
Abstract
This research explored parents’ lived experience of the autism spectrum disorder assessment process when a diagnosis was not received. Six mothers and one stepfather were interviewed and transcripts were analysed using interpretative phenomenological analysis. The identified themes: ‘My child is different’, The emotional and psychological journey and Understanding the outcome, illustrated issues encountered by parents during the assessment process and parenting a child with autistic-like characteristics but without a valid label. As a previously understudied area, clinical implications at the professional, service and policy level are discussed.
Lay abstract
Autism is diagnosed by a process of child assessment and parental interview. It has been well-documented by parents of children who received a diagnosis of autism, that the process can be lengthy and cause distress for families. Nevertheless, the outcome often compensated for the difficult assessment journey as it enables families to gain access to further information, support and intervention. However, less is known about the assessment process from parents who undertake the same process but at the end are told their child does not meet the diagnostic criteria, meaning no diagnosis is given. We interviewed six parents in North Wales, whose child did not receive a diagnostic of autism following an assessment. During the interview, parents were asked about their experience of the autism assessment process. We found that parents reflected on their experience according to three themes: (1) parents tried to navigate how they could make sense of their child being different despite not receiving a diagnosis; (2) parents referred to the assessment process as a journey, which encompassed many emotional and psychological components and (3) parents discussed what it was like to hear a non-diagnosis outcome, in terms of feeling relieved, confused and raising questions for the child’s future. These findings are important for professionals working in autism assessment services to help improve the assessment process for families, particularly when the assessment does not result in a diagnosis.
Keywords
In recent years, recognition of autism spectrum disorder (ASD) has increased. Many families seek assessment hopeful that diagnosis will explain their child’s missed milestones, unusual behaviours and provide greater understanding of their needs (Jacobs et al., 2020).
Within the intellectual disability literature, Makela et al. (2009) assessed the perceived value of diagnosis by comparing families with and without a diagnostic label. Diagnosis enabled families to access information, timely interventions and improved social support, but most importantly offered ‘validation’. Specifically, having a recognised label enabled parents to explain their child’s difficulties, reduced the impact of social disapproval regarding their child’s behaviours and empowered parents to advocate for their child in difficult social situations. Collectively, these factors were fundamental in helping families to overcome uncertainty, gain acceptance and equip parents with realistic expectations for the future (Midence & O’Neill, 1999). Some families even reported that the positives of a diagnosis outweighed the negatives (Wong et al., 2017). The perceived value of diagnosis may vary according to geographic location and/or culture (Papoudi et al., 2020). UK guidance recommends interventions based on clinical need (National Institute of Clinical Excellence [NICE], 2011), although this is not always parents experience (Griffith et al., 2013). In other countries, formal diagnosis is required to access health insurance or public-funded services (McDowell & O’Keeffe, 2012).
Despite perceived benefits associated with diagnosis, a large UK survey (n = 1295) found 49% of parents were ‘not very’ or ‘not at all’ satisfied with the assessment process (Howlin & Moore, 1997). Although published some time ago, a recent survey highlights similar findings (Crane et al., 2016). Barriers to satisfaction include professionals lacking autism awareness, absence of rapport, tendency to focus on negatives and inadequate assessment facilities (Crane et al., 2018).
Diagnostic delay is also widely linked to assessment satisfaction. ASD can be diagnosed from two years of age (Lord et al., 2006). However, Crane et al. (2016) found that parents typically waited 12 months to seek professional advice, and their concerns were dismissed or referred onwards. Average time from first contact to diagnosis was a further 3.5 years, with children typically diagnosed at 7.5 years (standard deviation (SD) = 5.0 years). Parents reported being told their child may ‘grow out of it’, ‘it’s too early’ (Zuckerman et al., 2015) or being labelled ‘neurotic’ (Legg & Tickle, 2019). Lappé et al. (2018) likened the journey of ASD diagnosis to an ‘Odyssey’ due to parents’ emotional conflict trying to reconcile advice from professionals and trusted others, in addition to service delays. Consequently, parents experienced profound uncertainty and frustration relating to missed opportunities for earlier intervention.
Interestingly, parents who saw fewer professionals and received an early diagnosis were more satisfied (Goin-Kochel et al., 2006). In their questionnaire study of 494 parents, on average, parents saw four professionals. Unsurprisingly, age at diagnosis was positively associated with the number of professionals seen (r = 0.15, p = 0.002) and negatively associated with satisfaction (r = −0.15, p = 0.001).
Assessment satisfaction has also been positively associated with collaborative parent–professional relationships where professionals acknowledged concerns, collaborated in making decisions, discussed the diagnosis and offered post-diagnostic support (Moh & Magiati, 2012). Legg and Tickle (2019) further highlight that promoting inclusive parent–professional relationships and information sharing can positively impact on numerous constructs related to assessment satisfaction and could reduce parents’ emotional distress. They also highlight the importance of tailoring relationships, as fathers often felt excluded from assessments which subsequently influenced adjustment to diagnosis.
