
Abstract
The assessment instruments for diagnosing children with autism spectrum disorder have been developed mostly in affluent, English-speaking countries. Among the most popular has been the Autism Diagnostic Interview–Revised. This article reports its use in Iran with the dual aims of confirming the factor structure of the revised Autism Diagnostic Interview when used to assess Iranian children for autism spectrum disorder and to identify the algorithms that best distinguish children with autism spectrum disorder from those who are developing typically and from those with intellectual disability. Study 1 contrasted the Autism Diagnostic Interview–Revised ratings given to 420 children with autism spectrum disorder from those of 110 typically developing children. In Study 2, the Autism Diagnostic Interview–Revised ratings of 720 children with autism spectrum disorder were compared with those of 172 children with intellectual disability, and from those with intellectual disability. Exploratory factor analyses identified one main factor that merged the social interaction and communication items of Autism Diagnostic Interview–Revised, but replicated the repetitive behaviour and verbal factors. Receiver operating characteristic analyses identified suitable cut-off points on the revised factor scores. Also, the age at which symptoms became apparent increased the sensitivity of the algorithm in distinguishing children with autism spectrum disorder from those with intellectual disability. These findings are in line with the Diagnostic and Statistical Manual of Mental Disorders (5th ed.), recommendations and suggest a commonality in autism spectrum disorder presentations across different nations. The methodology used in this research could guide similar adaptations of assessment instruments for use in other cultures.
Lay abstract
The diagnosis of autism spectrum disorder is a challenging task. Most of the current assessment scales have been developed in the West. The present study examines the applicability of one of the most used scales (the Autism Diagnostic Interview–Revised) in a Middle-Eastern culture. Two studies were undertaken. In the first, the Autism Diagnostic Interview–Revised ratings given to 420 children with autism spectrum disorder, aged 4–11 years, and 110 typically developing children were contrasted. In Study 2, the Autism Diagnostic Interview–Revised ratings of 720 children with autism spectrum disorder were compared with those of 172 children with intellectual disabilities to find out whether the Autism Diagnostic Interview–Revised scale would discriminate between these two types of developmental disabilities. The studies confirmed the acceptability of the scale to Iranian parents and assessors. However, the summary scores used to determine whether a child was likely to have autism spectrum disorder were recalculated on the two domains of social communication and repetitive behaviours, which were identified in the statistical analyses that are recommended for the evaluation of assessment scales. Thus the translated scale with the modified domain scoring proved very suitable for identifying Iranian children with autism spectrum disorder. Having a common tool such as Autism Diagnostic Interview–Revised will strengthen the opportunities to undertake cross-cultural research into the impact of autism spectrum disorder on the child and families.
Introduction
Across the world, increasing numbers of children are being identified as having an autism spectrum disorder (ASD; Matson & Kozlowski, 2011). In part, this reflects the increased awareness and knowledge about this condition which the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) currently captures (Kulage et al., 2019). However, there remains a marked variation in the prevalence rates of children identified with ASD across the globe with higher numbers reported in more affluent, English-speaking countries (Elsabbagh et al., 2012). The lack of suitable assessment tools in other languages as well as a shortage of suitably trained personnel in other countries may contribute to this variation (Samadi & McConkey, 2011). Nevertheless, a diagnosis is important for children and families, not least as it can enable them to obtain an understanding of their children’s difficulties and confirms their entitlement to access additional supports and services to manage and ameliorate the condition (Brett et al., 2016).
A range of assessment and diagnostic tools for ASD have been developed, foremost of which has been the Autism Diagnostic Interview–Revised (ADI-R; Le Couteur et al., 2003; Lord et al., 1994). As the name suggests, ADI-R consists of a structured interview undertaken with family caregivers. The items were drawn from the International Classification of Diseases–10th Revision (ICD-10; World Health Organization, 1992) and the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 2000) criteria for autism and are based on the triad of impairments originally proposed by Wing and Gould (1979). Responses to the items were grouped originally into three domains, reflective of the core characteristics of ASD: social interaction, communication and repetitive behaviours. Algorithms were developed to profile the pattern of scores on each domain. Subsequent factor analysis based on the scores on the items used in algorithms assigned to 226 children with pervasive developmental disorders, initially confirmed these three domains (Lecavalier et al., 2006) with one minor adjustment. However, a more extensive study by Snow et al. (2009), using data on over 1800 individuals recorded on a publicly available database – AGRE – identified a two-factor solution as a better fit: namely, social and communication behaviours as the main factor with restricted and repetitive behaviours as a second factor. Frazier et al. (2008) came to a similar conclusion with a sample of over 1100 youth and adults, but based on the 12 subscale algorithm scores rather than the ratings given to individual items across all subscales. Nevertheless, both studies concluded that a revision was needed of the algorithms used in ADI-R to identify children with ASD so as to better reflect the relationships between the items making up the identified factors.
Although ADI-R has been used internationally, there appear to have been no studies outside of the United States and Europe that have examined its factor structure and the associated algorithms for identifying the likelihood of ASD in children. This is unfortunate as tools developed in one culture may not transfer readily to others (van Widenfelt et al., 2005). Although the relationship between cultural influences and ASD has received little attention (Matson & Kozlowski, 2011), some recent studies have noted cultural differences in how ASD symptoms are perceived both in terms of individual items and groupings of items (Freeth et al., 2013). Nevertheless, the requirement for suitable diagnostic tools is just as urgent in non-Western countries so that families gain a better understanding of their child’s difficulties and governments are alerted to the need to adapt or extend education and other services to meet the particular needs of these children and their families (Lord & Bishop, 2010).
Iran has a population of 82.8 million, around one-quarter of whom are aged 0–14 years. It is classed by the World Bank as an upper-middle-income country-based Gross National Product. In Iran, there is a national screening programme for all children who are 5 years old and want to be registered in the first grade of elementary school (Iranian Special Educational Organization (ISEO), 2020). Those with developmental difficulties, including children with ASD, are referred for further diagnosis or assessment to determine their appropriate placement. These assessments are undertaken by trained professionals, mostly psychologists, employed in the Iranian Special Educational Organization (ISEO). Based on these assessments, the prevalence rate for 5-year-old pupils assessed as ASD was 6.28 per 10,000 in the years 2006 to 2009 (Samadi et al., 2012). In addition, a small number of children of preschool age with ASD may be assessed within the social welfare system and placed in special day centres for those with higher support needs rather than in schools or as a preparation for the national screening for school entry.
