
Abstract
In this second of two primary papers, we examined moderators of treatment effects for younger siblings of children with autism spectrum disorders whose parents were taught to use a parent-implemented intervention called “Improving Parents As Communication Teachers”. Investigators randomized 97 high-risk siblings and their primary parent to either the Improving Parents As Communication Teachers or control group, used intent-to-treat analysis, and used assessors and coders who were blinded to group assignment. We hypothesized that a cumulative risk score (incorporating younger siblings’ sex, multiplex status, and behavioral risk) would moderate the effect of Improving Parents As Communication Teachers on younger siblings’ proximal skills related to their continuously measured communication challenges. Pre-intervention level of parents’ depressive symptoms was the proposed moderator of Improving Parents As Communication Teachers on parenting-related stress and parenting efficacy. In high-risk siblings with no additional risk factors (i.e. girls with only one older sibling with autism spectrum disorder and who score at low risk on an autism spectrum disorder screen), parental receipt of Improving Parents As Communication Teachers training had indirect effects on children’s expressive language ability or autism spectrum disorder diagnosis through earlier effects on high-risk siblings’ intentional communication or expressive vocabulary. “Improving Parents As Communication Teachers” intervention did not show moderated or total effects on parenting-related stress or parenting efficacy.
Lay Abstract
In this second of two primary papers, we examined two pre-intervention characteristics that might describe for whom a parent-implemented intervention, “Improving Parents As Communication Teachers,” worked. Investigators randomized 97 high-risk siblings and their primary parent to either the Improving Parents As Communication Teachers or control group, used intent-to-treat analysis, and used assessors and coders who were blinded to group assignment. We predicted that a combined risk score (incorporating young siblings’ sex, multiplex status, and behavioral risk) would describe the subgroup for whom Improving Parents As Communication Teachers affected the targeted skills related to reducing communication challenges. We also predicted that pre-intervention level of parents’ depressive symptoms would describe the parents whose parenting stress and effectiveness as parents would be improved by learning to use Improving Parents As Communication Teachers. In girls with only one older sibling with autism spectrum disorder and who scored at low risk on an autism spectrum disorder screen, parental receipt of Improving Parents As Communication Teachers training had an indirect effect on children’s expressive language ability or autism spectrum disorder diagnosis through earlier effects on high-risk siblings’ intentional communication or expressive vocabulary. We did not confirm our prediction regarding Improving Parents As Communication Teachers’ effect on parenting-related stress or sense of parenting effectiveness.
Introduction
This is the second of two papers reporting primary results of a pre-registered randomized control trial using “Improving Parents As Communication Teachers” (ImPACT) with younger siblings of children with autism spectrum disorder (ASD) (i.e. high risk siblings of children with ASD: HR-Sibs) (Yoder, Stone, & Edmunds, in press). In this article, we examine whether additional risk for social communication disorders (i.e. being male, screening at risk for ASD, and having more than one sibling with ASD in the home) moderates the effect of ImPACT on proximal skills related to reducing communication challenges (i.e. expressive vocabulary ability and ASD symptomology). In addition, we examine whether ImPACT reduces parenting-related stress and increases parenting efficacy more for parents with low levels of pre-intervention depressive symptoms than parents with higher levels of these symptoms. The rationale for these aims follows.
In our first paper, we laid out evidence that a large minority of HR-Sibs are likely to meet criteria for a language delay or social communication disorder by 36 months and that one way to reduce the severity of these communication disorders in HR-Sibs may be to teach parents to use an intervention during the period at which symptoms have not yet become sufficiently severe to warrant a diagnosis (i.e. pre-emptive intervention). We also laid out the logic supporting the assertion that effects are most likely to be seen on continuous measures of children’s expressive language ability or social communication, as opposed to dichotomous diagnostic outcome, and that effects on expressive language ability and social communication are likely to be mediated by effects on proximal child outcomes. Before the study began, we predicted that the proximal skills, likely to be associated with reducing communication challenges, are generalized (a) intentional communication (Yoder et al., 2015); (b) expressive vocabulary level; (c) motor imitation (Ingersoll & Schreibman, 2006; Rogers, 1999); and (d) object play (Lieberman & Yoder, 2012). Each is empirically linked to expressive language ability or ASD symptomatology (Ingersoll & Schreibman, 2006; Lieberman & Yoder, 2012; Rogers, 1999; Yoder et al., 2015). Finally, we provided a rationale for selecting ImPACT as the parent-implemented intervention, in part, due to the fact that it targets the above-mentioned proximal skills (Ingersoll & Wainer, 2013).
The findings presented in the first paper confirmed that ImPACT indirectly affected HR-Sibs’ communication challenges by increasing parents’ use of ImPACT strategies and by increasing two of the proximal outcomes: motor imitation or intentional communication (Yoder, et al., in press). However, we do not yet know whether there is a subgroup of HR-Sibs for whom ImPACT works, and if so, the characteristics of this subgroup.
Cumulative risk as a possible descriptor of the subgroup for whom ImPACT works
To optimize the limited resources available to support parents in acting as their children’s interventionists, we need to identify the subgroup of HR-Sibs whose proximal outcomes are most likely to benefit from intervention. We chose to use a cumulative risk model, as these models tend to work better than single risk models in predicting later outcomes (Dunst & Trivette, 1994) and have been called for in the HR-Sibs literature (Yirmiya & Charman, 2010). Adding multiple risk factors to may further improve our ability to predict which HR-Sibs will benefit from parent-implemented intervention targeting proximal outcomes relative to single risk factors. For example, the probability of HR-Sibs eventually being diagnosed with ASD is higher when both sex (i.e. males) and number of siblings with ASD (i.e. more than one sibling with ASD in the family) are considered as risk factors (50%) than when sex (26% for males) or number of siblings with ASD in the family (32% for multiplex) are considered alone (Ozonoff et al., 2011). To our knowledge, no study has examined whether cumulative risk predicts the differential effect of an intervention for HR-Sibs. Herein, cumulative risk is computed from the child’s sex, number of siblings with ASD in the home, and behavioral risk as derived from commonly used ASD screening questionnaires.