Generally, the experiences of parents whose child receives a diagnosis are well-documented. Whilst it is clear the assessment process can be distressing, parents often reported a sense of relief following diagnosis (Avdi et al., 2000; Legg & Tickle, 2019), thus allowing them to work towards acceptance (Midence & O’Neill, 1999).
However, little is known about the experience of parents who embark on the same prolonged and stressful assessment journey, who received no or a vague diagnosis, for example, autism ‘traits’ or ‘features’. In the limited ASD research available, parents felt vague descriptions were unhelpful (Howlin & Moore, 1997). Nevertheless, findings from wider literature may be applicable. Lenhard et al. (2005) found that mothers of children with Down Syndrome reported less emotional burden than mothers whose children with learning difficulties had no specific diagnosis. Similarly, families of children with non-epileptic attack disorder reported distress due to being disbelieved (McWilliams et al., 2016). Furthermore, parents struggled to accept medically unexplained diagnoses (Moulin et al., 2015). These researchers speculated that parents’ uncertainty regarding prognosis, unresolved concerns and lack of professional recognition increased emotional burden and disrupted family functioning.
This research addresses an important missing piece in the autism literature, by exploring parents’ experience of the ASD assessment process when no diagnosis is received. Parents were asked about: (1) accessing an assessment, (2) the assessment process and (3) hearing the outcome. It is hoped the findings will enhance professionals’ understanding, inform service development and consider how best to communicate a non-diagnosis outcome.
Method
Design
Interpretative phenomenological analysis (IPA) enabled detailed exploration of participants lived experience, utilising three fundamental areas of philosophy (Smith et al., 2009): (1) phenomenology (the study of experience) focuses on how parents perceive their experience, (2) hermeneutics (the theory of understanding) allows the researcher to interpret the individuals’ experience and (3) idiography – the thorough analysis of each participant perspective, rather than concluding on probability (Smith et al., 1995).
Ethics
Approval was granted by the Health and Care Wales Research Ethics, Bangor University School of Psychology and Betsi Cadwaladr University Health Board (BCUHB).
Participants
Fifty recruitment packs were prepared aiming to recruit six to nine parents as appropriate for IPA. A small purposive sample (six mothers/one stepfather of six children) met criteria and opted in within the time frame (November 2016 to February 2017). They were recruited through a neurodevelopmental team (NDT) in North Wales according to the following criteria: aged 18+ with children (5–19 years) who underwent an ASD assessment in BCUHB between February 2016 and February 2017 but were not diagnosed and had been discharged from the assessment-only service. Parents were excluded if they could not provide consent; their child was accessing support for other neurodevelopmental difficulties; they received an alternative diagnosis, for example, Attention Deficit Hyperactivity Disorder or Speech and Language difficulties. The authors felt including parents who received alternative explanations/diagnosis would have deviated from the research question and experiences of the intended sample.
Procedure
Potential participants were identified and contacted via clinicians who assessed their child. Bilingual (Welsh/English) recruitment packs (invitation, participant information and opt-in forms) were distributed. Upon opting-in, the first author obtained informed consent and arranged interviews at the clinic. A £10 voucher was given in appreciation.
Pseudonyms were ascribed for anonymity. Table 1 displays the participant characteristics. Specific data on parental age, socioeconomic status, ethnicity and educational attainment were not recorded.
Participant characteristics.
