
Abstract
Caregivers of adolescents with autism spectrum disorder commonly experience stigma. However, how stigma influences social interactions of adolescents with autism spectrum disorder is unclear. We aimed to explore the impact of caregiver stigma on real-life social experiences of Taiwanese adolescents with autism spectrum disorder. In the context of everyday activities, 76 adolescents with autism spectrum disorder who were not intellectually disabled (69 males, aged 10–16 years) carried a mobile device that prompted them 7 times, randomly, each day for 7 days to record with whom they were interacting, what they perceived, and how they felt about the interactions. Caregivers completed the Affiliate Stigma Scale to measure caregiver stigma. Multilevel analyses revealed that participants whose caregivers perceived high levels of stigma were more likely than those whose caregivers experienced less stigma to interact with family members and less likely to be interested in interacting with people at school. However, those participants also experienced more anxiety while interacting with family members. The findings shed light on ways that caregiver stigma impacted the social experiences of adolescents with autism spectrum disorder and suggest that, in promoting social participation for adolescents with autism spectrum disorder, researchers and service providers must support caregivers to manage stigma.
Lay abstract
Caregivers of people with autism spectrum disorder commonly experience stigma. As a result, they may avoid contact with others, in turn, influencing their child’s social participation. This study aimed to explore the impact of stigma perceived by the caregivers on the everyday social experience of Taiwanese adolescents with autism spectrum disorder. We asked 76 adolescents with autism spectrum disorder who did not have intellectual disability (69 males, aged 10–16 years) to carry a mobile device for 7 days. The device prompted them 7 times each day to record who they were interacting with, what they perceived, and how they felt about their social interactions. In addition, we asked their caregivers to complete the Affiliate Stigma Scale to measure their experience of stigma. We found that participants whose caregivers perceived high levels of stigma were more likely to spend time with family members and less likely to be interested in interacting with people at school. Those participants also were more likely to experience anxiety while interacting with family. Our study suggests that it is important for clinicians to implement support services for adolescents with autism spectrum disorder and help caregivers in managing stigma to promote their child’s social participation.
Keywords
Introduction
Social participation is an integral, yet diminished, experience for adolescents with autism spectrum disorder (ASD), including those without intellectual disability (ID). Difficulties with social communication and restricted interests and behaviors characterize ASD (American Psychiatric Association [APA], 2013). Consequently, they experience difficulty understanding social expectations (Bauminger et al., 2010; Orsmond et al., 2013) and maintaining reciprocal friendships (Kasari et al., 2011; Locke et al., 2010). In comparison with typically developing (TD) peers, adolescents with ASD frequently limit their interactions with peers in social activities, spending time alone or with parents (Kasari et al., 2011; Orsmond & Kuo, 2011; Orsmond et al., 2013; Potvin et al., 2013; Taheri et al., 2016). They report poorer quality of social life than TD peers (Egilson et al., 2017). Furthermore, Sutton et al. (2005) found a negative association between ASD severity and self-awareness of social difficulties in children and young people with ASD who did not have ID. Similarly, Chen and colleagues (2016, 2017) found that individuals with milder ASD symptoms were less likely than those with more severe ASD symptoms to engage socially and experience greater anxiety during social interactions.
Despite social difficulties, many individuals with ASD seem to value and desire social engagement (Bauminger et al., 2004; Bauminger & Kasari, 2000; Chen et al., 2015; Maddox & White, 2015; Müller et al., 2008). Findings of reduced preferences to be alone and longing for deeper relationships as well as loneliness in the context of social interactions may support the presence of a desire for social engagement (Müller et al., 2008). Researchers (Chen et al., 2016; Cordier et al., 2016) found that people with ASD reported enjoying time with friends. However, conscious awareness of being different and fear of being rejected may contribute to fewer attempts at social engagement (Müller et al., 2008).