An Iranian translation of the ADI-R was chosen as the primary means of assessing children suspected for having ASD (Sasanfar & Toloie, 2006). The present article reports a statistical analysis of the ratings given to the Iranian translation of ADI-R items. In addition, two comparative studies were undertaken in which the ADI-R was administered to children who were typically developing and to children who had been assessed as having an intellectual disability (ID). This article describes the findings from these two studies and addresses the following questions:
What is the factor structure of the ADI-R when used to assess Iranian children for ASD?
What algorithms best distinguish children with ASD from those who are developing typically and from those with ID?
Although the findings are of particular relevance to the future use of ADI-R within Iran, the findings will also add to a better understanding of the common features of ASD across different cultures as well as providing an example of how assessment tools developed in one culture can be evaluated for their use in other cultures.
Method
ADI-R: Farsi version
ADI-R provides a semi-structured interview for use with a child’s caregivers and takes around 2 h to complete. It consists of 93 questions which are grouped into early child development, communication, social development and play, interests and behaviours. The items and groupings closely follow the criteria for autism outlined in DSM-IV and ICD-10. The interviewer uses the caregiver’s descriptions of the child to code each item on a scale from 0 to 3, with ‘0’ indicative of no definite behaviour of the type identified, ‘1’ for behaviour of the type specified probably present but defining criteria not fully met and ‘2’ for definite abnormal behaviour of the type described in the definition and coding. A score of ‘3’ is used to indicate extreme severity, although in arriving at summary scores these are recoded as ‘2’.
The criteria for a diagnosis of ASD is based on an algorithm using cut-offs on the summated scores for items grouped into the three domains of social interaction, communication and repetitive behaviour, provided that the onset of the disorder is evident by 36 months of age.
With permission of the publishers, the ADI-R guidebook with behaviour coding instructions and examples, the interview booklets and diagnostic algorithms were translated into Farsi by two senior staff from the testing and evaluation department of the Iranian Special Education Organization (ISEO) who were fluent English speakers (Sasanfar & Toloie, 2006). An independent fluent speaker of English and Farsi then made a back translation from Farsi to English. Any discrepancies were moderated across the three translators. As a further safeguard, the first author undertook a confirmatory review of the Farsi translation following his doctoral research in the United Kingdom and training in the use of ADI-R.
Due to international sanctions imposed on Iran, the usual accredited training opportunities on ADI-R available in the United Kingdom, for example, could not be accessed. However, two senior staff in ISEO had been trained in the United States in the use of ADI-R, and this training was replicated in Iran. The ADI-R training pack (including a DVD training program) was translated and training was provided by ISEO staff in the Central Bureau to the assessors based in the provinces. This consisted of pre-training information in the form of booklets on the signs and symptoms of ASD, and other developmental disorders on which assessors were then tested. Three days of training followed covering ADI-R questions, coding system, interpretations and reporting followed by a fourth day in which each assessor was video-recorded, undertaking an assessment using ADI-R. The video and the completed assessment forms were submitted to the trainers and feedback was provided along with the decision to confirm their status as an ADI-R assessor. In all, a total of 30 assessors were trained, 18 of whom came from Tehran province (10 for Tehran city and 8 for other cities in the Tehran province).
In order to maximise the fidelity of assessments across the assessors, each assessor had to submit video tapes annually of three interviews they had conducted over the course of the year, to assure the reliabilities of the assessments as per ADI-R procedures. Detailed feedback was also given to the assessors by their nominated supervisors. In addition, annual in-service training courses were organised for the test assessors to ensure ongoing fidelity with the assessment procedures and scoring. The supervision and training of assessors was overseen by the first and third authors.
The translated ADI-R was first evaluated on a sample of 211 children (101 with ASD, 101 typically developing and 9 with intellectual disabilities) aged 4–14 years. No major difficulties were encountered, although some minor modifications and clarifications were made to certain items based on parental feedback and the assessors’ experiences.
To assess the interrater level of agreement between different assessors, 30 children with ASD were selected randomly and reevaluated by a second assessor who was unaware of the previous ADI-R ratings and scores. This is done by the first author. In addition, test–retest reliability was determined with 28 children who were reassessed after a 3-week interval. Pearson’s product moments correlations between the four domain scores on the two ADI-R assessments were calculated. The interrater correlations ranged from r = 0.89 to 0.95 and for test–retest the range was r = 0.94 to 0.99. All correlations were statistically significant (p < 0.001). These were comparable to the test–retest reliabilities of ADI-R reported by Cicchetti et al. (2008), which ranged from r = 0.93 to 0.97. Moreover, there were no significant differences in the mean scores on any of the four domains on the two administrations.
Procedure for administering ADI-R
ADI-R was administered with children who were suspected of having ASD based on a screening using the Farsi translation of the Social Communication Questionnaire (Rutter et al., 2003; Sasanfar & Ghadami, 2006). Children who screened positive were referred for further assessment by ISEO assessors. In addition, referrals could also come for children up to 11 years of age already attending school when teachers suspected that pupil might have ASD.
The children and their parents were invited to attend an assessment centre held within the participating provinces. Details were provided about the procedures that would take place and parental consent was obtained. The ADI-R interview was conducted in a private room in the centre and mostly with the child present. However, the assessor did not undertake any formal tests or observations with the child. These same procedures were followed when ADI-R was used with typically developing children and those with ID.
The assessor’s scoring of the ADI-R was checked with a supervisor. For children assessed as having ASD, the parents were informed of the outcomes and school placement options were outlined and decided upon. These included attendance in a mainstream school, placement in a special unit or school for children with ASD or referral to day centre provided by the Iranian Social Welfare Organisation for children considered unsuitable for education.
