
Abstract
Parental self-efficacy, parents’ beliefs in their ability to successfully parent their child, plays an important role in family outcomes when a child has autism spectrum disorder. It is important to consider therapeutic self-efficacy, one’s feelings of self-efficacy regarding their implementation of an intervention, within parent-mediated interventions. The goal of this mixed methods study was to better understand factors that relate to parents’ therapeutic self-efficacy when implementing a telehealth-based parent-mediated intervention. Participants were 51 parents of children with autism spectrum disorder between 17 and 83 months old. Parents reported generally high therapeutic self-efficacy, and global parental self-efficacy was significantly related therapeutic self-efficacy. Thematic analysis of parents’ written reflections of the intervention’s lessons identified four themes that related to therapeutic self-efficacy: the importance of a good fit between the child’s skills and the intervention, the importance of a good fit between the parent’s interaction style and the intervention, environmental factors support intervention use, and the importance of the child’s response to the intervention. Several themes differed for parents with higher and lower therapeutic self-efficacy. Findings suggest that global parental self-efficacy plays an important role in parental therapeutic self-efficacy in parent-mediated interventions. Coaches should specifically ask about the child’s skills, parent’s interaction style, environmental challenges, and child’s response as they support parents in learning.
Lay abstract
Parental self-efficacy refers to parents’ beliefs in their ability to successfully parent their child. Parental self-efficacy plays an important role in family outcomes when a child has autism spectrum disorder. It is important to consider therapeutic self-efficacy, one’s feelings of self-efficacy regarding their implementation of an intervention, within parent-mediated interventions. The goal of this mixed methods study was to better understand factors that relate to parents’ therapeutic self-efficacy when using a telehealth-based parent-mediated intervention. Participants were 51 parents of children with autism spectrum disorder between 17 and 83 months old. Parents had generally high therapeutic self-efficacy, and global parental self-efficacy was significantly related therapeutic self-efficacy. Parents’ written reflections revealed four themes that related to their therapeutic self-efficacy: the importance of a good fit between the child’s skills and the intervention, the importance of a good fit between the parent’s interaction style and the intervention, environmental factors support intervention use, and the importance of the child’s response to the intervention. Several themes differed for parents with higher and lower therapeutic self-efficacy. Findings suggest that global parental self-efficacy plays an important role in parental therapeutic self-efficacy in parent-mediated interventions. To support parents in learning, coaches should ask about the child’s skills, parent’s interaction style, environmental challenges, and child’s response.
Keywords
Parental self-efficacy (PSE) refers to parents’ beliefs in their ability to successfully parent their child (Gross & Rocissano, 1988; Jones & Prinz, 2005). In the parenting literature, PSE has been consistently associated with positive parenting practices, coping, and persistence in the face of demanding parenting situations (see Jones & Prinz, 2005 for a review). PSE has had an impact on outcomes related to the parent and child relationship, parental mental health, and outcomes related to child development including socio-emotional, behavioral, and academic and school-related functioning (see Albanese et al., 2019 for a review).
PSE may play a particularly important role in family outcomes when a child has autism spectrum disorder (ASD). Research suggests that having a child with ASD can negatively impact PSE. For example, mothers of both a child with and without ASD reported a significantly lower sense of self-efficacy in parenting their child with ASD than parenting their typically developing child (Meirsschaut et al., 2010). In addition, PSE is inversely related to parenting stress (Batool & Khurshid, 2015; Karp & Kuo, 2015), and has been found to mediate the effect of child behavior problems on mothers’ anxiety and depression and moderate the relationship between behavior problems and anxiety in fathers (Hastings & Brown, 2002). This association is important, as a substantial body of literature suggests that parents of children with ASD experience higher levels of parenting stress and psychological distress than parents of typically developing children and children with other developmental challenges (e.g. Karst & Van Hecke, 2012).