Before the study, we were unable to predict which cumulative risk subgroup (i.e. highest vs lowest) would benefit more from ImPACT training due to the lack of prior research on this issue and the presence of contradictory, but arguably equally likely, logical arguments. On one hand, the highest cumulative risk HR-Sibs may be particularly likely to benefit from the intervention relative to a control group because they are in greater need of the special teaching methods that parents learn to use. On the other hand, children with lowest cumulative risk may benefit most from parent-implemented intervention because these children may have greater internal resources that enable them to learn from the intervention. Even when we cannot confidently predict the particular level of cumulative risk that describes the children for whom an intervention works, confirming our prediction that it is cumulative risk, rather than some other variable, which describes for whom intervention works will result in greater confidence that the finding will replicate, as compared to examining multiple moderators of intervention effects (Yoder & Compton, 2004).
Possible effects of ImPACT on parenting stress and efficacy
Because parents of children with ASD already have atypically high parenting stress and depressive symptoms (Ingersoll & Hambrick, 2011; Weitlauf et al., 2014), it is important to test whether asking them to implement ImPACT affects their parenting-related stress, particularly for parents with initially high depressive symptoms. In a previous small-sample trial that used listwise deletion to address missing data, a different parent-implemented treatment resulted in producing more stress for parents with initially high depressive symptoms (Lieberman-Betz et al., 2014). Depression tends to be associated with experiencing daily activities as burdensome and providing intervention to their later-born children adds additional responsibilities (Lovejoy et al., 2000). The finding regarding the depression-moderated treatment effect on parenting stress became nonsignificant when multiple imputation was used to address missing data, but the trend for the finding was still present in this small trial (Lieberman-Betz et al., 2014). A larger sample that appropriately addresses missing data might confirm that depression moderates the effect of a parent-implemented treatment on stress. More specific to the ImPACT treatment, other previous reports have noted that parents of children with ASD have reported less parenting stress after learning to use ImPACT strategies (Wainer & Ingersoll, 2013). However, asking parents to implement ImPACT with their HR-Sibs places an additional layer of demands on top of raising a child already diagnosed with ASD. Thus, additional study is needed to test ImPACT’s effect on parenting-related stress when they are asked to implement ImPACT with HR-Sibs. In addition, we hope that giving parents tools to ameliorate the risk of communication disorder in their HR-Sibs will lead parents to experience heightened parenting efficacy. ImPACT’s effect on parenting stress and efficacy may be conditional on initial level of depressive symptoms.
Research questions
This article addresses two questions:
Does the indirect effect of ImPACT on communication challenges through the facilitation of proximal skills vary by cumulative risk? That is, we asked whether HR-Sibs’ cumulative risk for communication disorder moderates ImPACT’s facilitation of proximal skills related to the reduction of communication challenges and whether this moderated effect on proximal skills mediates ImPACT’s effect on end-of-study communication challenges. This research question requires testing a moderated, mediated effect of ImPACT on communication challenges.
Does ImPACT reduce parenting-related stress and increase parenting efficacy more in parents with initially low depressive symptoms than in parents with initially high depressive symptoms? This research question requires testing a moderated treatment effect of ImPACT on parenting-related stress and parenting efficacy.
Methods
Participants
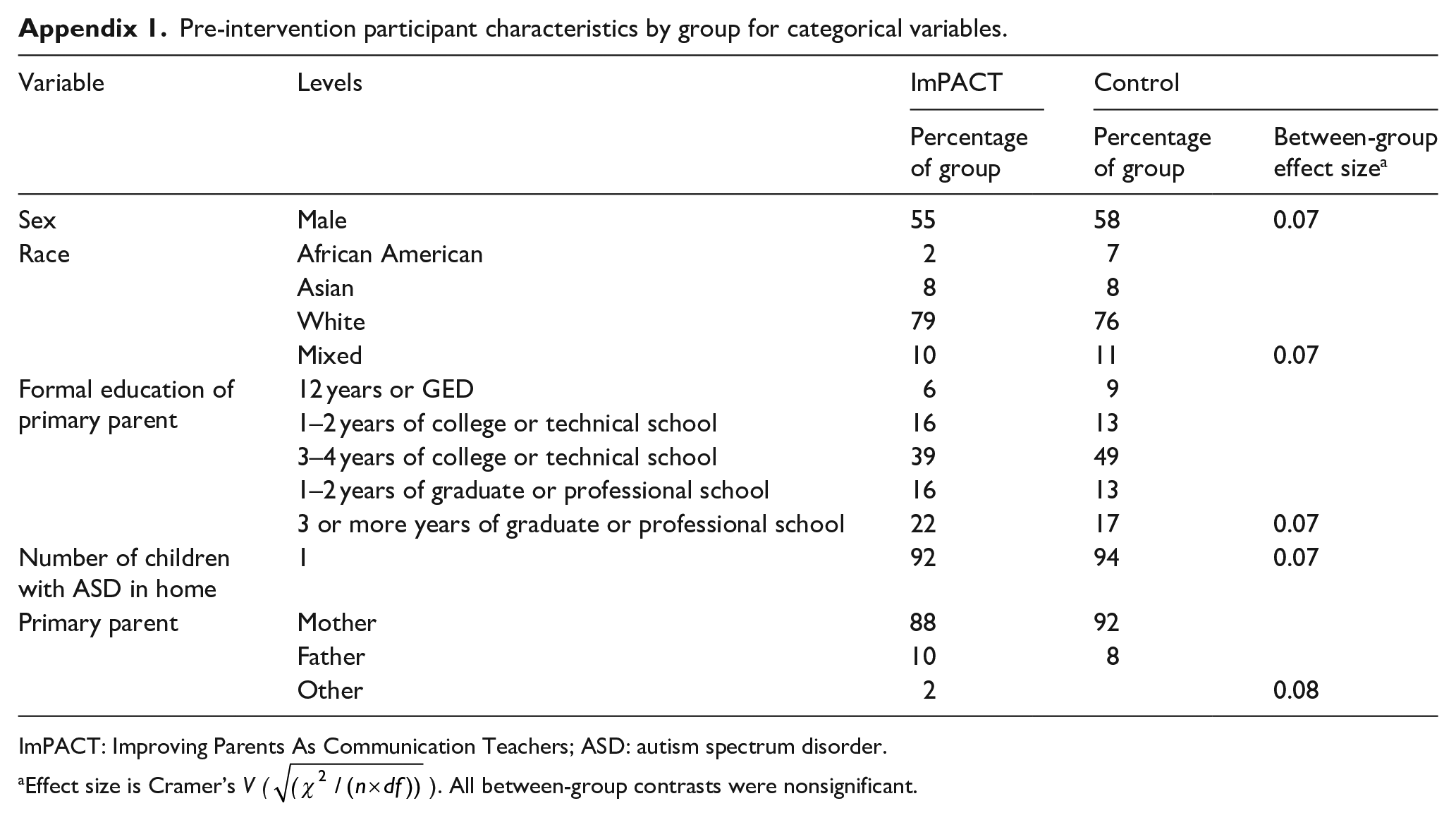
Ninety-seven children (M = 14 months, SD = 2 months) and their primary parent at two sites (Nashville, TN: n = 49, Seattle, WA: n = 48) participated in this study. Inclusion criteria and descriptive statistics are provided in the first paper, but descriptive information is provided in Appendix 1. Of particular note, over 90% of the families had only one child with ASD in the home prior to intervention onset. The caregivers were mothers (89%), fathers (9%), or grandmothers (1%). None of the descriptor variables differed significantly between intervention groups, p values: range = 0.12–0.95, M = 0.70, and SD = 0.24. All participants were consented, and the study was approved by the relevant institutional review boards.