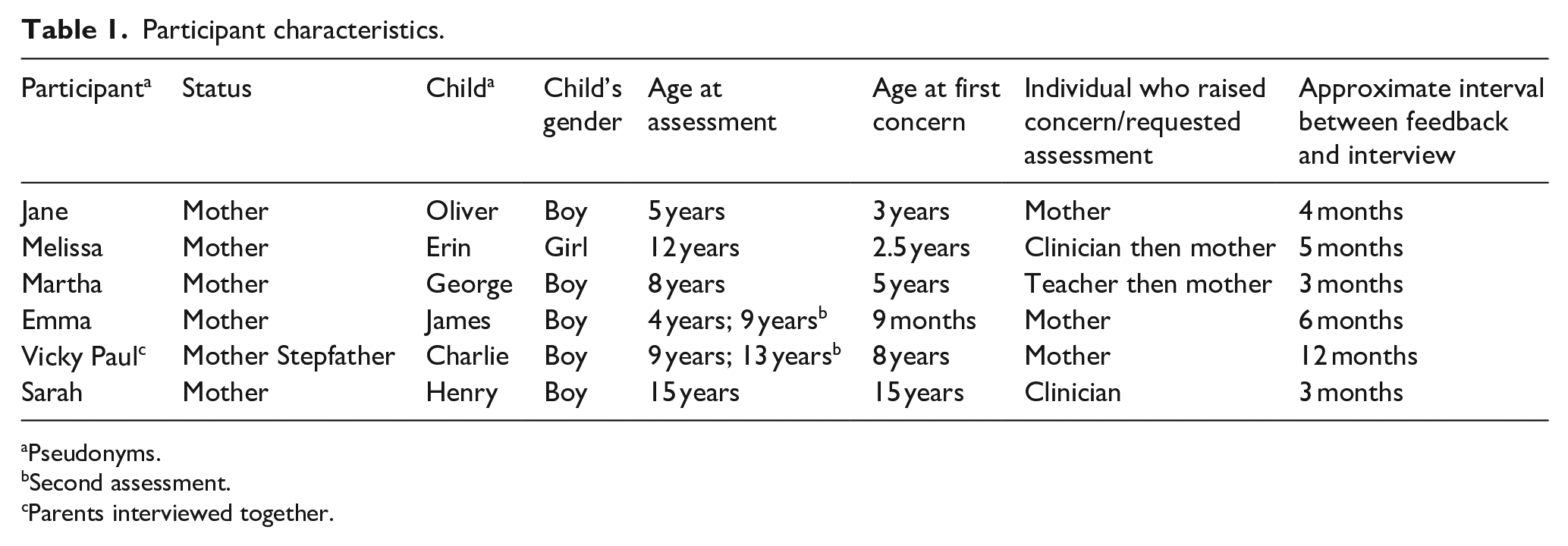
Pseudonyms.
Second assessment.
Parents interviewed together.
Data collection and community involvement
Face-to-face semi-structured interviews were conducted in English over a 4-month period by the first author, who was not involved with the assessment. Interviews were audio-recorded and ranged from 36 to 80 minutes. Six interviews were conducted, five individual (mother only) and one joint interview (mother/stepfather). As suggested by Smith and Osborn (2003), interviews followed a schedule (see Appendix 1), although participants’ experiences were explored further where necessary. Participant packs and questions were developed by the authors (clinical psychologists with ASD diagnosis experience) based on clinical experience and in response to a noticeable gap in the literature. They were reviewed by the NDT and a community member from the universities’ People Panel, a parent of a child with ASD. Positive feedback was received, and therefore, no changes were made. Following recommendations from Elliott and Timulak (2005), field notes recording observations and reactions were kept to aid coding.
Data analysis
In accordance with the hermeneutic phenomenological approach, interviews were manually transcribed and analysed (Smith et al., 2009). The first author read and re-read each transcript, before undertaking a line-by-line analysis where exploratory comments (descriptive, linguistic and conceptual) were recorded to identify abstract concepts. Similarities between concepts were highlighted to identify emerging themes, which reflected shared meanings between individual’s experiences. A table summarising themes and illustrative quotes was produced. Furthermore, a cross-case analysis involved searching for similarities between transcripts to generate superordinate themes.
Results
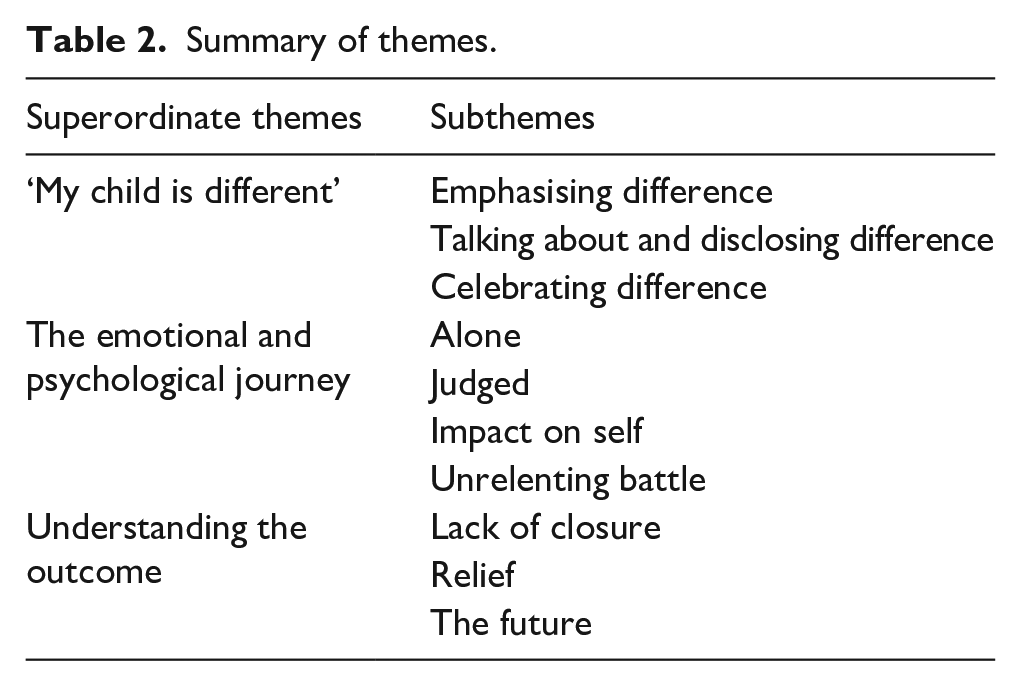
Three superordinate themes emerged as follows: (1) ‘My Child is Different’, (2) The Emotional and Psychological Journey and (3) Understanding the Outcome (Table 2).
