
Abstract
Parents of children with autism spectrum disorder appear to experience high levels of psychological distress, yet little is known about the prevalence of psychological disorders in this population. The aim of this systematic review and meta-analysis was to estimate the proportion of these parents who experience clinically significant psychopathology. Articles reporting proportions of psychological disorders in a sample of parents of children with autism spectrum disorder were located. The initial search returned 25,988 articles. Thirty-one studies with a total sample of 9208 parents were included in the final review. The median meta-analytic proportions were 31% (95% confidence interval = [24%, 38%]) for depressive disorders, 33% (95% confidence interval = [20%, 48%]) for anxiety disorders, 10% (95% confidence interval = [1%, 41%]) for obsessive-compulsive disorder, 4% (95% confidence interval = [0%, 22%]) for personality disorders, 2% (95% confidence interval = [1%, 4%]) for alcohol and substance use disorders and 1% (95% confidence interval = [0%, 5%]) for schizophrenia spectrum disorders. Significant heterogeneity was detected in these categories. Further research is needed to gain more insight into variables that may moderate parental psychopathology. This review and meta-analysis is the first to provide prevalence estimates of psychological disorders in parents of children with autism spectrum disorder.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder marked by persistent deficits in social communication and interaction, and repetitive patterns of behaviour (American Psychiatric Association (APA), 2013). Individuals with ASD may show little to no sharing of emotions or initiation of social interaction and can require very high levels of caregiver support (Bonis, 2016). Disruptive and challenging behaviours are more common in children with ASD than in any other neurodevelopmental disorder (APA, 2013). Such behaviours can include disruptive and unpredictable behaviours such as continuous periods of screaming, aggressive and violent behaviours, suicidal behaviours and meltdowns (McClintock, Hall, & Oliver, 2003). A substantial proportion of parents identify that child behavioural difficulties constitute the most challenging aspect of their parenting experience, above communication difficulties and the high level of practical support required by their child (Bitsika & Sharpley, 2004; Kissel & Nelson, 2016; Myers, Mackintosh, & Goin-Kochel, 2009). Although the literature tends to associate conditions with greater severity of cognitive impairment in children with ASD with poorer mental health outcomes for parents (Ekas & Whitman, 2010), the experience of parents who have children with ASD without intellectual disability (ID) cannot be overlooked. Some challenging behaviours, such as aggression and self-injury, are not predicted by ASD symptom severity or level of cognitive impairment (Kanne & Mazurek, 2011; McClintock et al., 2003). Despite these significant challenges, it is important to note that some parents report a sense of personal growth in the context of parenting their children with ASD, reflecting on the experience as something that fostered significant personal and/or spiritual change (Nichols, 2019; Wayment, Al-Kire, & Brookshire, 2018; Zhang, Yan, Barriball, While, & Liu, 2015).
Nevertheless, a recent meta-analysis found that many parents of children with ASD reported higher levels of stress than parents of neurotypical children and children with other disabilities such as Down syndrome, cerebral palsy and ID (Hayes & Watson, 2013). Given these high stress levels, it is appropriate to speculate that parents of children with ASD may be more at risk of psychological disorders than parents of typically developing children. Increased psychopathology in parents of children with ASD has been associated with poorer parental functioning (Zerach, Greene, Ein-Dor, & Solomon, 2012), greater conflict with children (Ruscio, Weathers, King, & King, 2002), greater severity of child behavioural problems (Baker, Seltzer, & Greenberg, 2011; Ekas & Whitman, 2010; Firat, Diler, Avci, & Seydaoglu, 2002; Machado Junior, Celestino, Serra, Caron, & Pondé, 2016) and the application of more severe discipline regimes (Cohen, Hien, & Batchelder, 2008). Although systematic reviews of the literature on parents of children with ASD have focused on parenting stress (Bonis, 2016; Cachia, Anderson, & Moore, 2016; Corcoran, Berry, & Hill, 2015; Hayes & Watson, 2013; Karst & Van Hecke, 2012), quality of life (Vasilopoulou & Nisbet, 2016) and social impacts (Saini et al., 2015; Serrata, 2012), there is currently only one meta-analysis that has explored psychological disorders in parents of children with ASD (Yirmiya & Shaked, 2005).
In evaluating psychological disorders in parents of children with ASD, the meta-analysis by Yirmiya and Shaked (2005) investigated the presence of a range of ‘psychiatric difficulties’ in parents of children with ASD, compared to a range of control groups, including parents of children with Down syndrome, mental retardation, psychiatric disorders, learning disabilities as well as those with neurotypical children. Interestingly, the authors did not report meta-analytic results for individual psychological disorders but instead reported an overall effect size for the presence of any ‘psychiatric difficulty’. In this meta-analysis, psychiatric difficulty included symptoms of depression and anxiety, as well as non-clinical variables such as personality traits (i.e. neuroticism). They found that parents of children with ASD reported higher psychiatric difficulties than the comparison groups (Cohen’s d = 0.26, 95% confidence interval (CI) = [0.18, 0.35]) across 35 independent effect sizes. As such, these data indicate that while parents of children with ASD show significantly more psychiatric difficulty than other parental groups, the effect is small (Yirmiya & Shaked, 2005). When taken together, these data provide preliminary support for a higher prevalence of psychological disorders in parents of children with ASD; however, the failure of this study to differentiate between clinical and non-clinical constructs means it is not possible to differentiate which specific disorders parents of children with ASD may be experiencing and at what rates.
In examining the impact of several moderator variables on the overall meta-analytic effects, Yirmiya and Shaked (2005) established that method of assessment was significant. Specifically, where self-report measures of parental psychiatric difficulty were used, the prevalence of psychological disorder in parents of children with ASD was significantly higher than when structured diagnostic interviews were used (Yirmiya & Shaked, 2005). This review included studies using self-report measures in assessing parental psychological outcome, without a clear rationale regarding the use of such measures (e.g. by reporting only on parents scoring in the ‘provisional range’ identified by the authors of the self-report measure). Therefore, it is not clear if clinical disorders such as depression were operationalized diagnostically, in terms of meeting DSM (Diagnostic and Statistical Manual of Mental Disorders) diagnostic criteria for that disorder, or in terms of symptomatology only, without consideration for whether these symptoms met diagnostic thresholds.
