
Abstract
Autistic traits are associated with frequent psychological distress, suicidal ideation, and everyday functional challenges. These associations may be especially prominent in women. Some women with autistic traits “camouflage” feelings of awkwardness in typical social situations by effortfully engaging in expected social behaviors. We explored camouflaging because emerging evidence posits an association between camouflaging behaviors and poorer outcomes related to mental health, daily functioning, and access to mental health care. We recruited a sample of 58 women (age M = 25 years; IQ M = 115) who reported that they find social situations confusing and who scored high on a measure of broad autistic traits (Broad Autism Phenotype Questionnaire score > 3). The majority of participants reported significant levels of psychological distress, suicidal ideation, and daily functioning difficulties. Regression models showed that camouflaging efforts (Camouflaging Autistic Traits Questionnaire) and autistic traits (Social Responsiveness Scale, Second Edition) modestly but significantly predicted psychological distress and functional challenges, respectively. In a subgroup of participants with high Camouflaging Autistic Traits Questionnaire scores, camouflaging scores were significantly associated with psychological distress and functional challenges. Camouflaging may help predict when clinicians should be concerned about higher mental health distress in autistic women and may be beneficial to measure as part of a comprehensive, multimethod assessment of mental health in women who report difficulties fitting into social situations.
Lay Abstract
Women who try to hide or “camouflage” their autistic traits are likely to report that they feel distressed, think of suicide, and/or struggle to function in everyday life. We asked 58 women with autistic traits to complete questionnaires about camouflaging and mental health. Most of these women did not have a formal diagnosis of autism, yet a majority reported that they camouflaged autistic traits, and a large majority reported significant mental health challenges. Some researchers have suggested that women with autistic traits are more likely than autistic men to experience mental health challenges because women may try more to “fit in” socially by camouflaging their autistic traits. Analyses showed that camouflaging was associated with feeling distressed (depressed, anxious, and/or stressed). For women who reported above-average levels of camouflaging, camouflaging was also associated with having thoughts about suicide and struggling to function in everyday life. Trying to camouflage autistic traits was associated with mental health challenges, regardless of whether those traits were very mild or more severe. The findings of this study may influence how mental health professionals evaluate and treat women with autistic traits.
There is growing concern that the mental health of many autistic women is poor, and perhaps worse than that of autistic men (e.g., Tint et al., 2017). Consistent with reported sex differences in mental health in the general population (Kessler et al., 2005), autistic females are more likely than autistic males to experience certain psychiatric concerns such as anxiety and depression (Lai et al., 2019; Mandy et al., 2012; Oswald et al., 2016; Solomon et al., 2012). Suicide rates among autistic women are reported to be much higher than in other clinical and non-clinical populations (Cassidy et al., 2014; Hirvikoski et al., 2019). And, in contrast to general population trends that show women are less likely than men to die by suicide (Hedegaard et al., 2018), autistic women are just as likely, if not more likely, to die by suicide as autistic men (Hirvikoski et al., 2016; Kirby et al., 2019). It is not well understood if and how internal distress and suicidality impact the daily functioning (e.g., performing work tasks, maintaining relationships, and engaging with the community) of autistic women (Howlin & Magiati, 2017; Kirby et al., 2016; Taylor et al., 2015); evidence from non-clinical and majority-male autistic samples suggests that the impact may be significant and negative (Katon, 2009; Wallace et al., 2016). To support the mental health of autistic women, there is an urgent need to better understand the factors that significantly impact their psychological distress, suicidality, and functional capacity.
One factor that may impact the mental health of autistic women is the severity of autistic traits. While few studies have recruited substantial samples of autistic women, studies of autistic individuals across the lifespan suggest that autism spectrum disorder is associated with increased risk for psychiatric concerns, such as anxiety, attention-deficit/hyperactivity, and affective disorders (Lai et al., 2019; Leitner, 2014; Lever & Geurts, 2016; Nylander et al., 2018; Stewart et al., 2006; White et al., 2009). Even mild, subclinical autistic traits (i.e., traits from the broader autism phenotype; Piven et al., 1997) are associated with increased prevalence of psychiatric concerns (e.g., Cassidy, Bradley, Shaw, & Baron-Cohen, 2018; Ingersoll & Hambrick, 2011; Nylander et al., 2018; Pine et al., 2008). Women with autistic traits may experience psychiatric concerns that are unrelated to those traits, of course, and the relationships between autistic traits and mental health concerns remain unclear (Bolton et al., 1998; Piven & Palmer, 1999).
Difficulty fitting in with neurotypical social situations may also contribute to mental health concerns. Such difficulty can lead to autistic women experiencing reduced support in their social networks, which in turn increases the likelihood of mental health concerns (see Howlin & Magiati, 2017). While some autistic women state that they are unconcerned by such social challenges, many others are keenly aware of these challenges and feel different, misunderstood, or lonely (Bargiela et al., 2016; Gotham et al., 2014). This may be especially true for undiagnosed autistic women who are more likely to attribute social challenges to personal traits rather than to traits shared with other autistic people, with the former often leading to poor self-concept and feelings of isolation, and the latter potentially leading to self-awareness and a sense of community (Hickey et al., 2018; Hurlbutt & Chalmers, 2002; Kanfiszer et al., 2017; Leedham et al., 2020; Portway & Johnson, 2005; Webster & Garvis, 2017).
Whether or not they have been previously diagnosed, autistic women and men often report attempting to “camouflage” themselves in social situations (Hull et al., 2019). Their camouflaging efforts may involve suppressing autistic tendencies and/or effortfully engaging in “typical” social behaviors (Hull et al., 2017). For example, to appear more typical, an autistic woman may avoid talking too much about a favorite topic or may practice looking at a conversation partner’s facial expressions before responding. Broadly speaking, camouflaging efforts themselves are typical social behaviors in that neurotypical adults report employing camouflaging strategies that are qualitatively similar to the strategies used by autistic women and men (Livingston et al., 2019). Adaptive camouflaging efforts may help autistic women fit in and avoid a range of social stressors associated with mental health concerns. For instance, a woman who consciously avoids talking excessively about topics of special interest may be more likely to make and keep friends, and a woman who effortfully makes eye contact and carefully evaluates a conversation partners’ facial expressions may be more likely to interview well and obtain employment. Camouflaging may also produce less-tangible benefits. One qualitative study quoted an autistic woman who shared that she feels camouflaging is rewarding for her because she “[shows people] that autistic people can have people skills and be good role models” (Hull et al., 2017). The numerous short- and long-term benefits of camouflaging efforts reinforce the behavior and make future efforts more likely.