Recruitment
The study was based in Tehran province, which is the most populous in Iran with a population of over 13 million at the last census in 2016. The ADI-R details on the children assessed as ASD in Tehran city and Tehran province were taken from the case files sent by assessors to the ISEO Central Testing and Evaluation Department. Their proximity to the central bureau of ISEO’s evaluation and testing department meant that closer supervision of their assessments was possible. All of the children received ongoing support from ISEO in special units or mainstream schools based on the diagnosis. These were all the complete files that were available at the time of the comparative study with the other two groups of children. The 18 assessors in Tehran province also came under the direct supervision of the first author who had trained as a reliable ADI-R administrator while studying in the United Kingdom.
The children who were typically developing were recruited through the Ministry of Education from kindergarten, preschools and schools in Tehran and whose parents agreed to participate in the study. All the children were screened using either M-CHAT or SCQ, based on their age and all scored below the cut-off score for possible ASD.
Children with ID were recruited from clinics and special schools under the supervision of ISEO. All had received their diagnosis based on the Wechsler Intelligence Scale for Children-Fourth Edition (WISC-IV) (Wechsler, 2003) from ISEO or based on clinical assessments by other professionals from other agencies such as the Iranian Social Welfare Organisation. Parents volunteered to participate although it was made clear that participation would not affect their existing services.
Ethics
No formal ethical approval for the study was sought as it involved the analysis of case file data which was anonymised for statistical analysis and no individual would be identified in the study. However, permission was obtained from ISEO to undertake the studies. Informed consent was obtained from parents and assurances were given to them about the confidentiality of the information given.
Data analysis
The ratings given to the individual items on the ADI-R for each child were entered into an SPSS Spreadsheet along with demographic information. Following the procedures adopted by Snow et al., 2009), the items that contributed to the algorithms were recoded into 0,1,2 (3 coded as 2). In order to maximise the number of cases, the scores of ASD children designated as non-verbal (Item 30) were coded as 2 (indicative of impairment) on all the verbal items (numbers 33–39).
An exploratory factor analysis was undertaken with an oblimin rotation with Kaiser normalisation. This rotation allows for the factors to be correlated.
Summary scores were computed by totalling the ratings given to each item that had a factor loading greater than or close to 0.400. The internal reliability of the factor scores was assessed using Cronbach’s alpha and comparisons were made between the ASD and the two comparator groups using independent t-tests.
Receiver operating characteristic (ROC) curves were used to determine suitable cut-off points on each factor scale to distinguish children with and without ASD.
Sensitivity and specificity analyses were made using MedCalc Statistical Software (https://www.medcalc.org/calc/diagnostic_test.php).
Study 1: Comparisons between ASD children and typically developing peers
Participants
ADI-R assessments were completed on 460 children with a diagnosis of ASD and 110 children who were typically developing. Table 1 summarises the child and family characteristics of the two groups.
Characteristics of the children and parents in Study 1.
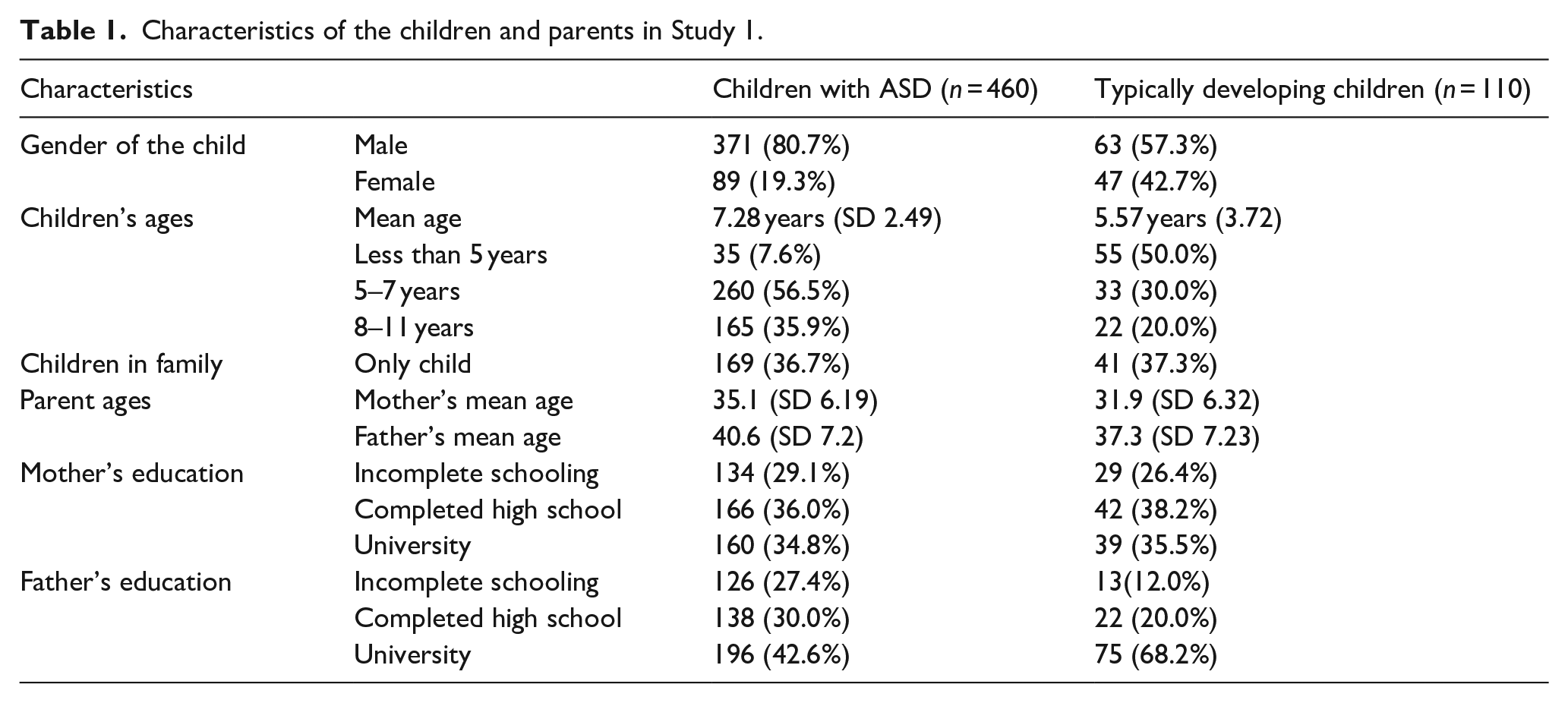
The ADI-R interviews were mostly conducted with the child’s mother. For children with ASD, the informants were mothers (n = 371, 72.0%), fathers (n = 77, 16.7%) and both parents (n = 48, 10.4%). For typically developing children, the informants were mothers (n = 62, 56.4%), fathers (n = 28, 25.5%) and both parents (n = 20, 18.2%).