Furthermore, there is evidence that parents who participate in parent-mediated interventions, in which they are taught strategies to help their child develop social communication skills or manage their child’s behavior, experience increases in PSE and concomitant decreases in parenting stress (Keen et al., 2010). Conversely, PSE is a significant predictor of parent involvement in their child’s intervention (Solish & Perry, 2008) and may also influence parents’ successful implementation of strategies in parent-mediated interventions (Schertz & Odom, 2007). For example, a qualitative study of parents’ experience with a parent-mediated joint attention intervention indicated that parental competence and self-efficacy positively impacted the effectiveness of the intervention (Schertz & Odom, 2007).
Research on PSE in ASD has traditionally used global measures of PSE that examine parents’ sense of competence in the parenting role, rather than measures of task-specific self-efficacy, that assesses their sense of competence in specific parenting behaviors. This is surprising given that research indicates parents’ self-efficacy in managing difficult child behaviors was a better predictor of their positive parenting practices than general PSE, although both types of self-efficacy were related (Sanders & Woolley, 2005). In the context of parent-mediated interventions for children with ASD, therapeutic self-efficacy is task-specific and may be particularly important to consider, given that these programs are designed to teach parents to use specific intervention strategies. What little work has been done suggests that several parent, child, and environmental factors influence parents’ therapeutic self-efficacy for children with ASD. For example, parenting stress, the severity of the child’s autism, and the amount of support received from the program all predicted mothers’ level of therapeutic self-efficacy in an early intensive behavioral intervention program (Hastings & Symes, 2002).
The goal of this mixed methods study was to better understand factors that relate to parents’ therapeutic self-efficacy when implementing a telehealth-based parent-mediated intervention. The first aim was to use quantitative data to identify parent and child demographic factors that relate to parents’ therapeutic self-efficacy while completing the program. The second aim was to identify qualitative themes related to parents’ therapeutic self-efficacy to better understand parents’ experience learning and using the intervention with their child and to inform additional supports that may be needed.
Method
Methodological and theoretical approach
A convergent design with greatest emphasis on qualitative data (quan + QUAL) was utilized for this mixed methods study. Data were gathered quantitatively through child assessment, parent interview and self-report measures, and were gathered qualitatively through short answer, reflection questions from an online parent-mediated intervention program. Quantitative methods provided information about the relationship between parent and child factors and therapeutic self-efficacy. Qualitative methods then provided a deeper insight into parents’ experiences with intervention implementation, and how they relate to therapeutic self-efficacy.
Participants
Participants were parents of a child with ASD between the ages of 17 and 83 months (M = 45.38, SD = 14.29) who participated in one of the two research studies evaluating the efficacy of a telehealth-based parent-mediated intervention (Ingersoll et al., 2016). Participants in the pilot study (n = 28) were enrolled between 2012 and 2014; participants in the full-scale efficacy trial (n = 23) were enrolled between 2015 and 2020 (recruitment ongoing). To participate in either trial, the parent had to identify as the child’s primary caregiver and be proficient in English, the child needed to have an expressive language age equivalent no higher than 48 months on the Mullen Scales of Early Learning (MSEL; Mullen, 1995) and needed to meet Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria for autism spectrum disorder, and receive an “autism” or “autism spectrum” on the Autism Diagnostic Observation Schedule–Second Edition (ADOS-2; Lord et al., 2012). The only difference in inclusion criteria was that the randomized controlled trial (RCT) study had an extended age eligibility of up to 84 months old from the pilot study’s 73 month cutoff. All assessments and eligibility requirements were determined through parent phone screenings and in-person assessment conducted by blinded graduate student and postdoctoral researchers.
Pilot study participants were randomly assigned to a self-directed or therapist-assisted group. Participants in the full-scale study were randomly assigned to a self-directed, therapist-assisted, or informational control group. As part of their participation, parents in the self-directed and therapist-assisted groups received access to a self-directed web-based tutorial, which included open-ended reflection responses for each of 12 lessons. Only parents who participated in the self-directed or therapist-assisted groups and who completed the open-ended reflection questions for at least five lessons of the online tutorial were included in this study, yielding a total of 51 participants (17 self-directed and 34 therapist-assisted).