Summary of themes.
‘My child is different’
Emphasising difference
All parents described their child as different. Some used terms such as ‘non neuro-typical’, ‘complex’, ‘not normal’ or listed characteristics which set their child apart. As illustrated by Melissa, noticing disparities with others was often the catalyst for identifying, and later accepting, their child as being ‘different’: I could see she was emotionally behind (. . .) I made excuses for it a bit y’know but at high school everyone was boyfriends and makeup and she wasn’t . . . I could just really notice. – Melissa
1
Other parents emphasised their child’s differences through similarities to those with a diagnosis. They also used the severity of symptoms and diagnostic label as a benchmark for interpreting their own child’s differences: I’m not saying that he’s got a very bad case (. . .) I’d say he is . . . he has . . . he shows traits (. . .) my brother’s son had autism (. . .) he didn’t speak until five, so I know there is extreme cases. Charlie’s not like that (. . .) but he is . . . he does have the traits . . . I watch the programme The Undateables
2
and there are sometimes some characters in that and I’ll go ‘that’s Charlie!’ – Vicky
Vicky perceived Charlie’s presentation was synonymous with people diagnosed with autism, and while she appreciated the spectrum of symptom severity, she believed the similarities were compelling. Consequently, she was confused and frustrated about why Charlie was not diagnosed. This is detected through the repetition and hesitation in her quote. Like Vicky, other parents affirmed that they knew their child best, and by emphasising the differences, they were attempting to highlight their need for diagnosis.
Talking about and disclosing difference
Most parents did not want their child defined by a ‘label’. However, this provided a dilemma of how best to describe their difficulties: I hate using the word different or not normal but it’s the only language I’ve got. He will say, ‘I know mummy that my mind isn’t built like everyone else, but I can’t cope with it’ which is difficult to hear. – Emma
Emma’s quote illustrates that limited knowledge and terminology to explain James’ differences is a painful experience. It also indicates how powerless she feels not being able to resolve this.
Some parents reflected on the dilemma of disclosing their child’s differences as a way of pre-empting difficult situations. Jane reported ‘you’re constantly battling between do I point out that he’s different or do we wait until there’s a crisis?’ Alternatively, Melissa described that without a valid label, pre-emption is futile: I’d gone to the high school and said these are Erin’s traits, this is what she’s going to have difficulty with. They said ‘oh we have lots of people like that’. So I think because there wasn’t any specific diagnosis they just thought I was a worried mum. – Melissa
Celebrating difference
Parents acknowledged that their child’s differences formed their character and made them who they were: Even though I want to take all this away from him, I don’t because if I did he wouldn’t be my James. – Emma He’s super clever where the computer is concerned. He’s designing his own games (. . .) and he’s like ‘I’m going to go and work for Google’ and I’m like ‘you’re going to own Google’. I couldn’t be prouder. – Vicky
Throughout the interview, Vicky highlighted her son’s fascination with computers as an ‘autistic trait’ impacting negatively on his ability to make friends. Yet she recognised that this unique attribute sets him apart from others in a positive manner and should be celebrated.
The emotional and psychological journey
Alone
Throughout the journey, parents felt alone. Some reported feeling marginalised by friends due to their child’s behaviour or their lack of time for socialisation. Others perceived their loneliness as a consequence of their concerns being dismissed.