Exploratory factor analysis
Three factors were identified with an eigenvalue greater than 1 and together accounted for 66% of the variance, but with the first factor accounting for 54% of the variance (eigenvalue = 20.48), the second factor for 8% (eigenvalue = 2.96) and a third factor for 4% of the variance (eigenvalue = 1.57). Table 2 summarises the item loading as identified in the pattern matrix from the oblimin rotation.
Item loading on the three factors in analysis of data from children with and without ASD (n = 570).

ADI-R: Autism Diagnostic Interview–Revised.
The items on Factor 1 were drawn largely from the social interaction and communication domains of the ADI-R. Factor 2 consisted of the verbal items and Factor 3 the Repetitive behaviour items.
Cronbach’s alpha internal reliability
A summary score was calculated for the items within each factor. A high score indicated greater difficulties. A check was made of the internal reliability of each factor using Cronbach’s alpha. For the social-communication factor it was α = 0.977, for the verbal items it was α = 0.964 and for the behaviour items, α = 0.757. The latter may reflect the idiosyncratic nature of the repetitive behaviours shown by children with ASD.
Intergroup comparisons
The difference in scores between children assessed as ASD and those with typical development were compared on the three factors as shown in Table 3. All were significantly different with t-tests (equal variances not assumed), p < 0.001. However, children identified with ASD had mostly greater SDs on the verbal and behaviour items.
Mean and SD of scores on the three factors for children with and without ASD.

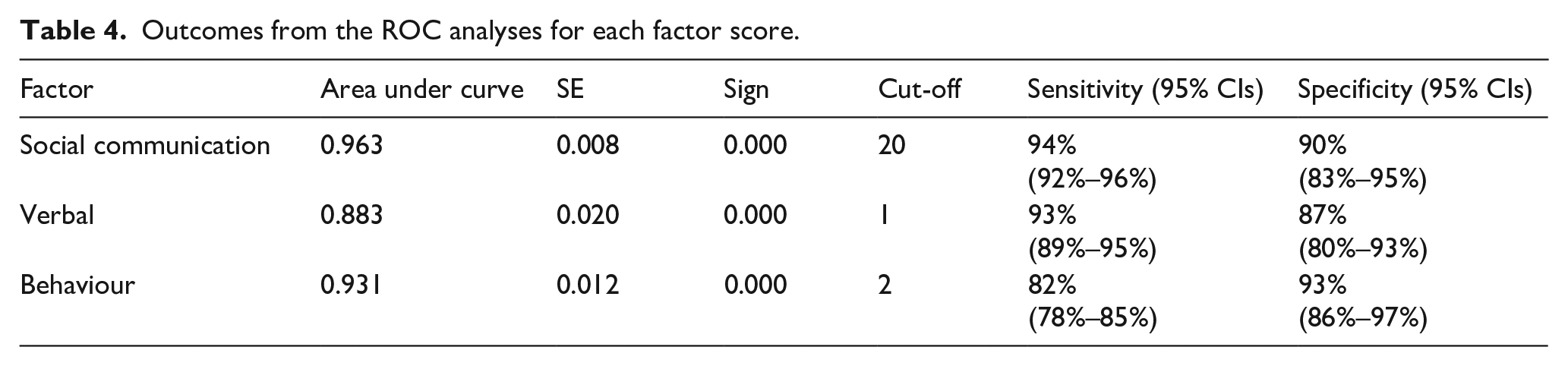
ROC curve analysis
Table 4 summarises the analyses that were undertaken to determine suitable cut-off points on each factor scale to distinguish children with ASD from those developing typically. Sensitivity and specificity were the highest for the social-communication factor with sensitivity being the weakest for the behaviour factor.
Outcomes from the ROC analyses for each factor score.
Study 2: Comparison children with ASD and ID
Participants
ADI-R assessments were completed on 712 children with a diagnosis of ASD and 172 children who were diagnosed as having an ID. Table 5 summarises the child and family characteristics of the two groups.
Characteristics of the children and parents in Study 2.
