africa and Sweden. One category emerged from the 100% agreement group (e310 Immediate family), one from the obvious differences between the South African and Sweden groups (b140 Attention functions) and one from differences between South Africa and/or Sweden and pooled global data (e115 Products and technology for personal use in daily living).
Two of the three categories were environmental factors (e115 Products and technology for personal use in daily living and e310 Immediate family) and one represented body functions (b140 Attention functions). Differences in these categories are described below and exemplary meaningful phrases to illustrate differences are given.
Immediate family
Swedish participants mentioned ‘immediate family’ 21 times, all of which was as a facilitator, whereas South African participants mentioned it 52 times as a facilitator and eight times as a barrier to functioning. Barriers mentioned by South African participants included fathers’ negative attitude and/or lack of understanding towards/of their child with ASD, parents not disciplining their children appropriately, thus reinforcing challenging behaviour, and lack of support from siblings. Table 4 shows exemplary phrases to illustrate these perspectives.
Summary of meaningful phrases referring to e310 Immediate family.
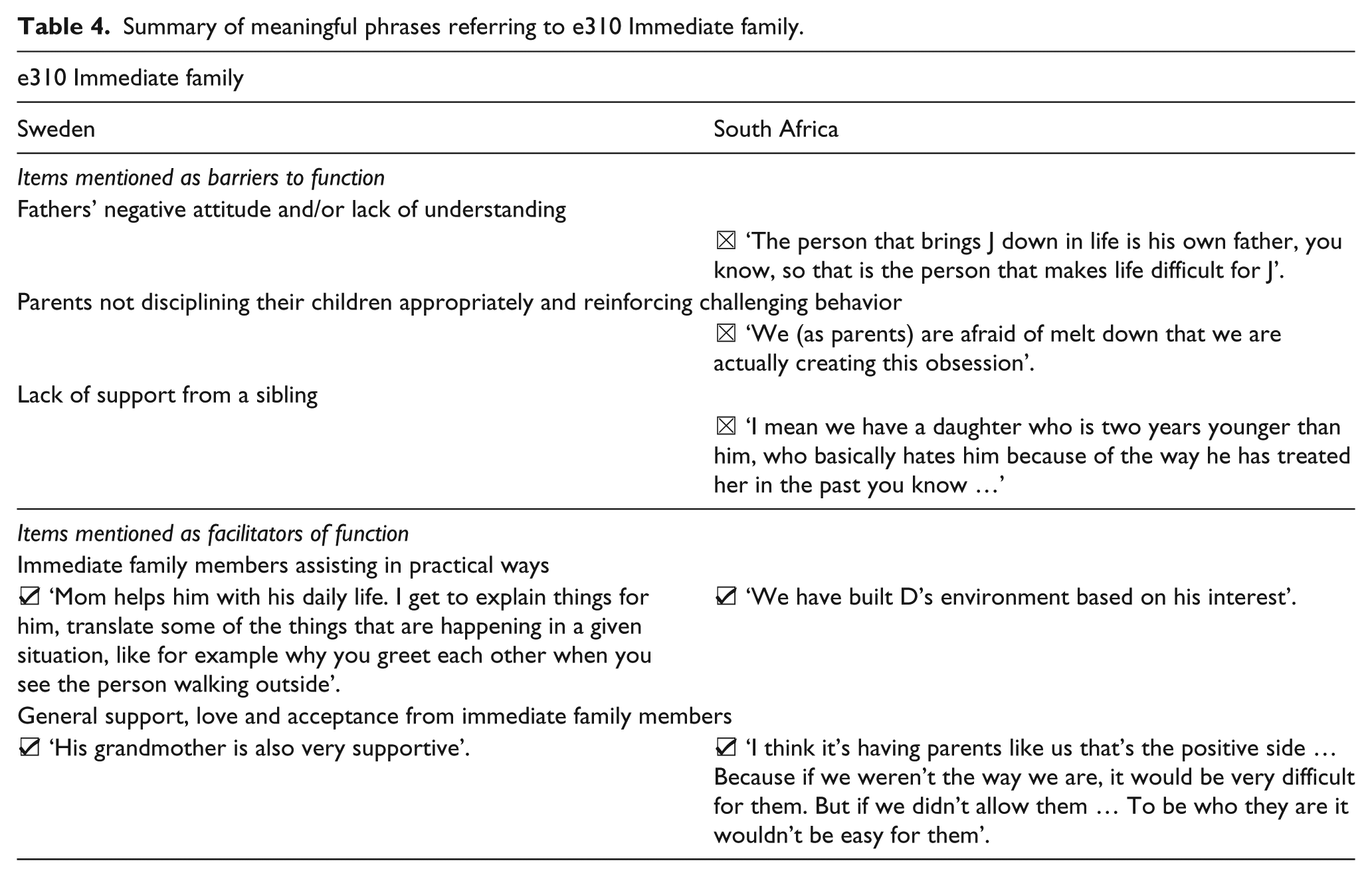
Although ‘Immediate family’ was identified as a category with qualitative differences between South Africa and Sweden, it also contained qualitative similarities in how immediate family members facilitate functioning in their children/family members with ASD. These similarities between South African and Swedish data include parents and other immediate family members (such as grandparents and siblings) helping in practical ways. These practical ways include giving medication, adapting the environment to the person with ASD’s needs, helping them avoid challenging environments/situations, communicating for them when they are unable to, assisting in developing healthy lifestyle habits such as eating, helping them understand communication