Research design
Investigators randomly assigned parent–child dyads to either ImPACT (n = 49) or control (n = 48) groups. The intervention phase lasted 3 months (Times 1–2). Proximal outcomes, parenting stress, and parenting efficacy variables were measured at study entry and 6 months after study entry (Times 1 and 3), and communication challenges were measured at study entry and 9 months after study entry (Times 1 and 4). Proximal skills were measured 3 months after the end of the treatment to provide time for competent use of the ImPACT methods to be manifested in children’s generalized skills. A past report indicated that a parent-implemented treatment resulted in more stress 3 months after the end of the treatment phase in parents with initially more depressive symptoms (Lieberman-Betz et al., 2014). Study assessors and coders of observational procedures were blinded to group assignment. Intent-to-treat analysis procedures were used (i.e. including all participants in primary analyses, regardless of attendance at intervention and assessment sessions). Full information maximum likelihood estimation was used to address missing values. This study was pre-registered with www.clinicaltrials.gov with clinical trials registration number 140924. The CONSORT chart is provided in the first paper. Overall and differential attrition were low.
Intervention groups
ImPACT
This instantiation of the ImPACT intervention involved staff offering parents 24 in-home teaching sessions over 12 weeks (Ingersoll & Dvortcsak, 2010). The staff who provided the parent teaching was either a certified ImPACT trainer or staff members trained and supervised by this trainer. Examples of the ImPACT curriculum are provided in the first paper. Staff adherence to the ImPACT protocol for teaching parents was estimated using self-administered, session-specific checklists on at least two sessions per parent–child pair and averaged 91% (SD = 3%).
Control
Staff did not restrict intervention outside of the research study for either group, including the control group. Nonproject therapy attendance per month during the intervention phase was low and almost equal between groups (ImPACT M(SD) = 0.6(1.6) h; control M(SD) = 0.5(1.4)h, p > 0.05).
Procedures
Administration manuals and fidelity of implementation instruments are available from the first author. The measurement procedures’ interaction style, location, examiner, and materials differed from those used in the intervention sessions. Longer descriptions of the proximal outcome and communication challenge measures are available in the first paper (Yoder, et al., in press) and Appendix 2. All coding manuals are available from the first author. More detailed descriptions of coding are in the first paper (Yoder, et al., in press) and Appendix 2. Session-level, point-by-point agreement checks and discrepancy discussions were conducted on at least 20% of randomly selected sessions throughout the study to reduce observer drift. Interobserver reliability estimates for all variables at all measurement periods were greater than our accepted threshold of intraclass correlation coefficient (ICC) >0.69.
To measure cumulative risk for communication disorders at Time 1, we used a demographic questionnaire and either the first year inventory (FYI; Watson et al., 2007) or the modified checklist for autism in toddlers, revised with follow-up (M-CHAT-R/F; Robins et al., 2014), depending on the age of the HR-Sib. Parents filled out the demographic form to report the HR-Sibs’ binary sex and the number of siblings with ASD living in the home. If under 16 months (n = 73), behavioral risk was determined using the FYI social communication risk threshold (Turner-Brown et al., 2012). If 16–18 months, behavioral risk was determined by the M-CHAT-R/F using the ASD risk threshold (Robins et al., 2014). 1 There was no difference between intervention groups in the proportion of participants receiving the FYI versus M-CHAT-R/F (χ2(1) = 0.12, p = 0.82). Thus, the consequence of functionally equating behavioral risk from different instruments is greater random measurement error and increased probability of Type II errors (Thompson & Vacha-Haase, 2000). Being male, having more than one sibling with ASD (i.e. multiplex status), and scoring above the risk threshold were equally weighted; i.e. the presence of each was coded as “1.” Behavioral risk, sex, and number of siblings with ASD were summed to compute cumulative risk for communication disorder that ranged from 0 to 3.
