
Abstract
Prior research studies suggest that maternal polyunsaturated fatty acids could have protective effects on neurodevelopmental outcomes. The objective of this study was to examine associations between maternal polyunsaturated fatty acid intake during pregnancy and risk for autism spectrum disorder and other non-typical development in a prospective cohort. Eligible women already had a child with autism spectrum disorder and were planning a pregnancy or were pregnant with another child. Children were clinically assessed longitudinally and diagnosed at 36 months. Maternal polyunsaturated fatty acid intake during pregnancy was estimated using food frequency questionnaires. Maternal third-trimester plasma polyunsaturated fatty acid concentration was measured by gas chromatography. In all, 258 mother–child pairs were included. Mothers consuming more total omega-3 in the second half of pregnancy were 40% less likely to have children with autism spectrum disorder (relative risk = 0.6, 95% confidence interval: 0.3–0.98). No significant associations were observed between maternal third-trimester plasma polyunsaturated fatty acid subtype concentrations and risk of autism spectrum disorder. However, higher plasma eicosapentaenoic acid and docosahexaenoic acid concentrations were associated with lower non-typical development risk (relative risk ranging from 0.47 to 0.88). This study provides suggestive evidence of associations between risk of autism spectrum disorder in the children and maternal omega-3 intake in late pregnancy but not with third-trimester plasma polyunsaturated fatty acids. Further research is needed to evaluate these potential relationships.
Lay abstract
Prior studies suggest that maternal polyunsaturated fatty acids intake during pregnancy may have protective effects on autism spectrum disorder in their children. However, they did not examine detailed timing of maternal polyunsaturated fatty acid intake during pregnancy, nor did they evaluate plasma concentrations. This study investigates whether maternal polyunsaturated fatty acids in defined time windows of pregnancy, assessed by both questionnaires and biomarkers, are associated with risk of autism spectrum disorder and other non-typical development in the children. Food frequency questionnaires were used to estimate maternal polyunsaturated fatty acid intake during the first and second half of pregnancy. Gas chromatography measured maternal plasma polyunsaturated fatty acid concentrations in the third trimester. In all, 258 mother–child pairs from a prospective cohort were included. All mothers already had a child with autism spectrum disorder and were planning a pregnancy or pregnant with another child. Children were clinically assessed longitudinally and diagnosed at 36 months. For polyunsaturated fatty acid intake from questionnaires, we only found mothers consuming more omega-3 in the second half of pregnancy were 40% less likely to have children with autism spectrum disorder. For polyunsaturated fatty acid concentrations in the third-trimester plasma, we did not observe any statistical significance in relation to the risk of autism spectrum disorder. However, our study confirmed associations from previous studies between higher maternal docosahexaenoic acid and eicosapentaenoic acid plasma concentrations in the late pregnancy and reduced risk for non-typical development. This study markedly advanced understandings of whether and when maternal polyunsaturated fatty acid intake influences risk for autism spectrum disorder and sets the stage for prevention at the behavioral and educational level.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that affects approximately 1 in 59 children in the United States (Baio et al., 2018). ASD is characterized by impaired social interaction and communication as well as restricted interests and/or stereotyped behaviors, and its prevalence has increased over the past 20 years. This increase can partly be explained by changes in diagnostic criteria and greater awareness (Hertz-Picciotto & Delwiche, 2009); however, environmental factors could also play a critical role (Hallmayer et al., 2011; Levine et al., 2018).
Polyunsaturated fatty acids (PUFAs), especially omega-3, play significant roles in the structural and functional development of human brains (Freeman et al., 2006; Haggarty, 2004). Maternal diet strongly influences the fetal PUFA supply (Peet, Laugharne, Mellor, & Ramchand, 1996; Richardson, Calvin, et al., 2000). Dietary and supplemental omega-3 consumption during pregnancy have already been associated with improved neurodevelopmental outcomes in children, such as intelligence quotient (IQ) (Richardson, Easton, & Puri, 2000) as well as cognitive and social skills (Richardson & Ross, 2000). However, relationships between maternal PUFA intake and children’s risk of ASD are not well understood. Although some previous studies (Lyall, Munger, O’Reilly, Santangelo, & Ascherio, 2013; Steenweg-de Graaff et al., 2016; Suren et al., 2013) suggest maternal PUFA insufficiencies, including lower omega-3 and linoleic acid (LA), are significantly related to either higher ASD risk or more autistic traits in their offspring, these studies were unable to examine maternal intake by detailed timing during pregnancy. Moreover, they only used self-reported intake and did not assess these relationships using maternal PUFA concentrations in plasma during pregnancy. Plasma PUFA concentrations could reflect dietary PUFA status over the past 1 to 4 weeks (Harris & Thomas, 2010) and are considered to be more representative of real PUFA status. Understanding these associations is of particular importance given the substantial evidence linking higher maternal intakes of certain nutrients and vitamin supplements to a reduction in the ASD risk (Lyall, Schmidt, & Hertz-Picciotto, 2014).