and/or others’ reactions, home schooling, implementing therapy programmes, helping them understand concepts, helping them manage stress, emotional support and assisting with time management. These practical strategies were often linked by participants to them understanding their child/family member with ASD. Support, love and acceptance of parents, grandparents and siblings were also mentioned in a general, non-specific way. See Table 4 for exemplary meaningful phrases.
Attention functions
‘Attention functions’ were mentioned six times as not impaired in Sweden and three times as impaired in South Africa. Swedish participants mentioned the ability to concentrate/focus for an extended period of time as a positive, where South African participants commented that individuals with ASD are not able to concentrate/focus as expected. Table 5 provides meaningful phrases illustrating viewpoints from both countries.
Summary of meaningful phrases referring to b140 Attention functions.

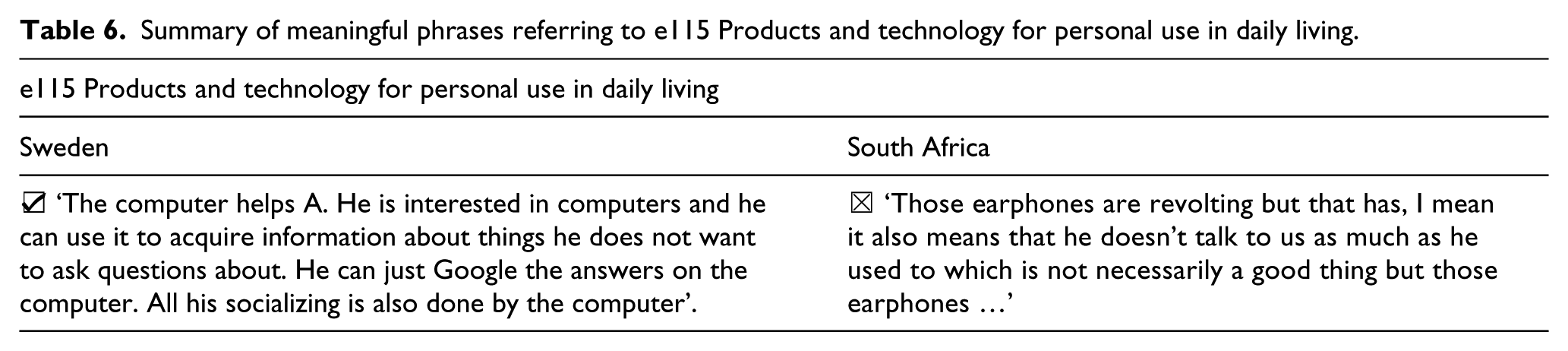
Products and technology for personal use in daily living
South African participants mentioned ‘products and technology for personal use in daily living’ a total of four times, all of which was as a barrier, whereas Swedish participants mentioned it 14 times as a facilitator and only four times as a barrier.
In both South Africa and Sweden, participants identified several barriers in relation to products and technology for personal use. These included earphones limiting communication, restricted behaviours and/or difficulty dealing with change relating to toys and sensory sensitivity such as sensitivity to certain types of clothing or lights.
Swedish participants mentioned several facilitators in relation to products and technology for personal use. These included computers and iPads helping with communication, socializing and translation of words/language, timers and schedules assisting with daily routine, travel apps helping with travel-related issues and board games facilitating socialization. Exemplary meaningful phrases are illustrated in Table 6.