Intervention
ImPACT Online is a secure, password-protected, website that was adapted from the naturalistic, developmental behavioral intervention (NDBI; Schreibman et al., 2015) called Project ImPACT (Ingersoll & Dvortcsak, 2010). Project ImPACT consists of 12, 75-min self-directed lessons that teach parents to promote their child’s social communication skills during play activities and daily routines (Ingersoll et al., 2017). The intervention uses a pyramid to demonstrate the flow of the use of intervention strategies, with strategies promoting the child’s engagement at the bottom and prompting for new skills at the top. The self-directed lessons included a narrated slideshow, PDFs of the written manual, self-check questions, video exercises, a homework plan, reflection questions (used as qualitative data for this study), and access to a video library containing video examples of the intervention.
Measures
Family demographics
At intake, parents provided information on their family demographics through an online survey. Parents provided information on their gender, education level, their child’s gender, and their child’s age. See Table 1 for parent and child demographics.
Parent and child demographics.
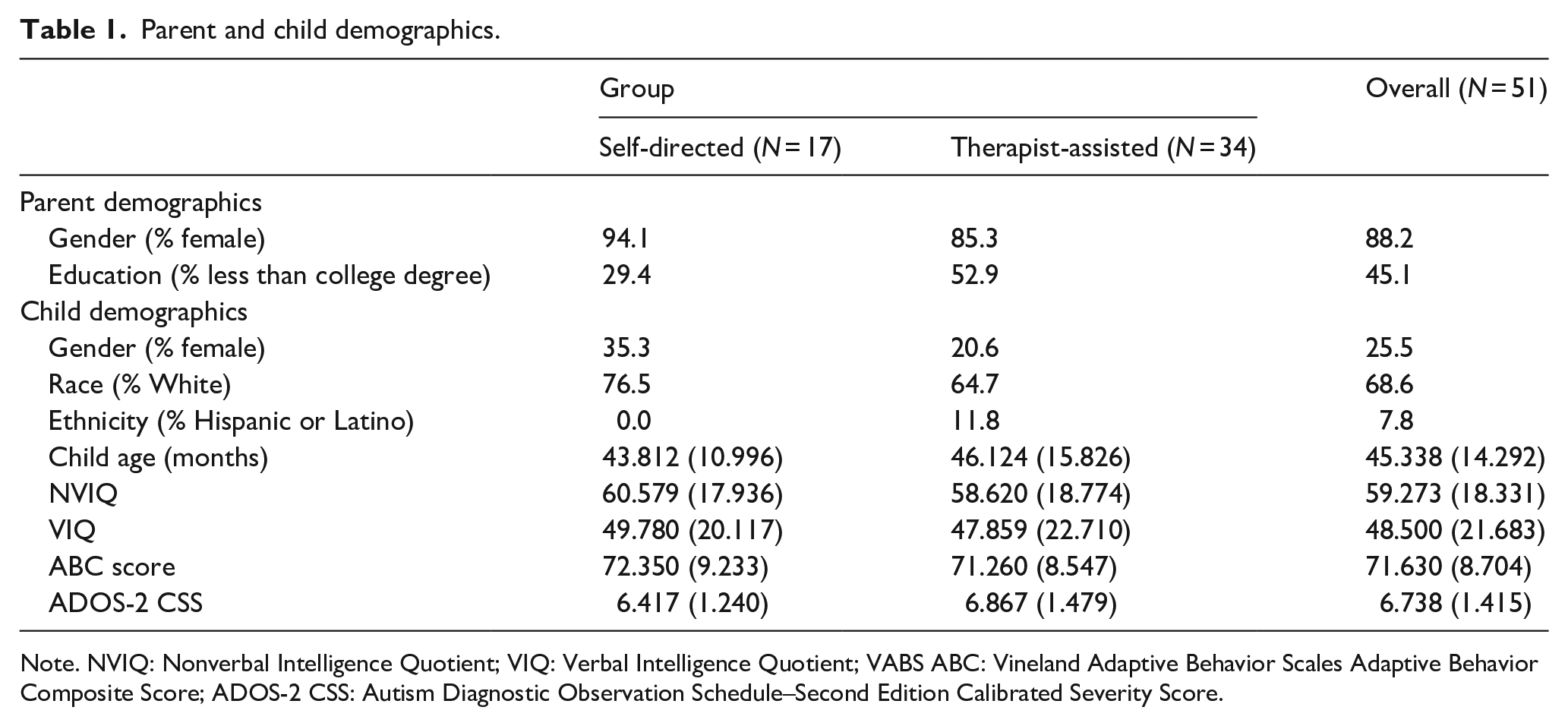
Note. NVIQ: Nonverbal Intelligence Quotient; VIQ: Verbal Intelligence Quotient; VABS ABC: Vineland Adaptive Behavior Scales Adaptive Behavior Composite Score; ADOS-2 CSS: Autism Diagnostic Observation Schedule–Second Edition Calibrated Severity Score.
Global parenting self-efficacy
Parents completed the Parenting Sense of Competence (PSOC) scale at intake as a measure of global parent self-efficacy (Gibaud-Wallston & Wandersman, 1978). The PSOC is a 17-item scale, with each item rated on a six-point Likert-type scale. Higher scores on the items represent higher PSE. The PSOC is a widely used and tested measure. A factor analysis of the PSOC by Gilmore and Cuskelly (2008) found three subscales having sufficient internal consistencies using Cronbach’s alpha for both mothers (0.62–0.72) and fathers (0.57–0.76).
Autism severity
The ADOS-2 Calibrated Severity Scores (CSS) were used as a measure autism severity (Lord et al., 2012).
Child developmental level