Despite the advantages of successful camouflaging, camouflaging efforts may also contribute to poor mental health, and the relationship between camouflaging efforts and mental health in autistic women is of interest for several reasons. First, while camouflaging is not unique to autistic women, it seems to be especially common among them (Cassidy, Bradley, Shaw, & Baron-Cohen, 2018; Hull et al., 2020; Schuck et al., 2019). Second, women who camouflage often report that they experience mental health concerns such as low self-esteem, stress, exhaustion, anxiety, and depression (Cage & Troxell-Whitman, 2019; Milner et al., 2019). Therefore, camouflaging may partly explain the prevalence of internalizing disorders and suicidality in autistic women. Third, camouflaging may also partly explain why autistic women are diagnosed with autism later, on average, than their male counterparts (Begeer et al., 2013). For some women, social challenges may outstrip camouflaging abilities only later in life (Giarelli et al., 2010). Also, just as a depressed patient who presents a smile may not be referred for treatment (despite significant internal distress), an autistic woman who successfully camouflages and presents as socially competent may not be referred for clinical assessment. Fourth, while interventions for autistic adults potentially ameliorate distress and support successful functioning (Jones et al., 2014), many interventions encourage camouflaging behaviors that may perpetuate distress.
Although camouflaging is theoretically associated with mental health benefits and risks, investigations of the relationship between camouflaging and mental health in autistic women have yielded mixed but generally negative associations. One study of combined autistic men and women showed that autistic men (n = 30) who manifested camouflaging were more likely to report depression (r = 0.3), but camouflaging among autistic women (n = 30) was not associated with depression (Lai et al., 2017). However, another study (N = 306; approximately 1/3 men) showed significant associations between self-reported camouflaging and symptoms of depression and anxiety (Hull et al., 2019). Another recent study of autistic adults (N = 262; 52% women) reported that individuals who camouflage inconsistently across contexts (e.g., camouflage at work but not in less formal contexts) experience greater psychological distress (Cage & Troxell-Whitman, 2019). Regarding suicidality, some research suggests that camouflaging may play a role (Camm-Crosbie et al., 2019; Cassidy, Bradley, Shaw, & Baron-Cohen, 2018; Kirby et al., 2019). Cassidy, Bradley, Shaw, and Baron-Cohen (2018) reported that, for autistic men and women (N = 164) who were first diagnosed in adulthood, self-reported camouflaging efforts were predictive of suicidality even after controlling for sex, depression, anxiety, age, and employment. Finally, camouflaging efforts may contribute to challenges in functioning well at work, home, and other contexts. A majority of autistic women with average intellectual functioning may struggle to secure or maintain full-time employment and so rely on extensive support from family (Engström et al., 2003; Howlin, 2000). To our knowledge, no study has directly investigated the relationship between camouflaging in women and everyday functional challenges.
Study aims
In response to calls to explore mental health concerns in autistic female samples that include undiagnosed autistic women (see Halladay et al., 2015; Livingston & Happé, 2017), we recruited a sample that included many women in a diagnostic “gray zone” who potentially are undiagnosed because of efforts to camouflage their autistic traits. All participants reported feeling awkward and confused in social situations. Approximately one third of participants had previous autism diagnoses (see Table 1). In this unique sample, we aimed to model psychological distress, suicidality, and daily functioning challenges as predicted by camouflaging behavior, while controlling for autistic traits.
Participant demographics.
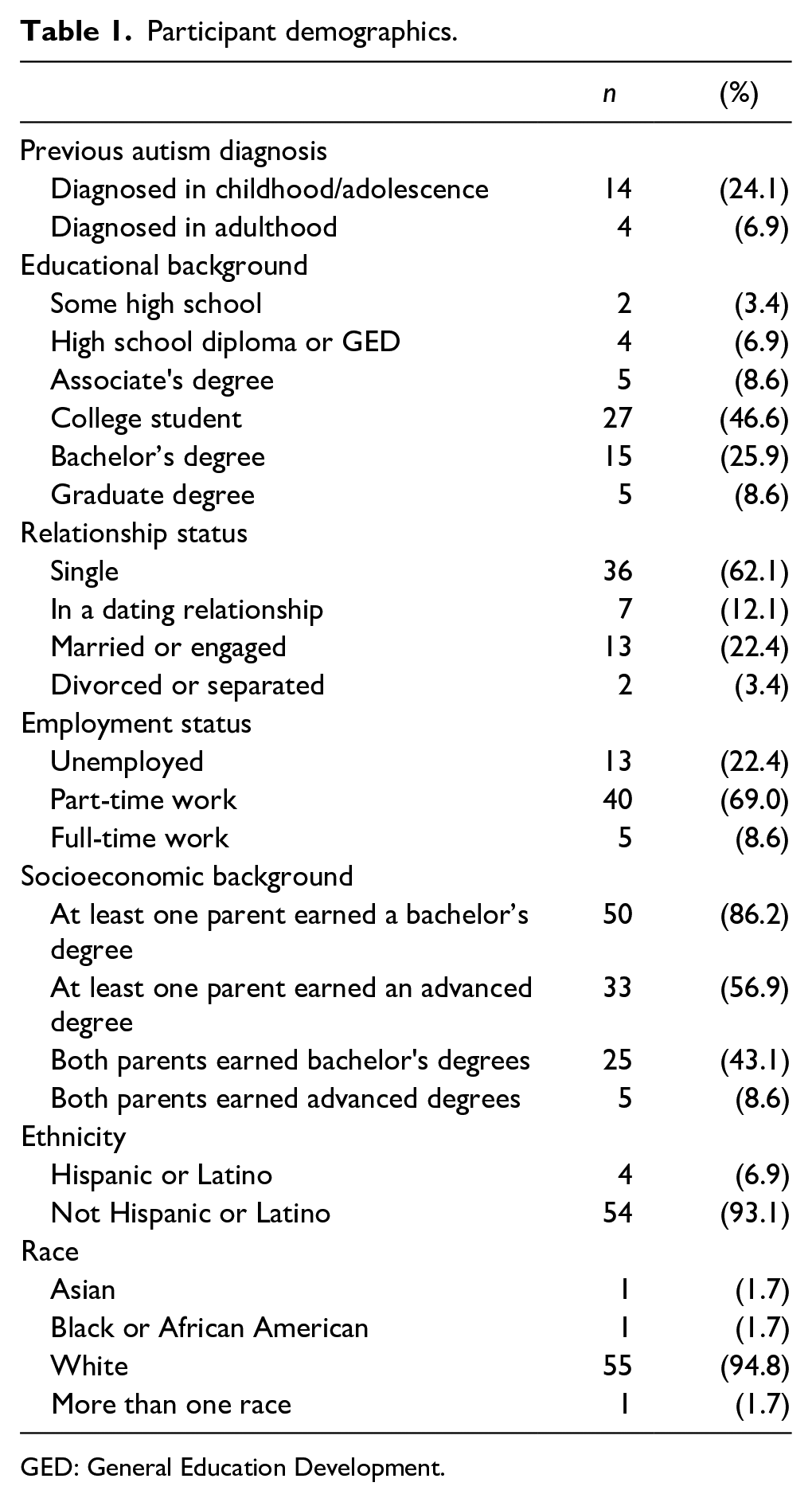
GED: General Education Development.