Summary of meaningful phrases referring to e115 Products and technology for personal use in daily living.
Additional themes identified through content analysis
Two additional themes emerged from the data using thematic analysis. The two themes will be discussed below.
Health professionals
ICF categories e355 ‘Health professionals’ and e450 ‘Individual attitudes of health professionals’ both describe participants’ perspectives on health care professionals. Although neither category on its own indicated significant qualitative differences, they did differ qualitatively when grouped together.
South African participants mentioned health professionals and individual attitudes of health professionals mostly as a facilitator, whereas Swedish participants only mentioned it as a barrier.
South African participants mentioned that health professionals understand or make an effort to understand ASD and are helpful. One South African participant mentioned that doctors and nurses do not understand what ASD is. All Swedish meaningful phrases referring to health professionals mentioned lack of understanding. See Table 7 for a summary of meaningful phrases referring to health professionals.
Summary of meaningful phrases referring to health professionals.

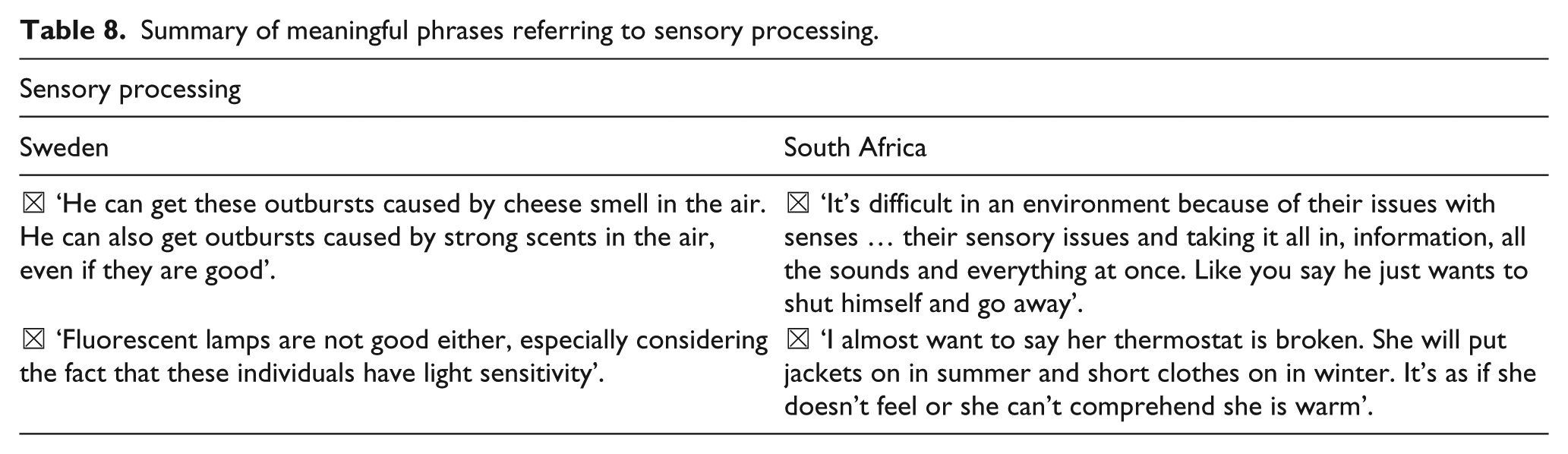
Sensory processing
Several meaningful concepts over many different categories referred to sensory sensitivity or low registration of sensory information (not noticing sensory information others would). Sensory processing was mentioned only as a barrier to function by participants from both Sweden and South Africa. See Table 8 for a summary of meaningful phrases referring to sensory processing.
Summary of meaningful phrases referring to sensory processing.
Discussion
The purpose of this study was to examine the impact of context on functional ability and disability in children with ASD. We focused on parent/caregiver perceptions of functioning by deliberately comparing and contrasting an HIC and an LMIC who participated in the ICF Core Sets for Autism Spectrum Disorder development project (Mahdi, Viljoen, et al., 2018). We aimed to identify and compare the frequency of the most commonly reported functional ICF items identified in the preparatory Core Sets for ASD study in South Africa and Sweden and then to examine and compare the content of these categories. Based on Berry et al.’s universal viewpoint, we predicted that ICF categories from body functions and body structures would be similar in frequency of reporting, but that environmental barriers would be reported more in South Africa than in Sweden, as suggested in the formative literature.