In this study, we used a prospective cohort design to investigate maternal PUFAs during pregnancy in defined time windows, assessed by both questionnaires and biomarkers, in relation to ASD or other non-typical development (non-TD) in the offspring at 3 years of age. Omega-3, specifically docosahexaenoic acid (DHA), becomes incorporated into the phospholipid membrane of retina and brain and accumulates quickly during the latter part of pregnancy, primarily in the third trimester (Denomme, Stark, & Holub, 2005; Greenberg, Bell, & Ausdal, 2008; Jacobson et al., 2008; Jensen, 2006). These accumulations are preferentially transferred across the placenta, suggesting a particular need for PUFAs at this time period (Hornstra, 2000; Innis, 2000, 2007a, 2007b). On this basis, we hypothesized that higher maternal omega-3 during late pregnancy would be associated with reduced ASD risk in the offspring.
Methods
Study population
Markers of Autism Risk in Babies-Learning Early Signs (MARBLES) study is the first prospective cohort study to recruit mothers of children with ASD in a subsequent pregnancy, who were thus at high risk for delivering another child with ASD. Families were recruited from lists of children receiving autism services obtained via the California Department of Developmental Services (DDS), from other studies at the MIND Institute, or by self-referrals. The inclusion criteria were as follows: (a) mother or father had a biological child with ASD, and the mother was (b) at least 18 years old; (c) pregnant or planning a pregnancy, and biologically able to become pregnant; (d) living within 2 h of the MIND Institute; and (e) sufficiently fluent in English. Participants in the current report were enrolled into the MARBLES study between 2006 and 2016, and included only one child per family. Both the Institutional Review Board at the University of California, Davis and the State of California Committee approved this study.
Outcome
At the 36-month visit, children were classified into 1 of 3 algorithmically defined neurodevelopmental outcome groups: ASD, typical development (TD), and non-TD (and not ASD). The outcome algorithm (Schmidt, Iosif, Guerrero Angel, & Ozonoff, 2019) was defined following previously published methods from the Baby Siblings Research Consortium (Chawarska et al., 2014; Ozonoff et al., 2015). It was derived from four subscale scores (fine motor, expressive language, receptive language, and visual reception) on the Mullen Scales of Early Learning (MSEL; Mullen, 1995) as well as the scores on Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2000). Children with an ASD diagnosis scored over the ADOS cutoff as well as met Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) criteria for ASD (American Psychiatric Association, 2013). Children with TD outcomes had all MSEL T-scores within 2 standard deviations (SDs) and no more than 1 MSEL subscale score that was 1.5 SD below the normative mean, while their ADOS scores were at least 3 or more points below the ADOS cutoff. The rest of the children were categorized into the non-TD group (e.g. those with low MSEL or high ADOS scores, who did not meet criteria for ASD).
Maternal PUFA measurements
Questionnaire: maternal dietary PUFA intake
We used the Block 2005 Food Frequency Questionnaire (FFQ) (Johnson, Herring, Ibrahim, & Siega-Riz, 2007) to assess the comprehensive history of maternal dietary intake in the first and second half of pregnancy. It has 114 food items, and each item has nine frequency options, ranging from never to daily, and several quantity options, such as 1/4 cup per day and 2 cups per day. Individual portion size was also asked for each food, and pictures were provided to enhance the accuracy of quantification. Block FFQs were sent to NutritionQuest (Berkeley, California) to calculate nutrients as previously described (Johnson et al., 2007). The frequency of each food item was defined as the decimal fraction from 0 (=never) to 1 (=every day), and the proportion of each item was converted into grams. The formula used in the calculation of average nutrients per day was the following: ((frequency × proportion)/100) × (nutrient per 100 g). Nutrient per 100 g were derived from Food and Nutrient Database for Dietary Studies (FNDDS), United States Department of Agriculture (USDA) data files, published sources, imputation, and manufactures or label data. At last, the average daily nutrients for all foods were added up to obtain the full average dietary intake per day, including omega-3, omega-6, DHA, eicosapentaenoic acid (EPA), alpha-linolenic acid (ALA), arachidonic acid (AA), and LA.