Previous meta-analyses have also identified that diagnostic interviews, relative to self-report measures, tend to result in lower and narrower estimates of prevalence rates (Osborn, Mathias, Fairweather-Schmidt, 2016; Spaans, Molendijk, de Beurs, Rinne, & Spinhoven, 2017). Self-report measures typically assess presence and severity of symptoms and often do not assess the degree of functional impairment stemming from these symptoms, which is ultimately required for diagnosis (Cabizuca, Marques-Portella, Mendlowicz, Coutinho, & Figueira, 2009). While such measures provide important information regarding symptomatology, they do not operationalize this impact where it causes functional and clinical impairment. Given the lack of a demarcation between symptomatology and psychopathology in the Yirmiya and Shaked (2005) meta-analysis, it remains unclear as to whether parents of children with ASD experience clinically significant psychopathology. To elaborate on these findings and explore psychopathology of parents of children with ASD (as opposed to symptomatology only), in the current meta-analysis we sought to identify the proportions of parents of children with ASD with diagnoses (or provisional diagnoses) of psychological disorders.
Methods
This review was conducted in accordance with the evidence-based guidelines for systematic reviews described in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (see Supplemental Figure 1; Liberati et al., 2009).
Search strategy
CINAHL, Embase, Informit, MEDLINE and PsycINFO were searched in November 2016 for empirical studies published in English using the following search terms: depression OR anxiety OR stress OR ‘mental health’ OR ‘mental illness’ OR ‘psychological distress’ OR symptom* OR psychopathology OR ‘mood disorder*’ OR ‘depressive disorder*’ OR ‘anxiety disorder*’ OR diagnos* OR ‘affective disorder*’ OR ‘mental disorder*’ OR psychiatric AND parent* OR mother* OR father* OR maternal OR paternal AND child* OR infan* OR toddler OR adolescen* OR teen* AND ASD OR ‘autism spectrum disorder’ OR aspergers OR ‘autistic disorder’ OR ‘developmental disabilit*’. The database was updated in January 2019. Using this search strategy, a total of 25,988 articles were located. An additional sample of two articles were located in the reference list of a review article (Stewart, McGillivray, Forbes, & Austin, 2016); 9716 exact duplicate articles were filtered, leaving 16,274 articles for title and abstract review.
Study selection
To be included in the analysis, articles had to be (1) empirical studies, (2) written in English, (3) reporting proportions of diagnoses or provisional diagnoses of psychological disorders in a sample of parents of children with ASD and (4) report on diagnoses or provisional diagnoses occurring after the birth of the child with ASD. We included strict criteria around the use of self-report measures to obtain clearer proportions of parental psychopathology; by only including studies reporting on the proportion of the sample scoring above the threshold for a provisional diagnosis of a psychological disorder. Self-report measures with cut-off scores that indicate provisional diagnoses of psychological disorders are typically informed by validation studies, using clinical patients with the disorder of interest as their sample. Psychological disorders were operationalized in this review as diagnoses (i.e. ‘Major Depressive Disorder’) or categories of diagnoses (i.e. ‘Depressive Disorders’) represented in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013). Proportions of non-clinical variables that were not related to psychological disorders, such as quality of life or personality variables like neuroticism, were excluded. Based on title and abstract review, 15,641 papers were excluded; 633 papers were screened on their full manuscripts – of this, 602 were excluded. Papers were excluded for assessing non-clinical constructs (n = 322) and for assessing symptomatology of psychological disorders only (n = 153). These papers did not report on the proportion of the sample scoring above the cut-off score for likely diagnosis on the self-report measure. Papers were also excluded for using a sample not comprised of parents of children with ASD (n = 42) and for using qualitative data only (n = 35). Several non-empirical papers (i.e. editorials) were excluded (n = 15), as well as studies not in English (n = 15). English abstracts were available for the articles in languages other than English and were reviewed to establish that all 15 non-English articles did not satisfy other elements of the inclusion criteria, including assessing non-clinical constructs (n = 7), being of a non-empirical nature (n = 5) and using samples not comprised of parents of children with ASD (n = 3). A total of 31 studies comprised the final database. The screening process is summarized in Figure 1.

Flow diagram of systematic review and meta-analysis screening process.
Screening and estimation of screener reliability
Screening was performed by the first author (A.S.) in full; a sample of 10% of title/abstract and 10% of full text articles were also independently screened by two review authors (A.S. and E.J.H.) for interrater reliability testing. Interrater reliability was determined using prevalence-adjusted bias-adjusted kappa (PABAK; Byrt, Bishop & Carlin, 1993). PABAK was calculated to determine the agreement between A.S. and E.J.H. on inclusion and exclusion of articles. There was very strong agreement between the two authors for both title/abstract screening, PABAK = 0.96, and full text screening, PABAK = 0.93. Any inconsistencies or disagreements were resolved by discussion.
Data extraction
The following variables were extracted: year of publication, sample size, age of parents, sex of parents, age of children, sex of children, country of publication, diagnostic measure for ASD, if the study was limited to parents of children with diagnosed ASD only and what these inclusion/exclusion criteria were, measure of parental psychopathology, type of measure (self-report or diagnostic interview), the cut-off value used for provisional diagnoses in self-report measures, diagnosis category and the percentage of the sample reported to be in the clinical range for that diagnosis.
To assess study quality, information on methodology was extracted to complete the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH; 2014) Quality Assessment of Observational Cohort and Cross-Sectional Studies, a 14-item quality assessment tool developed for observational studies. Twenty-five of the included studies were cross-sectional or cohort studies, and cross-sectional baseline data were extracted from one randomized controlled trial. Four criteria were excluded as they were not relevant in our review, leaving 10 criteria. There were five case-control studies; these were assessed for study quality using a 12-item quality assessment tool specifically for case-control studies (NHLBI NIH, 2014). Each criterion was assigned 1 point if the quality criterion was met. Given some criteria not applicable to some studies, a total percentage of met criteria were tallied for each study, with greater percentages indicating greater study quality. The third author (D.J.H.) assessed a sample of studies (20%) for interrater reliability.
