
Abstract
People with autism spectrum disorder are less physically active than are their peers. Nurses can play a key role in helping to promote such behaviors, but they do so sparingly. The purpose of this study, therefore, was to examine the degree to which nurses recommend physical activity to patients with autism spectrum disorder, and to identify antecedents thereof. Adopting a mixed methods approach, data were collected from a representative sample of nurses (n = 180) working in the United States. Results from regression analyses indicate that nurses were only moderately likely to recommend physical activity. When perceived barriers to physical activity were low, perceived benefits of physical activity held a positive, significant association with recommendations. However, when perceived barriers were high, the relationship between perceived benefits and recommendations was no longer significant. Inductive thematic analysis of the qualitative data showed the value nurses place on physical activity, how they interpret barriers and benefits, and strategies for making physical activity inclusive for people with autism spectrum disorder. In conclusion, nurses have an opportunity to more frequently promote physical activity to their patients with autism spectrum disorder and, in doing so, help mitigate some of the poor health outcomes people with autism spectrum disorder experience.
Lay abstract
Participation in regular physical activity is linked with physical, psychological, and social improvements. Nevertheless, persons with autism spectrum disorder participate at lower levels than do their peers. Nurses can play a key role in helping to promote such behaviors, but do so sparingly. The purpose of this study is to examine the degree to which nurses recommend physical activity to people with autism spectrum disorder. Even though a number of scholars have examined the role of health professionals in promoting physical activity, comparatively little research has examined nurses. Further, previous scholars have largely focused on the promotion of physical activity to patients in general. However, people with disabilities and people with autism spectrum disorder, specifically, are frequently overlooked when it comes to physical activity promotion. Data were collected from a representative sample of nurses (n = 180) working in the United States. Results indicate that nurses were only moderately likely to recommend physical activity. When perceived barriers were low, perceived benefits held a positive, significant association with recommendations. However, when perceived barriers were high, the relationship between perceived benefits and recommendations was no longer significant. Analysis of qualitative data showed the value nurses place on physical activity, how they interpret barriers and benefits, and strategies for making physical activity inclusive for people with autism spectrum disorder. In conclusion, nurses have an opportunity to more frequently promote physical activity to their patients with autism spectrum disorder and, in doing so, help mitigate some of the poor health outcomes people with autism spectrum disorder experience. The authors identified implications for nursing education and professional development, as well as for sport and recreation managers charged with delivering physical activity to people with autism spectrum disorder.
Introduction
People with autism spectrum disorder (ASD) have an elevated risk of poor health outcomes. Relative to their peers without ASD, people with ASD have higher risk of early mortality (Bilder et al., 2013), with chronic conditions, accidents, and medication complications all uniquely contributing (Smith DaWalt et al., 2019). Disparities exist for other health outcomes, as well, including anxiety, depression, diabetes, hypertension, and seizure, among others (Croen et al., 2015). People with ASD also report lower quality of life (Ayres et al., 2018), which might result from social support and subjective well-being (Kapp, 2018), and many have limited access to healthcare (Cheak-Zamora et al., 2014). As a result, researchers have increasingly examined interventions aimed at improving health outcomes (Benevides et al., 2020).
The role of physical activity
Physical activity represents one potential mechanism for improving health among people with ASD (Dillon et al., 2017; Healy et al., 2018; Lang et al., 2010). Participation in regular physical activity is associated with a bevy of physical, psychological, and social benefits (Tamminen et al., 2020; Teychenne et al., 2020; Warburton & Bredin, 2017; Zahrt & Crum, 2017), and these benefits are often strongest among populations that would benefit the most (Cunningham, 2019), including people with ASD. Consistent with this perspective, past researchers have shown how physical activity is associated with improvements in social interactions and experiences (Colombo-Dougovito et al., 2020; Tse, 2020), motor skills and control (Ketcheson et al., 2017; Pan et al., 2017), sleep quality (Tse et al., 2019), cognition (Tan et al., 2016), stereotypic behaviors (Tarr et al., 2020), and physical fitness (Pan, 2011).
Despite the many benefits of physical activity for people with ASD, relative to others, they are less likely to be physically active and are more likely to lead sedentary lives (Benson et al., 2019; Healy et al., 2017; Jones et al., 2017). These findings have been most commonly observed among children, adolescents, and young adults. Benson et al. (2019), for example, observed that young adults with ASD engaged in approximately half the daily moderate-intensity physical activity that their peers without ASD did. In a large-scale study of US children, Healy et al. (2019) found that children with ASD were less physically active and had more screen time than did youth with typical development. Whereas much of the research to date has focused on children and young adults, these patterns are likely to carry over into adulthood, too (Garcia-Pastor et al., 2019). Thus, the lack of physical activity among people with ASD might be contributing to their poor health outcomes.