Biomarker: maternal PUFA concentrations
Third-trimester maternal plasma samples were collected in sodium citrate vacutainers, processed the same day, and immediately placed into –80°C freezers for storage. Staff working with these samples received annual biosafety training, took precautions such as personal protective equipment, and followed laboratory safety standards. The sample aliquots of 100 µL were then shipped to the analytical lab OmegaQuant (Sioux Falls, South Dakota), which is CLIA (Clinical Laboratory Improvement Amendments) certified (number: 43D1105229). As previously described (Harris, Varvel, Pottala, Warnick, & McConnell, 2013; Jimenez et al., 2015), internal standard (C17:0 or C23:0 in chloroform) was added to heparinized plasma samples, and vortex-mixing methods were used to extract fatty acids twice. After centrifugation, the chloroform extract was combined, dried, and then used BF3 in methanol to hydrolyze and methylate to fatty acid methyl esters. Samples were extracted twice with n-hexane and quantitatively measured by a capillary GC2010 Gas Chromatograph (Shimadzu, Japan). PUFA concentrations were identified by comparison with a standard mixture of fatty acids characteristic of plasma (GLC 727, NuCheck Prep, Elysian, Minnesota), which were also used to determine individual PUFA response factors. Five PUFA plasma concentrations (mg/L) were sent back to us and included in this study, including LA, ALA, AA, EPA, and DHA.
Questionnaire: maternal supplemental PUFA intake
As described in more detail elsewhere (Hertz-Picciotto et al., 2018), trained interviewers obtained data on omega-3 supplementation via telephone calls with the mother. She was asked whether or not each item had been consumed, and if so, what brand and dose had been consumed, how frequently, and in which months (first month of pregnancy and continuing throughout each month of gestation) the supplement was taken. Based on this information, we calculated average daily intake for each product and summed all values to a total omega-3 supplementation amount per month (100 mg/day, first to ninth month or end of pregnancy) for each woman.
Statistical analyses
Descriptive and univariable analyses were conducted to summarize maternal PUFA intake, child outcomes, and demographic characteristics. When examining associations between maternal PUFAs and diagnosis of ASD or non-TD, we first investigated maternal PUFA intake collected from the FFQ questionnaire during the first and second half of pregnancy in relation to risk of ASD or non-TD in children, including total omega-3, omega-6, DHA, EPA, ALA, AA, and LA. Second, we explored relationships between maternal PUFA plasma concentrations in the third trimester, including DHA, EPA, ALA, AA, and LA, and risk of ASD or non-TD in the offspring; for these analyses, we report relative risk for 10 mg/l increase in maternal PUFA plasma concentration. Sensitivity analyses were also conducted for PUFA plasma samples in the third trimester with no previous thaws. Finally, we evaluated associations between maternal omega-3 supplementation from the first to ninth month during pregnancy and risk of ASD or non-TD in the offspring.
Potential confounders were those who had been reported to be associated with either ASD or non-TD in previous publications. Demographic variables included maximum education in the household (categorized as either “some college or less,” “bachelor’s degree,” or “graduate or professional degree” (i.e. MD, DDS, and DVM)), maternal pre-pregnancy body mass index (BMI) (categorized as either “normal and underweight” (<25 kg/m2), “overweight” (25–30 kg/m2), or “obese” (>30 kg/m2)), mom’s race (categorized as either “white” or “non-white”), maternal age (years), paternal age (years), and gestational age (days) at delivery and at sample collection. We also considered other maternal nutrition intake factors from both dietary intake and supplement during the same pregnancy period as each exposure of interest, including total energy intake (kcals), dietary folate equivalents (DFE) intake (mcg), iron intake (mg), calcium intake (mg), magnesium intake (mg), vitamin B1 intake (mg), vitamin B2 intake (mg), vitamin C intake (mg), vitamin E intake (mg), vitamin B6 intake (mg), vitamin A intake (mcg), vitamin B12 intake (mcg), vitamin K intake (mcg), folic acid supplement (yes/no), calcium supplement (yes/no), vitamin C supplement (yes/no), vitamin E supplement (yes/no), vitamin B6 supplement (yes/no), vitamin A supplement (yes/no), and vitamin B12 supplement (yes/no). Moreover, to account for sample quality, we also examined laboratory variables, including sample numbers of thaws (categorized as either “0” or “⩾1”) and storage time (days).