The Mullen Scales of Early Learning (MSEL) was administered at intake to evaluate the developmental level of participants (Mullen, 1995). The MSEL is a standardized developmental assessment which provides scores in four domains: Receptive Language, Expressive Language, Fine Motor, and Visual Reception. A verbal IQ score was calculated for each child by dividing the Receptive Language and Expressive Language subscales average age equivalent scores by chronological age and multiplying by 100 (Bishop et al., 2011). A nonverbal IQ score was calculated for each child by doing the same with the Fine Motor and Visual Reception subscales age equivalents scores.
Child adaptive functioning
Parents completed the interview version of Vineland Adaptive Behavior Scales–Second Edition (VABS-II; Sparrow et al., 2005) by phone at intake, as a measure of the child’s adaptive functioning. The VABS-II is a standardized assessment of adaptive functioning that measures behaviors in four domains: Communication, Daily Living Skills, Socialization, and Motor Skills. The Adaptive Behavior Composite (ABC) score was used to as a measure of child overall adaptive functioning.
Therapeutic self-efficacy
Parents completed a five-item scale adapted from the Parent Adherence to Treatment and Competence measure (a-PATC; Kasari et al., 2010) after each lesson as part of the online tutorial. This scale was used to measure parents’ feelings of self-efficacy regarding their implementation of the intervention strategies presented in the lesson. The adapted measure consisted of three questions concerning parental adherence to treatment protocol: (1) I made time to carry out the strategies, (2) I found it natural to carry out the strategies, and (3) I made an effort to carry out the strategies. Two questions concerning parental competence: (1) I was confident carrying out the strategies, and (2) I was comfortable with the strategies. Items were rated on a five-point Likert-type scale with higher scores representing higher therapeutic self-efficacy within the intervention. Cronbach’s alphas for the a-PATC for each lesson were ⩾0.67 suggesting adequate internal consistency. Parent a-PATC scores were averaged across all lessons to calculate one overall a-PATC score per parent.