We specifically hypothesized that camouflaging efforts would significantly predict poor mental health even after accounting for clinician-rated autism severity and self-reported autistic traits. Our aim in seeking predictors of mental health in autistic women is to help clinicians know whom to reach out to and how to ease distress and improve functioning, perhaps by assessing and addressing problematic camouflaging.
Methods
Measures
Screening measure
The Broad Autism Phenotype Questionnaire (BAPQ; Hurley et al., 2007) is a 36-item self-report measure of autism-related traits (e.g., “I like being around other people”) with high inter-item reliability (Cronbach’s α = 0.95). We chose the BAPQ as a screening measure because, in contrast to other autism measures administered for this project, it was designed to be sensitive even to subclinical autistic traits. In the Hurley et al. (2007) validation sample (n = 150 women), using a total score cutoff of 3.25 yielded 75% sensitivity and 87% specificity for autistic personality traits in female relatives of autistic individuals. A more recent study (n = 18 women) used a lower total score cutoff of 3.17 and reported 33% sensitivity and 100% specificity for women (Sasson et al., 2013). In order to include all potential participants with significant autistic traits, we valued sensitivity over specificity and used a liberal cutoff of 3.0.
Psychological distress
The Depression Anxiety Stress Scales 21 (DASS-21; Lovibond & Lovibond, 1995) is the 21-item form of the 42-item self-report DASS. The DASS-21 invites respondents to rate their experience of seven symptoms each of depression, anxiety, and stress over the past week. The DASS-21 total score is a valid measure of general psychological distress with high inter-item reliability (Cronbach’s α = 0.93; Henry & Crawford, 2005).
Suicidality
The Suicidal Behavior Questionnaire–Revised (SBQ-R; Osman et al., 2001) is a brief, four-item self-report measure of suicidal behavior that has been validated in clinical and non-clinical samples. Two items assess lifetime incidence of suicidal ideation, threats, and attempts; one item assesses suicidal ideation over the past year; and one item assesses the probability of future attempts. For the future-oriented item (“How likely is it that you will attempt suicide someday?”), two of the six response options are similar: “Never” and “No chance at all.” With the approval of Augustine Osman, PhD, one of the measure’s authors, we changed the wording of these response options to “Never thought about suicide” and “Thought about suicide, but no chance at all.” For a non-clinical, undergraduate sample, a total cutoff score of seven differentiates well between those at risk for suicide and non-suicidal adults, with sensitivity of 93% and specificity of 95%. The SBQ-R has not yet been validated in an adult autistic sample, but neither has any other suicide screening measure (Cassidy, Bradley, Bowen, et al., 2018).
Functional challenges
The World Health Organization Disability Assessment Schedule, Second Edition (WHODAS 2.0; Üstün, 2010) uses 12 face-valid questions to measure disability or dysfunction in six areas: cognition, mobility, self-care, getting along, life activities (e.g., “taking care of household responsibilities”), and community participation. The respondent rates how much difficulty (ranging from “None” to “Extreme or Cannot do”) has been caused by health conditions over the past 30 days for each of the 12 tasks. The measure explicitly includes “mental or emotional problems” that are “short or long lasting” in its definition of health conditions. Before being entered into regression models, total scores reflecting percent decreased functioning were multiplied by 100 for ease of interpretability (i.e., a score of 100 means the respondent cannot do any of the 12 activities). The 12-item version of the original 36-item assessment, the WHODAS 2.0 explains 81% of the variance of the 36-item version, has excellent test–retest reliability (intra-class coefficient of 0.98), and has been validated in autistic adults without intellectual disability (Park et al., 2019).
Clinician-rated autistic traits
The Autism Diagnostic Observation Schedule, Second Edition, Module 4 (ADOS-2; Lord et al., 2012) is a valid and reliable instrument that is internationally recognized as the gold-standard diagnostic measure for adolescents and adults with ASD (Gotham et al., 2006). Due to its superior sensitivity (90.5%) and specificity (82.2%), we used the revised algorithm to classify participants as autistic or not (Hus & Lord, 2014). The examiners all had received formal clinical ADOS-2 training and were supervised by clinicians who have attained ADOS-2 research reliability. ADOS-2 administrations were video recorded, and 86% were scored by a second clinician. Raters achieved mean inter-rater reliability of 0.88 across all items.
Self-reported autistic traits
The Social Responsiveness Scale, Second Edition, Adult Self-Report (SRS-2; Constantino, 2012) is a 65-item self-report questionnaire that asks respondents to consider their behavior over the past 6 months and rate the presence of a variety of autistic traits, including social communication deficits, restricted interests, and repetitive behaviors. Mandell et al. (2012) reported that a cut score of > 84 (raw total score), which is interpreted within a moderate-to-severe severity range, maximized specificity (0.60) and sensitivity (0.86). Test–retest correlations range from 0.88 to 0.95, and across parents, spouses, and relatives, inter-rater reliability coefficients range from 0.61 to 0.92 (Bruni, 2014).
The Autism-Spectrum Quotient (AQ; Baron-Cohen et al., 2001) is a 50-item self-report measure of personal traits related to autism, such as social skills, attention switching, attention to detail, communication, and imagination. The authors reported good test–retest (r = .70) and inter-rater (no significant differences between adult- and parent-report) reliability (Baron-Cohen et al., 2001). A total score cutoff of > 32 distinguishes most male and female adults with autism from controls.
Camouflaging
The Camouflaging Autistic Traits Questionnaire (CAT-Q; Hull et al., 2019) is a 25-item self-report measure of social camouflaging behaviors (i.e., strategies used to compensate for or mask autistic characteristics to facilitate social assimilation). Unlike measures of camouflaging derived from behavioral observations, the CAT-Q measures both successful and failed camouflaging attempts based on intention. The CAT-Q was developed for online administration, and the normative sample included 354 autistic and 478 non-autistic adults (recruited through social media, a clinic, and word-of-mouth, similar to our sample). Internal consistency (α = 0.94) and test–retest reliability (r = 0.77) are acceptable. In the measure’s validation sample of autistic adults, the mean total score was 4.79 (SD = 0.99). The measure’s authors reported that autistic adults scored higher on the CAT-Q than non-autistic adults, and autistic females scored higher than autistic males (Hull et al., 2019, 2020).
IQ
The Wechsler Abbreviated Scale of Intelligence, Second Edition (WASI-II; Wechsler & Hsiao-Pin, 2011) is a valid, brief measure of IQ. We administered the two-scale full-scale IQ (FSIQ-2) which includes the Vocabulary and Matrix Reasoning subtests. The WASI-II has excellent psychometric properties, including test–retest reliability of 0.88 for FSIQ-2 in adults.
Procedure
All study procedures were approved by the university Institutional Review Board (IRB), and written consent was obtained for all participants in accord with the Declaration of Helsinki. This project was part of a larger series of studies that included additional self-report, behavioral, and parent-report measures detailed in the supplementary materials.