Physical activity participation partially is a function of the perceived benefits of the activity, coupled with the barriers encountered (Biddle & Mutrie, 2001; Rhodes, 2017). For example, people with ASD report participating in sport because they believe it is good for them, is a way to make friends, will make them feel good, and is fun (Stanish et al., 2015). People with ASD who have pleasant, successful physical activity experiences early in life might also persist with those behaviors into adulthood (Colombo-Dougovito et al., 2020). On the other hand, barriers also play a meaningful role. A number of researchers have shown that intrapersonal and interpersonal barriers are the most salient factors influencing their sport and physical activity participation (Must et al., 2015; Obrusnikova & Cavalier, 2011). For example, in a phenomenological study of the parents of young adults with ASD, Nichols et al. (2019) found that behavioral limitations associated with ASD, as well as a lack of access and opportunities, all contributed to the relative lack of physical activity participation. Thus, both benefits and barriers, among other factors, contribute to physical activity participation among people with ASD.
Communicating the benefits of and opportunities to be physically active could serve to promote more physical activity among people with ASD (Sorensen & Zarrett, 2014). Parents and caregivers play an important role, especially when considering the time they spend with people with ASD (Brown et al., 2020). These individuals might communicate encouragement or provide the instruction needed to maintain a physically active lifestyle.
In addition to parents and caregivers, nurses are likely to play an influential role. Consider, for example, that people working in the health professions are uniquely qualified to deliver these messages (Lobelo & de Quevedo, 2016; Patrick et al., 2009). After all, people are likely to see healthcare professionals multiple times a year (McCarthy, 2014), thereby allowing for regular, consistent messaging. Researchers have also shown that people are likely to trust nurses’ feedback because of their expertise in the field (E. Hayes, 2007), and nurses play an important role in the promotion of public health (Kemppainen et al., 2013). In addition, nurses’ regular interactions with patients might engender trust and goodwill, key factors that make people receptive to health-related information (Schollin Ask et al., 2017). Given this research, it is not surprising that many professional societies encourage healthcare professionals to promote physical activity, and they also provide toolkits to equip them to do so (e.g. Long, 2015; Oncology Nursing Society, n.d.).
Despite these possibilities, many nurses do not provide physical activity information or recommendations to their patients (Lamarche & Vallance, 2013), a pattern also observed among healthcare providers in general (Huijg et al., 2015; Laws et al., 2008). To be sure, many note potential benefits (Esposito & Fitzpatrick, 2011), and some nurse practitioners perceive exercise counseling as equally valuable to prescribing medications (Tompkins et al., 2009). However, they also cite a bevy of barriers, including consideration of physical activity as of secondary importance (Ribera et al., 2005), and a lack of understanding about fitness and physical activity represents a meaningful barrier (Marks & Sisirak, 2017). To illustrate the magnitude of the educational deficit among nurses, 63% of nurse practitioners in one study reported that they had limited understanding of obesity prevention, physical activity, and nutrition (Lamarche & Vallance, 2013). Other nurses might believe that people with ASD will experience too many constraints to their participation, such as those previously outlined (Must et al., 2015; Nichols et al., 2019; Obrusnikova & Cavalier, 2011), and therefore forego making such recommendations.
Current study
The purpose of this study was to examine the degree to which nurses recommend physical activity to people with ASD. Even though a number of scholars have examined the role of health professionals in promoting physical activity, comparatively few have examined nurses (Crisford et al., 2018). Further, previous scholars have largely focused on the promotion of physical activity to patients in general, but have comparatively overlooked similar efforts among people with disabilities in general, and people with ASD specifically (Cunningham, 2019; Cunningham & Warner, 2019).
Based on the collective evidence thus far, we hypothesized that perceived benefits of physical activity would be positively associated with nurses recommending physical activity to patients with ASD (Hypothesis 1). Similarly, we predicted that perceived barriers to physical activity would be negatively associated with nurses recommending physical activity to patients with ASD (Hypothesis 2). Whereas the two hypotheses suggest direct effects are possible, we also explored the potential for moderation. A focus solely on direct effects ignores the complexities that arise when people have potentially contrasting information that informs their decisions. Huijg et al. (2015) recognized as much in their systematic review of the literature, arguing that more research was needed to examine the relationships among antecedents. Applied to the current context, it is possible, for example, that nurses will recommend physical activity when they believe the benefits are high and the barriers are low. Or, nurses might be disinclined to advocate for physical activity when the opposite occurs, such that the perceived barriers outweigh the benefits. These possibilities suggest that perceived barriers and perceived benefits might interact to inform nurses’ decision-making. We explore this possibility with the following research question:
Method
Study design and participants
We examined the hypotheses and research question through a mixed methods approach. Using services offered by Qualtrics, we drew from a non-probability-based Internet panel (Hays et al., 2015) to survey the nurses. Previous researchers have shown (a) the value of using Qualtrics panels when seeking feedback from otherwise hard-to-contact populations (Holt & Loraas, 2019) and (b) that Qualtrics panels are frequently more diverse and representative of the population than when other online systems are used (Boas et al., 2020). We asked for a nationally representative sample of nurses to be included in the panel. A power analysis using G*Power (Faul et al., 2009) for multiple regression (moderate effect size of 0.15, α = 0.05, power of 0.95, and number of predictors = 9) indicated a sample of at least 89 was needed. However, because tests of moderation are frequently underpowered (Aguinis et al., 2005; Cunningham & Ahn, 2019), we requested responses from 180 nurses. Each participant received US$15 for their participation.