Meta-analysis
Meta-analyses were conducted using the metafor package v1.9.8 (Viechtbauer, 2010) in R software v3.3.1 (RStudio Team, 2015). The proportion of the sample reported to be in the clinical range (as measured by meeting criteria for diagnosis or reaching a cut-off value on a self-report measure) was used as an effect size measure. Given that proportions were used as the measure of effect size, analyses were conducted using a binomial-normal model (with logit link). Effects were subsequently back-transformed to represent the median meta-analytic proportion of parents with the clinical diagnosis of interest. A random effects model was estimated for all meta-analysis calculations. This model assumes that effect sizes in a population are not constant, and that variance can be attributed to factors other than sampling error, such as sample characteristics, study design and methods of measurement (Borenstein, Hedges, Higgins, & Rothstein, 2009). Effect sizes were weighted in each analysis by the inverse of their variance (Borenstein et al., 2009). Meta-analyses were conducted separately for each diagnostic group if at least two studies providing effect sizes were available for analysis. Analyses were conducted for depressive disorders, anxiety disorders, obsessive-compulsive disorder (OCD), personality disorders, alcohol and substance use disorders and schizophrenia. While there were studies meeting the inclusion criteria for post-traumatic stress disorder, somatic symptom disorder and behavioural disorders, there were an insufficient number of studies in each diagnostic category to be included in the meta-analysis.
We examined whether the meta-analytic effects were robust to the following variables that might moderate any effects: assessment method, diagnosis type, parent gender and child age. Specifically, we examined whether these variables were significant moderators of the meta-analytic effect when there were at least two effects available for the categories of interest. The heterogeneity of proportions was assessed using the I² statistic, which shows the size of heterogeneity among effect sizes, where 50% or higher typically indicates significant variance between effect sizes (Borenstein et al., 2009). Funnel plots were inspected to assess for publication bias in the selected studies. There is evidence to suggest that conventional funnel plots (constructed by plotting log odds on the x-axis and standard error on the y-axis) can result in erroneous conclusions regarding asymmetry in proportional meta-analyses, due to the correlation between the standard error and the value of the log odds (Hunter et al., 2014). An alternative method of funnel plot construction, with sample size as the measure of accuracy on the y-axis, has been indicated for such meta-analyses (Hunter et al., 2014); hence, publication bias was assessed using this method. The trim-and-fill procedure (Duval & Tweedie, 2000) was used to correct for asymmetry, whereby studies are removed from the asymmetrical side of the funnel plot and then re-imputed along with studies on the opposite side of the funnel that may be missing due to publication bias in favour of significant results. This procedure provided an adjusted proportion estimate after accounting for this trim-and-fill procedure.
Results
Sample characteristics
A total of 54 proportions of parents of children with ASD scoring in the clinical range for a psychological disorder from 31 studies were included. Studies were published between the years 1997 and 2018. A summary of the included studies can be seen in Table 1. None of the studies identified in the previous meta-analysis on this subject (Yirmiya & Shaked, 2005) were included in this study. This is likely due to its focus on lifetime psychological difficulty prior to having a child with ASD, in contrast to the current study that sought to explore psychological disorders emerging in the context of parenting a child with ASD.
Study characteristics, measures and proportion of sample observed to have met criteria for a full or provisional diagnosis (N = 29).

ICD: International Classification of Diseases; SD: standard deviation; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.); WHO: World Health Organization.
The studies were conducted in 15 different countries. The largest group consisted of North American studies (29%), followed by Australian studies (23%). More than half of the proportions identified in this review were related to depressive disorders such as major depressive disorder and dysthymia (52%), while 31% of the proportions were related to anxiety disorders such as generalized anxiety disorder and social anxiety disorder. Due to the small number of studies explicitly referring to specific disorders (e.g. social anxiety disorder), proportions for these specific disorders, where present, were collated into an overall category, that is, anxiety disorders. The remaining proportions of effect sizes identified related to OCD (5.5%), alcohol and substance use disorders (3.7%), personality disorders (3.7%) and schizophrenia spectrum disorders (3.7%). Seventy percent of the proportions identified in this study came from self-report measures, and 15% were from diagnostic interviews. The remaining 15% of proportions were collated using historical diagnoses from hospital and mental health service records.
In total, 9208 parents of children with ASD were included in the studies with a mean sample size of 149 (standard deviation (SD) = 162.94, range = 20–722). A proportion of studies assessed only mothers of children with ASD (20%) and seven studies (13%) used an evenly proportioned sample of both mothers and fathers. No studies in this review assessed fathers only. Age of children was not always clear; 20% of studies did not report any details of the age of the children of participants. A further 20% of studies reported children of participants in the broad age brackets of 2 up to 33 years of age. Thirty-one percent of studies reported clearer age categories, identifying participants as ‘parents of toddlers with ASD’ or ‘parents of adolescents with ASD’. Sixty percent of studies reported on a sample of parents of children with ASD only, while 40% either did not report characteristics of the diagnosis of children in the sample or utilized a mixed sample of parents of children with ASD and parents of children with other developmental disorders and developmental delay.
Study quality
The results of the quality assessment of included studies can be seen below. Cross-sectional studies are reported in Table 2 and case-control studies are reported in Table 3. The average quality rating was 48% (SD = 16%) for cross-sectional/cohort studies and 65% (SD = 21%) for case-control studies. With regard to interrater reliability, A.S. and D.J.H. were in agreement on all criteria.
Quality assessment of cross-sectional/cohort studies included in meta-analysis (k = 26).