Loneliness was predominantly experienced at the beginning of the journey as parents interpreted symptoms differently. Emma stated ‘my husband was in denial’. She reflected on how difficult this was, but interpreted his optimism as a disguise for fear of ‘stigma’. Martha’s views differed to her husband’s; she interpreted this as ‘mother’s intuition’ and assumed responsibility to seek support. The quote below demonstrated that loneliness impacted more after the assessment: We’ve just been left! I feel like I’ve been blindfolded and put in the most peculiar maze ever and I can’t find my way out and I’m trying to get to Charlie . . . and I can’t, I can’t get to him, because I . . . try and help him but he just doesn’t understand and that’s frustrating, that’s why as a family we need help. – Vicky
Vicky’s use of a metaphor emphasises her feeling abandonment due to lacking professional support. She also demonstrates a sense of ambivalence; she wants to get out of the maze aware that Charlie is stuck inside. There is a sense of feeling lost, hopeless and needing guidance, as they are struggling to understand and communicate with him. Her words ‘I’m trying to get to Charlie and I can’t’ gives a sense of Charlie’s loneliness and isolation: If you’ve got a diagnosis they say ‘right we’ll take you on all these courses’, but if you’ve got a diagnosis of non neuro-typical (. . .) you drift and you’re alone. There’s no counselling or no one to talk to . . . you can’t talk to your husband cos it’s painful. – Jane
Jane illustrated her belief that diagnosis would have prevented feeling marginalised by professionals. She also highlights the emotional impact of parents feeling unable to support each other which exacerbates feelings of loneliness.
Parents placed a high value on shared identity. However, most reported to seek support and shared experiences externally due to the heightened emotional impact within the family. Jane, who had a supportive family network, reflected that parenting a child with autistic traits and undergoing assessment was ‘the undoing of a lot of families!’ Although she and her husband struggled to comfort one another, she valued the supportive aspect of attending ‘groups with other children with special needs’. Similarly, Emma valued the support from a mother whose son has autism, stating ‘that’s the one positive thing that’s come from this’. This demonstrates the importance of belonging, acceptance and shared experience. Parents felt that having a diagnosis would offer commonality with others.
Judged
Many parents worried about whether their concerns would be validated. This was heavily influenced by the perceived judgement or ‘paranoia’ they would receive in the event that a diagnosis was not given: I did say to Dr A I hope you don’t think this is (. . .) Munchausen by proxy. I’m not afraid to say that [laughs]. I’m afraid you think that (. . .) because obviously Oliver has been in and out of hospital for lots of reasons, medical reasons, and of course when it’s medical you can see it can’t you? – Jane
Judgement or ‘paranoia’ is driven by fear and anxiety, as illustrated in Jane’s quote. She was anxious that due to having no visual symptoms, her concerns would be disregarded. Consequently, she feared professional judgement. Jane’s own use of the phrase ‘Munchausen by proxy’ suggests that naming this openly would provide a level of control over this thought and ease her anxiety of this being considered by others. Her laughter, however, demonstrated that she felt uncomfortable about raising the topic: I was so apprehensive because I thought if she goes ‘nah, there’s nothing wrong with him’, then I thought it’s all in my head, but when she said she might see him like very low on the spectrum I thought oh at least she’s seeing something. – Martha
Martha’s quote highlights the extent to which parents are affected by the perceived judgement of professionals not validating their concerns. Martha initially felt assessment was unnecessary, but requested it to satisfy the school’s concerns. Nevertheless, she was relieved that ‘something’ was identified, as this alleviated the burden of it being in her head: Because he hasn’t had a diagnosis I kind of get the feeling that other people think . . . it’s just in her head because they’ve said there’s nothing you know . . . clearly wrong . . . she’s just making it up . . . it used to be really hard to deal with. Now as time’s progressing I kind of think ‘stuff what anyone else thinks’. – Emma
Emma illustrated that she had learnt to manage her worries about being judged and recognised this as an area of self-growth. While diagnosis is not appropriate in all cases, feeling heard was invaluable. One mother stated ‘I had a good experience with Dr C, he listens and doesn’t say ‘no you’re wrong or that’s not it’, it’s easier when you have a ‘it doesn’t fit’, it’s easier because people actually listened’.
Impact on self
Throughout the interviews, all parents described a great sense of responsibility. This was largely due to their own expectations of how they ‘should’ react and their desire to feel in control: Horrendous, just horrendous. I felt helpless. As his mother, I should be able to help and I couldn’t. I couldn’t take it away. Whatever it was I couldn’t take it away. I couldn’t help. – Emma
Emma’s use of the words ‘horrendous’, ‘helpless’ and repetition of ‘I couldn’t’ illustrates the strong emotional impact on parents when they were unable to meet their own expectations of parenting.
Some parents described the multifaceted roles of being a parent, including being ‘an investigative journalist’, ‘the most organised diary keeper’, ‘an advocate’, a ‘teacher’ and a ‘therapist’. Trying to fulfil these as a way of trying to gain control and minimise hopelessness. However, parents highlighted that this required sacrificing other commitments. Having this level of involvement in their child’s life led to their emotions ‘bubbling up’ during assessments which they felt they had to ‘put a lid on’ to present the case coherently.