The center for epidemiologic studies depression scale (CES-D; Radloff, 1991) was administered at Time 1 to assess pre-intervention levels of parents’ depressive symptoms. The CES-D is a self-report on 20 symptoms, rated on four levels of frequency of occurrence in previous week. The total raw score was the analyzed metric. In another study of parents of young children with ASD, the internal consistency of the total raw score was 0.92 (Lieberman-Betz et al., 2014).
To measure parenting-related stress, we administered the parenting stress index short form (PSI; Abidin, 1983) at Times 1 and 3. The PSI short form is a 36-item self-report measure of perceived child difficulty, parent distress, and parent–child dysfunctional interactions. The total raw score was the analyzed metric to reflect parental stress. In another study of parents of children with ASD, the total raw score’s internal consistency was between 0.93 and 0.95, depending on measurement period (Lieberman-Betz et al., 2014).
To measure parenting efficacy, we administered the maternal efficacy scale (MES) at Times 1 and 3 (Teti & Gelfand, 1991). The MES is a 10-item self-report measure designed to assess perceptions and feelings of efficacy in different childcare domains. The total raw score was the analyzed metric. The internal consistency of the total raw score was between 0.81 and 0.86 in unpublished data on parents of children with ASD associated with Lieberman-Betz et al. (2014).
The measures of motor imitation, intentional communication, object play, expressive vocabulary, expressive ability, and social communication were described in detail in the first paper (Yoder, et al., in press). Table 1 summarizes how these constructs were quantified. Appendix 2 also provides detailed information about the variables.
Constructs, procedures, measurement periods, and variables.
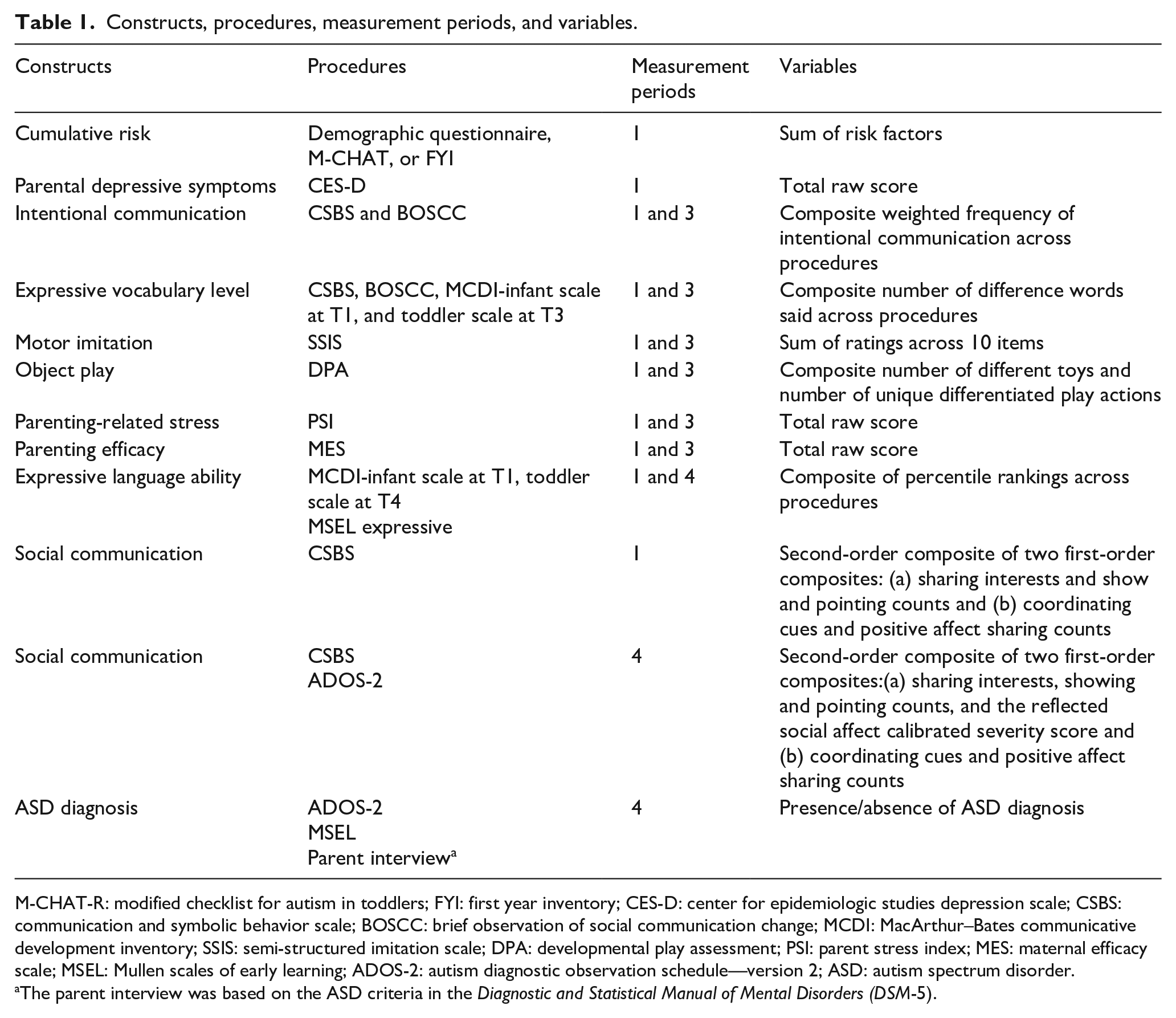
M-CHAT-R: modified checklist for autism in toddlers; FYI: first year inventory; CES-D: center for epidemiologic studies depression scale; CSBS: communication and symbolic behavior scale; BOSCC: brief observation of social communication change; MCDI: MacArthur–Bates communicative development inventory; SSIS: semi-structured imitation scale; DPA: developmental play assessment; PSI: parent stress index; MES: maternal efficacy scale; MSEL: Mullen scales of early learning; ADOS-2: autism diagnostic observation schedule—version 2; ASD: autism spectrum disorder.