Women participants were recruited through university-based and private mental health clinics, social media, and an intense residential support program for autistic young adults. The recruiting flyer read, “In social situations, do you often find yourself confused, anxious, or exhausted?” An existing autism diagnosis was not required for participation. Interested participants initially completed self-report questionnaires using the Qualtrics online survey platform (Qualtrics, Inc., Provo, Utah), including BAPQ, SRS-2, DASS-21, and a custom questionnaire regarding demographic information, treatment history, and additional topics related to health and social history. Women with a BAPQ total score > 3.0 indicating the presence of autistic traits (3.0 is a liberal cutoff; see Sasson et al., 2013) were invited to our lab to complete an in-person assessment involving the WASI-II, ADOS-2, WHODAS 2.0, and SBQ. Following the assessment, researchers invited participants to complete the AQ and CAT-Q, also through Qualtrics. See Figure 1 for a summary of the sample formation process. Participants were compensated $10/hour for their participation in both online and in-person portions.
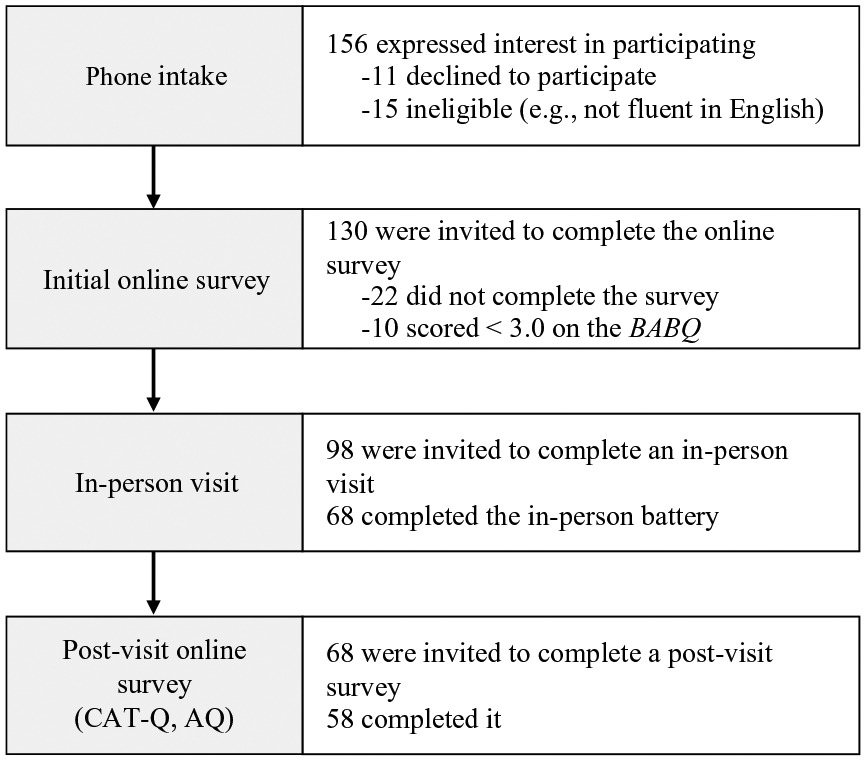
Summary of the process of sample formation.
Participants
The final sample reported here includes 58 adult women who completed all measures for this study. Participants had a mean age of 25.2 years (range: 18–42; SD = 6.17; see Table 2) and mean IQ of 114.60 (range: 89–140; SD = 11.27). All participants scored high on a measure of broad autistic traits (BAPQ score > 3). Eighteen participants (31%) had received a previous, formal diagnosis of autism spectrum disorder (autism or Asperger syndrome). Of these 18, 10 were diagnosed in childhood, 4 in adolescence, and 4 in adulthood. A majority of participants (63.8%) reported receiving a formal psychiatric diagnosis other than autism spectrum disorder, such as generalized anxiety disorder (39.7%), major depressive disorder (31.0%), or attention-deficit/hyperactivity disorder (17.2%; see Table 3). Most participants were White (94.8%), working part time (69.0%), and single or divorced (65.5%), and many were currently attending college (46.6%; see Table 1).
Participant characteristics.
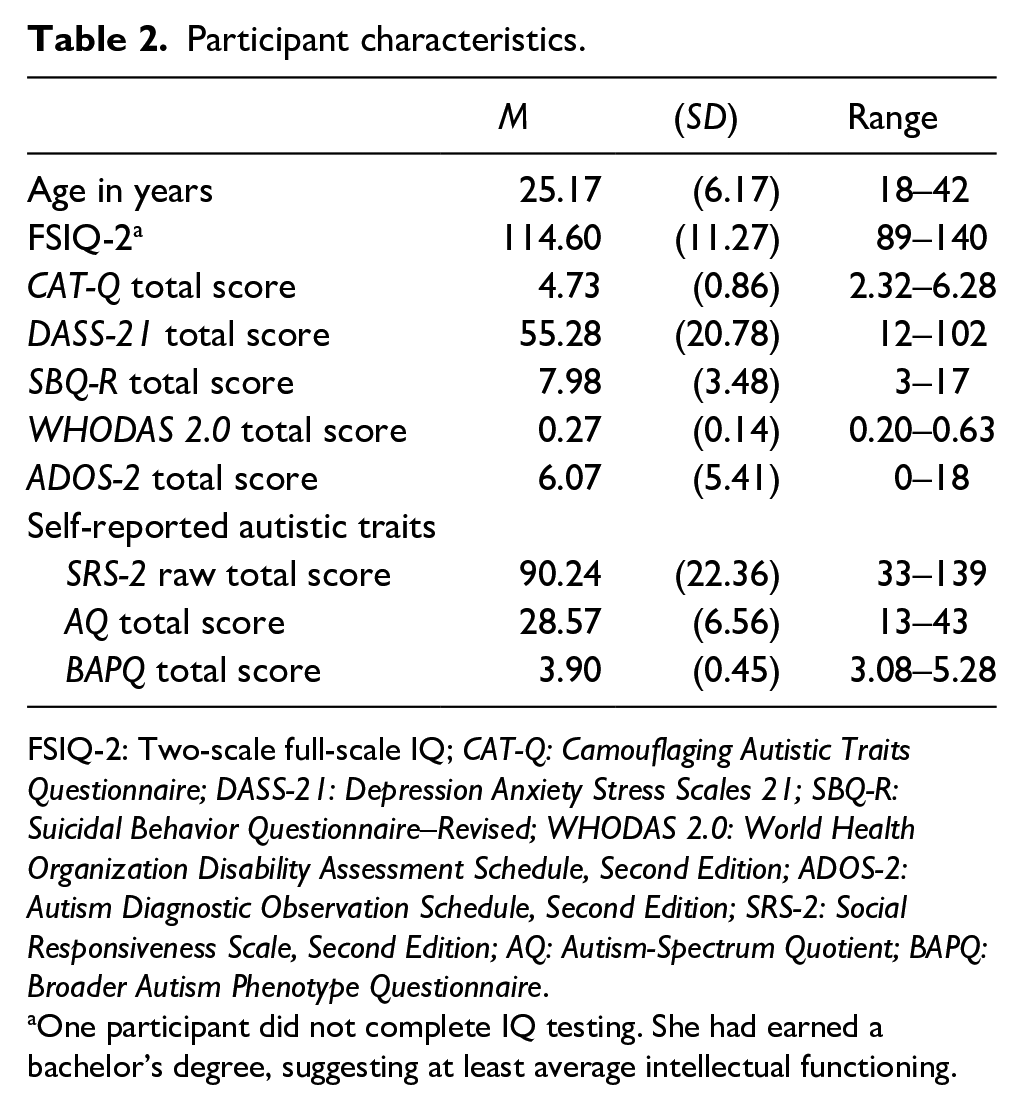
FSIQ-2: Two-scale full-scale IQ; CAT-Q: Camouflaging Autistic Traits Questionnaire; DASS-21: Depression Anxiety Stress Scales 21; SBQ-R: Suicidal Behavior Questionnaire–Revised; WHODAS 2.0: World Health Organization Disability Assessment Schedule, Second Edition; ADOS-2: Autism Diagnostic Observation Schedule, Second Edition; SRS-2: Social Responsiveness Scale, Second Edition; AQ: Autism-Spectrum Quotient; BAPQ: Broader Autism Phenotype Questionnaire.