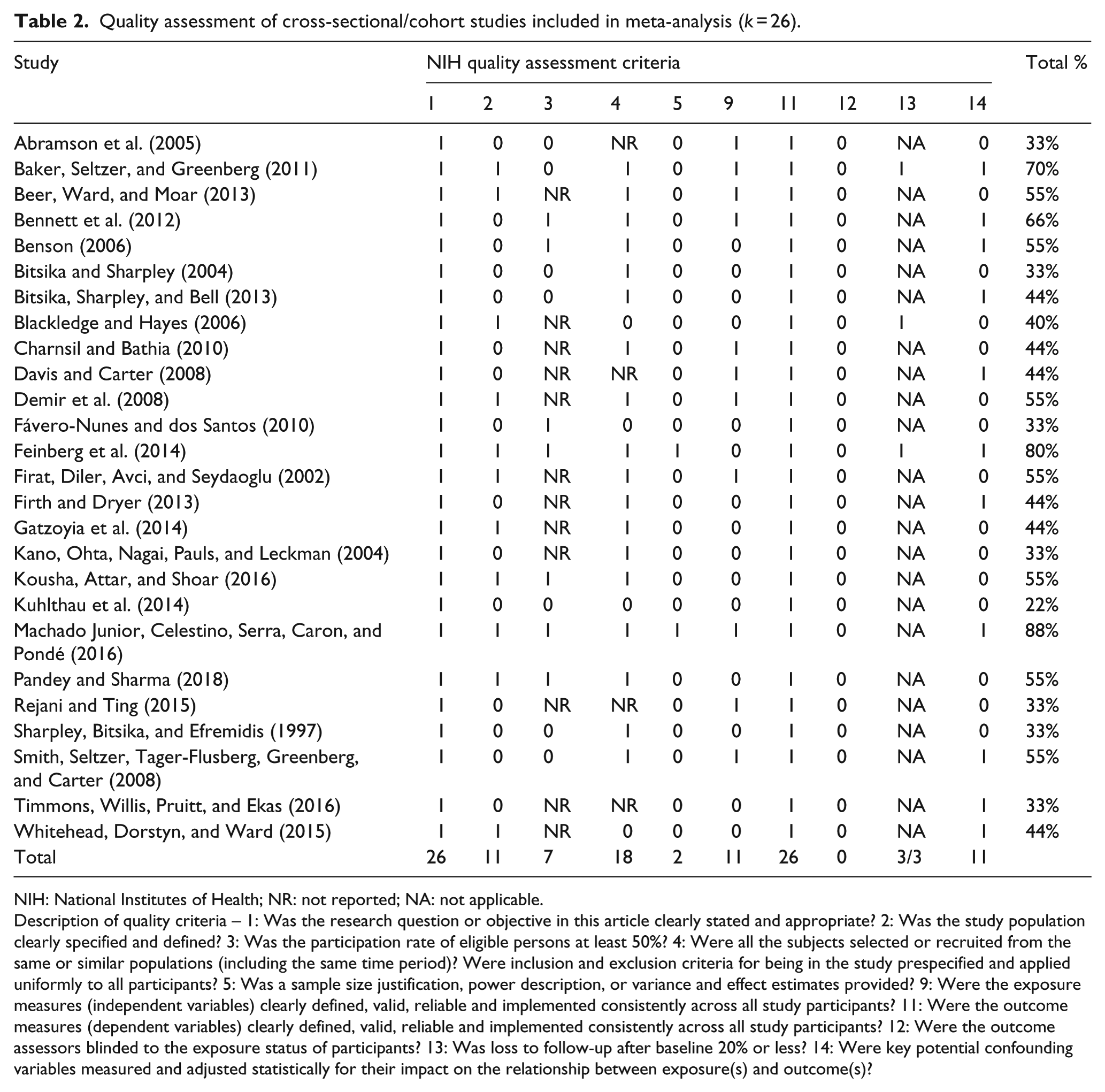
NIH: National Institutes of Health; NR: not reported; NA: not applicable.
Description of quality criteria – 1: Was the research question or objective in this article clearly stated and appropriate? 2: Was the study population clearly specified and defined? 3: Was the participation rate of eligible persons at least 50%? 4: Were all the subjects selected or recruited from the same or similar populations (including the same time period)? Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? 5: Was a sample size justification, power description, or variance and effect estimates provided? 9: Were the exposure measures (independent variables) clearly defined, valid, reliable and implemented consistently across all study participants? 11: Were the outcome measures (dependent variables) clearly defined, valid, reliable and implemented consistently across all study participants? 12: Were the outcome assessors blinded to the exposure status of participants? 13: Was loss to follow-up after baseline 20% or less? 14: Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?
Quality Assessment of Case-Control Studies Included in Meta-Analysis (k = 5).