Qualitative data
As part of the online tutorial, parents were asked to complete two to three open-ended reflection questions at the end of each lesson, for lessons 3–12 (10 lessons total). Lessons 1 and 2 are for introduction to the intervention and do not include intervention strategies, so they were excluded for the purpose of this study. The majority of participants completed all 10 lesson reflections (M = 9.26; SD = 1.37). Reflection questions asked parents to describe their child’s response to the intervention techniques, as well as which aspects of the techniques the parent felt were successful and difficult to implement.
Data analysis
Quantitative analysis
Bivariate Spearman’s correlations were used to examine the relationship between group assignment, child age, ADOS-2 CSS, child verbal and nonverbal IQ, child adaptive skills, parent demographics and global PSE at intake, and therapeutic PSE throughout the program.
Qualitative analysis
Thematic analysis (Braun & Clarke, 2012) using an inductive approach was utilized to analyze the semantic content of the parent responses to the reflection questions. Parent-written responses for each lesson were extracted from the online program. The first author and an undergraduate research assistant independently read through the written responses to familiarize themselves with the data and generated a list of potential codes. They then met to finalize the codes using an iterative process and created a codebook. The first author and research assistant met twice a week to consensus-code all responses using Dedoose. Next, both authors independently reviewed the parent responses with the assigned codes and met to organize the codes into themes and subthemes. Themes that were present across the data set were finalized through multiple meetings with the authors and colleagues. To examine similarities and differences in the experience of parents who reported lower and higher therapeutic self-efficacy, a median split of parents’ mean rating of therapeutic self-efficacy was conducted to create a higher therapeutic self-efficacy (HTSE; n = 24) group and lower therapeutic self-efficacy (LTSE; n = 27) group.
Mixed methods analysis
The overall frequency of themes and subthemes, as well as the number of parents endorsing each theme and subtheme from the HTSE and LTSE groups were compared (Bailey et al., 2020). To facilitate the mixed methods analysis, a joint display of the quantitative and qualitative data was developed by the authors based on a structure that the authors felt best represented the key findings (see Table 3).
Results
Quantitative results
Overall, a-PATC scores ranged from 3.0 to 4.59 (M = 3.92, SD = 0.35) out of 5.0, indicating that the parents reported generally high therapeutic self-efficacy. Bivariate Spearman’s correlations found that global PSE on the PSOC at intake was significantly and positively related to parent-reported therapeutic self-efficacy on the a-PATC (ρ = 0.329, p < 0.05; Table 2). Group assignment, parent education level, child age, autism severity, adaptive skills, and verbal and nonverbal IQ were not significantly related to a-PATC scores.
Correlations between variables of interest at time 1.

Note. A-PATC: adapted-Parent Adherence to Treatment and Competence; VABS ABC: Vineland Adaptive Behavior Scales Adaptive Behavior Composite Score; PSOC: Parenting Sense of Competence Scale; NVIQ: Nonverbal Intelligence Quotient; VIQ: Verbal Intelligence Quotient; ADOS-2 CSS: Autism diagnostic observation schedule–Second Edition Calibrated Severity Score.
p < 0.05. **p < 0.01.
Qualitative results
The importance of a good fit between the child’s skills and the intervention
Most parents indicated that their child’s abilities influenced their intervention implementation. Parents who perceived their child’s skills to be at the appropriate developmental level for the technique described their child’s skills as a facilitator of their use of the intervention. For example, a parent described her experience with language prompting: “Leading comments seemed to work best with him. He’s very intuitive and picks up easily on what people are inferring.” In contrast, parents who perceived their child’s skills as being less well-developed, described their child’s skills as a barrier to their use of the intervention. One parent expressed, I can tell that [he] tries really well to follow through with it but I often see that he shies away [. . .] I am thinking because it is a little more than he can handle [. . .] when he tries to follow directions [he] gets lost carrying through.