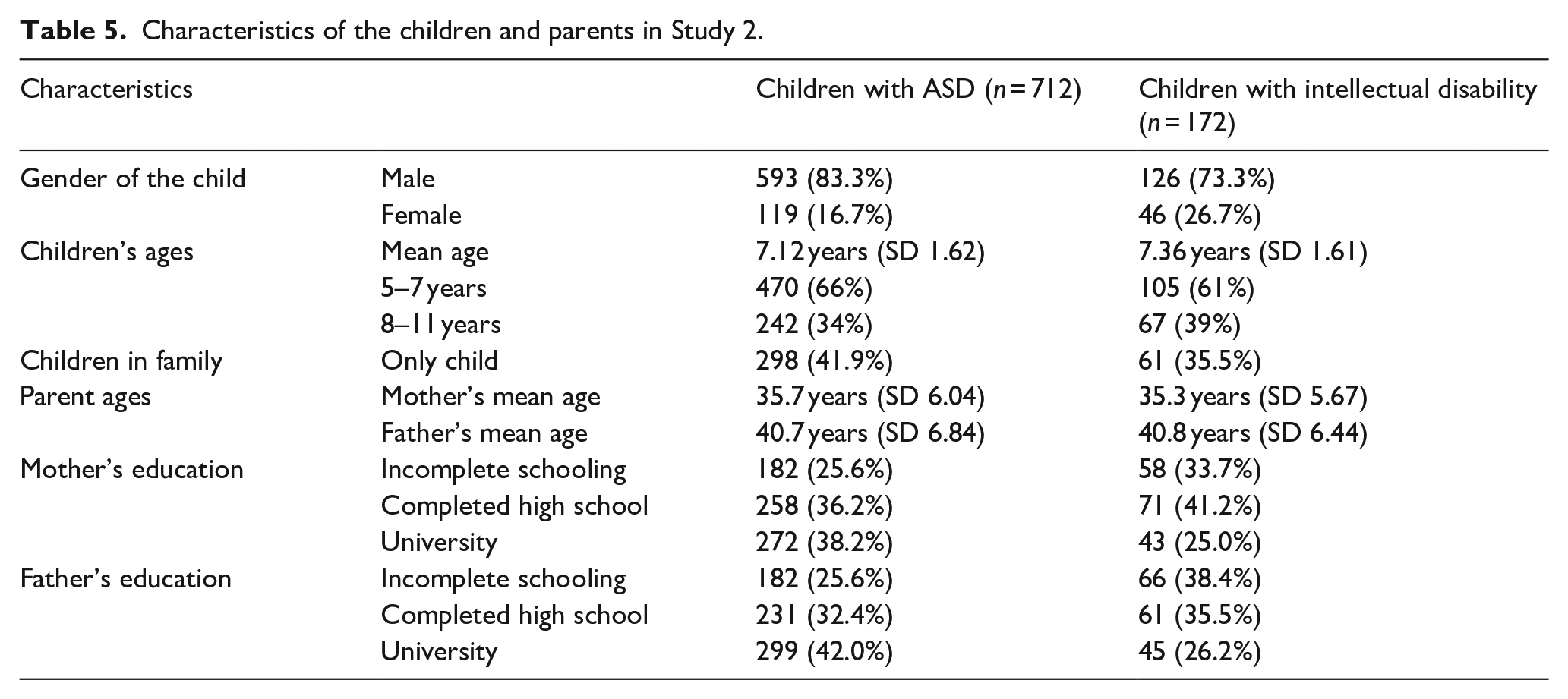
The ADI-R interviews were mostly conducted with the child’s mother. For children with ASD, the informants were mothers (n = 559, 78.5%), fathers (n = 67, 9.4%) and both parents (n = 83, 11.7%). For children with ID, the informants were mothers (n = 150, 87.2%), fathers (n = 7, 4.1%) and both parents (n = 14, 8.1%).
Exploratory factor analysis
As in Study 1, an exploratory factor analysis was undertaken using an oblimin rotation with Kaiser normalisation. Four factors were identified, which together accounted for 60% of the variance. The first factor accounted for 42% of the variance (eigenvalue = 15.63), the second factor for 10% (eigenvalue = 3.80), a third factor for 4% of the variance (eigenvalue = 1.63) and a fourth factor for 3% of the variance (eigenvalue = 1.21). Table 6 presents the item loadings on each factor.
Factor loadings for items in analysis comparing children with ID and ASD (n = 884).
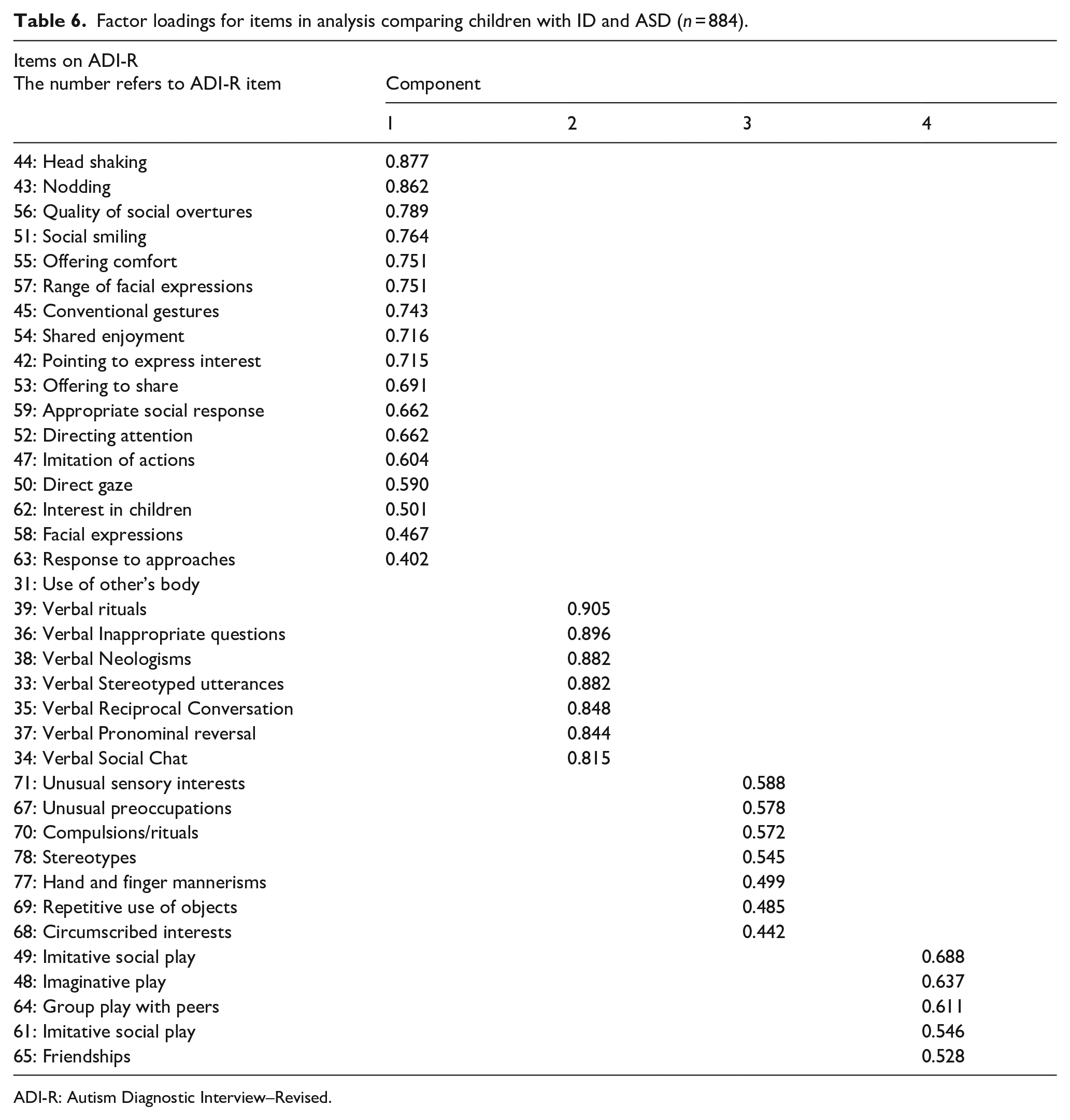
ADI-R: Autism Diagnostic Interview–Revised.