One participant did not complete IQ testing. She had earned a bachelor’s degree, suggesting at least average intellectual functioning.
Participant-reported previous psychiatric diagnoses.
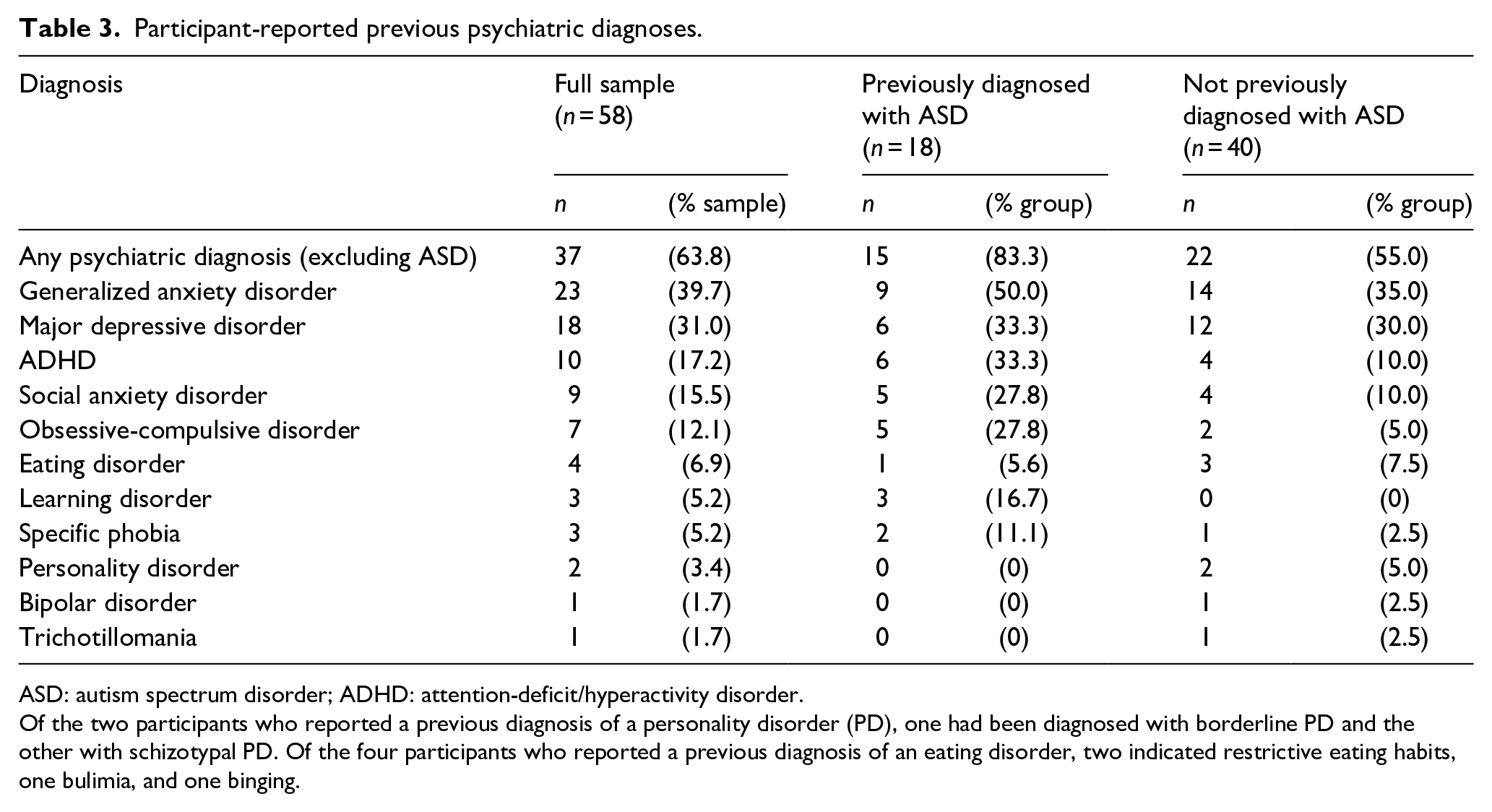
ASD: autism spectrum disorder; ADHD: attention-deficit/hyperactivity disorder.
Of the two participants who reported a previous diagnosis of a personality disorder (PD), one had been diagnosed with borderline PD and the other with schizotypal PD. Of the four participants who reported a previous diagnosis of an eating disorder, two indicated restrictive eating habits, one bulimia, and one binging.
Data analyses
We tested ordinary least-squares linear regression models of psychological distress (DASS-21), suicidality (SBQ-R), and functional challenges (WHODAS 2.0) with clinician-rated autistic traits (ADOS-2), insight into autistic traits (SRS-2, AQ), and camouflaging (CAT-Q) as potential predictor variables. To examine associations between entered dependent and predictor variables, we generated scatterplots to confirm linearity. Given the early stage of research about these constructs, we completed simultaneous (versus hierarchical) regressions. Since camouflaging might differentially predict distress depending on the level of severity of autistic traits (e.g., efforts to camouflage more severe traits may be more psychologically taxing), we entered interaction terms in regressions involving the relevant predictors. Before creating the product terms that represent interactions, we mean-centered the involved quantitative predictors (Warner, 2013). Centered scores were not entered as predictors. Shapiro–Wilk tests showed normality in the distributions of regression residuals (Thode, 2002), scatterplots of residuals against predicted/fitted variables did not show notable heteroscedasticity, and collinearity was not problematic as the variance inflation factors (VIF) for all variables was < 3 (O’Brien, 2007).