The sample included nurses (n = 180) in the United States, with sample demographics presented in Table 1. Additional demographic information includes the age range (20–86 years) and occupational tenure range (1–64 years). Most of the participants indicated they “sometimes” interacted with patients with ASD (n = 127, 70.6%), followed by those who indicated “about half the time” (n = 21, 11.7%), “most of the time” (n = 127, 70.6%), and “always” (n = 11, 6.1%).
Sample demographics.

SD: standard deviation.
The final sample demographics mirrored those reported from the 2017 National Nursing Workforce Survey (Smiley et al., 2018). Specifically, Smiley et al. (2018) reported that nurses in the United States were mostly women (90.9%) and mostly White (80.8%). These data are consistent with our sample, which was mostly women (93.3%) and mostly White (80.6%); thus, the participants who took part in the panel are at least representative of the larger population with respect to gender and race.
Measures
Participants responded to a questionnaire where they provided their demographic information and then responded to items measuring the perceived benefits of physical activity for people with ASD, perceived barriers people with ASD face when seeking to be active, and the extent to which they recommend physical activity.
Demographics
Participants responded to questions in which they provided their age (in years), gender (women or man), race (African American, Asian American, Hispanic or Latino, Native American, White, or Other), occupational tenure (measured as years as a nurse), and type of nurse (nursing assistant, licensed practical nurse, registered nurse, and advanced practice nurse).
Perceived benefits
Drawing from Lang et al.’s (2010) review, we developed nine items to reflect perceived benefits of physical activity. The items were preceded by the following stem: “People with autism spectrum disorder who participate in regular physical activity are likely to have.” The items then included “improved physical fitness,” “decreased health concerns,” “better motor control,” “decreased body fat,” “better behavioral outcomes,” “more friends,” “decreased aggressive behavior,” “decreased sedentary behaviors,” and “improved psychological health.” Participants responded to the items using a 7-point scale from 1 (strongly disagree) to 7 (strongly agree).
We examined the dimensionality of the scale through a principal components analysis with varimax rotation. Results demonstrated support for a one-factor solution that explained 65% of the variance. All factors loadings were greater than 0.73, which is higher than the 0.40 threshold suggested by Hair et al. (2010). Thus, we treated perceived benefits as a one-dimensional construct and computed the overall mean of the items to reflect the final score. The reliability for the scale was acceptable (α = 0.93).
Perceived barriers
Drawing from Must et al. (2015), seven items were developed to measure perceived barriers people with ASD experience in sport and physical activity. The stem read “Please rate your agreement with the degree to which the following serve as barriers to people with ASD’s physical activity participation.” The items included “people with autism spectrum disorder have behavioral problems,” “people with autism spectrum disorder require too much supervision,” “sports are over-stimulating,” “people with autism spectrum disorder have difficult social skills,” “people with autism spectrum disorder do not feel welcome,” “coaches and organizers lack the skills to include people with autism spectrum disorder,” and “other sport participants exclude people with autism spectrum disorder.” Each item was followed by 7-point scale from 1 (strongly disagree) to 7 (strongly agree).
As with perceived benefits, we first examined the dimensionality of the scale through a principal components analysis with varimax rotation. Results demonstrated support for a one-factor solution that explained 43% of the variance. All factors loadings were greater than 0.57, thereby surpassing the 0.40 threshold recommended by Hair et al. (2010). Given the findings, we treated perceived barriers as a one-dimensional construct and computed the overall mean of the items to reflect the final score. The reliability was acceptable (α = 77).
Recommendations
We measured recommendations using three items. Ajzen (1991) suggested measuring intentions and behaviors in a time-bound manner. Thus, the stem read “Think about your interactions with people with autism spectrum disorder over the past three months. How frequently have you:” The three items were “suggested they engage in more physical activity,” “talked to them about physical activity,” and “told them they need to take part in regular physical activity.” Response options ranged from 1 (never) to 5 (always), and the reliability was acceptable (α = 93). We used the mean of the three items to reflect the final score.
Open-ended
Finally, we gave the participants a chance to add qualitative responses by answering the following question: “Do you have anything else to add about physical activity and sport for people with autism spectrum disorder?”