We predicted that body structures and body functions would not show differences between HICs and LMICs, given the absolute or universal nature of ASD. However, obvious differences in frequency of reporting between South Africa and Sweden were observed in 6 out of 10 categories relating to body function. No meaningful concept relating to body structures was identified. ICF body functions include categories describing the core characteristics of ASD and we therefore did not expect to see so many of these items in the ‘obvious differences in frequency of reporting’ category. We can reason that some of these core characteristics of ASD were either present in more participants from one country than the other or they were considered more relevant and subsequently reported more in one setting than the other. Given that this study did not measure actual functioning or symptom manifestation, we are not able to say which of these two options are more accurate, or whether a combination is perhaps the most relevant. Some of the categories such as ‘mental functions of language’, ‘speaking’ and/or ‘involuntary movement functions’ relate directly to the diagnostic criteria of ASD and it can therefore be speculated that they were also present, but not mentioned in most of the individuals with ASD from the other country. The fact that they were not mentioned in both countries could be due to contextual and/or cultural factors, but might also have to do with the way in which participants answered questions and the items were subsequently coded.
Categories that were present in all South African and Swedish groups were mostly from activities and participation (three categories). This result supports previous studies (Azad & Mandell, 2016; Baker-Ericzén et al., 2005; Coonrod & Stone, 2004; Guinchat et al., 2012) suggesting that the functional impact of ASD in activities of daily living are more relevant to families than body functions and often the motivating factor for seeking help. This could be true for other childhood-onset disabilities too, as illustrated by Schiariti and Mâsse (2014) who found that caregivers were mostly concerned with activities and participation and environmental factors in a study using the four preparatory phases of the ICF-CY Core Set development process for children/youth with cerebral palsy to compare perspectives from researchers, clinicians and caregivers.
Our prediction was that environmental factors would be more frequently raised as a concern in LMIC settings due to contextual limitations. Interestingly, only one environmental factor (health professionals) was identified as different in frequency of reporting. Health professionals were mentioned only in South Africa and not Sweden, and were mentioned as a facilitator rather than a barrier to functioning by South African participants, in contrast to our expectation. This observation suggests that South African participants did not mention environmental factors more than Swedish participants, and that environmental factors can therefore not be assumed to be more relevant/important in an LMIC versus an HIC setting, as suggested in the existing literature. Results from this study showed that parent/caregivers from an LMIC such as South Africa did not raise environmental factors to a greater extent in relation to their child’s functioning compared to parent/caregivers from Sweden.
When comparing South Africa and Swedish data to global pooled data, several categories were mentioned only in South Africa and nowhere else in the world. Others were mentioned only in Sweden and nowhere else, and a few were mentioned in both Sweden and South Africa but nowhere else. At first glance, several of the categories mentioned only in South Africa such as ‘transportation services and systems’, ‘social norms, practices and ideologies’ and ‘looking after one’s safety’ seemed to be specific to the South African context, but when exploring the content, it was found that only ‘social norms, practices and ideologies’ reflected cultural aspects unique to South Africa, such as ancestral worship. The other categories were mentioned relating to the person with ASD’s restricted and repetitive behaviours or inability to judge situations accurately and did not make any direct mention of South African-specific contextual factors such as crime or lack of services. These comments suggest that the way in which family members of participants interact with the environment, rather than the environment or context itself, may be relevant to parent/caregivers.
Similarly, apart from ‘air quality’, categories unique to Sweden were also not obviously specific to the environment (‘conversation’ and ‘making decisions’). When exploring the content of comments under air quality, it was found that all participants spoke about sensitivity to an aspect of the environment not perceived by most such as a certain smell. It was thought that these comments could also be classified under the heading of sensory processing (not included in the ICF) and was therefore identified as one of the additional themes discussed below.