There were no missing data among analyzed variables. Before regression analyses, extreme scores were Winsorized to 5th and 95th percentile values (Dixon & Yuen, 1974). Re-analysis of un-Winsorized data did not significantly change our findings. Power analyses are reported in the supplementary materials. Statistical analyses were implemented using Stata version 15.1 (StataCorp, 2017). Deidentified data are available upon request.
Results
This sample of women with significant self-reported autistic traits reported considerable psychological distress. On the DASS-21, 62% reported moderate or severe depression, 67% reported moderate or severe anxiety, and 66% reported moderate or severe stress (Figure 2). According to the SBQ-R, 62% of participants were at risk for suicide. This distress comes alongside significant everyday functional challenges. Scores on the WHODAS 2.0 indicate that 57% rated themselves as functioning in a range of everyday activities at three-fourths or less of their full capacity, and 15% of that group rated themselves as functioning at half or less. Participants were most likely to report difficulty on WHODAS 2.0 items related to social tasks (e.g., “How much of a problem did you have in joining in community activities . . .?”) or emotional health (“How much have you been emotionally affected by your health problems?”).
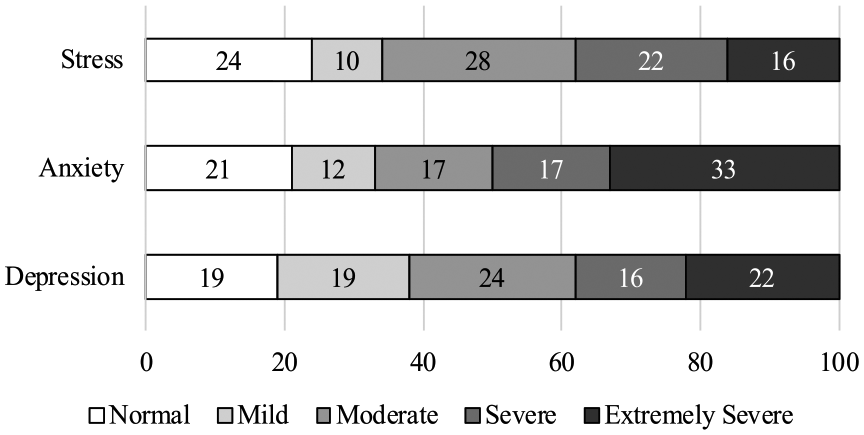
DASS-21 subscale scores — full sample (N = 58).
During the in-person assessment, many participants expressed their distress to examiners with comments such as “I’m more worried about making a [social] mistake than dying” or “I was tired of trying [to succeed socially] and making social mistakes, so I started avoiding people.” One participant who had a formal diagnosis of autism shared that she felt “ashamed” about her diagnosis. Another described how she was glad to receive a diagnosis, although it did not make social interactions easier: “I always wondered what was wrong with me. After my diagnosis, I realized nothing was wrong, things are just harder for me. It is nice to have a reason for things. Now I know it is not my fault.” Further evidencing their distress, 72% of participants had received psychotherapy, 74% had taken medication for mental health concerns, and 64% were receiving pharmacological or psychotherapy treatment at the time of their participation in the study.
On the CAT-Q, the present sample reported camouflaging to a degree very similar to that reported for the measure’s autistic validation sample, with 55% of the sample reporting camouflaging above the autistic sample’s mean. Of the three CAT-Q subscales, participants were most elevated on the masking subscale that assesses “strategies used to hide autistic characteristics or portray a non-autistic persona,” with 74% of the sample reporting masking above the autistic sample’s mean (see Table S1).
Regression analyses
We ran three regression models. A regression model of psychological distress (DASS-21 total scores) was statistically significant, F(6, 51) = 2.30, p = .048, and accounted for 12% of the variance in distress (see Table 4). The model showed that camouflaging efforts (CAT-Q total scores) significantly predict such distress in the sample (β = 0.29, p = .03), and self-reported autistic traits (SRS-2 raw total scores) approached significance as a predictor (β = 0.30, p = .06). A regression model of suicidality (SBQ-R scores) was not statistically significant, F(6, 51) = 1.43, p = 0.22. A regression model of daily functional challenges (WHODAS 2.0 total scores) was statistically significant, F(6, 51) = 2.56, p = 0.03, and accounted for 14% of the variance in such challenges. In this model, self-reported autistic traits (SRS-2 raw total scores) significantly predicted functional challenges in the sample (β = 0.33, p = .04), while camouflaging efforts (CAT-Q total scores) approached significance as a predictor (β = 0.24, p = .06). Neither clinician-rated autistic traits (ADOS-2 scores) nor self-reported autistic traits per the AQ significantly predicted any of the mental health measures. Interactions between self-reported autistic traits and camouflaging efforts were also not statistically significant in any model.
Linear regression models of mental health (N = 58).

Psychological distress = Depression Anxiety Stress Scales 21 total score; Suicidality = Suicidal Behavior Questionnaire–Revised total score; Functional challenges = World Health Organization Disability Assessment Schedule, Second Edition total score; ADOS-2: Autism Diagnostic Observation Schedule, Second Edition; SRS-2: Social Responsiveness Scale, Second Edition; AQ: Autism-Spectrum Quotient; CAT-Q: Camouflaging Autistic Traits Questionnaire.
Post hoc analysis of a high-camouflaging subgroup
Investigation of the scatterplots created before the regression analyses (see Figure S1) suggested that camouflaging might relate to measures of distress and functional challenges more strongly for participants who reported high levels of camouflaging versus those who reported low levels. Therefore, we used the reported mean CAT-Q total score of autistic adults in the validation sample (4.79) to split our sample into two groups: high-camouflaging (n = 32) and low-camouflaging (n = 26). Nine participants of the high-camouflaging subgroup (28%) had received autism diagnoses prior to their participation; 12 members of this group (38%) scored above autism cutoffs on the ADOS-2. We completed Doornik-Hansen omnibus tests to confirm bivariate normality in the relationships between CAT-Q total scores and each mental health measure (DASS-21, SBQ-R, WHODAS 2.0; Doornik & Hansen, 2008). We then calculated Pearson correlations between CAT-Q total scores and scores on the mental health measures, first in the high-camouflaging subgroup, and then in the low-camouflaging subgroup for comparison. In the high-camouflaging subgroup, CAT-Q total scores were significantly associated with each measure of mental health. In the low-camouflaging subgroup, CAT-Q total scores were not associated with any of the three measures of mental health (ps > 0.2; Table 5).
Correlations between CAT-Q total scores and mental health measures for high- and low-camouflaging subgroups.