Data analysis
As ours is a mixed methods study, we first analyzed the quantitative data and then proceeded to the qualitative analyses. We first computed descriptive statistics (means, standard deviations, and bivariate correlations) for all variables. To test the hypotheses and examine the research question, we computed a moderated regression model using PROCESS (A. F. Hayes, 2018; Model 1). We included the demographic variables (age, race, gender, registered nurse or not, and interactions with patients with ASD) as controls, and used the mean-centered first-order variables (benefits of physical activity and barriers to physical activity). We did not include occupational tenure because of the high association with age. Recommendations served as the dependent variable.
For the qualitative data, we engaged in inductive thematic analysis (Braun & Clarke, 2006; see also Creswell, 2003) to analyze the qualitative responses to the question “Do you have anything else to add about physical activity and sport for people with autism spectrum disorder?” The inductive approach represents “a process for coding the data without trying to fit into a pre-existing coding frame, or the researcher’s analytical preconceptions (Braun & Clarke, 2006, p. 83). Specifically, we initially sorted the text into codes and then grouped the codes into larger abstract categories, or themes. We sought to identify semantic themes, whereby we described the patterns of the data and then later interpret and link to the existing scholarship (see also Patton, 1990).
Community involvement
We designed the study with various forms of involvement from the autism community. The first author is a caregiver for a child with ASD. The second author is a professor whose focus is on physical activity and sport and who also coached baseball teams for players with various special needs, including players with ASD. The third author is a registered nurse and university professor whose teaching includes topics related to ASD. The research team did not, however, include individuals with ASD or their immediate family members.
Results
Descriptive statistics
Means, standard deviations, and bivariate correlations for all data are reported in Table 2. Nurses were moderately likely to recommend physical activity to their patients with ASD. In terms of the correlations, perceived benefits and perceived barriers to physical activity were not related to one another, perceived benefits held a moderate association with recommendations, and perceived barriers was not associated with recommendation. Further, racial minority nurses were significantly younger and had been in the profession for a shorter period of time than had their White counterparts. Racial minority nurses were also more likely to recommend physical activity for patients with ASD. Other significant correlates of recommendations included the amount of interactions with patients with ASD and perceived benefits. Finally, women perceived more barriers than did men.
Means, standard deviations, and bivariate correlations.
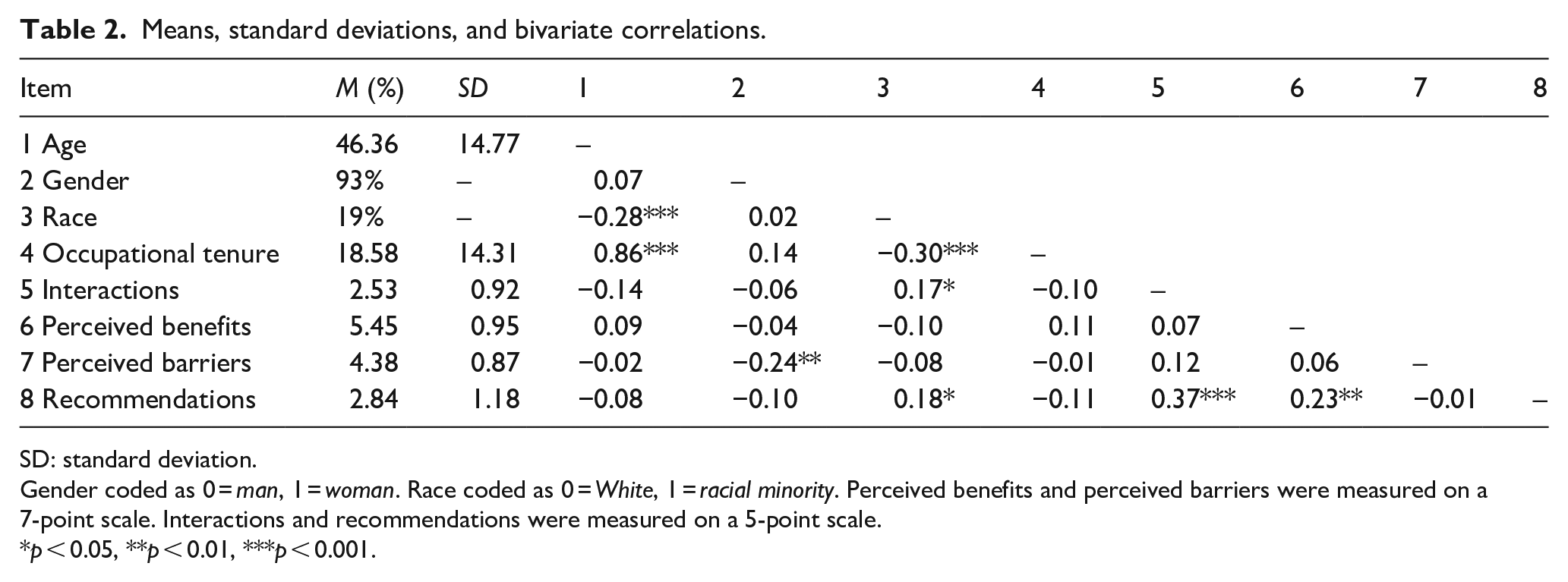
SD: standard deviation.