Given that social participation in adolescence strongly predicts life satisfaction and adult well-being (McCullough et al., 2000; Olsson et al., 2013), promoting positive social experiences and a supportive social environment would be beneficial for emotional and behavioral development (Camara et al., 2017; Vitaro et al., 2009). Thus, there is a need to explore the ways in which social contexts influence the experiences of social participation of adolescents with ASD.
Stigma, a phenomenon whereby people in society reject individuals with physical or social attributes that disqualify them from being socially accepted (Goffman, 1963), may be a significant barrier to social participation for adolescents with ASD. Although individuals with ASD have a typical physical appearance, behavioral tendencies that may not fit social norms, coupled with the public’s lack of knowledge about the disorder, can generate a stigma aimed at individuals with ASD and their carers (Broady et al., 2017). In fact, caregivers commonly report that their child is misunderstood, humiliated and excluded due to peers’ lack of awareness or reluctance to accept ASD symptoms (Kinnear et al., 2016; Whitaker, 2007). Although fewer ASD symptoms may lead to less stereotyping and exclusion (Kinnear et al., 2016), stigma is still a prominent factor restricting participation for adolescents with ASD who are not intellectually impaired (Broady et al., 2017; Liao et al., 2019).
Parents often report experiencing stigma because they have a child with ASD (Mitter et al., 2019; Ng et al., 2020). Many report feeling blamed for their children’s behaviors (Broady et al., 2017; Farrugia, 2009), leading to isolation from family and friends (Broady et al., 2017; Kinnear et al., 2016) and feelings of helplessness to change the situation (Daniels et al., 2017). Consequently, many caregivers restrict contact with others and avoid going out with their child (Blanche et al., 2015; Farrugia, 2009; Mitter et al., 2019). Furthermore, family context influences social participation of adolescents with ASD (Krieger et al., 2018). Thus, caregiver isolation may influence both the quantity and quality of adolescents’ social experiences.
Cultural contexts may play a critical role in heightening stigma associated with ASD. Papadopoulos and colleagues (2002, 2013) noted the impacts of cross-cultural variations in individualism and collectivism on stigma toward mental illness. Specifically, stigma toward mental illness tends to be heightened in more collectivistic cultures where interdependence and following social norms are highly valued. In contrast, stigmatizing attitudes are less common in more individualistic cultures where independence and tolerance for deviation from social norms are higher. Regarding stigma toward ASD, previous researchers (Obeid et al., 2015; Someki et al., 2018) found that college students in Japan and Lebanon, of which their cultures are often associated with being collectivistic, reported greater autism-related stigma than counterparts in the United States.
Chinese culture is characterized by collectivism, emphasizing the importance of adherence to social norms. Thus, the traditional Chinese perspective of disability bringing shame to a family has been noted repeatedly in previous studies (Chou & Schalock, 2007; Lin et al., 2012; Mak & Chen, 2006). Not surprisingly, Chinese parents of children with disabilities and mental illness report high levels of stigma (Mak & Cheung, 2008; Mak & Kwok, 2010; Zhou et al., 2018).
The sequelae to caregiver stigma may significantly influence participation in daily activities among Chinese adolescents with ASD. In a study of 91 young adults in Taiwan, C. F. Chang (1996) identified limited participation in employment, schooling and community life, with most staying at home. Chen et al. (2017) revealed that Taiwanese adolescents and adults with ASD were more likely than their Australian counterparts to stay at home. While there has been only one study, to date, showing negative relationships between stigma perceived by parents living in Hong Kong and adolescents’ involvement in community and self-care activities (Ng et al., 2020), how caregiver stigma influence the subjective experiences in social participation of adolescents with ASD, especially those who live in Eastern countries, remains unknown.