The parent interview was based on the ASD criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
The diagnosis of ASD at Time 4 was determined by a licensed clinical psychologist on the basis of information obtained from the autism diagnostic observation scale, version 2 (ADOS-2, a parent interview based on the ASD criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), and other clinical assessments (e.g. Mullen scales) as available. This variable was used as a dependent variable in an exploratory analysis.
Data analysis plan
The indicator variables purported to measure each construct, indicated in the research questions and detailed in the procedures section, were examined to determine if their intercorrelation was sufficient to justify composite measures (Cohen, 1988). Composite measures of constructs were selected to improve validity and reduce the number of significance tests and resulting familywise error. Preliminary analyses were conducted to ensure that the assumptions of statistical control of the baseline measures of the dependent variable were met. Controlling the baseline scores for the dependent variable improves precision of the treatment effect size estimates. Full information maximum likelihood estimation was used to estimate coefficients in the moderated, mediated models. Bias-corrected bootstrapped confidence intervals (CIs) around indirect effects were estimated.
Results
Preparatory analyses
Data reduction
Details of the data reduction are in the first paper. To reduce the number of significance tests and to increase the construct validity of analyzed variables, equally weighted composite variables were computed. The variables selected for the analyses that follow are indicated in Table 1.
Testing the need and assumptions of pretest covariates
As indicated in the first paper, all pretests were nonsignificantly different between groups, except motor imitation from the semi-structured imitation scale (SSIS), t(92) = 3.7, p < 0.001, which was significant and positively predicted all four proximal outcomes at Time 3 and the two communication challenge variables at Time 4. Having found that the data fit the assumption of homogeneity of slopes, Time 1 motor imitation was partialed out of the child dependent variables.
Testing the convergent construct validity of the cumulative risk index
Lower risk scores were associated with higher means on object play at Time 3 (Wald χ2(3) = 12.2, p = 0.007), intentional communication at Time 3 (Wald χ2(3) = 11.4, p = 0.01), social communication at Time 4 (Wald χ2(3) = 8.4, p = 0.04), and expressive language ability at Time 4 (Wald χ2(3) = 9.2, p = 0.03). The positive predictive value (PPV) for the cumulative risk index predicting ASD diagnosis is the proportion of participants correctly predicted to have an ASD diagnosis. The PPV was 0.59, indicating that 59% of children identified as having ASD by the risk index actually received an ASD diagnosis, which is significantly higher than the actual rate of ASD diagnoses at Time 4 in the sample, 24%, χ2(3) = 14.9, p = 0.002. The false positive rate is 1-PPV. While the PPV provides evidence for the construct validity of cumulative risk, cumulative risk produced 41% false positives. Thus, the cumulative risk index is not sufficient evidence of ASD or language delay by itself. Nonsignificant differences among cumulative risk groups occurred on motor imitation at Time 3 and expressive vocabulary level at Time 3, p values > 0.05.
Conditional and unconditional intervention effects did not vary by site
Nonsignificant effects were found for (a) site × intervention group and (b) site × group × putative moderator (i.e. risk or depressive symptoms) predicting proximal outcomes at Time 3 or communication challenges at Time 4; p values range from 0.36 to 0.80, M = 0.60, and SD = 0.13.
Primary analyses
ImPACT has effects on HR-Sibs’ communication challenges through risk-moderated mediated effects on proximal outcomes
Bias-corrected bootstrapping was used to estimate CIs around moderated indirect effect coefficients (Hayes, 2017). Table 2 presents the significant moderated indirect effects of ImPACT on HR-Sibs’ communication challenges through one of the proximal skills. Moderated mediated effects involving play and motor imitation were nonsignificant (i.e. CIs included zero).
ImPACT’s statistically significant risk-moderated indirect effects on children’s communication challenges.