Gender coded as 0 = man, 1 = woman. Race coded as 0 = White, 1 = racial minority. Perceived benefits and perceived barriers were measured on a 7-point scale. Interactions and recommendations were measured on a 5-point scale.
p < 0.05, **p < 0.01, ***p < 0.001.
Hypothesis testing
Results from the regression analysis are shown in Table 3. The overall regression model explained 22.5% of the variance (p < 0.001). Hypothesis 1, which predicted that perceived benefits of physical activity would be positively related to recommendations, was supported (B = 0.272 SE = 0.086, p = 0.002, lower level of confidence interval (LLCI): 0.102, upper level of confidence interval (ULCI): 0.443). On the other hand, Hypothesis 2 was not supported, as perceived barriers to physical activity were not related to recommendations (B = 0.010, SE = 0.107, p = 0.928, LLCI: −0.201, ULCI: 0.220).
Results of the PROCESS regression analysis examining the effects of perceived benefits, perceived barriers on nurse recommendation of physical activity to patients with ASD.
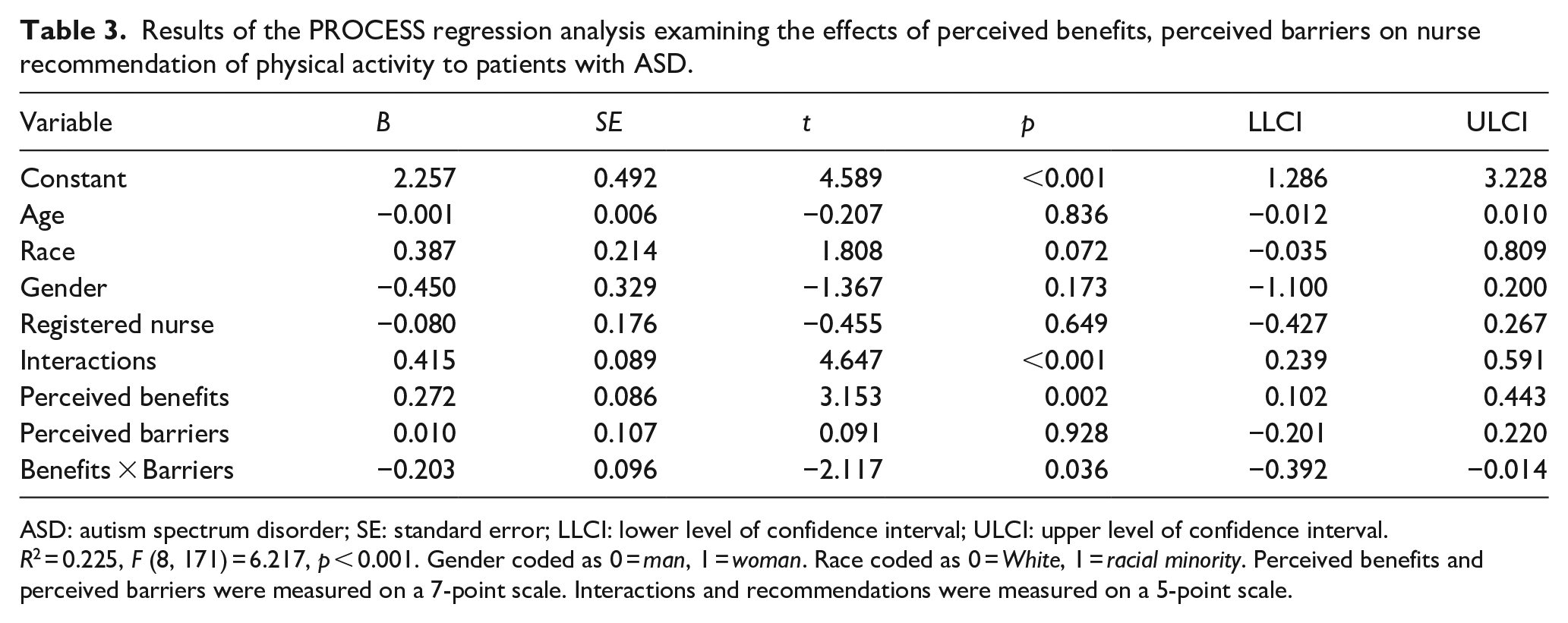
ASD: autism spectrum disorder; SE: standard error; LLCI: lower level of confidence interval; ULCI: upper level of confidence interval.