With increasing awareness and prevalence of ASD in Taiwan in the past two decades (Chien et al., 2011), a better understanding of this area can facilitate health professionals to support adolescents with ASD and prioritize interventions to improve caregivers’ management of stigma. Examining the implications of caregiver stigma on children will help identify the specific needs of both caregivers and their adolescents with ASD. The purpose of this study was, therefore, to investigate the impact of caregiver stigma on the real-life social experience of Taiwanese adolescents with ASD. First, we explored with whom the adolescents spent their time. Second, we examined how caregiver stigma was associated with their adolescents’ engagement in social interactions. Given the heterogeneity of ASD, we also investigated the extent to which levels of ASD severity influenced adolescents’ engagement in social interactions. Third, we investigated adolescents’ experience of real-life social interactions. Finally, we examined whether caregiver stigma and severity of ASD moderated the relationships between the social experiences and engagement in social interactions for adolescents with ASD. We hypothesized that higher levels of caregiver stigma would be associated with more negative social experiences for adolescents with ASD. We also hypothesized that adolescents with less severe ASD or fewer ASD symptoms would be more likely than adolescents with more severe ASD to have reduced social participation due to an increased awareness of social deficits.
Methods
This study is part of a larger project led by the second and third authors to investigate the everyday social experiences of adolescents with ASD. The study had ethics approval from the University of Sydney Human Research Ethics and the Research Ethics Committee of National Taiwan University Hospital (NTUH). All participants and their parents provided informed consent.
Participants
Using research flyers and social media, we advertised the study at schools, ASD-related organizations, and parent support groups. Participants met the following inclusion criteria: (1) formally diagnosed with ASD by a psychologist or psychiatrist with the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000) or DSM-5 (APA, 2013), (2) aged 10–16 years, and (3) competent in reading comprehension to understand the surveys. While we had previously explored social experience in people with ASD aged 16 years and older (Chen et al., 2016, 2017), in this study, we extended the research population to young people aged between 10 and 16 years. To ensure participants had sufficient reading comprehension to respond to an experience sampling methodology (ESM) survey that contained Chinese characters read by Taiwanese students at Grade 3 (i.e. approximately 10 years of age) (Wang et al., 2008), participants were required to have passed their Grade 3 Chinese subject without any additional educational support. We included participants with a concomitant mental health diagnosis (e.g. attention deficit/hyperactivity disorder (ADHD) and/or anxiety). To ensure the participants did not have an ID, they were required to attend mainstream classes without any special education supports for academic or cognitive difficulties. Participants’ caregivers completed a questionnaire to collect caregivers’ and adolescents’ demographic information. They also completed the Social Communication Questionnaire–Current Form (SCQ) (Rutter et al., 2003) to evaluate severity of the participants’ ASD. We excluded participants if (1) they had a concomitant diagnosis of ID or other neurological disorder (e.g. cerebral palsy) or (2) they received educational supports for academic or cognitive difficulties. In addition, those who completed fewer than 17 ESM surveys in 7 days were excluded (see section “Procedures”).
Participants included 76 adolescents with ASD who were not intellectually disabled according to parent reports and school records (69 males, 7 females), aged 10–16 (M = 12.7; SD = 2.1). Their main caregivers (n = 76) completed the demographic questionnaire and measures of ASD severity and stigma. All participants had at least one sibling and were residents of Taiwan. All had good comprehension and expression of Mandarin as evidenced by their ability to converse fluently with the researcher during the training session. Thirty-five participants attended elementary schools and 41 attended high schools. Thirty-three participants had at least one concomitant mental health diagnosis (e.g. ADHD, emotional disorders, obsessive–compulsive disorder). Some participants received therapy for behavior management or to improve social skills. More than half of participants took medication for attention or behavior management. The caregivers’ mean age was 43.9 (SD = 5.4) years. Mothers were the primary (93.4%) participating caregiver. Tables 1 and 2 present the characteristics of participants and their caregivers.
Characteristics of participants (N = 76).