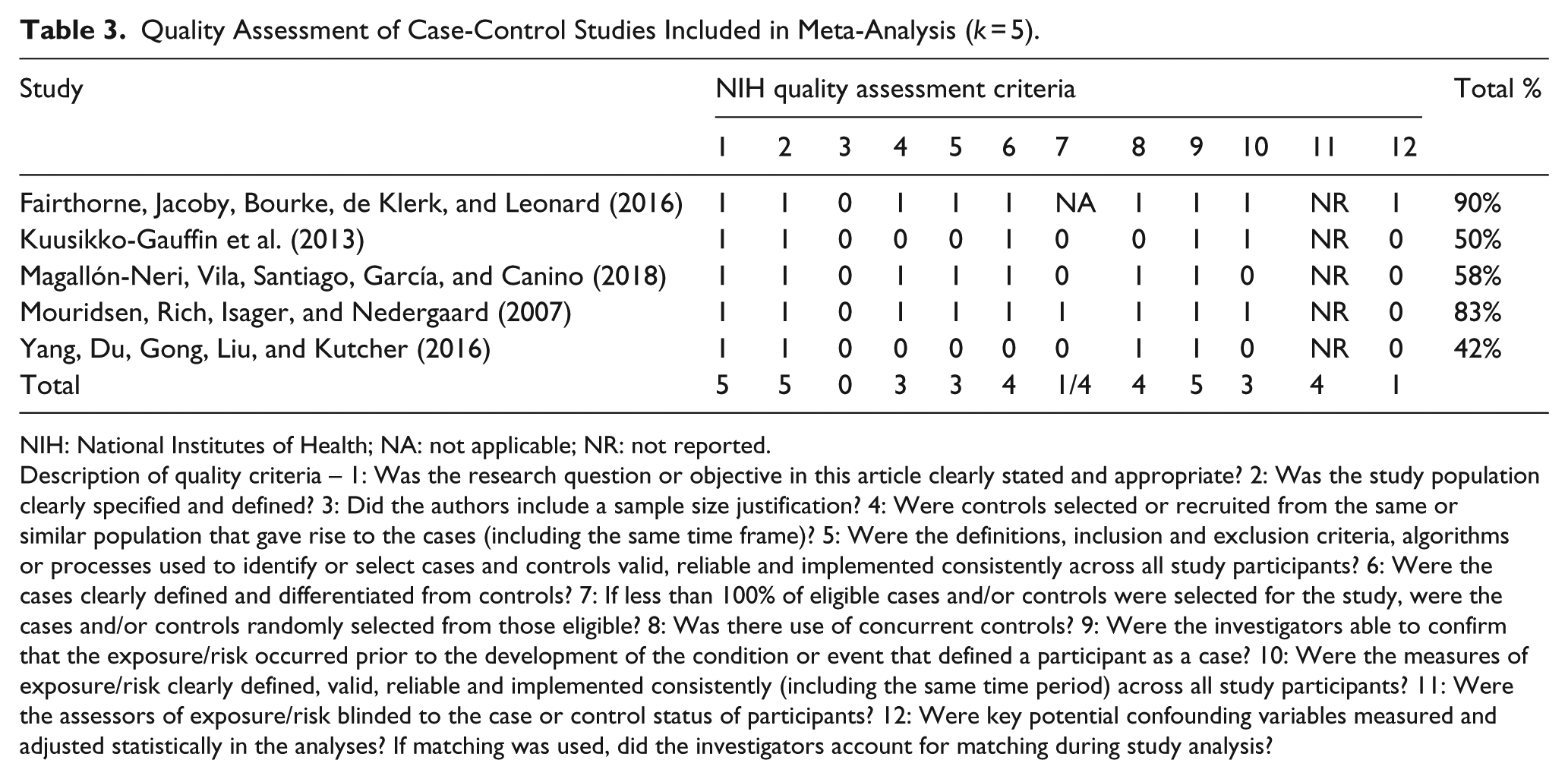
NIH: National Institutes of Health; NA: not applicable; NR: not reported.
Description of quality criteria – 1: Was the research question or objective in this article clearly stated and appropriate? 2: Was the study population clearly specified and defined? 3: Did the authors include a sample size justification? 4: Were controls selected or recruited from the same or similar population that gave rise to the cases (including the same time frame)? 5: Were the definitions, inclusion and exclusion criteria, algorithms or processes used to identify or select cases and controls valid, reliable and implemented consistently across all study participants? 6: Were the cases clearly defined and differentiated from controls? 7: If less than 100% of eligible cases and/or controls were selected for the study, were the cases and/or controls randomly selected from those eligible? 8: Was there use of concurrent controls? 9: Were the investigators able to confirm that the exposure/risk occurred prior to the development of the condition or event that defined a participant as a case? 10: Were the measures of exposure/risk clearly defined, valid, reliable and implemented consistently (including the same time period) across all study participants? 11: Were the assessors of exposure/risk blinded to the case or control status of participants? 12: Were key potential confounding variables measured and adjusted statistically in the analyses? If matching was used, did the investigators account for matching during study analysis?
Proportion of sample in the clinical range of psychiatric disorders
Meta-analytic results for proportions of parents of children with ASD scoring in the clinical range of psychological disorders are presented in Table 4.
Median proportion of parents of children with autism spectrum disorder in the clinical range of psychological disorders.
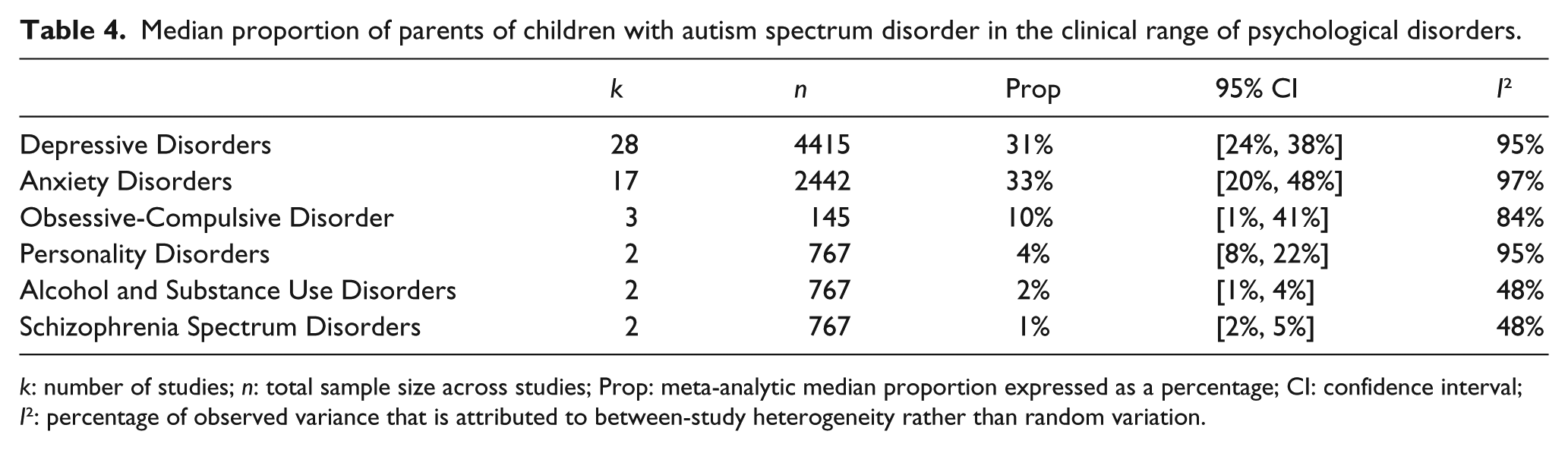
k: number of studies; n: total sample size across studies; Prop: meta-analytic median proportion expressed as a percentage; CI: confidence interval; I²: percentage of observed variance that is attributed to between-study heterogeneity rather than random variation.