R2 = 0.225, F (8, 171) = 6.217, p < 0.001. Gender coded as 0 = man, 1 = woman. Race coded as 0 = White, 1 = racial minority. Perceived benefits and perceived barriers were measured on a 7-point scale. Interactions and recommendations were measured on a 5-point scale.
With respect to the research question, we observed a significant perceived benefits × perceived barriers interaction, and the interaction explained 2% unique variance (p = 0.036). We then computed simple slopes and plotted the interactions, per Cohen et al.’s (2003) recommendations. When perceived barriers were low, perceived benefits held a positive, significant association with recommendations (B = 0.450, SE = 0.118, p < 0.001, LLCI: 0.217, ULCI: 0.683). However, when perceived barriers were high, the relationship between perceived benefits and recommendations was no longer significant (B = 0.095, SE = 0.123, p = 0.773, LLCI: −0.147, ULCI: 0.337). We show the pattern of results in Figure 1.
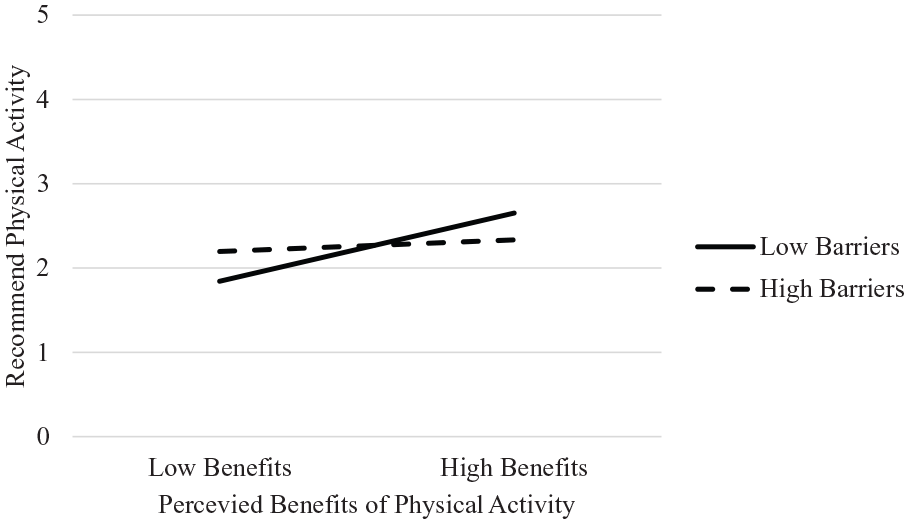
Perceived benefits, perceived barriers, and recommendation of physical activity.
Qualitative responses
As the second portion of the mixed methods study, we analyzed the qualitative responses. Consistent with Braun and Creswell (2006), and our approach of identifying semantic themes, we describe the patterns of the data and then, in the “Discussion” section, interpret and link to the existing scholarship We present an overview of the findings in Table 4, where we offer illustrative quotations, codes, and emergent themes.
Illustrative quotations, codes, and themes.

ASD: autism spectrum disorder.
Praise for physical activity
Many of the nurses offered general praise of physical activity. One nurse wrote, “Physical activity is beneficial to anyone, including those with ASD,” whereas another wrote that physical activity “is needed by the body regardless of other disorders.” Another participant wrote, “More things like sports activity need to be offered to people with autism,” while still another nurse offered the following, “The more movement and activity you have the better off you will be.” These comments are reflective of the others in this theme, all of which centered around the general praise for physical activity and sport.
Barriers to physical activity
Codes grouped in the next theme centered on the barriers persons with ASD experience in accessing sport and physical activity. This theme included exclusion and the nature of ASD. With respect to exclusion, one nurse noted, “It is easier to exclude than to include.” Another nurse offered a fuller explanation, noting the following: I personally think people with ASD are greatly misunderstood. Once given the opportunity, I believe that they could excel at anything. It’s takes patience to let them express themselves and get their points across. So many times, people lack that.
Relatedly, some nurses suggested that people with ASD had limited access to be active. One nurse commented that there was a “lack of resources for them,” while another added, “Young people living with an autism spectrum disorder (ASD) have less access to sports and physical activity.” As another example, a nurse suggested, “They are very limited in what they are offered and allowed to do.”
Other nurses pointed to the nature of ASD. One nurse wrote the following: I believe the main barrier to overcome is over stimulating the individual and knowing when to stop. Also need to take into consideration the individuals’ routines and their reactions to changes I think the main thing is having people trained to deal with the disorder.
Another nurse commented, “Some patients do not like the touch of physical activity.”