Multinomial logistic regression was used to examine associations between maternal PUFAs and diagnosis of ASD or non-TD outcome relative to TD. Since our exposures were from different sources, model building was carried out separately for each exposure of interest to ensure correct confounders in final models. Bivariate analyses examined unadjusted associations of potential confounders with each outcome (ASD or non-TD) and each exposure of interest separately to identify those that were broadly associated (p < 0.3). Then, multivariable models were built, separately for ASD and non-TD risk, via adding 1 variable at a time to the multinomial logistic model and retaining those that caused at least a 10% change in the exposure parameter estimates. This approach led to final models that included different confounders for different exposures. Five variables met our model selection criteria across all models, including maternal food iron intake (exposures: dietary omega-3 intake, omega-6 intake, LA intake, ALA intake, LA plasma concentration, and ALA plasma concentration), gestational age at delivery (exposures: ALA plasma concentration), specimen number of thaws (exposures: all plasma concentration), sample storage time (exposures: AA, EPA, and DHA plasma concentration), and paternal age (exposures: EPA plasma concentration, supplemental omega-3 intake). After selecting final models, multivariable adjusted relative risk (RR) (with 95% confidence intervals (CIs)) for ASD and non-TD were calculated directly using SAS macro %RELRISK9 (Wacholder, 1986). All analyses were carried out using SAS version 9.4 (SAS Institute Inc., Cary, North Carolina). Tests were two-sided, with α = 0.05.
Results
In all, 258 (57 ASD, 62 non-TD, and 139 TD) mother–child pairs were eligible for the study and had maternal supplemental PUFA intake information. Among them, 32 (56%) ASD, 33 (53%) non-TD, and 82 (59%) TD reported the FFQ questionnaire on maternal PUFA dietary intake in the first half of pregnancy, while 30 (52%) ASD, 31 (50%) non-TD, and 70 (50%) TD had these information in the second half of pregnancy. In addition, 218 (84%) participant pairs also had information on maternal plasma PUFA concentrations in the third trimester, including 50 (88%) ASD, 52 (84%) non-TD, and 116 (83%) TD.