As a comparison between Tables 2 and 6 illustrates, the item groupings broadly replicate the factor structure identified in Study 1 – albeit with different loadings on the factors – but in this analysis the items relating to play which formed part of Factor 1 in Study 1 became a separate fourth factor in this analysis.
However, when the factor analysis was repeated only for ASD children, the first three factors were replicated: Social Communication, Verbal and Behaviour, although the amount of variance was reduced to 47% overall and to 30% on Factor 1. The other two factors accounted for similar amount of variance.
Cronbach’s alpha internal reliability
A summary score was calculated for the items within each factor with a high score indicative of greater difficulties. A check was then made of the internal reliability of each factor using Cronbach’s alpha. For the social-communication factor α = 0.960, for the verbal items α = 0.831, for the behaviour items α = 0.698 and for the play factor α = 0.842.
Intergroup comparisons
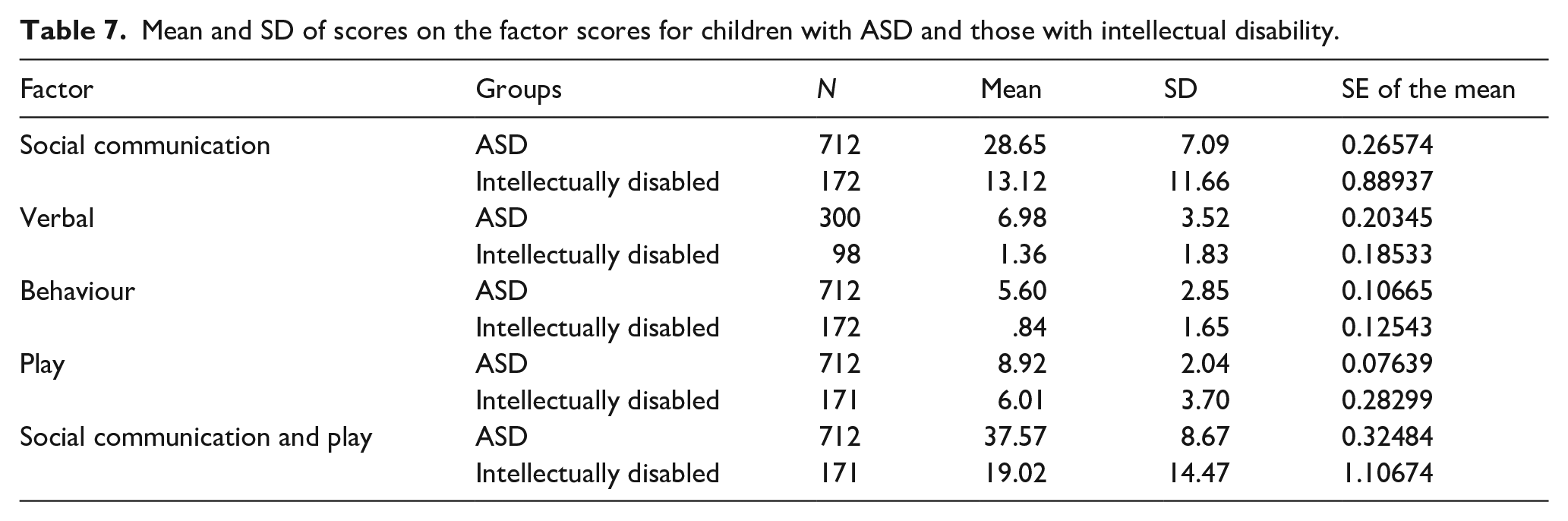
The difference in scores between children assessed as ASD and those with ID were compared on the four factors as shown in Table 7. In addition, a new score was created that combined the social-communication and play items as found in Study 1, also reflecting the three factors found with children with ASD in Study 2. All the differences were significantly different with t-tests (equal variances not assumed) p < 0.001.
Mean and SD of scores on the factor scores for children with ASD and those with intellectual disability.
ROC curve analysis
Table 8 summarises the analyses that were undertaken to determine suitable cut-offs points on each factor scale to distinguish children with ASD and ID.
Outcomes from the ROC analyses for each factor score.