The pressure of ‘getting it right’ differed between parents. Sarah described the assessment as ‘a lot of pressure’, because she ‘didn’t want a label more than anything’. She stated ‘I was trying not to get upset, cos I was trying to put into context how we felt’. Whereas Jane, who believed her son will be diagnosed with autism in the future, described ‘it was sadness I felt, like I’d let him down’. Martha described difficulty with her memory during the assessment and worried this had impacted on her responses. These examples demonstrate the pressure parents experience during assessments and their subsequent feelings of doubt that the outcome was affected by their poor reporting.
Unrelenting battle
Parenting a child with autistic characteristics and the journey of seeking diagnosis and support was described as a ‘huge battle’. Melissa stated ‘you’re continually fighting for services, fighting for support, fighting for a better life’. Parents used words such as ‘painful’, ‘exhausting’, ‘disheartening’, ‘a sinking feeling’ and ‘like you’re walking through mud’ to describe the emotional impact of their perceived battle with the assessment process. Major factors contributing to this perception were long waiting times and the involvement of multiple professionals. This was evident as some families reported they had been ‘under services’ for years. Use of the word ‘under’ suggests that services are perceived as powerful and further denotes parents’ feelings of losing control: I’ve waited long enough. It’s . . . he’s been battling this since he was eight . . . no I’ve been battling since he was eight. – Vicky There’s always a road block at the end of the road we go down so we just have to U-turn. There are very long waiting lists to get seen, so if you get knocked back and try again it’s another six months. – Paul
Vicky and Paul illustrated their frustration about long waits and their use of the first person shows how the journey can affect the whole family. Other parents noted that being informed of long waiting times, albeit frustrating, helped to manage expectations: I’m angry now because I should have been stronger. I should have fought harder! One side of me was saying right well, there’s nothing wrong so that’s good (. . .) the other side was like no this isn’t right! – Emma
Emma described that she ‘should’ have fought harder, signifying an internal battle as if she did not do herself or her son justice. Jane emphasised the need to be strong and emotionally in control. She described mothers who were ‘fighting’ for diagnosis as ‘Lions . . . they’re strong women (. . .) y’know that overly dead sweet nurturing lioness thing, but y’know fiercely protective’.
Another aspect of the battle reported by parents was trying to gain public acceptance. Typical daily activities were described as a ‘challenge’. The lack of public awareness for autism and misinterpretation of the child’s behaviours often resulted in criticism or ‘staring’. This was illustrated by Melissa, whose quote depicts her interpretation that continually fighting with services and being judged in public led to personal self-growth. Consequently, she felt determined and ‘more confident’ to tackle situations directly to protect her daughter: I’m a lot more protective (. . .) if we’re in Tesco and she’s having a tantrum, which looks quite strange to most people at 13, and somebody will say something, I do sort of turn around (laughs). Whereas once I would have bit my tongue and got upset . . . I was just fed-up of people being negative towards her. – Melissa
Parents reflected that gaining a diagnosis might have changed this experience, giving the impression that diagnosis is a badge, which symbolises they have won the battle.
Understanding the outcome
Lack of closure
In discussing assessment outcomes, six parents reflected on their perceived lack of closure and the associated mixed feelings: It’s like having a boat and somebody holding onto the rope and that’s fine but then somebody lets the boat go, and you’re going ‘ok, now what we gonna do? (. . .) It’s going to be like until we get to a point where Oliver is either diagnosed or I get him a statement for what he is, because he’s not functioning in mainstream, but he hasn’t got any particular label to peg on a board. – Jane
Jane’s metaphor describes processing her emotions after the assessment. She illustrated a sense of the process being unfinished.
Some parents doubted the outcome perceiving professionals had only observed a ‘snap shot’ or seen the child on ‘a good day’. In addition, conflicting opinions from health and education services and in some cases between same service professionals, left parents confused and frustrated: Teachers have told me they can’t understand why he hasn’t been given a diagnosis because they can quite clearly see. – Emma I don’t understand how one person can say ‘yeah he’s on the spectrum’ and somebody else can do a U-turn and say ‘we don’t feel he needs help’. – Vicky
Their confusion was exacerbated by a lack of knowledge regarding access to further support or explanation. One parent felt relieved they could access emergency appointments, while others felt like a ‘burden’ or were too ‘angry’ to re-contact the service: It just feels like I’ve just had a locked door . . . I’m having to find this key, that is on a key chain with about a million keys on it . . . it’s just been, shut the door, lock it, that’s it. – Vicky
While Vicky’s quote suggested complete closure from the service, she lacked personal closure and felt alone in searching for answers and that her commitment was being tested. Consequently, she felt let down by the service: I think you need to know you’re not excluded from the building, ‘don’t come here anymore with your er . . . Munchausen by proxy, saying your son’s this and that and the other’ cos that’s not what I heard. – Jane
In many cases, parents recommended that the service should allow parents time to process the outcome before being invited to further discussions.