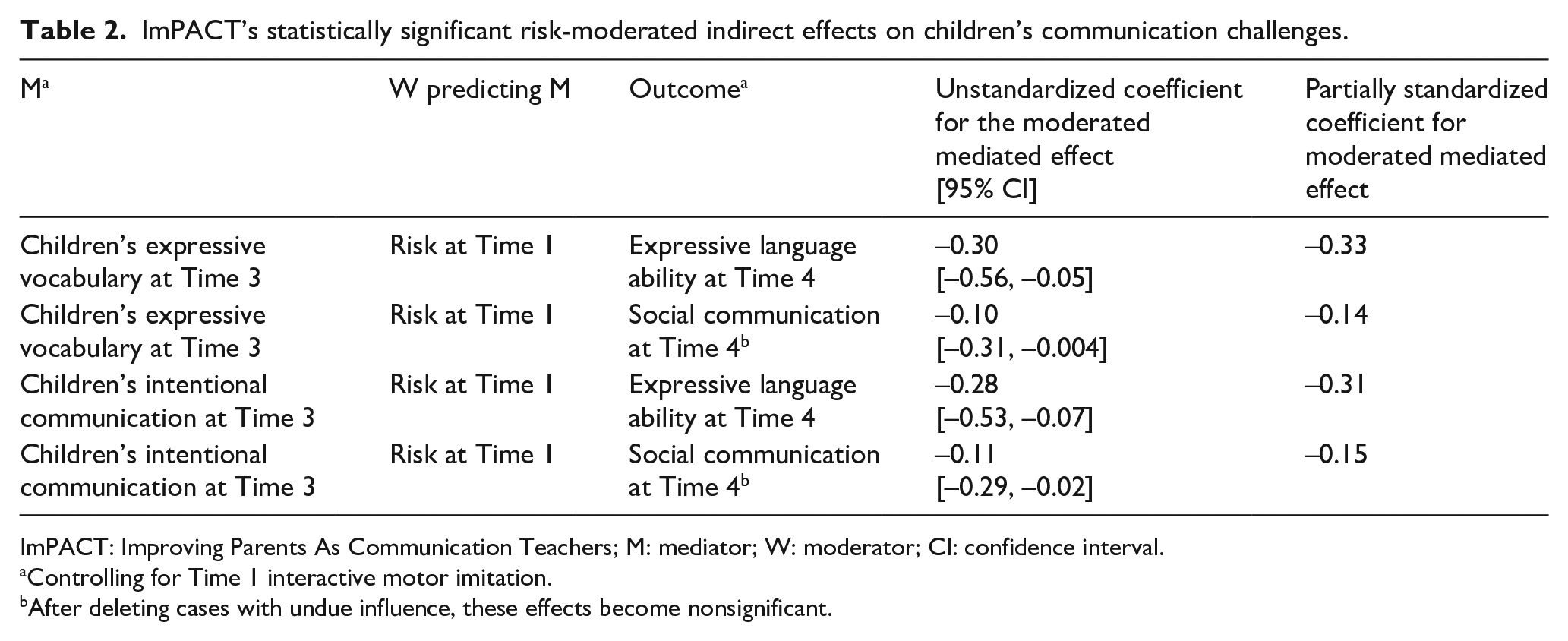
ImPACT: Improving Parents As Communication Teachers; M: mediator; W: moderator; CI: confidence interval.
Controlling for Time 1 interactive motor imitation.
After deleting cases with undue influence, these effects become nonsignificant.
ImPACT teaching had an indirect effect on children’s continuously measured expressive language ability at Time 4 by increasing children’s Time 3 intentional communication, but this indirect effect only occurred in the subgroup of HR-Sibs with no additional risk, 0.40, 95% CI [0.07, 0.76], partially standardized effect size = 0.49. This indirect effect was nonsignificant in HR-Sibs with additional initial risk. Figure 1 illustrates this moderated indirect effect as an example. A similar finding occurred for children’s Time 4 social communication, but became nonsignificant when cases with undue influence were deleted.
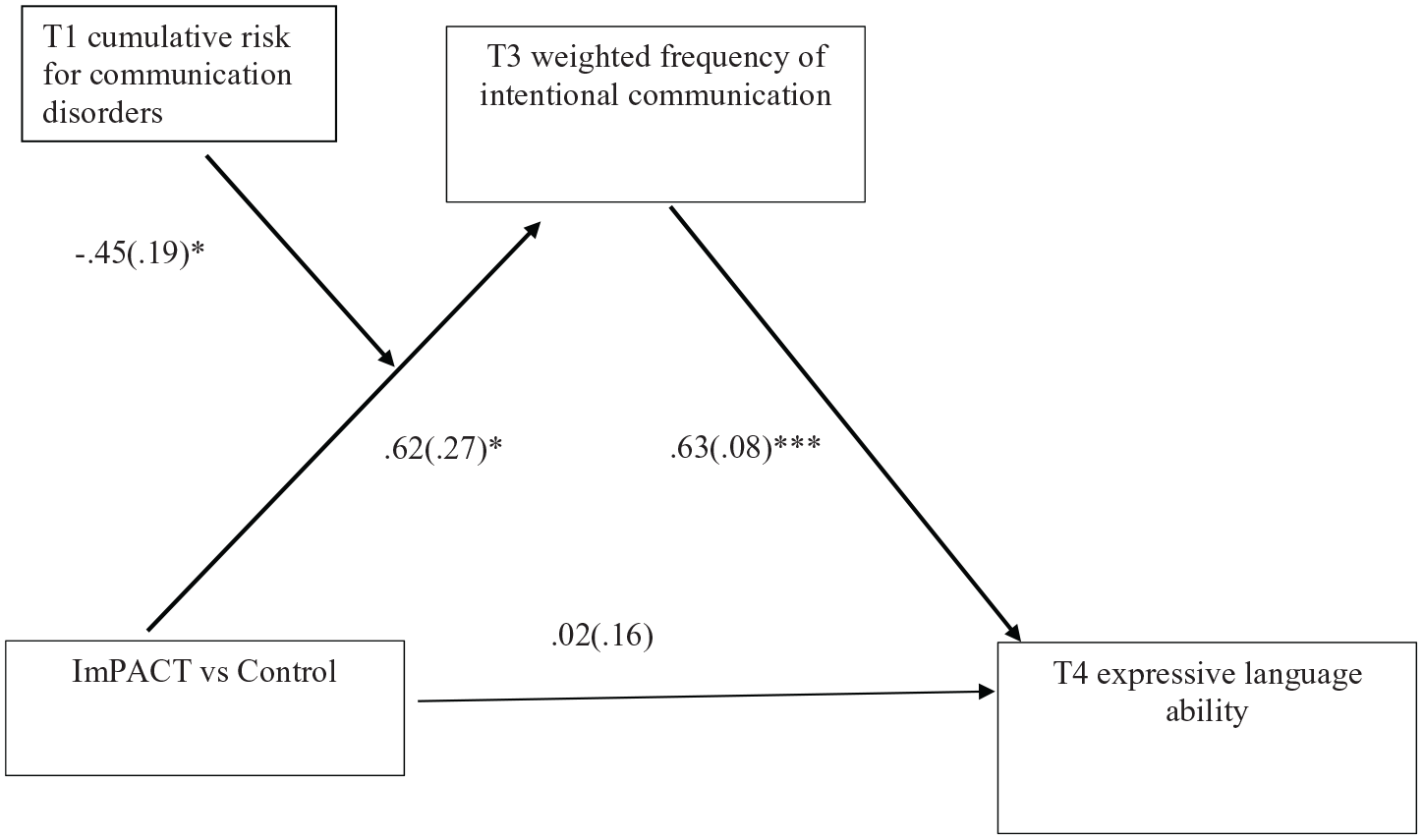
Path diagram of the ImPACT teaching’s risk-moderated indirect effect on expressive language ability at Time 4 through HR-Sibs’ intentional communication at Time 3.