Characteristics of mother and child pairs are shown in Table 1. Children with ASD were significantly more likely to have longer gestational age (p = 0.0002), and their mothers’ plasma samples were stored for shorter periods (p = 0.02). Mothers with ASD children had borderline significantly lower iron intake from food in the second half of pregnancy than mothers of TD children (p = 0.06), but their total energy intake was not significantly different. Mothers of non-TD children were more likely to be non-white, compared to those of TD children (p = 0.04).
Demographic and clinical characteristics of children and their mothers.
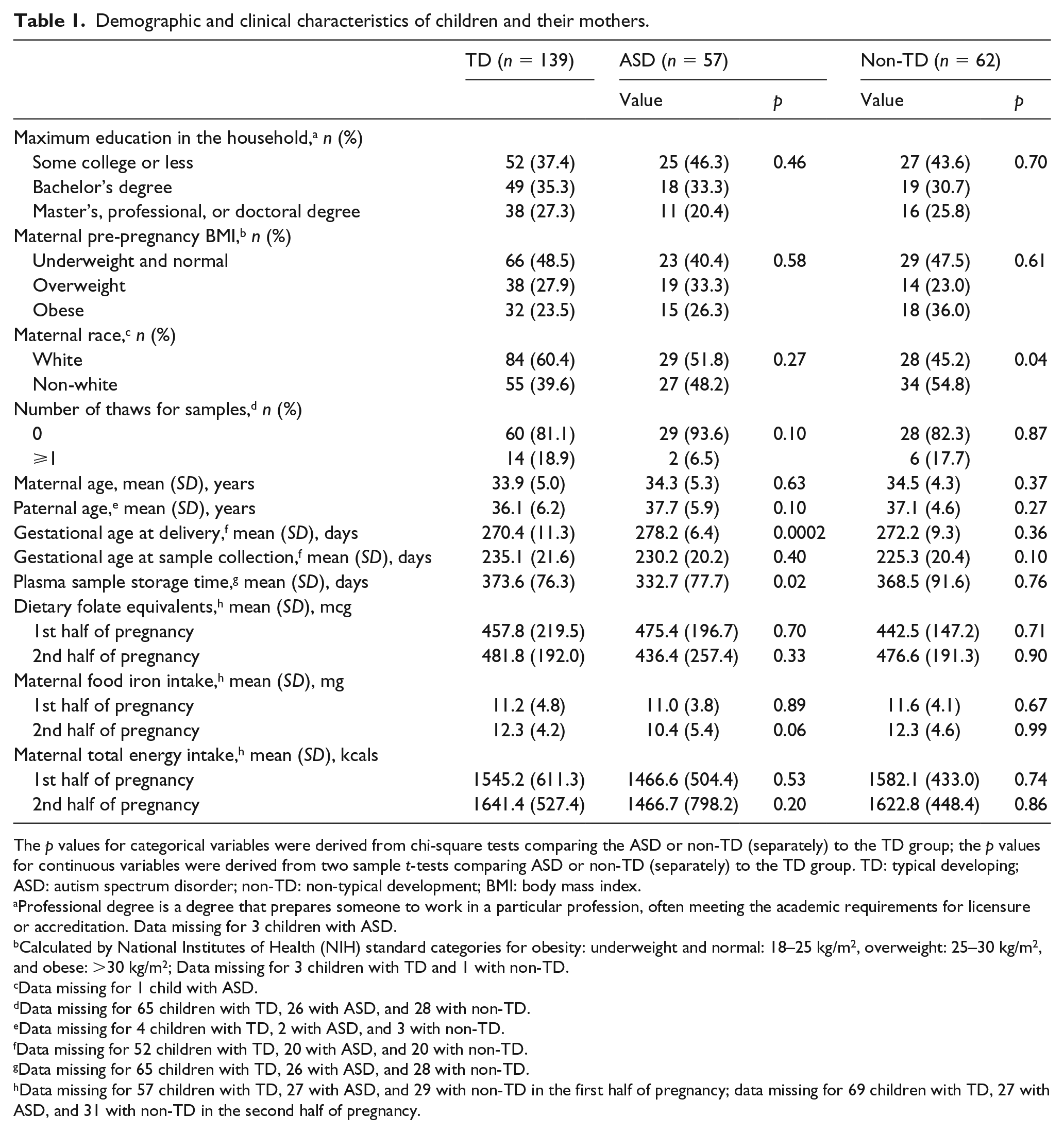
The p values for categorical variables were derived from chi-square tests comparing the ASD or non-TD (separately) to the TD group; the p values for continuous variables were derived from two sample t-tests comparing ASD or non-TD (separately) to the TD group. TD: typical developing; ASD: autism spectrum disorder; non-TD: non-typical development; BMI: body mass index.
Professional degree is a degree that prepares someone to work in a particular profession, often meeting the academic requirements for licensure or accreditation. Data missing for 3 children with ASD.
Calculated by National Institutes of Health (NIH) standard categories for obesity: underweight and normal: 18–25 kg/m2, overweight: 25–30 kg/m2, and obese: >30 kg/m2; Data missing for 3 children with TD and 1 with non-TD.
Data missing for 1 child with ASD.
Data missing for 65 children with TD, 26 with ASD, and 28 with non-TD.
Data missing for 4 children with TD, 2 with ASD, and 3 with non-TD.
Data missing for 52 children with TD, 20 with ASD, and 20 with non-TD.
Data missing for 65 children with TD, 26 with ASD, and 28 with non-TD.
Data missing for 57 children with TD, 27 with ASD, and 29 with non-TD in the first half of pregnancy; data missing for 69 children with TD, 27 with ASD, and 31 with non-TD in the second half of pregnancy.
In the second half of gestation, maternal mean dietary intake of total omega-3 (unit: gm/day) in mothers of children with ASD (1.2, SD = 0.7) was significantly lower than in those of children with TD (1.5, SD = 0.6, p = 0.04). After adjusting for confounders, this association was still evident (RR: 0.6, 95% CI: 0.3–0.98) (Table 2). However, no other statistically significant associations were found for all other PUFA subtypes intake during both the first and second half of pregnancy (Table 2).