Benefits of physical activity
Other nurses focused on the benefits of physical activity for people with ASD, including psychological benefits and social benefits. With respect to the former codes, one nurse commented, “It would definitely benefit them both physically and mentally. May cut down on some of the more rigid behaviors they tend to have.” Other focused on how physical activity might spur confidence and self-assurance: “Physical activity is very good for people with autism spectrum disorder; it helps them develop more security on them self [sic].”
Most of the benefits focused on the social elements. One nurse explained the following: I feel participating in physical activity, especially organized team activities, is a great place for clients with ASD to improve on social skills and find a healthy avenue to focus. For some the physical activity is a place they can interact with peers without the 1 on 1 conversations that can prove to be very stressful.
A different nurse commented, “Physical activity even walking in a group would give everyone a sense of community and would help get them moving.” Another nurse relayed the success story of which she was aware: Sports create structure as well which help individuals with ASD because it teaches them discipline and they learn about normal social interaction. I know a child who was put into hockey, football, lacrosse, track all at the age of 5 and up he is now a freshman in college living 5 hours away from home and succeeding because he learned how to do things with his sports teams.
Ideas for engagement
Finally, many of the nurses offered suggestions for ways to get people with ASD more involved in physical activity and sport, or what we term ideas for engagement. These ideas fell into two categories: personnel and design.
With respect to personnel, nurses advocated for training of coaches, administrators, and other players so that they are better equipped to include people with ASD. Examples included “Advanced training for involved coaches/volunteers greatly improves results during gaming,” “More physical education teachers/coaches should be required to participate in continuing education regarding this issue,” and “There should be more awareness and training for younger students on how to interact and play with children who had ASD.” Others suggested specific steps they took to include people with ASD, such as employing occupational therapists with specific training to effectively include people with ASD.
Other nurses offered design recommendations on how to design sport and physical activity for people with ASD. Some focused on the nature of the activity, suggesting, “Make it fun for them and they are more likely to participate more.” Another nurse offered the following: I work with children who are on the Autism Spectrum and we have a playground and encourage fitness. We have a pool and along with wearing a life jacket we encourage water play. Low impact for the less coordinated children.
Another nurse suggested, “Since loud noises and crowds can be an issue, I suggest sports with smaller audiences and less commotion if that is a barrier to someone with ASD.”
Discussion
Regular physical activity promotes many physical, psychological, and social benefits (Ding et al., 2016), and this is especially the case for people with ASD (see also McCoy & Morgan, 2020; Nichols et al., 2019)—individuals who also experience comparatively poor health (Ayres et al., 2018; Bilder et al., 2013; Croen et al., 2015). Given these trends, communicating the benefits of physical activity is particularly important (Sorensen & Zarrett, 2014), and nurses can play a key role in doing so (Kemppainen et al., 2013). Unfortunately, many nurses do not offer such information to their patients because of a variety of barriers and constraints (Lamarche & Vallance, 2013; Marks & Sisirak, 2017; Ribera et al., 2005). The purpose of this mixed methods study, therefore, was to investigate the degree to which nurses recommend physical activity to people with ASD. Results show that nurses were only moderately likely to recommend physical activity to their patients with ASD. They were most likely to offer such recommendations when perceived benefits were high and perceived barriers were low. Analysis of the qualitative data revealed nurses’ recommendations for involving people with ASD in physical activity, including personnel considerations and specific design considerations. In the following space, we overview the contributions of the study, offer practical implications, note limitations, and suggest avenues for future research.
Overview and contributions
Our research makes several contributions to the literature. First, our focus on nurses and their interactions with patients with ASD advances the current scholarship. Few investigators have focused on physical activity recommendations among nurses (Crisford et al., 2018), even though this group of healthcare providers can have regular interactions with their clients with ASD. Second, we also found that, even though nurses were just moderately likely to recommend physical activity, there are factors that influence their decisions to do so, including previous interactions with patients with ASD. It is possible that the positive association is simply a function of the chance to promote physical activity—the more one sees patients with ASD, the more chances they have to make recommendations. From another perspective, it is possible that the previous interactions resulted in decreased biases toward patients with ASD (Maunder & White, 2019). In this case, the nurses would have a better understanding of the benefits and barriers patients with ASD might experience and therefore be able to recommend the appropriate physical activities moving forward.
Third, although we found that perceived benefits held a positive association with physical activity recommendations, this relationship was qualified by a significant perceived benefits × perceived barriers interaction. Previous researchers have largely focused on the additive effects of potential antecedents, and while helpful, additive effects frequently only tell a portion of the story. Instead, moderators can offer a deeper understanding of when and under what conditions relationships take place (Cunningham & Ahn, 2019). Huijg et al. (2015) seemingly recognized as much, too, as they encouraged additional examination of how the relationship among the antecedents of physical activity recommendations. In our study, we found that when perceived barriers were high, the perceived benefits were not related to physical activity recommendations; however, benefits were positively associated with recommendations when nurses believed the barriers to be low. These findings suggest that nurses weigh the tradeoffs between benefits and barriers when suggesting physical activity to people with ASD. These findings are consistent with research from Arnell et al. (2020) where parents of teens with ASD noted the many benefits of physical activity but found that promoting such behaviors was “an overwhelming task,” given personal and social barriers in place. Thus, it is important for researchers and policy makers to take into account both benefits and barriers, as well as their interaction, when considering physical activity promotion.