Some parents also expressed that strategies from the top of the ImPACT pyramid, such as prompting, did not feel as successful as strategies from the bottom of the ImPACT pyramid did with their child. Although not as commonly mentioned, some parents described difficulty implementing the intervention when their child’s skill level seemed to be above the skills that the strategies were targeting. A parent shared, “We struggled with gesture imitation. [He] uses a lot of words and we are trying to encourage that so when he uses a gesture, we typically ask for him to use his words instead of the gesture.”
While parents in both groups mentioned this theme, it was more prevalent among parents in the LTSE group (theme occurrence: HTSE = 29, LTSE = 48). Furthermore, parents in the HTSE group were more likely to describe their child’s skills as a facilitator (subtheme count: HTSE = 8, LTSE = 6), whereas parents in the LTSE group were more likely to describe their child’s skills as a barrier (subtheme count: HTSE = 14, LTSE = 35), with most parents viewing their child’s skills as less well-developed. Restricted and repetitive behaviors (RRBs) were also mentioned as a specific behavior that interfered with intervention implementation. One parent shared that, “[He] just wants to revert back to his ritualistic behavior of lining up toys or pushing buttons and so I’m still working on ways of breaking him of this while not just taking over the lead entirely.”
The importance of a good fit between the parent’s interaction style and the intervention
Many parents described the importance of their own feelings and experiences with intervention implementation. Parents who perceived the techniques as natural to use described their implementation of the intervention as easier. When discussing the use of animation, a parent indicated, “I supposed in some ways I was already animated; in part because of my education background.” Parents also mentioned that they had fun during interactions with their child while implementing the techniques. One parent reflected that playing with his daughter felt, “very easy and enjoyable.”
Parents in both groups equally mentioned this theme (theme occurrence: HTSE = 59, LTSE = 60). However, parents in the HTSE group were more likely to describe intervention strategies as fun and natural (subtheme count: HTSE = 35, LTSE = 20), whereas parents in the LTSE group were more likely to describe difficulty with implementing intervention strategies (subtheme count: HTSE = 28, LTSE = 43). One parent shared, I’m not sure I used the 3-prompt sequence properly . . . I think I gave her a few more prompts and a little more time while expecting an answer; and may not have finished the reinforcement and simplification on prompts she struggled with.
Parents also mentioned that they struggled with pacing (i.e. knowing when to use strategies) during playtime and also struggled with balancing the use different strategies and parts of the pyramid.
Environmental factors support intervention use
Many parents indicated that environmental factors played an important role in their ability to implement the intervention. Parents reported certain activities as a facilitator of their use of the intervention, especially when the activity is engaging for the child. For example, after modeling language around her child’s play a mother noted, “When playing with something of interest, he will use new words on his own.” In contrast, parents also described activities that were disliked by the child or discussed RRBs as a barrier to their use of the intervention. One mother described trying to imitate her child’s play, saying that, “He would become frustrated when it involved a toy that he usually lines up like blocks or his cars.”
Parents in both groups mentioned this theme, though it was more prevalent among parents in the LTSE group (theme occurrence: HTSE = 29, LTSE = 52). Parents in the LTSE group were more likely to describe environmental factors as both facilitators (subtheme count: HTSE = 14, LTSE = 28) and barriers (subtheme count: HTSE = 23, LTSE = 38) to intervention implementation. External barriers such as illness, time constraints, and change in routine were also mentioned as specific environmental factors that interfered with intervention implementation. One parent expressed, “This week was challenging for us only because she was sick, and we have not been able to really work this week’s lesson as I would like to have.” Within this theme, parents also noted that holiday and summer breaks affected their ability to implement the intervention with their child.
The importance of the child’s response to the intervention
All parents in this study reported that their child’s response to the intervention strategies influenced their implementation. Almost all parents reported that their child showed engagement in social interactions with them when implementing the intervention. One father noted engagement while following his daughter’s lead: “Yesterday she was having fun with having me drop little figures down our stairs. She would tell me which figure to drop and we would say ‘bye-bye’ to each one before we dropped them.” Almost every parent also reported that their child had fun in social interactions with them when they were using the intervention. Another father mentioned that his daughter, “smiles, laughs, and continues to try to do things to see if I’ll imitate them” while using the techniques with her.