Unadjusted and adjusted associations of maternal PUFA dietary intake (gm/day) during pregnancy with child outcome.
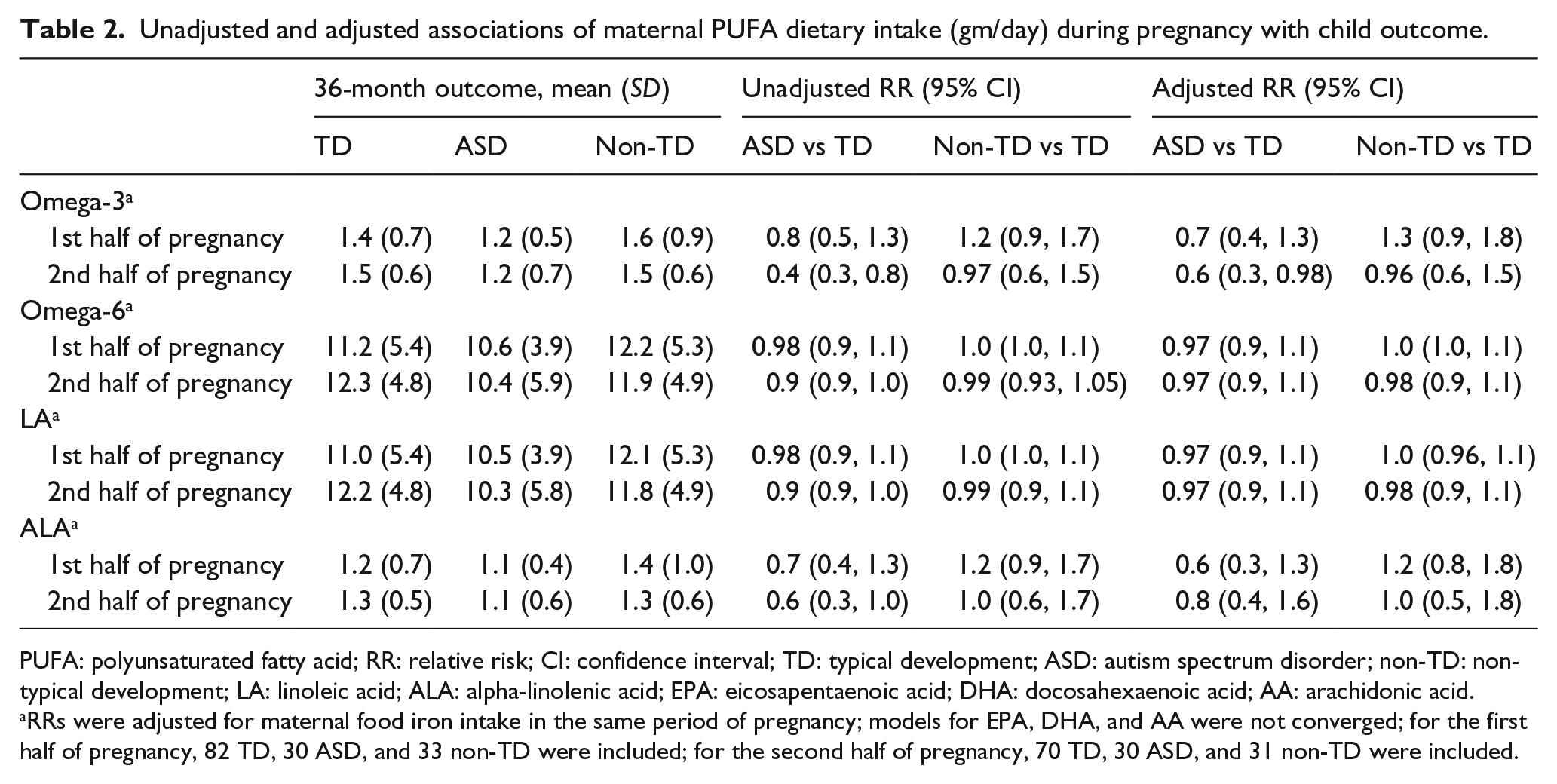
PUFA: polyunsaturated fatty acid; RR: relative risk; CI: confidence interval; TD: typical development; ASD: autism spectrum disorder; non-TD: non-typical development; LA: linoleic acid; ALA: alpha-linolenic acid; EPA: eicosapentaenoic acid; DHA: docosahexaenoic acid; AA: arachidonic acid.
RRs were adjusted for maternal food iron intake in the same period of pregnancy; models for EPA, DHA, and AA were not converged; for the first half of pregnancy, 82 TD, 30 ASD, and 33 non-TD were included; for the second half of pregnancy, 70 TD, 30 ASD, and 31 non-TD were included.
All maternal fatty acid concentrations in the third-trimester plasma were similar among mothers of children with ASD or TD in both unadjusted and adjusted multivariable analyses (Table 3). However, after adjusting for confounders, higher maternal EPA (RR = 0.47, 95% CI: 0.24–0.91) and DHA (RR = 0.88, 95% 0.78–0.99) plasma concentrations were significantly associated with lower risk of non-TD in the children (Table 3). In sensitivity analyses restricted to PUFA samples with no previous thaws (ASD: 29, Non-TD: 28, TD: 60), we did not observe similar significant results (see the Supplemental material S1).
Unadjusted and adjusted associations of maternal PUFA plasma concentration (mg/L) in the third trimester of pregnancy with child outcome.

Included were 116 TD, 50 ASD, and 52 non-TD. PUFA: polyunsaturated fatty acid; RR: relative risk; CI: confidence interval; TD: typical developing; ASD: autism spectrum disorder; non-TD: non-typical development; LA: linoleic acid; ALA: alpha-linolenic acid; AA: arachidonic acid; EPA: eicosapentaenoic acid; DHA: docosahexaenoic acid.
RRs were adjusted for maternal food iron intake and sample numbers of thaws; RR are reported for 10 mg/l increase in maternal PUFA plasma concentration.
RRs were adjusted for maternal food iron intake, gestational age at delivery, and sample numbers of thaws; RR are reported for 10 mg/l increase in maternal PUFA plasma concentration.