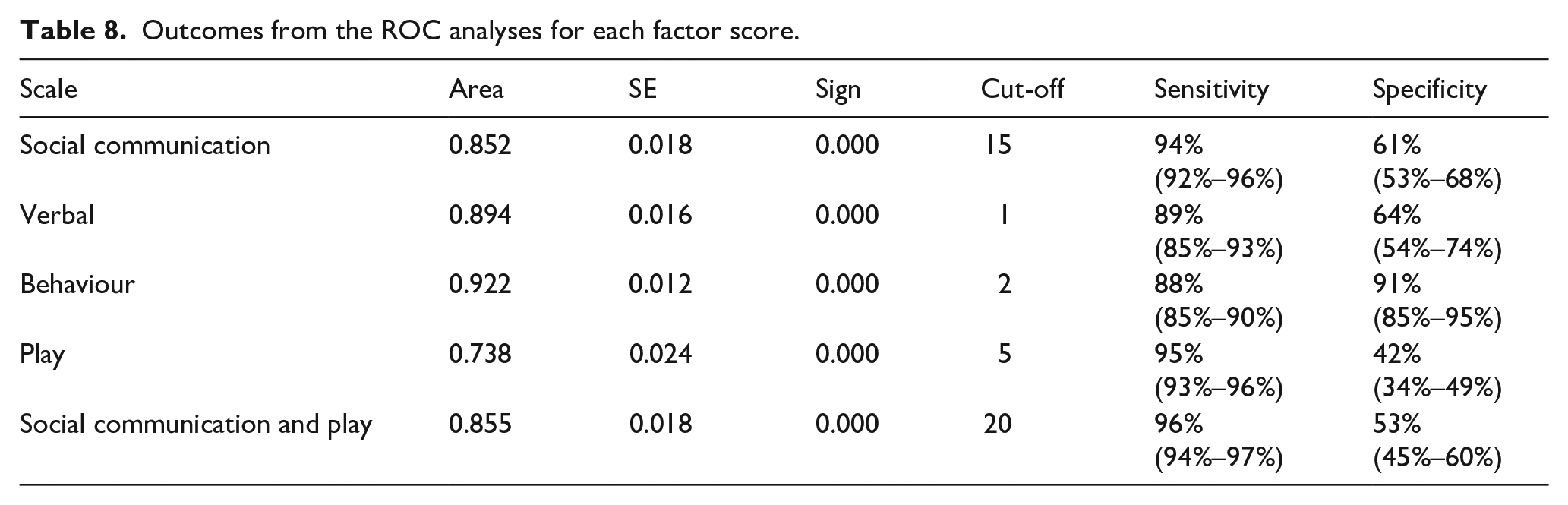
On all the items, sensitivity scores were higher than specificity which indicates that although the scores were able to correctly identify most of the children with ASD, the specificity rates were much lower with the exception of the behaviour scale. Thus children with ID might also be considered to have ASD.
However an additional discriminating variable between children with ASD from those with ID was the age of onset of the symptoms as determined by the assessor as part of the ADI-R procedures. A further approach to determining suitable cut-off algorithms is to examine whether a combination of the scales and age of onset might produce better specificity. To that end, a Discriminant analysis identified that the cut-off scores for the behaviour, social-communication and the assessor assessed age of onset of symptoms (before or after 12 months) were the best discriminants of the two groupings with verbal scores making little additional contribution (Wilks’ lambda = 0.411, χ2 = 782.3, p < 0.001). The loadings on the structure matrix from the analysis (similar to item loadings in factor analysis) were as follows: behaviour 0.770, social communication and play (0.557) and early onset of symptoms (0.506). The verbal loading was 0.368.
A grouping variable was created by combining the social communication and play (SCP) scores, the behaviour scores and age of onset of symptoms. This resulted in five main groupings as shown in Table 9 with the number of children with ASD and ID in each of them.
Number of children with ASD and intellectual disability in the combined groupings.
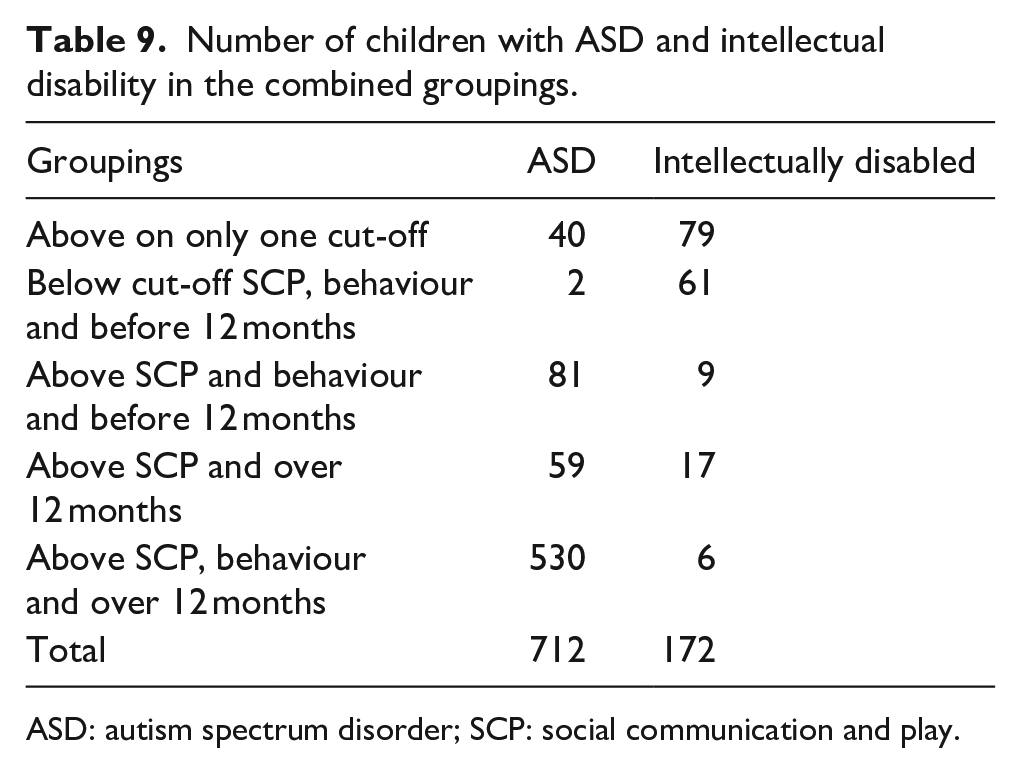
ASD: autism spectrum disorder; SCP: social communication and play.
When children who scored above and below on all three cut-offs were considered (n = 599, 84% of all children assessed), the sensitivity was 99.6% (CI = 98.7%–100%) and specificity was 91% (CI = 82%–97%).