Finally, our qualitative analyses allowed for a more nuanced understanding of how nurses understood physical activity for patients with ASD. The themes related to benefits (psychological and social) and barriers (exclusion and nature of ASD) corresponded with the items used to quantitatively measure those constructs. The nurses also identified strategies for making sport and physical activity more inclusive. These included training coaches and administrators to more effectively lead participants with ASD. The nurses also offered suggestions related to design elements, such as ensuring that low-impact activities, such as swimming, are offered. These themes are consistent with the need to build capacity in sport organizations to ensure equitable provision of sport for all persons (Cunningham & Warner, 2019; Wicker & Breuer, 2014).
Practical recommendations
Results from the study lend themselves to practical recommendations, too. We have already noted some of these, having overviewed the nurses’ recommendations. There are also implications for nurses’ education and professional development. Nurses who are reticent to recommend physical activity report that other prescribed behaviors are more important (Ribera et al., 2005), and lack an understanding about physical activity and fitness promotion (Marks & Sisirak, 2017). The nurses in one study reported an educational deficit related to obesity prevention, physical activity, and nutrition (Lamarche & Vallance, 2013). Nursing programs can help alleviate these gaps by including modules on the benefits of physical activity and ways to promote it. From a different perspective, nurses might benefit from developing their motivational interviewing, or “a collaborative, person-centered form of guiding to elicit and strengthen motivation for change” (Miller & Rollnick, 2009). Systematic reviews suggest such methods can prompt moderate physical activity increases among people who are otherwise unlikely to be active (O’Halloran et al., 2014). Future research is needed in to further explore this possibility.
But, the onus of promoting physical activity for people with ASD does not fall all on the shoulders of nurses. Caregivers can provide important social support needed to facilitate more physical activity among people with ASD. Indeed, recent research has demonstrated that supportive others “play an instrumental role in the physical activity behaviour of children and youth with autism spectrum disorder” (Brown et al., 2020). For their part, sport and recreation managers can take steps to promote physical activity for all populations. Ohrberg (2013) offered several recommendations related offering services for people with ASD, specifically; (a) build organizational capacity through staff training and the development of a department handbook; (b) draw from local expertise by way of a small group of parents, educators, and healthcare professionals; (c) leverage online resources offered by the Autism Society of America, Autism Speaks, and the Autism Science Foundation, among others; (d) offer support for families of people with ASD; and (e) provide reasonable accommodations to ensure maximum participation. We build on Ohrberg’s work to offer a sixth strategy: ensure that nurses and other healthcare professionals have the materials needed to promote physical activity engagement. This includes detailing the benefits of being active, the opportunities in the city or municipality, and success stories.
Limitations and future directions
As with all research, our study is not without limitations. First, our qualitative data were limited to the nurses’ responses to an open-ended prompt. Their feedback offered valuable information, but engaging in more in-depth interviews is likely to have yielded a fuller account of their perspectives. Future researchers should consider employing semi-structured interviews, focus groups, or other techniques to further examine nurses’ decision to recommend physical activity to patients with ASD. Second, the nurses responded to the open-ended question on the same survey where they completed the questionnaire; thus, their responses might have been primed by the other items to which they responded. We do note, however, that it is common for participants in qualitative studies to have an understanding of the topic or general questions prior to their participation. Related to this point, we collected self-report data from a single questionnaire; thus, common method bias is a potential limitation for the quantitative data (Podsakoff et al., 2003). We do note, however, that the concern is assuaged to some degree by our testing of moderation (instead of simple additive effects) and the mixed methods approach.
Finally, we note potential areas for future research. First, the nurses in our study identified personnel considerations and design characteristics that could help to get more people with ASD involved in sport and physical activity. Future researchers could examine the efficacy of these recommendations or investigate the degree to which sport and recreation managers employ them. Second, we have drawn from the perspective of nurses, but they offer one side of the story. Future researchers might consider asking people with ASD and their families how they prefer to learn about physical activity and sport opportunities, as well as how frequently other healthcare providers recommend physical activity to people with ASD. Finally, we recommended that providing nurses with more information about the benefits of physical activity and ways for their patients to be involved could help motivate them to recommend such activities. Future researchers could examine these linkages, specifically. Given the value of engaging in sport and physical activity for all people, including those with ASD, such efforts are needed.