Parents also mentioned that their child did not engage with them at times, which made it difficult to implement the intervention. For example, a parent noted that her son, “doesn’t seem to notice when I follow his lead. He doesn’t react to it.” Parents also mentioned instances of their child ignoring them or walking away. Likewise, parents wrote about their child responding with frustration to the techniques. A mother reported, “When I was trying to follow his lead with his toys, he got irritated and pushed me out.” Within this theme, parents also mentioned their child crying, screaming, and feeling anxiety in response to techniques. Parents from both groups mentioned this theme at a similar rate (theme occurrence: HTSE = 231, LTSE = 220), with equal reports of positive responses (subtheme count: 182) and negative responses (subtheme counts: HTSE = 117, LTSE = 118) from both groups. See Table 3 for a joint display for factors relating to therapeutic self-efficacy.
Joint display for factors relating to parent self-efficacy.

ISE: Intervention Self-Efficacy from the adapted Parent Adherence to Treatment and Competence score; PSOC: Parenting Sense of Competence; VIQ: Verbal Intelligence Quotient; NVIQ: Nonverbal Intelligence Quotient; VABS ABC: Vineland Adaptive Behavior Scales Adaptive Behavior Composite Score.
Theme count is the number of times that the theme or subtheme was mentioned by participants. The percentages are the percent of participants in the High Therapeutic Self-Efficacy (HTSE) and Low Therapeutic Self-Efficacy (LTSE) groups who mentioned the theme or subtheme.
p < 0.05.
Discussion
This study sought to identify factors that relate to parents’ therapeutic self-efficacy when implementing a telehealth-based parent-mediated intervention. Our quantitative analysis suggested that parents’ feelings of global PSE at intake were positively related to their sense of therapeutic self-efficacy throughout the program, suggesting that parents who have higher levels of global PSE to begin with are more likely to feel efficacious when learning and using a parent-mediated intervention. This finding suggests that therapists should consider a parent’s overall PSE before beginning a parent-mediated intervention. For example, if a parent has low PSE, the therapist may wish to utilize a brief PSE intervention, such as Karp and Kuo’s (2015) program of six, 30-min sessions, prior to starting a parent-mediated intervention program or the therapist may integrate encouragement and support for PSE into the already existing intervention program.
Interestingly, parent therapeutic self-efficacy was not related to other parent or child demographic variables. This finding is surprising, given previous work indicating a relationship between PSE and child functioning. This could be due to the fact that most of the literature has found a relationship between PSE and child behavior problems specifically (Hastings & Brown, 2002; Hastings & Symes, 2002), which we did not measure in this study. Another explanation is that therapeutic self-efficacy is less related to child functioning than PSE. However, it is also possible that parents’ perception of their child’s functioning is more influential than their child’s actual abilities. This explanation is more in line with our qualitative analyses, which found that parents with lower therapeutic self-efficacy were more likely to view their child’s (lack of) skills as negatively impacting their ability to use the intervention. Future research should examine this possibility using a larger sample size and objective measures.
Therapeutic self-efficacy was also not related to group assignment (self-directed or therapist-assisted). This finding was unexpected given previous research indicating that parents’ therapeutic self-efficacy in running their child’s ABA program was positively related to their perceptions that they received the support they needed from a professional (Hastings & Symes, 2002). At the same time, in a previous investigation of the impact of this program on parent outcomes, we found similar improvements in parenting self-efficacy for parents in the therapist-assisted and self-directed groups, suggesting that parents experience a greater sense of competence when receiving instruction in strategies to help their child, regardless of instructional format (Ingersoll et al., 2016). It may also be possible that other factors interact with group assignment (e.g. global PSE, child functioning) in predicting therapeutic self-efficacy; however, our current sample size precludes this analysis. Future studies that look for moderation would be informative.