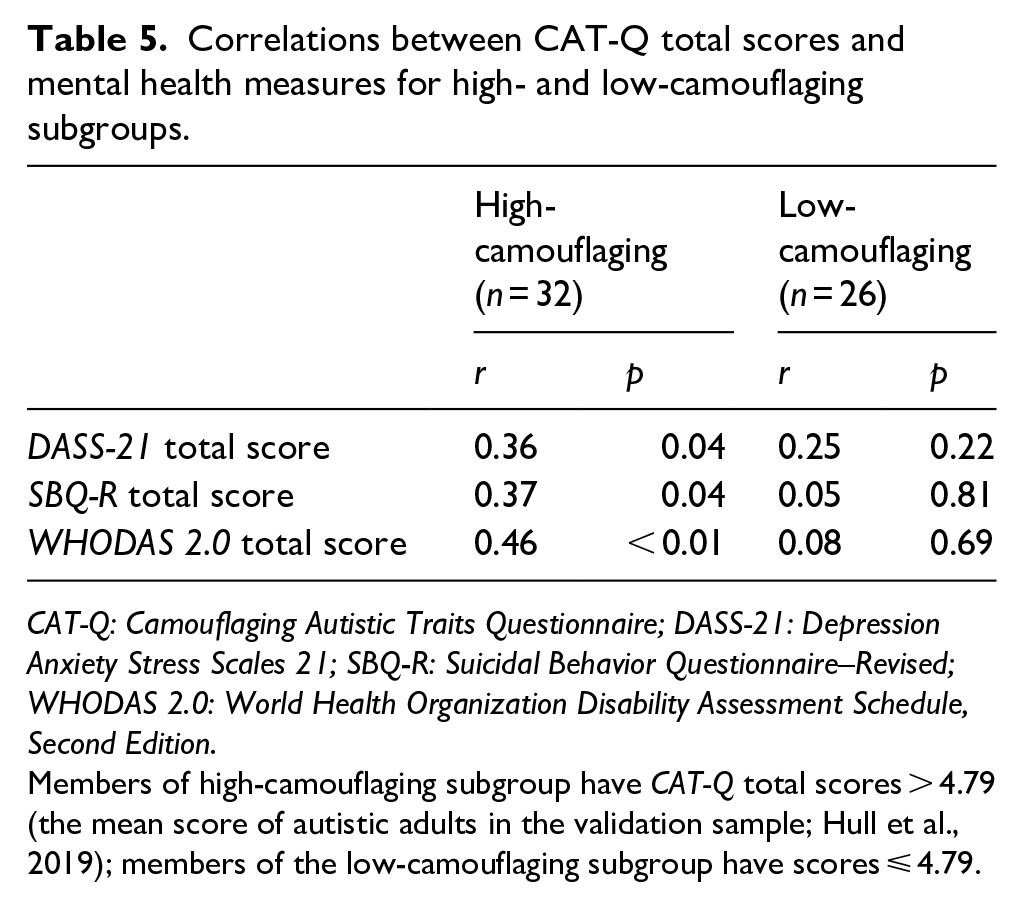
CAT-Q: Camouflaging Autistic Traits Questionnaire; DASS-21: Depression Anxiety Stress Scales 21; SBQ-R: Suicidal Behavior Questionnaire–Revised; WHODAS 2.0: World Health Organization Disability Assessment Schedule, Second Edition.
Members of high-camouflaging subgroup have CAT-Q total scores > 4.79 (the mean score of autistic adults in the validation sample; Hull et al., 2019); members of the low-camouflaging subgroup have scores ⩽ 4.79.
Post hoc analysis of subgroups based on diagnostic classification
We did not include diagnostic status as a binary independent variable in the regression models because we included ADOS-2 scores, and diagnostic status is conflated with these scores. However, we wondered whether participant characteristics varied significantly by ADOS-2 diagnostic classification. We completed t tests to compare the participants who scored above ADOS-2 cut score (revised Module 4 algorithm overall score ⩾ 8) with those who did not. On average, those who met ADOS-2 criteria for autism spectrum disorder were older by about 5 years. Otherwise, there were no significant differences on participant characteristics, including on the dependent variables in the regression analyses (i.e., DASS-21, SBQ-R, WHODAS 2.0). Group mean differences for non-normal variables (age, FSIQ-2, ADOS-2 total scores, SRS-2 total raw scores) were confirmed with Whitney–Mann U tests. Full results are reported in the supplementary materials (Table S2).
To explore whether participants’ scores on mental health measures (the dependent variables) varied systematically for participants who were autistic per other diagnostic measures, we classified participants for autism “caseness” by applying each tool’s published cut score or interpretive guideline: SRS-2 total scores in the Moderate range (total raw score > 84) and AQ scores ⩾ 32 were considered indicative of autism. A review of Table S3 shows there is no clear pattern between diagnostic stringency and average scores on the mental health measures. Interestingly, approximately 71% of the sample—including all participants previously diagnosed with autism—had scores in the range of severity consistent with autism on at least one measure, yet no single measure or combination of measures classified all previously diagnosed participants as autistic.
Measures of mental health and camouflaging were more strongly associated in a subgroup of women who did not have a diagnosis of autism (n = 40). In this group, CAT-Q total scores were significantly associated with psychological distress (DASS-21 total scores) and functional challenges (WHODAS 2.0 total scores); see Table S4.
Discussion
A majority of the sample of women with autistic traits reported significant psychological distress (depression, anxiety, and stress), suicidality, and reduced daily functioning. Self-reported camouflaging efforts (CAT-Q total scores) significantly predicted psychological distress while measures of autistic traits (ADOS-2, AQ, and SRS-2) did not. CAT-Q scores also showed a trend toward predicting functional challenges, and self-reported autistic traits (SRS-2 total scores) significantly predicted such challenges. For a subsample of participants with high CAT-Q camouflaging scores, CAT-Q scores were significantly associated with suicidality, in addition to psychological distress and reduced functioning. These strong associations between camouflaging and mental health in the high-camouflaging subgroup, in combination with the nonsignificant interactions between camouflaging efforts and self-reported autistic traits in the full-sample regression models, suggest that camouflaging’s relationship with mental health is linked to the degree of camouflaging effort and not to the severity of autistic traits being camouflaged.
Our findings echo results from adults diagnosed with autism as reported in Cassidy, Bradley, Shaw, and Baron-Cohen (2018) showing that self-reported suicidality (SBQ-R) was not associated with AQ scores. Furthermore, we partly replicated their finding that self-reported camouflaging (which they assessed using four brief questions) was significantly associated with suicidality (assessed using the SBQ-R) in women and men who reported a diagnosis of autism spectrum disorder. In our intentionally broader sample that included women with mild autistic traits, we found a significant association between camouflaging and suicidality only in participants who reported engaging in camouflaging behaviors to a high degree.
Evaluating mental health concerns in women with autistic traits
The high prevalence of mental health concerns in the present sample raises the question of whether these concerns are common among women with autistic traits, or autistic traits are common among women with mental health concerns, or both. What is clear from our results is that many women with symptoms of the broader autism phenotype are in significant distress. This finding emphasizes the importance of thorough, multimethod assessment of mental health concerns in women with autistic traits, especially as such concerns may mask or exaggerate autistic traits. For example, Gotham et al. (2018) found that autistic adults showed neural activity in response to emotional stimuli that seemed different from neurotypical peers, yet similar to depressed neurotypical peers. Their finding suggests that traits often attributed to autism (e.g., ruminative thoughts; Gotham et al., 2014) may be better explained by depression or other mental health concerns rather than by autism traits per se. Clinicians must carefully consider how mental health concerns affect presentation of autism symptoms, and vice versa. One important strategy for doing this is to listen carefully and thoroughly to the individual client (Crane et al., 2019).