RRs were adjusted for sample numbers of thaws and sample storage time; RR are reported for 10 mg/l increase in maternal PUFA plasma concentration.
RRs were adjusted for paternal age, sample numbers of thaws, and sample storage time; RR are reported for 10 mg/l increase in maternal PUFA plasma concentration.
Finally, there were no significant associations between average intake of supplemental omega-3 from vitamins and supplements (100 mg/day) during pregnancy (first to ninth month) and risk of ASD (RR ranging from 0.92 to 0.99) or non-TD (RR ranging from 0.98 to 1.00) after adjusting for confounders, including paternal age (see Supplemental material, S2).
Discussion
In our study, we found that higher maternal total omega-3 intake in the second half of pregnancy was statistically associated with 40% lower risk of ASD in the child. However, intake of PUFA subtypes, including LA and ALA, were not statistically associated with risk of ASD in both the first and second half of pregnancy, even after adjusting for confounders. The lack of significant associations was also observed in plasma measures of PUFA subtypes in the third trimester, which might also suggest protective effects of total omega-3 instead of their subtypes on child risk of ASD. The total amount of omega-3 collected by the FFQ contained other fatty acids, such as docosapentaenoic acid and stearidonic acid, which were not measured in the plasma of this study. However, the limited statistical power to detect small effect sizes in this study could also have contributed to the lack of associations observed for omega-3 in plasma, given the associations observed for omega-3 subtypes in late pregnancy were in the same direction as that of total omega-3. In addition, our study confirmed relationships from general population studies between higher maternal DHA and EPA concentrations in the late pregnancy and reduced risk for non-TD in a high-risk ASD younger sibling population.
Taking purified fish oil supplements during pregnancy is recommended by some physicians (Genuis & Schwalfenberg, 2006). Our findings suggest that maternal omega-3 intake in the second half of gestation has a protective association with the child’s risk of ASD. Similar findings have been documented in a sub-cohort of the Nurses’ Health Study (NHS) II with 317 mother–child pairs, where researchers showed that children whose mothers had very low omega-3 consumption during pregnancy were associated with increased risk of ASD (Lyall et al., 2013) in the offspring. This study used the Willett FFQ to measure PUFA intake, which is different from our Block FFQ in several aspects, including food items and portion size; however, these two questionnaires have been demonstrated to have the similar capacity to predict diet–disease risk (Caan et al., 1998; Subar et al., 2001). We also observed that the second half of pregnancy appeared to be a critical time window for this association, which is consistent with previous evidence about the significant influence of PUFAs in the late pregnancy upon neurodevelopmental outcomes. For example, studies reported that the third trimester is a critical time for maternal DHA intake levels in relation to child cognitive development (Rees, Sirois, & Wearden, 2014). Previous studies have also reported that children whose mothers consumed cod liver oil (rich in omega-3) in late pregnancy had improved IQ and mental processing scores at 4 years old (Helland, Smith, Saarem, Saugstad, & Drevon, 2003; Willatts, 2002). Nevertheless, in our study, all other subtypes of maternal PUFA dietary and supplemental intake, such as DHA and EPA, were similar among mothers of children with ASD or TD within all time windows. Null findings were also observed in maternal plasma samples in the third trimester. These results are consistent with a study in the Norwegian mother and child cohort with 85,176 participants (Suren et al., 2013). Fish oil supplements (mainly EPA + DHA) consumed from 4 weeks before pregnancy to 8 weeks after pregnancy were reported to be not associated with risk of ASD in the children. Similarly, a randomized clinical trial with 726 mother–child pairs also observed that autism diagnoses did not differ in groups with or without prenatal DHA supplementation (Makrides et al., 2014). This could also be evidence for residual confounding, given intake may be related to other healthy behaviors.
The finding that there is an association between maternal omega-3 intake in late pregnancy and the likelihood of offspring’s risk of ASD is noteworthy. This relationship might be due to biological effects of omega-3 fatty acids on brain development. Omega-3 fatty acids occupy 20% of the brain’s dry weight (Bourre et al., 1991; Freeman et al., 2006), and previous animal studies indicate that they have potential therapeutic effects on ASD symptoms as well as other cognitive and behavioral capacities (Davis-Bruno & Tassinari, 2011; Neuringer, Connor, Lin, Barstad, & Luck, 1986). Since omega-3 fatty acids cannot be synthesized by the fetus and must be provided by placental transfer from the mother, prenatal intake is critical for brain development in later stages of gestation (Genuis & Schwalfenberg, 2006) and plays important roles in gene expression, signal transduction, and as components of cell membranes (Casper, 2004; Deckelbaum, Worgall, & Seo, 2006). Animal studies have also shown that omega-3 fatty acid deprivation during pregnancy was associated with behavioral deficits, which could not be reversed with postnatal supplementation (Nesheim, 2007). Moreover, omega-3 fatty acids are anti-inflammatory precursors (Green, Orr, & Bazinet, 2008) and may be able to counter damage from neuroinflammation, which has been demonstrated in some individuals with ASD (Careaga, Van de Water, & Ashwood, 2010; Onore, Careaga, & Ashwood, 2012).