Another aim of this mixed methods study was to identify themes that were related to parents’ therapeutic self-efficacy. Across qualitative responses, it became clear that parents’ perception of the fit between the intervention and their child’s skills, their own interaction style, as well as environmental factors, and their child’s response influenced parents’ experience with implementing the intervention.
Although parents in both HTSE and LTSE groups identified all of these themes, parents with LTSE were more likely to mention child fit and parent fit with the intervention as barriers to intervention implementation. For example, parents in the LTSE group were more likely to describe their child’s skills as a barrier and were more likely to describe their own difficulty with implementing the strategies. In contrast, parents with higher therapeutic self-efficacy were more likely to mention these factors as facilitators of intervention implementation, such as describing their child’s skills as a facilitator and describing intervention strategies as fun and natural.
Parents with LTSE were more likely to mention the influence of environmental factors and their child’s response to the intervention. Parents in the LTSE group were more likely than the HTSE group to mention these themes as both facilitators and barriers. These findings suggest that, particularly for parents with lower therapeutic self-efficacy, problem-solving around environmental challenges may be particularly important.
These findings extend the current literature on self-efficacy in parent-mediated interventions by adding the qualitative component to gain a more comprehensive idea of the parents’ experiences. The findings of this study also add to the current literature by emphasizing the importance of monitoring parental therapeutic self-efficacy with a parent-mediated intervention. These findings suggest that coaches may want to specifically ask about the child’s skills, parent’s interaction style, environmental challenges, and child’s response as they support parents in learning NDBIs, such as Project ImPACT.
Limitations
Multiple limitations were present in this study. Parents in this study had generally high self-efficacy, both globally and within the intervention. This could be because parents with higher global self-efficacy seek out opportunities to be involved in parent-mediated intervention research. This study also primarily consisted of White, non-Hispanic, highly-educated female parents. Because of the lack of diversity within this sample, our findings may not be generalizable to the intervention implementation experience of all caregivers of children with ASD. Future studies should aim to recruit samples of caregivers from different educational and racial backgrounds.
Another limitation of this study was that the qualitative data used for thematic analysis were written short answer responses from an online program. Because of this, responses differed greatly in length and density. Parents were not required to complete the responses for every lesson, resulting in a range of 5 to 10 complete responses per participant across the sample. Future research should consider using additional qualitative data collection methods, such as interviews or focus groups, which would allow more specific interview questions, elaboration, and back and forth conversations, as qualitative data for thematic analysis.
Future work should explore the relationship between these identified themes and self-efficacy in other NDBIs as well as parent-mediated interventions that are not specific to ASD. A wider variety of measures should also be considered when examining factors relating to therapeutic self-efficacy, such as locus of control, parent depression, parental stress, and child internalizing and externalizing behaviors. Finally, future studies should examine the relationship between parental therapeutic self-efficacy and intervention fidelity, as well as the relationship between parental therapeutic self-efficacy and the maintenance of intervention implementation over time.
Conclusion
Global PSE plays an important role in parental therapeutic self-efficacy in parent-mediated interventions. Coaches should specifically ask about the child’s skills, parent’s interaction style, environmental challenges, and child’s response as they support parents in learning NDBIs. Implications call for supports for helping parents feel confident in their use of the intervention and maintain their efforts over time.
Footnotes
Acknowledgements
We would like to thank all of the families who participated in this study. We would also like to thank Grace MacDonald for all of her hard work in helping to create the codebook and consensus-code the data for this project. Finally, thank you to Karís Casagrande and Kyle Frost for providing advice on data analysis and theme development.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.I. receives royalties from the sale of the manual that was adapted for use in the online tutorial. Royalties are donated to the research. There are no conflicts of interest to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Congressionally Directed Medical Research Programs (W81XWH-10-1-0586), and the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) (R40MC27704).