To reiterate, the fact that an autistic woman is verbally fluent, has IQ in the average range or above, and seems to function well does not indicate that she is functioning well emotionally. Indeed, she may be in a significant amount of distress. It is important to properly assess all concerns because, for many, a proper diagnosis leads to greater self-acceptance, a sense of belonging in the autism community, and access to appropriate care, including support in managing suicidality, anxiety, and the many challenges inherent in navigating the neurotypical social space (Jones et al., 2014).
Camouflaging and mental health
Our findings suggest that camouflaging efforts are pervasive among women who perceive themselves as socially atypical, regardless of whether they have been or could be diagnosed as autistic. Our findings also suggest that assessing camouflaging efforts is clinically relevant because, although camouflaging behaviors may often be adaptive and facilitate social inclusion, they are significantly associated with psychological distress, even after accounting for severity of autistic traits. The direction of this association is unclear. Perhaps camouflaging efforts come about in response to feeling social isolation, low self-concept, and/or low self-acceptance, or perhaps vice versa. Notably, however, many women with autistic traits describe camouflaging efforts as having many negative consequences. For example, a qualitative investigation of camouflaging in a sample of women and men (N = 92; 60% women) reported themes regarding the long-term consequences of camouflaging that were all negative: “I fall to pieces,” “People have a stereotyped view [of me],” and “I’m not my true self” (Hull et al., 2017).
Our finding that camouflaging efforts are more associated with mental health concerns in undiagnosed women supports the idea that undiagnosed women may be more likely to feel different, misunderstood, or lonely, possibly because they are more likely to attribute social challenges to personal traits rather than lack of acceptance of one’s community or other factors (Bargiela et al., 2016; Hickey et al., 2018; Kanfiszer et al., 2017; Leedham et al., 2020). This finding is tentative due to the small sample size of formerly diagnosed autistic women, who did not show a similar correlation between camouflaging and psychological distress or functional challenges (Table S4), but who might also have mental health concerns associated with camouflaging.
Given growing evidence that camouflaging is generally associated with significant mental health concerns, clinicians who administer interventions that promote camouflaging efforts should consider whether these efforts are manageable and in line with the patient’s values (Camm-Crosbie et al., 2019; Crane et al., 2019). Clinicians who encourage camouflaging efforts might also consider arranging wraparound services (e.g., support groups to discuss possibly less desirable effects, social clubs that support autistic women in “being themselves”) to prevent possible mental health issues in the event camouflaging itself is a causal contributor to psychological distress.
Limitations and strengths
Our study has notable limitations. First, the all-female sample was relatively homogeneous in terms of age, cognitive ability, ethnicity, and socioeconomic background. Therefore, the findings may not generalize to children, individuals with intellectual challenges, people of color, or individuals who experience poverty or other significant psychosocial stressors unrepresented in this study. Second, the validity of findings may be impacted by mono-operation bias as several of the constructs (e.g., camouflaging) were quantified using a single measure. Third, since all measures were self-reported except for the ADOS-2 and WASI-II, common-method variance possibly inflated the associations between most predictors and the dependent variables. Fourth, although many analyses were sufficiently powered, the study has low (< 0.8) power to detect some effects of interest, especially in the small high-camouflaging subgroup. And fifth, our cross-sectional study design does not allow us to investigate questions regarding causality or changing trajectories over time. It is important that future studies investigate these constructs longitudinally across the lifespan.
Our study also has notable strengths. The unique and inclusive sample of women with autistic traits allowed us to investigate constructs dimensionally and trans-diagnostically. Arguably, unlike many “clean” research samples, the present sample represents a broad range of women with autistic traits who seek clinical services: some participants were diagnosed autistic women, some are probably autistic women who are undiagnosed due to successful camouflaging efforts, and some are neurotypical women with autistic traits. We encourage other researchers to heed the calls for research that explores distress trans-diagnostically as this approach will allow samples to include undiagnosed (potentially camouflaged) autistic women (Halladay et al., 2015; Livingston & Happé, 2017). Another strength of our study is that it incorporated a measure of daily functional challenges in addition to measures of psychological distress. To our knowledge, ours is the first study to report on the relationship between camouflaging of autistic traits and functional challenges.
Future directions
The predictor variables included in our study accounted for about a quarter or less of the variance in the clinically important dependent variables. Potential predictive factors not included in the current study design are numerous, including the perceived ratio of successful to unsuccessful camouflaging efforts. Our findings regarding camouflaging and social difficulties (SRS-2) harmonize with Cassidy, Bradley, Shaw, and Baron-Cohen’s (2018) finding that camouflaging and unmet support needs were risk factors for severe psychological distress, as well as with a recent finding that loneliness is among the strongest predictors of depression in autistic adults (Han et al., 2019). Together, these results suggest that self-perceived social atypicality and social isolation likely are key predictors of mental health challenges in individuals with autistic traits. Somewhat ironically, feeling chronically different from their peers may be something people with autistic traits all share regardless of diagnostic status. Along with increasing public awareness of autism, there is increasing awareness that loneliness is a widespread public health concern (Beutel et al., 2017; Holt-Lunstad et al., 2017; Leigh-Hunt et al., 2017). As society adapts to address loneliness in the neurotypical majority, there is opportunity to create inclusive communities that can meet the social needs of all people, including those with autistic traits. Future research can explore how best to socially include women with autistic traits and whether increased social connection reduces psychological distress and increases functional capacity.
Supplemental Material
AutismSI_SecondRandR_SupplementaryText – Supplemental material for Looking good but feeling bad: “Camouflaging” behaviors and mental health in women with autistic traits
Supplemental material, AutismSI_SecondRandR_SupplementaryText for Looking good but feeling bad: “Camouflaging” behaviors and mental health in women with autistic traits by Jonathan S Beck, Rebecca A Lundwall, Terisa Gabrielsen, Jonathan C Cox and Mikle South in Autism
Footnotes
Acknowledgements
We are deeply indebted to the study participants. We thank the research assistants who contributed to the work reported in this article, including Ava Dixon, Brinnley Lemmon, Eli Haun, Claire A. Chelladurai, Greyson Schuenman, Madyline Spencer, Marissa Farmer, Trevor DeMordaunt, Laurel Peacock, Katherine E. Christensen, Rachel Nuttall, Lacy Ekins, and Sarah Kamhout.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Mentoring Environment Grant from Brigham Young University to Drs. Lundwall and Cox, a Graduate Research Fellowship from Brigham Young University to Dr. Beck, and a graduate research grant from the Organization for Autism Research to Dr. Beck.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.