Relief
Four parents expressed some degree of relief that their child was not diagnosed. A stronger sense of relief was reported by parents whose child was referred based on professional advice, rather than their concern.
Sarah acknowledged the enormity of her relief by describing the potential impact of diagnosis. ‘It was a big relief! Because it’s not just about school, it’s about relationships and the rest of his life’. Martha also expressed relief, but demonstrated some ambiguity by questioning what the problem was if not autism. She also reflected on the importance of understanding her son’s needs better, particularly as they worried that his difficulties may have been attributed to their ‘parenting’: A relief! And a bit of a shock! (. . .) obviously he was showing a little bit of signs cos otherwise he wouldn’t have been assessed (. . .) it’s a mixture of feeling relieved (. . .) but a bit shocked as well cos we were like well why is he the way he is? – Martha
For other parents, relief was expressed as a fluid emotion that changed according to fluctuations in the child’s presentation. For example, Emma stated ‘initially I was relieved’ as her son exhibited improvements. However as these were short lived, her journey to fight for a diagnosis continued. Jane who also continued to seek a diagnosis explained, ‘It wasn’t easy to hear “no”, but it was easier than hearing yes’. She appeared to be relieved that despite her own concerns, she was pleased a diagnosis was not confirmed.
The future
When summarising the assessment process, all parents reflected on their future hopes and worries. Some expressed concerns regarding education and their child’s ability to independently manage the transition to adulthood: If she doesn’t get an education and doesn’t get the social support then what’s she going to do, what job will she have and what life will she have? – Melissa
Six parents also spoke of the value that a diagnosis would have provided in terms of gaining educational or therapeutic support, understanding and acceptance: If I’ve got that little piece of paper, just that little piece of paper, that just says what’s going on, give him a break, give him a chance. – Emma
Emma’s use of the phrase ‘that little piece of paper’, also used by two other parents, minimised the impact of diagnosis to being words on paper. Ultimately, they felt that their child’s difficulties could be explained by autism, but worried that without this validation they would not receive support. For some, this meant their child was unlikely to fulfil their potential, while others expressed concerns about their child’s well-being and mental health. Parents who worried less about the future felt that the assessment offered a deeper understanding of their child and were pleased that they could move forward.
Despite the difficulties parents reported in navigating this process, many highlighted positive aspects. They described it as ‘sensitively managed’, professionals as ‘skilled’, ‘friendly’ and that they ‘helped us understand’ by highlighting the child’s strengths rather than focusing on their difficulties.
Discussion
Interviewing parents about experiences of ASD assessments when no diagnosis was given offers important insights into: (1) Parents difficulties describing yet celebrating their child’s differences. (2) The varied emotional and psychological constructs experienced during the journey, for example, feeling alone and judged. Contributing factors are identified including waiting times and fighting to be heard or for acceptance which led parents to view the journey as a battle. (3) Mixed emotions related to hearing the outcome, such as, feeling relieved yet lacking closure and questioning the future.
Similar to Lappé et al. (2018), one of the main issues raised by parents was making sense of and feeling conflicted about how to describe their child’s differences. Lappé advocates for increased societal acceptance to reduce burden for those diagnosed with autism. However, we suggest this is extended further to promote wider acceptance around neurodiversity and behavioural differences. This could be achieved through providing a formulation, as Legg and Tickle (2019) advocate information sharing is fundamental to parents making sense of their child’s presentation.
NICE (2011) guidance recommends that parental concerns are appropriately acknowledged. However, similar to other research (Legg & Tickle, 2019), the theme of parents feeling ‘paranoid’ that professionals would not believe or validate concerns was apparent. While two parents felt professionals did not listen, others experienced this fear was unfounded. They reported that professionals were ‘friendly’, ‘listened’ and ‘asked the right questions’. One parent described that being informed of their child’s strengths and weaknesses in relation to why the diagnosis was not made, improved her understanding and empowered her to seek educational support. Although mixed experiences were reported, this somewhat contradicts the experience of parents who received a diagnosis in Crane et al. (2016), who felt ignored or were re-referred. Nevertheless, this highlights the importance of patient–professional relationships and the impact of power dynamics. These relationships involve a careful balance between vulnerability and trust; impaired relationships result in poor outcomes and patient dissatisfaction (Gordon & Beresin, 2016). Interestingly, in Crane et al. (2018), professionals felt parents entered ‘knowing’ their child had ASD and were reluctant to consider otherwise. Therefore, professionals should invest time to build positive patient relationships based on mutual trust, knowledge and respect, which are key to empowering patients and improving satisfaction (Chipidza et al., 2015).