Calculating a pooled prevalence rate for all psychological disorders combined was not indicated, as many studies examined only single disorders or had multiple disorders in one sample with comorbidity between participants. Only one study (Machado Junior et al., 2016) reported an overall total proportion of the sample experiencing any psychological disorder (41.2% in this sample). Of the 16 studies reporting proportions of only one category in the study, 13 of these studies were related to depressive disorders; a further 2 were related to OCD and 1 was related to anxiety disorders. Therefore, it was not possible to meaningfully capture the prevalence of all psychological disorders in this meta-analysis, as the available studies were not representative of the studies included in the overall meta-analysis.
Heterogeneity statistics were significant (p < 0.001) for all analyses except for alcohol and substance use disorders and schizophrenia, suggesting the presence of important confounding variables that may account for the variability in the observed proportions. Meta-regression analyses were conducted to attempt to account for the effect of these variables; however, these were only possible for the depressive disorder and anxiety disorder categories, as there was an insufficient number of studies in remaining categories.
Meta-regression analyses
The moderator variable of assessment type was categorically coded, with two categories reflecting either (0) self-report measures or (1) diagnostic interviews. Child diagnosis was also categorically coded, with two categories reflecting either (0) children with ASD only or (1) children with ASD and children with other developmental disabilities, such as developmental delay. Given that the studies in this review either had a sample of almost exclusively mothers (90%+ mothers) or were half comprised of mothers, parent gender was analysed as a categorical variable, with two categories reflecting (0) mothers only (100% of the sample) or (1) an evenly proportioned sample of mothers and fathers. Finally, child age was analysed as a continuous variable, with the mean age of the sample’s children used for these analyses (where it was reported). Due to too few studies in other diagnostic categories, meta-regression analyses were only possible for the category of depressive disorders and anxiety disorders. Meta-regression analyses for the type of assessment used was only possible for the category of depressive disorders. The results of these analyses are presented in Table 5.
Series of unstandardized meta-regression analyses for moderator variables of parent psychopathology.
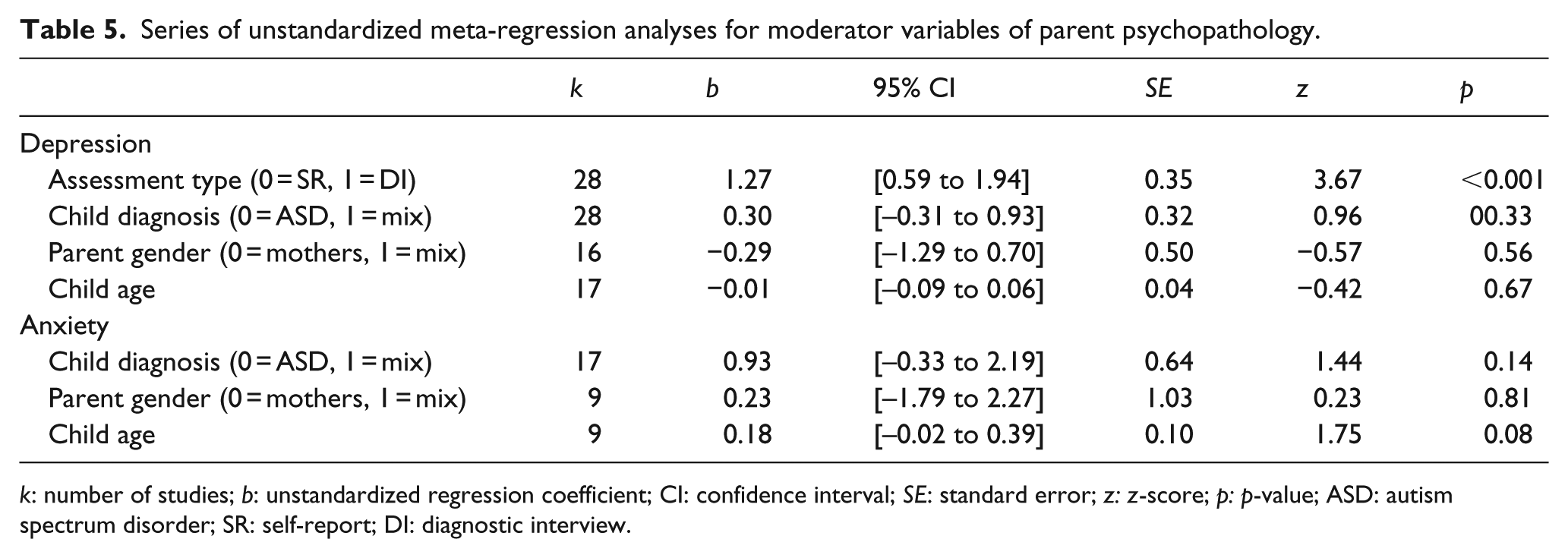
k: number of studies; b: unstandardized regression coefficient; CI: confidence interval; SE: standard error; z: z-score; p: p-value; ASD: autism spectrum disorder; SR: self-report; DI: diagnostic interview.
The use of self-report measures was associated with a higher median proportion of depressive disorder diagnoses in parents of children with ASD (k = 23, prop = 36%, 95% CI = [29%, 42%]) when compared to diagnostic interviews (k = 5, prop = 13%, 95% CI = [7%, 21%]). Moderator analysis found that there was no significant difference in the median proportion when examining child diagnosis, parent gender or child age. Proportions of depressive disorders and anxiety disorders were not significantly different when analyses included studies where child diagnosis was mixed (e.g. a mixed sample of parents of children with ASD, and parents of children with other developmental disabilities, such as developmental delay). Parent gender was not a statistically significant moderator of proportions of mental illness in parents of children with ASD and there was no significant difference in analyses where evenly mixed gender samples were used, compared to samples using only mothers of children with ASD. Where child age was analysed continuously, there was no significant difference in parental depression where child age increased or decreased between studies. The effect of child age on parental anxiety was trending towards significance (p < 0.08), whereby anxiety was somewhat greater for parents of older children with ASD.