ImPACT teaching had an indirect effect on children’s continuously measured expressive ability at Time 4 through children’s Time 3 expressive vocabulary, but again, this indirect effect occurred only in a subgroup of HR-Sibs described by no additional risk, 0.5, 95% CI [0.12, 0.88], partially standardized effect size = 0.62. Again, this indirect effect was nonsignificant in HR-Sibs with additional initial risk, p values > 0.05. A similar, smaller effect occurred on HR-Sibs’ Time 4 social communication, but it became nonsignificant when cases with undue influence were deleted.
ImPACT teaching had no effect on parents’ stress or efficacy, regardless of parents’ initial level of parental depressive symptoms
The statistical interactions of initial parental depressive symptoms and intervention group predicting either parental stress or parental efficacy at Time 3 were nonsignificant, Wald’s χ2(1) < 1.0, p > 0.05. In addition, there was no main effect of ImPACT on parenting stress, χ2(1) = 0.09, p = 0.76, or parenting efficacy, χ2(1) = 0.34, p = 0.56. Thus, there is no evidence that ImPACT teaching had positive or negative effects on parents’ stress or efficacy, regardless of whether parents’ initial depressive symptoms are considered.
Post hoc analyses
Although not expected due to statistical power loss when we dichotomize outcomes, we conducted an analogous analysis predicting ASD diagnosis at Time 4. Using logistic regression, analyses indicated that ImPACT teaching had an indirect effect on children’s ASD diagnosis at Time 4 by increasing children’s Time 3 intentional communication, but this indirect effect only occurred in a subgroup of HR-Sibs with no additional risk, −0.08, 95% CI [−0.18, −0.004]. This indirect effect was nonsignificant in HR-Sibs with additional initial risk. The overall moderated mediated treatment coefficient was positive and significant, 0.06(0.03), 95% CI [0.005, 0.13]. The R2 change for the product term of initial cumulative risk × treatment group predicting intentional communication at Time 3 was 0.05, p < 0.05.
None of the Time 1 variables both correlated with initial cumulative risk and moderated ImPACT total effects on intentional communication or expressive vocabulary at Time 3. Thus, we could find no evidence that other measured Time 1 variables better explained ImPACT teaching’s conditional indirect effects on intentional communication or expressive vocabulary at Time 3 than did initial cumulative risk.
Discussion
Herein, we tested whether two characteristics describe for whom ImPACT works in a sample of HR-Sibs and their parents. We confirmed that initial cumulative risk identifies the HR-Sibs for whom ImPACT improves intentional communication and expressive vocabulary, which subsequently affects expressive language ability or ASD diagnosis. Specifically, these effects occurred in HR-Sibs who had no additional risk before the intervention phase began. Even though the conditional indirect effect of ImPACT on ASD diagnosis was not expected due to statistical power considerations when outcomes are dichotomized, this finding has potential clinical importance. Together with the confirmed predictions, we have stronger expectations for replication for the findings predicting expressive language ability than the findings predicting ASD diagnosis. In addition, the convergent construct validity evidence supported our prediction that sex, number of siblings with ASD, and behavioral risk are relevant for quantifying cumulative risk. But because fewer than 10% of the families had more than one sibling with diagnosed ASD in the home before intervention began, cumulative risk in this study mostly reflected sex and behavioral risk.
For parenting-related stress and parenting efficacy, we did not confirm a prediction that pre-intervention levels of parents’ depressive symptoms would describe for whom ImPACT worked. In addition, ImPACT teaching did not affect parenting-related efficacy or stress levels, regardless of initial level of depressive symptoms. About a quarter of the parents in each group scored above the clinical cut score for depression at Time 1. Thus, there was sufficient variance in depressive symptoms to detect the predicted moderated effect had it been present. Although a past report suggested that parents with initially high depressive symptoms who were assigned to a parent-implemented treatment group reported more parenting stress than similar parents assigned to a control group, this finding was nonsignificant when appropriate handling of missing data was used (Lieberman-Betz et al., 2014). Thus, increasing the sample size and proper handling of missing data did not result in supporting the hypothesis that parents with initially high depressive symptoms experience more parenting stress when asked to implement a treatment with their HR-Sib.
Limitations and future research
The link between HR-Sibs’ initial cumulative risk and ImPACT teaching’s causal effect on proximal outcomes is correlational. Covarying pretreatment variables might explain why initial cumulative risk moderated ImPACT’s effect on proximal outcomes (i.e. potential third variable explanations). Although we excluded several third variable explanations for ImPACT’s risk-moderated effect, unmeasured pretreatment variables might do so.