However sizable numbers of children score above the cut-offs on two of the three items. With them, a pattern is discernible across the children with ASD in that compared with those with ID, they scored above the cut-offs for SCP and behaviour with the symptoms apparent after 12 months of age. A further group scored above the cut-off for SCP but not for behaviour with symptoms appearing after 12 months. When these two groups are added to those who scored above all three cut-offs, 670 children could be considered to have ASD: 94% of those assessed.
By contrast, people with ID had scores above the cut-off mostly on only one factor or below on all three, suggesting that 81% are unlikely to have ASD, but this remains a possibility with 19% of them as they scored above the cut-offs on two of the three factors.
Finally, the distinction between children who were judged to be using functional verbal communication can further discriminate among those with ASD. Of the 670 children with ASD who scored above the cut-offs on two or three of the factors, 282 were verbal and 388 non-verbal. For those with ID, 11 were verbal and 21 were non-verbal. Thus the cut-offs described here can be used to discriminate among children with ASD as follows:
282 verbal children with ASD – 40% of total;
388 non-verbal children with ASD – 54% of total;
42 children with a varied profile who are less likely to have ASD – 6% of total;
11 verbal children with ID as possibly having ASD – 6% of the total sample;
21 non-verbal children with ID as possibly having ASD – 12% of the total sample;
141 children with ID not likely to have ASD – 82% of the total.
Discussion
This study had two main aims, both of which were fulfilled. The same factor structure was largely replicated in the two sets of data analysis when either typically developing children or those with ID were included alongside children with ASD. Moreover, the structure partially confirms the two-factor structure reported in previous studies which found a social-communication factor and behaviour factor underlying the item ratings (Snow et al., 2009). Furthermore, this aligns with the DSM-5 criteria that modified the former triad of impairment into a dyad by merging the social interaction and communication domains into one (Mandy et al., 2012)
In addition, however, verbal items within the communication section of ADI-R formed a distinct factor in our analyses, whereas ADI-R had originally proposed that all communication items be considered together. However, this factor contributed little to the overall variance. Also, the play items in ADI-R formed a separate factor when children with ID were included in the analyses. Previous studies had included these play behaviours within the social-communication factor which indeed happened in Study 1 when typically developing children were included. That said, in our analyses the social-communication factor was the first and main factor, with the other identified factors accounting for much less of the variance.
These findings would suggest that revised algorithms should be adopted when ADI-R is used for diagnosing ASD with Iranian children. Our analyses has illustrated that the two factors of social communication and stereotyped behaviours are central to this. The identified cut-offs for the summary scores on these two factors had high specificity and sensitivity in identifying children with ASD from those who were typically developing.
However, the distinction between children with ASD from those with ID was not so straightforward. Although the cut-offs on these two factors still had a high degree of specificity, in that they correctly identified most of the children with ASD, the low specificity of the social communication cut-off in particular, resulted in sizable numbers of children with ID being identified as ASD. The approach we adopted was to augment the specificity by including a further indicator when a child was above the cut-off on only one of the two factors. Our analyses suggested that the age of onset of the symptoms was the most promising. When this cut-off was added, the number of children correctly identified as ASD rose to 94%. Thus, this three-factor algorithm involving above cut-off scores on social communication and on behaviours with symptoms appearing after 12 months will best identify children with ASD.
Moreover, this algorithm might also help to identify a comorbidity for ASD in children with an ID. In this study, the figure of 18% may be an underestimation compared with reports of the comorbidity of ASD and ID in the United States (Braun et al., 2015). Conversely, it is likely that a proportion of the children assessed as having ASD may also have an ID, especially those classed as non-verbal in ADI-R. This could not be ascertained in the present study, as no assessments were made of the children’s intellectual or adaptive functioning. However, Baio et al. (2018), in an extensive analysis of 8-year-olds with ASD across the United States, reported that 31% also had an ID with moderate to severe levels.
Furthermore, we have proposed that the algorithms identified from ADI-R ratings enable different profiles of children with ASD to be identified, especially as the importance of attuning interventions and supports in accord with the child’s particular profile is increasingly recognised (NICE, 2013). The proposed algorithms seem to accord with DSM-5 in that the levels of severity of symptoms are the main source for describing different diagnostic profiles rather than using the five diagnostic categories described in DSM-IV. Hence the algorithms in this study can be used to identify children with marked levels of ASD, such as those with limited verbal communication, repetitive behaviours and poor social communication, which is apparent from 12 months of age. Conversely, those whom DSM-5 identifies as Level 1 ASD (previously labelled as Asperger’s syndrome) will have verbal communication but poor social communication and some repetitive behaviour but the symptoms only became apparent after 12 months. A further study could usefully examine the correspondence between the algorithm items used in Iran and the indicators of ASD derived from DSM-5 as has been undertaken by Magaña and Vanegas (2017) for Latino children in the United States. This would also provide further evidence for the criterion validity of the ADI-R.
The study has a number of limitations. It involved children who had been referred to educational services for assessment and diagnosis. In Iran, preschool children are more likely to have been referred to health services and they may have been diverted to social welfare centres if they were considered unsuitable for education. It may be that the factor structure and cut-offs for ADI-R may need to be adjusted for younger children, although studies in the United States have identified a similar factor structure for infants aged 12–47 months (Kim et al., 2013). Intellectual assessments were not undertaken with children as part of their assessment for ASD, although this is now seen as good practice. Likewise, limited resources meant that multidisciplinary assessments could not be undertaken or observations made of the child using a tool such as Autism Diagnostic Observation Schedule (ADOS; Lord et al., 2012). This constraint applies to many less affluent countries and will likely exist for a considerable time.
In conclusion, the study suggests that ADI-R is suited to use in other cultures. The factor structure that merged suggests that the core symptoms of ASD, notably in terms of social communication and repetitive behaviours, are likely to be found across different cultures. Having a common tool such as ADI-R will strengthen the opportunities to undertake cross-cultural research into the impact of ASD on the child and families.
Footnotes
Acknowledgements
The authors are grateful to the staff in the Evaluation and Testing Department of the Iranian Special Education Organization (ISEO) for making available the data on which this paper is based.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.