‘Relief’ was commonly reported across the ASD assessment literature. For parents who received a diagnosis, this related to knowing the outcome, working towards acceptance or vindicating their concerns (Abbott, Bernard & Forge, 2013; Midence & O’Neill, 1999). Parents in the current sample similarly attributed relief to knowing the outcome, but also not having their child defined by a label. However, in some cases, relief was transient as on reflection hearing that ASD symptoms were evident, despite not meeting the full diagnostic criteria, mitigated their perceived judgement or strengthened their fight for further assessment. Given the theme of parents feeling ‘judged’, it is reasonable to consider their expressed relief potentially as a socially desirable response. Positive parent–professional relationships may allow further exploration of individual reactions during feedback sessions along with providing parents time to process and adjust to the outcome. In such cases, post-assessment support informed by Acceptance and Commitment Therapy (Hayes & Strosahl, 2005) may be beneficial.
Like the parents whose child was diagnosed with ASD in Goin-Kochel et al. (2006), parents were dissatisfied with long waits. While not unique to this sample, this was often related to parents interpreting their experience as a ‘battle’ and unlike other samples, could be explained by the outcome not justifying the process as they lacked closure. However, parents who expected waits, having been informed by friends or support groups, rather than the service itself, were more accepting. One parent, whose child was seen urgently, reflected positively. She explained that knowing the outcome quickly enabled them to move forward rather than ‘it hanging over your head’.
Clinical implications
The difficulties reported by parents predominantly related to issues before and after the assessment. Therefore, providing information at the point of referral about waiting times, the assessment process and advice to record information prior to assessment, could alleviate parents’ apprehension and ‘pressure to get it right’. Adopting a similar model to dementia services, where pre- and post-assessment counselling is offered, might provide the associated benefits of parents’ engagement with services and better adjustment to outcomes (La Fontaine et al., 2014). In autism services, counselling could enhance the parent–child–professional relationship and reduce parents’ perception of ‘fighting’ services. During pre-assessment counselling, parents’ concerns, their reasons for seeking diagnosis and expectations can be discussed to ensure parents feel heard and are aware of all possible outcomes. Providing a named clinician or ‘expert by experience programme’ at all stages could reduce parents feeling ‘alone’. Following the outcome, the programme would be facilitated by ‘experts’ who also did not receive a diagnosis. This would allow parents space to reflect, experience ‘shared identify’ or seek advice around acceptance or wider support where necessary. Post-assessment counselling to provide a formulation developed in collaboration with parents outlining why the diagnostic criteria was not met is also encouraged. This may empower parents while affording the opportunity to explore the emotional impact of the assessment, reduce feelings of ‘abandonment’ and henceforth reduce re-referrals. Formulation will also equip parents with appropriate language to describe their child’s needs whilst celebrating their strengths, and address worries that the outcome was based on a ‘snap shot’ or that their inadequate reporting impacted decisions. Furthermore, the authors strongly advocate for support based on clinical need rather than diagnosis; thus, formulation is critical. Sharing the formulation will educate other professionals involved, enhance collaborative working, knowledge and acceptance of neurodiversity and embed needs-based plans.
To achieve this, the interpersonal, therapeutic and diagnostic skills of the professional are important. They must have the appropriate training, knowledge and attitude to conduct assessments and provide sensitive feedback. Specific training to deliver non-diagnosis along with time to reflect on the impact of this during supervision is vital.
Ultimately, improving families’ experience of the assessment process may facilitate acceptance of the outcome. However, whilst it is important to consider areas of improvement to ensure best practice, positive aspects were highlighted and should be recognised as areas of strength for future benchmarking.
Strengths, limitations and future research
Key strengths relate to the unique sample and in-depth exploration of their experiences using high-quality IPA (Smith, 2011). However, the cross-sectional design meant parents’ experiences were only explored at one time point. Parents reported needing time to process the outcome, suggesting their feelings and reflections may change. Therefore, future research should utilise longitudinal methodologies. In addition, some parents planned to seek further assessment; thus, a follow-up to compare assessment outcomes and parents’ experience of this would be useful. Interviews were conducted in the clinic where the child was assessed, which may have inhibited parents to share certain experiences. Future research may benefit from neutral interview facilities, recruiting participants from multiple services, and the inclusion of more fathers. Additional socio-demographic data are recommended to ensure inclusion of participants from minority backgrounds. The authors, clinical psychologists, acknowledge potential bias towards psychological aspects of parents’ experiences, although minimised this by keeping field notes and reflecting openly on their interpretations.
Conclusion
Important insights into parents’ practical, emotional and psychological experiences associated with not gaining an ASD diagnosis for their child are provided along with useful clinical implications: promoting positive parent–professional relationships, pre-/post-assessment counselling, and the importance of formulation and needs-led support.