Analysis of publication bias
The heterogeneity statistics indicated significant between-study variance in the categories of depressive disorders (I² = 95%), anxiety disorders (I² = 97%) and OCD (I² = 84%). Inspection of the funnel plot indicated some asymmetry (see Supplemental Figures 3–5). The trim-and-fill procedure was used to yield an adjusted proportion for each category. While personality disorders had high heterogeneity (I² = 95%), there was an insufficient number of studies for trim-and-fill procedures (k = 2). The adjusted proportions can be seen in Supplemental Table 6.
The trim-and-fill procedure did not result in a change to the observed proportions for the categories of depressive disorders and anxiety disorders, nor did it remove or impute any studies from the funnel plot. For the category of OCD, the adjusted proportion (33%, 95% CI = [1%, 41%]) was greater than the original proportion (10%, 95% CI = [5%, 81%]). Two studies were imputed to the right of the plot (see Supplemental Figure 6). These results suggest that, for the categories of depressive and anxiety disorders, the observed proportions were robust to the trim-and-fill procedure and thus provided no evidence for publication bias or significant outliers in the sample. For the category of OCD, it is likely that the large change in proportions using the trim-and-fill procedure is a consequence of only having a small number of studies in this analysis (k = 3) and should not be interpreted as confirmation of publication bias.
Discussion
This review and meta-analysis aimed to identify the prevalence of clinical psychological disorders in parents of children with ASD. Depressive disorders were evaluated in 28 studies (N = 4415) and were seen to have a combined proportion of 31% (95% CI = [24%, 38%]) in parents of children with ASD, a higher proportion than the estimated global prevalence of depression in the general population of 4.4% (World Health Organization [WHO], 2017). Anxiety disorders were evaluated in 17 studies (N = 2442) and were seen to have a combined proportion of 33% (95% CI = [20%, 48%]), significantly higher than the estimated global prevalence of anxiety disorders in the general population of 3.6% (WHO, 2017). OCD was evaluated in three studies (N = 145) and the combined proportion of 10% (95% CI = [1%, 41%]) is higher than the Australian 12-month prevalence of OCD in the general population of 1.9% (Australian Bureau of Statistics (ABS), 2008) and the 12-month prevalence of OCD in the US general population of 1% (Kessler, Chiu, Demler, & Walters, 2005). Personality disorders were evaluated in two studies (N = 767); the combined proportion of 4% (95% CI = [8%, 22%]) in parents of children with ASD appears to be lower than cross-national estimates of 6.1% (Huang et al., 2009). Alcohol and substance use disorders were evaluated in two studies (N = 767); the combined proportion of 2% (95% CI = [1%, 4%]) in parents of children with ASD appears to be lower than the 5.1% 12-month prevalence rates of alcohol and substance use disorders in the Australian general population (ABS, 2008). Schizophrenia spectrum disorders were evaluated in two studies (N = 767); the combined proportion of 1% (95% CI = [2%. 5%]) in parents of children with ASD appears to be in line with prevalence rates of approximately 1.4% in the global population (Jablensky, 2000).
With regard to moderator variables, the type of assessment used to capture psychological disorders was seen to have a significant effect, with proportions of depressive disorder diagnoses lower when diagnostic interviews were used than self-report measures. This is in line with previous meta-analyses, which document that the use of diagnostic interviews (compared to self-report measures) tended to result in lower estimates of prevalence rates (Osborn et al., 2016; Spaans et al., 2017). Self-report measures and diagnostic interviews both capture important information regarding symptomatology; however, diagnostic interviews go beyond these data by exploring the level of functional impact stemming from these symptoms, helping to better guide clinical decision making. This is especially useful in complex cases where comorbidity is present. In many studies in this meta-analysis, many parents were reported to experience high levels of comorbid depressive and anxiety symptoms. Diagnostic interviews can be seen to usefully differentiate functionally impaired individuals from those who are not and are likely to be more clinically useful than self-report measures. This meta-analysis utilized self-report measures with cut-off thresholds that, when exceeded, suggest a provisional diagnosis of that disorder. These cut-off scores are typically informed by validation studies utilizing clinical patients with the disorder of interest as their sample. In such cases, it can be assumed that these cut-off scores are diagnostically valid, as they should differentiate individuals with the diagnosis from those not meeting diagnostic criteria. In this meta-analysis, it is possible that some of the self-report measures used may not have been informed by validation studies utilizing clinical samples. Therefore, this may represent a limitation of the present meta-analysis and impact the sensitivity of the results.
There was a trending association observed between child age and parental anxiety, whereby increases in child age were found to be related to increases in parental anxiety. It is surprising that child age did not emerge as a significant moderator of proportions of parental psychopathology, given evidence to suggest that the experience of parenting an adult child with ASD carries unique challenges and implications for symptoms of depression and anxiety (Barker et al., 2011; Cadman et al., 2012; Hines, Balandin, & Togher, 2014). It is possible that the relationship between child age and parental psychopathology was obscured in this meta-analysis, as some of the included studies either did not report on child age (k = 6) or reported broad age ranges in their sample (k = 5; reporting samples ranging from 3 to 20 years), resulting in low power to detect relationships between child age and parental psychopathology.