Several limitations of the FFQ dietary data should be considered when interpreting our findings. First, since FFQ is a self-administrated questionnaire with a fixed list of foods, the reported amount may be underestimated if the individual consumed food items that were not on the list. For example, although salmon is a primary contributor to the omega-3 fatty acid intake, salmon consumption was not specifically asked in this FFQ version. However, this information might have been captured by the “Other fish. Not fried” question. Second, although the FFQ asked participants to report portion sizes, individuals may not be able to describe and conceptualize food sizes accurately, and substantial within-person variation may exist (Haraldsdottir, Tjonneland, & Overvad, 1994). Under these circumstances, non-differential misclassification might have occurred, which could have weakened the observed associations, especially for specific subtypes of PUFAs (Willett, 1998).
Our study is also the first of which we are aware to investigate maternal PUFA plasma concentrations in the third trimester and risk of ASD or non-TD in the child. Even though our findings of null associations between plasma PUFA subtypes and ASD are consistent with our questionnaire results that also show null associations, we should still interpret the plasma findings with caution due to differences in these two methods. First, plasma PUFA concentrations may not be highly correlated with the FFQ dietary intake. Plasma is a sensitive marker of short-term changes in fatty acid intake (Harris & Thomas, 2010) and easily affected by food intake changes across seasons or even throughout the courses of a single day. FFQs, on the other hand, were completed for the entire second half of pregnancy in our study, thus representing a longer period than the plasma samples which were specifically collected in the third trimester and represented episodic status. Moreover, because the 2–4 weeks within the trimester represented by our plasma measurement differed across individuals, it could have averaged out and thus muddied our exposure measurement and comparisons within the trimester. This would attenuate our ability to find differences by adding non-differential bias toward the null. In addition, total omega-3 plasma concentrations were also lacking in our study. Future studies with this information should be conducted to replicate our questionnaire findings.
In this prospective cohort study, detailed information on demographic factors, medical conditions, maternal nutrient intake during pregnancy, and laboratory information were systematically collected and examined as potential confounders. However, limitations of the study design still should be noted while interpreting our results. First, this study was conducted in a high-risk cohort of families affected by ASD; therefore, our findings might not be generalizable to the general U.S. population. Second, we only measured third-trimester plasma PUFA concentrations, because late pregnancy was hypothesized to be the critical window for these relationships based on results from previous studies of other neurodevelopmental outcomes (Denomme et al., 2005; Greenberg et al., 2008; Jacobson et al., 2008; Jensen, 2006). However, we acknowledge that critical windows could still differ across neurodevelopmental disorders with unique etiologies. We did not assess plasma PUFA in early pregnancy, which could be a critical period for ASD development (Levine et al., 2018; Lyall et al., 2014). In addition, we did not have information on fish contaminants including mercury. While mercury is a common contaminant of fish, one of the main sources of PUFAs, Modabbernia, Velthorst, and Reichenberg (2017) recently reviewed and suggested that mercury might also be a risk factor for ASD development, revealing both direct and indirect effects. Thus, it is possible that mercury and other fish contaminants might be potential and uncontrolled confounders in our analyses.
Conclusion
In summary, this prospective study of high-risk younger sibling pregnancies provides evidence for an association between higher maternal total omega-3 fatty acid intake in the second half of pregnancy and reduced risk of ASD in the offspring. However, no statistically significant associations are observed for all other PUFA subtypes from both self-reported questionnaires and third-trimester plasma. Future studies with larger sample size, mercury measurement, and measures at different time during pregnancy should seek to replicate these findings.
Supplemental Material
AUT877792_Supplemental_material – Supplemental material for Maternal polyunsaturated fatty acids and risk for autism spectrum disorder in the MARBLES high-risk study
Supplemental material, AUT877792_Supplemental_material for Maternal polyunsaturated fatty acids and risk for autism spectrum disorder in the MARBLES high-risk study by Yunru Huang, Ana-Maria Iosif, Robin L Hansen and Rebecca J Schmidt in Autism
Footnotes
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Environmental Protection Agency Science to Achieve Results (STAR) (grant number RD-83329201) and National Institutes of Health (grant numbers R01ES025574, P01ES011269, P50MH106438, and R01ES020392).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.