We also predicted that the content of the themes from body functions would be similar in direction (either impaired or not impaired), but that the content of themes from environmental factors would be different in direction (either facilitator or barrier) in LMIC and HIC settings. Out of the 34 categories identified as part of the frequency analysis, only 3 were qualitatively different with one additional difference that could be identified when 2 categories were combined (‘health professionals’ and ‘attitudes of health professionals’). The content of identified categories was more similar than we anticipated between these two very different countries. Differences in content were mostly relating to environmental factors, but these differences were often not in the direction we expected. For example, ‘immediate family’ was mentioned as a facilitator and a barrier by South African participants and only as a facilitator by Swedish participants. Another example is ‘health professionals’, reported by most groups in South Africa as a facilitator to functioning, but Swedish groups mentioned ‘attitudes of health professionals’ as a barrier to function. We know that health services and systems are more advanced and better implemented in Sweden than in South Africa (Långh et al., 2017; Stockholm County Council, 2010; Van Schalkwyk et al., 2016), but it seems, at least based on the data from this study, that South Africans were more satisfied with the limited resources they have access to. In a study examining expectations and responsiveness within health care systems, Busse and colleagues (WHO, 2013) described that patients with different expectations rated similar experiences differently. It might therefore be that South African participants had lower expectations with regard to availability and access to health professionals and were therefore more satisfied with the services they received, even if these services were limited. Lower expectations can also be influenced by lack of knowledge regarding the role of the environment and its impact on functioning. The difference in recruitment methods between Sweden and South Africa might also have influenced the perspectives given by participants which would have impacted results from both the frequency and content analyses. For example, all South African participants were receiving or had previously received some sort of intervention from health care systems since this was the means through which they were recruited. Since Swedish participants were recruited via a broader range of methods, it is possible that not all Swedish participants had the same level of contact with health care systems and professionals as South African participants had. This could have influenced participants’ viewpoints on health professionals specifically, but also on other aspects of functioning. We therefore conclude that some environmental factors may be different between cultures, but that these differences are complex and should not be assumed.
Some of the other categories that differed qualitatively such as ‘products and technology for personal use in daily living’ were not surprising given that the category reflected the fact that Sweden is more advanced technologically than South Africa. It should be noted that these results pertain to environmental factors as operationalized by the ICF. It is therefore possible that some environmental factors were coded as ND (not definable) or NC (concept not covered by the ICF). Concepts coded as NC or ND would not have been captured under this result, but might contain valuable information about parent/caregiver perceptions. These codes could be further analysed to identify recurring themes (Finger, De Bie, Selb, & Escorpizo, 2016).
Additional themes identified included ‘health professionals’ as discussed above and ‘sensory processing’. Sensory processing refers to the neurological process through which sensory input is interpreted and organized to action a motor or behavioural output (Ayres, 1971, 1972). Individuals with atypical sensory processing are either more or less sensitive to sensory stimuli than their peers and have difficulty regulating their level of alertness (sensory modulation). It has been reported that individuals with ASD respond differently to sensory stimuli than their typically developing peers (Cesaroni & Garber, 1991; Ermer & Dunn, 1998; Kientz & Dunn, 1997; Ornitz, Lane, Sugiyama, & de Traversay, 1993; Tomchek & Dunn, 2007; Watling, Deitz, & White, 2001; Yeung-Courchesne & Courchesne, 1997). Several other comments coded under a broad range of other categories described difficulties with sensory processing or regulation. There is however not one ICF category that clearly describes sensory processing which resulted in these comments being coded under either of the environmental factor, activity or body functions they relate to. When reading through data, it was clear that these comments referred to an additional aspect of functioning not captured in the ICF manual.
Results from this study support the usefulness of ICF Core Sets for Autism Spectrum Disorder for providing a common language for parents/caregivers, professionals and researchers to facilitate greater collaboration when planning and implementing interventions. ICF Core Sets for Autism Spectrum Disorder can also provide the framework for the development of new services or the adaptation interventions to new settings.
One of the challenges faced in low-resource settings is the lack of financial and human resources hindering the delivery of evidence-based interventions to children with ASD. Involving and coaching parents/caregivers in treatment delivery offers a possible and effective solution to this challenge (Divan et al., 2015; Guler et al., 2018; Kasari et al., 2014; Rahman et al., 2016; Reichow, Servili, Yasamy, Barbui, & Saxena, 2013). Since results from this study suggest that many similarities are present in parent/caregiver perceptions of functioning in different settings, we can conclude that priority parent intervention targets might therefore share similarities in different settings and among different population groups. We therefore suggest that parent/caregiver-focused interventions developed in western HIC settings will be relevant to populations in LMICs, provided that it is adapted and implemented with the local context in mind (Daley et al., 2013).