Furthermore, parent gender did not emerge as a significant moderator of proportions of parental psychopathology. It may be that mothers and fathers experience similar levels of psychopathology in their parenting experience. There is some evidence to suggest that mothers of children with ASD experience greater rates of stress (Allen, Bowles, & Weber, 2013; Dabrowska & Pisula, 2010; Foody, James, & Leader, 2015; Little, 2002; Soltanifar et al., 2015) and self-reported depression and anxiety (Foody et al., 2015; Hastings, 2003; Hastings et al., 2005). There is also conflicting evidence suggesting that parents do not differ in their experience of stress (Davis & Carter, 2008; Hastings, 2003), depression (Hastings, 2003) or anxiety (Davis & Carter, 2008). No studies included in the present meta-analysis assessed fathers only, and only seven studies recruited an evenly balanced sample of both genders. The number of mothers in the studies in this meta-analysis (N = 3566) far outweighed the number of fathers (N = 613). Any comparisons made in this meta-analysis between mothers and fathers were likely to have been confounded by this difference in group sample sizes. Given the dearth of research with gender-balanced samples of parents of children with ASD, more research focusing on fathers is needed to adequately capture paternal psychopathology and to make adequate comparisons with mothers.
Child diagnosis did not emerge as a significant moderating variable in this meta-analysis, but there is some potential that these effects were masked by high heterogeneity within the studies. It is important to note that many studies failed to report on this variable. Other studies relied on parental report of child diagnosis, without access to medical records. It could be that moderating effects of these variables, and thereby differences in parental psychopathology between groups of parents of children with different neurodevelopmental disorders, were masked by imprecise methods of data collection.
The range of proportions in this meta-analysis was broad, with some studies reporting proportions of disorders as low as 3% in their sample and others reporting proportions as high as 90%. Sample sizes of studies ranged from those with 20 participants, to studies with samples of 700+ participants. It is possible that the moderating effects of any variables were clouded by heterogeneity between proportions and sample sizes across studies. Indeed, while trim-and-fill procedures did not suggest any evidence of publication bias for the categories of depressive disorders and anxiety disorders, a high level of heterogeneity was still observed in these categories. The diagnosis of ASD itself is highly heterogeneous, subject to much debate regarding the diagnostic features of the disorder (Masi, DeMayo, Glozier, & Guastella, 2017) and few observed neurobiological commonalities across individuals with ASD (Lenroot & Yeung, 2013). It appears that the population of parents of children with ASD is highly heterogeneous also, given markedly different observations of parent distress reported across studies.
In several studies in this meta-analysis, the challenging behaviours of children with ASD were implicated in parental psychopathology (i.e. Baker, Seltzer & Greenberg, 2011; Ekas & Whitman, 2010; Firat, Diler, Avci, & Seydaoglu, 2002; Machado Junior et al., 2016). Some parents of children with ASD face a chronically stressful parenting experience marked by patterns of a variety of challenging behaviours, including physical violence towards their caregivers, meltdowns and self-harming and suicidal behaviours (McClintock et al., 2003). It has been demonstrated that higher frequency and diversity of behavioural ASD symptoms, including hyperactivity, shrieking or screaming, sleep problems, meltdowns and tantrums, self-injury and aggression towards others, were predictive of greater parental depression and stress (Ekas & Whitman, 2010). Severe behavioural symptoms in children with ASD have been seen to increase the severity of symptoms of anxiety and depression in parents. Parents of children with severe behavioural problems are three times more likely to experience symptoms of anxiety and depression than parents of children with less severe behavioural problems (Machado Junior et al., 2016). Despite evidence to suggest a significant relationship between challenging behaviours and psychopathology, it was not possible to examine the moderating role of such behaviours in the present meta-analysis, as not enough studies reported these data. Future research exploring parental psychopathology would benefit from the inclusion of data relating to challenging child behaviours, which may serve as a helpful anchor point for predicting parental psychopathology in an otherwise heterogeneous population.
In summary, this meta-analysis is the first to provide prevalence rates of psychological disorders in parents of children with ASD. Differences between proportion rates in studies examining depressive disorders were accounted for in some part by the types of measures used to capture parental depression. Differences in child age, parent gender and child diagnosis were not seen to have a significant impact on levels of parental psychopathology. However, these potential moderating variables were impacted by gaps in data collection; future research would benefit from the inclusion of data around child age and verification of the diagnosis of the child. It was not possible to examine the moderating impact of challenging child behaviours, despite evidence to suggest a positive relationship between parental symptomatology and challenging behaviours. Future research would benefit from the inclusion of more fathers and detailed collection of data around challenging child behaviours. Given the high levels of comorbidity in this population, the utility of diagnostic interviews is indicated in both future research and clinical settings, to yield more accurate proportions of psychological diagnoses and better guide clinical decision making in treating parents of children with ASD.
Supplemental Material
AUT844636_Lay_Abstract – Supplemental material for Psychopathology in parents of children with autism spectrum disorder: A systematic review and meta-analysis of prevalence
Supplemental material, AUT844636_Lay_Abstract for Psychopathology in parents of children with autism spectrum disorder: A systematic review and meta-analysis of prevalence by Alexandra Schnabel, George J Youssef, David J Hallford, Eliza J Hartley, Jane A McGillivray, Michelle Stewart, David Forbes and David W Austin in Autism
Supplemental Material
AUT844636_Supplemental_material_Figures_3-6_Table_6 – Supplemental material for Psychopathology in parents of children with autism spectrum disorder: A systematic review and meta-analysis of prevalence
Supplemental material, AUT844636_Supplemental_material_Figures_3-6_Table_6 for Psychopathology in parents of children with autism spectrum disorder: A systematic review and meta-analysis of prevalence by Alexandra Schnabel, George J Youssef, David J Hallford, Eliza J Hartley, Jane A McGillivray, Michelle Stewart, David Forbes and David W Austin in Autism
Supplemental Material
AUT844636_Supplemental_material_Figure_1 – Supplemental material for Psychopathology in parents of children with autism spectrum disorder: A systematic review and meta-analysis of prevalence
Supplemental material, AUT844636_Supplemental_material_Figure_1 for Psychopathology in parents of children with autism spectrum disorder: A systematic review and meta-analysis of prevalence by Alexandra Schnabel, George J Youssef, David J Hallford, Eliza J Hartley, Jane A McGillivray, Michelle Stewart, David Forbes and David W Austin in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.