Because we were unable to predict before the study was conducted which end of the cumulative risk continuum would describe the HR-Sibs who benefited from ImPACT, it would be most conservative to require replication prior to clinical use of the current significant findings. This study’s confirmation that cumulative risk is a moderator of ImPACT’s effect on intentional communication and expressive vocabulary provides the basis of future replication studies.
Although the unexpected absence of ImPACT’s effect on parenting stress is consistent with a conclusion that ImPACT is relatively safe for parents of children with ASD, nonsignificant findings are always subject to misinterpretation because weaknesses in measurement can sometimes explain null findings. For example, it is possible that we did not have a sufficiently sensitive measure of the type of parenting stress affected by ImPACT teaching. Future investigation using more sensitive measures of parenting stress is needed.
In addition, future research that examines the add-on effects of mindfulness training on parenting-related stress and parenting efficacy might enhance the degree to which parents use ImPACT strategies, which might in turn affect the extent to which ImPACT reduces HR-Sibs’ communication challenges. Initial investigations are encouraging (Singh, 2019).
ImPACT’s effect on children may have been cumulative and gradual, which may make it difficult for parents to attribute their children’s skill increase to parents’ use of ImPACT strategies. Logically, feelings of efficacy may increase in response to immediate evidence that taught strategies elicit children’s use of new or infrequently used behaviors. Future research is needed to better understand which interventions affect parents’ perception of their efficacy.
Strengths
This study’s internally valid design and multi-method measurement approach strengthen confidence in the replicability of the current significant findings. In addition, the use of a moderated mediated model, instead of separate models, to confirm that cumulative risk moderates ImPACT’s effects on communication challenges through proximal outcomes reduces the number of significance tests and improves the probability of replication.
Relation of current findings to extant literature
This article adds to our previous findings regarding proximal outcomes that affect later communication challenges in HR-Sibs by specifying whether initial cumulative risk describes for whom the proximal outcomes indirectly reduce the severity of communication challenges. Our previous study found that ImPACT increased intentional communication and motor imitation through parents’ use of ImPACT strategies, and each of these proximal outcomes mediated treatment effects on children’s communication challenges (Yoder, et al., in press). This article’s findings indicate that ImPACT’s effect on intentional communication occurs only in HR-Sibs with no additional initial cumulative risk. In addition, this study findings indicate that cumulative risk is not a descriptor of the children for whom motor imitation is a proximal outcome associated with reduction of communication challenges (i.e. a pivotal skill). We have not yet identified for whom motor imitation is a pivotal skill. This article’s finding that expressive vocabulary is a pivotal skill in HR-Sibs with no additional risk is new to the literature. The current findings indicated that children with no additional risk had better communication and play skills than children with additional risk factors. We speculate that relatively good communication and play skills may make it easier or more rewarding to implement ImPACT techniques well, frequently, and consistently and children with relatively high communication and play skills may have greater capacity to learn from the ImPACT strategies.
Conclusion
This study supports using ImPACT as a pre-emptive intervention to enhance expressive language ability and reduce the probability of an ASD diagnosis in HR-Sibs by indicating that intentional communication or expressive vocabulary are proximal outcomes for girls who do not score in the behavioral risk range on a screening instrument. Together with an earlier report showing that indirect effects of ImPACT occurred through improving motor imitation, regardless of initial cumulative risk level, the results suggest that motor imitation is also a pivotal skill for reducing communication challenges. Taken together, the results of these two papers do not support treating only those HR-Sibs who score in the “risk” range on screening instruments, as this group of children appears to benefit from ImPACT regardless of their screening status.
Footnotes
Appendix 2
Derivation of the child outcomes.
Appendix 1.
Pre-intervention participant characteristics by group for categorical variables.
| Variable | Levels | ImPACT | Control | |
|---|---|---|---|---|
| Percentage of group | Percentage of group | Between-group effect size a | ||
| Sex | Male | 55 | 58 | 0.07 |
| Race | African American | 2 | 7 | |
| Asian | 8 | 8 | ||
| White | 79 | 76 | ||
| Mixed | 10 | 11 | 0.07 | |
| Formal education of primary parent | 12 years or GED | 6 | 9 | |
| 1–2 years of college or technical school | 16 | 13 | ||
| 3–4 years of college or technical school | 39 | 49 | ||
| 1–2 years of graduate or professional school | 16 | 13 | ||
| 3 or more years of graduate or professional school | 22 | 17 | 0.07 | |
| Number of children with ASD in home | 1 | 92 | 94 | 0.07 |
| Primary parent | Mother | 88 | 92 | |
| Father | 10 | 8 | ||
| Other | 2 | 0.08 | ||
ImPACT: Improving Parents As Communication Teachers; ASD: autism spectrum disorder.
Effect size is Cramer’s V (
Acknowledgements
The authors are grateful to the skillful and conscious work of our staff: Catherine Bush, Elizabeth Gardner, Cassandra Newsom, Amy Nicholson, Jessica Buenahora, Heather Redix, Katherine Ragsdale, Kathryn Coddington, Danielle Trzil, Sonja Kottke, Karen Bearss, Courtney Froehlig, Veronica Kang, Shanni Geller, Allycen Kurup, Hailee Hannah, Rachel Hantman, Colleen Harker, Elizabeth Karp, and Catherine Dick. The authors are also grateful to the families who participated in this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant to the lead author from NIDCD (R01DC013767), to the parent institution by the National Institute for Child Health and Disorders (NICHD; P30HD15052), and to S.E. from NIDCD (F31DC015696), but it does not necessarily express the views of employees of these agencies.