Limitations
We acknowledge a number of limitations of this study. First, the number of participants was relatively small. However, qualitative research typically places a stronger emphasis on data saturation than sample size (Malterud, Siersma, & Guassora, 2015). While we recognize this as a limitation and recommend that more studies of this type with larger samples be done, we also recognize that this is the first study, to our knowledge, where perceptions of functioning were compared in this manner. Second, even though South Africa has 11 official languages, all South African focus groups were conducted in English. We therefore acknowledge that the use of a second language may have influenced participants’ ability to express their thoughts clearly. Although it was not possible to conduct the focus groups in all official languages due to limited resources, all group facilitators were proficient in one more language in addition to English. Third, we observed some differences in response styles between South African and Swedish participants. South African participants were more descriptive, but less direct when answering questions, while Swedish participants gave shorter, more direct answers. It is possible that this was due to the language limitation described above, and that it may have impacted on the way in which a category was coded. However, we used both a South African and a Swedish coder for data extraction, which reduced the likelihood that response styles may have biased the data analysis. We also acknowledge that the developmental level or severity of ASD of the individuals was not known. It is possible that their developmental level and severity of ASD could have affected the abilities and disabilities reported by parents/caregivers. Guidelines for the qualitative study did, however, not include prior documentation of developmental level or severity of ASD symptoms and this aspect was considered in the clinical cross-sectional study (Mahdi, Albertowski, et al., 2018). While we tried to include a representative sample of the population in both Sweden and South Africa, we acknowledge that the SES of our participants was not known. Socioeconomic factors can have a significant impact on participants’ experience of environmental factors and thus influence similarities and differences reported in the data. Selection of participants based on SES was however not one of the guidelines or inclusion criteria for the qualitative study as prespecified by the ICF Research Branch. We took care, especially in South Africa where vast socioeconomic disparities exist to select a sample representing different groups as far as possible. It may be beneficial for future research to ensure more data on SES and level of functional ability of all participants. We finally acknowledge the possibility that diving into categories on the third and fourth levels might have yielded more differences and similarities than linking and comparing second-level ICF categories that are often very broad. Since one of the aims of this study was to determine the generalizability of ICF categories between two very divergent countries who participated in the overall ASD ICF qualitative study (Mahdi, Viljoen, et al., 2018), second-level ICF categories were used to ensure that this study was comparable with Mahdi, Viljoen, et al. (2018).
Conclusion
Despite the divergent nature of contexts, the content of parent/caregiver perceptions was, with a few exceptions, similar. Perceptions more frequently differed regarding body functions as well as activities and participation than about environmental factors relevant to functioning in ASD. Our results suggest that the interaction between context and functioning may be more complex than we predicted. We recommend that more comparative studies on ASD and functioning should be conducted to gain a better understanding of ASD in different contexts. Our findings suggest that our initial concern about unique perceptions being lost by pooling data from very diverse countries in the ICF Core Sets for Autism Spectrum Disorder development process was unfounded. Results from this study thus support the potential future usefulness of ICF Core Sets for Autism Spectrum Disorder for clinical or other use, even across diverse cultures (de Vries & Bölte, 2016; Schiariti, Mahdi, & Bölte, 2018). Examples for clinical use include the development of concrete tools to document strengths and weaknesses in individual functioning, which could be used to personalize interventions. Another use is the development of tools to map environmental facilitators and barriers which could facilitate environmental modification and assist in the development of policies of inclusion for individuals with ASD.
Daley (2002) discussed the fact that individuals experiencing the same contextual factors may attach very different values to it and that the experience of ability/disability is therefore subjective or relative. The findings of our study underline the importance of the subjective rather than absolute nature of parental experience of context, and of ability and disability in their children with ASD.
Supplemental Material
AUT829868_Lay_Abstract – Supplemental material for Parent/caregiver perspectives of functioning in autism spectrum disorders: A comparative study in Sweden and South Africa
Supplemental material, AUT829868_Lay_Abstract for Parent/caregiver perspectives of functioning in autism spectrum disorders: A comparative study in Sweden and South Africa by Marisa Viljoen, Soheil Mahdi, David Griessel, Sven Bölte and Petrus J de Vries in Autism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by a Harry Crossley Foundation Masters Research Scholarship award to M.V. P.J.d.V. was supported by the University of Cape Town, Struengmann Fund and the National Research Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.