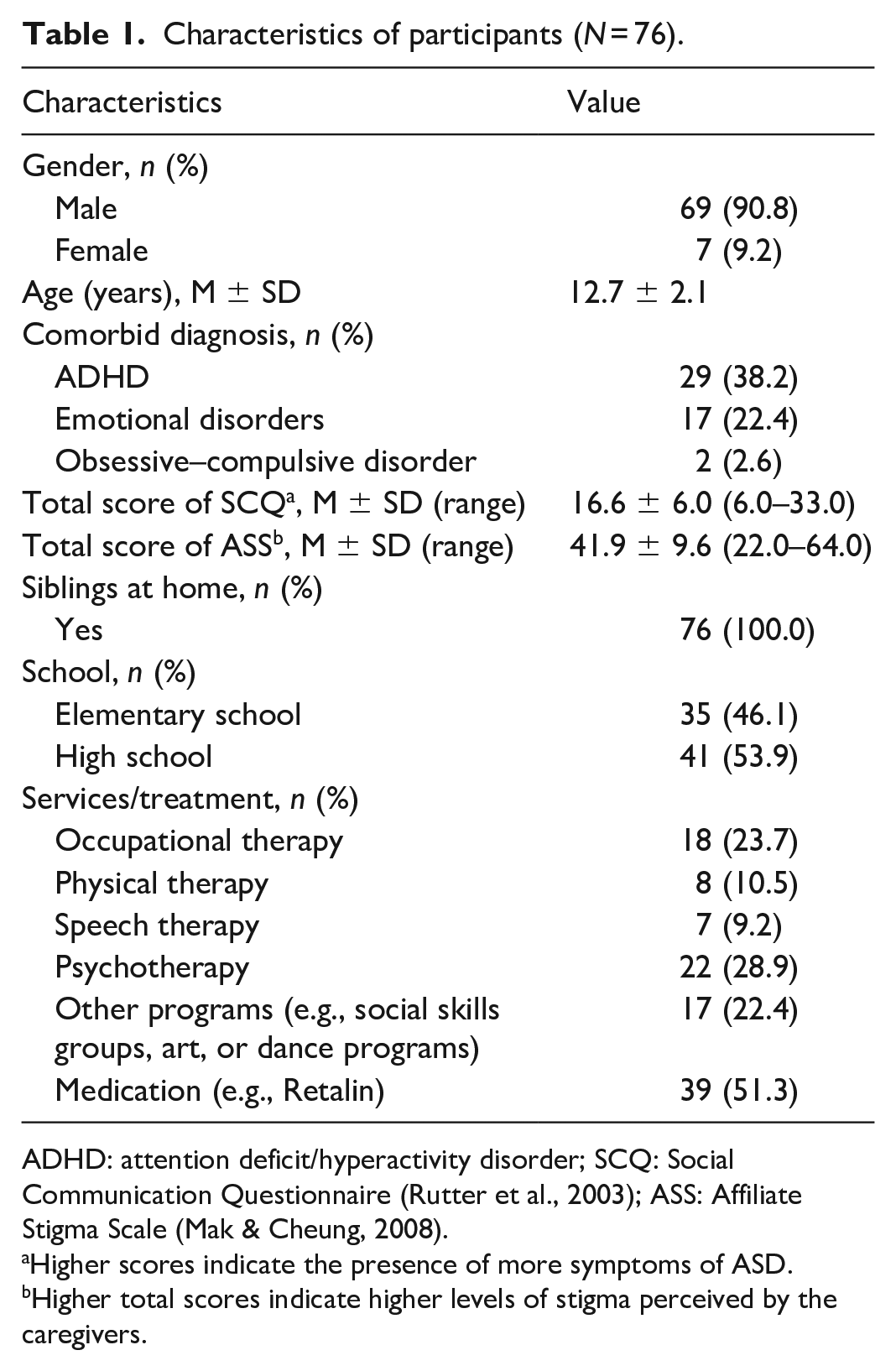
ADHD: attention deficit/hyperactivity disorder; SCQ: Social Communication Questionnaire (Rutter et al., 2003); ASS: Affiliate Stigma Scale (Mak & Cheung, 2008).
Higher scores indicate the presence of more symptoms of ASD.
Higher total scores indicate higher levels of stigma perceived by the caregivers.
Characteristics of caregivers who completed the SCQ and ASS (N = 76).
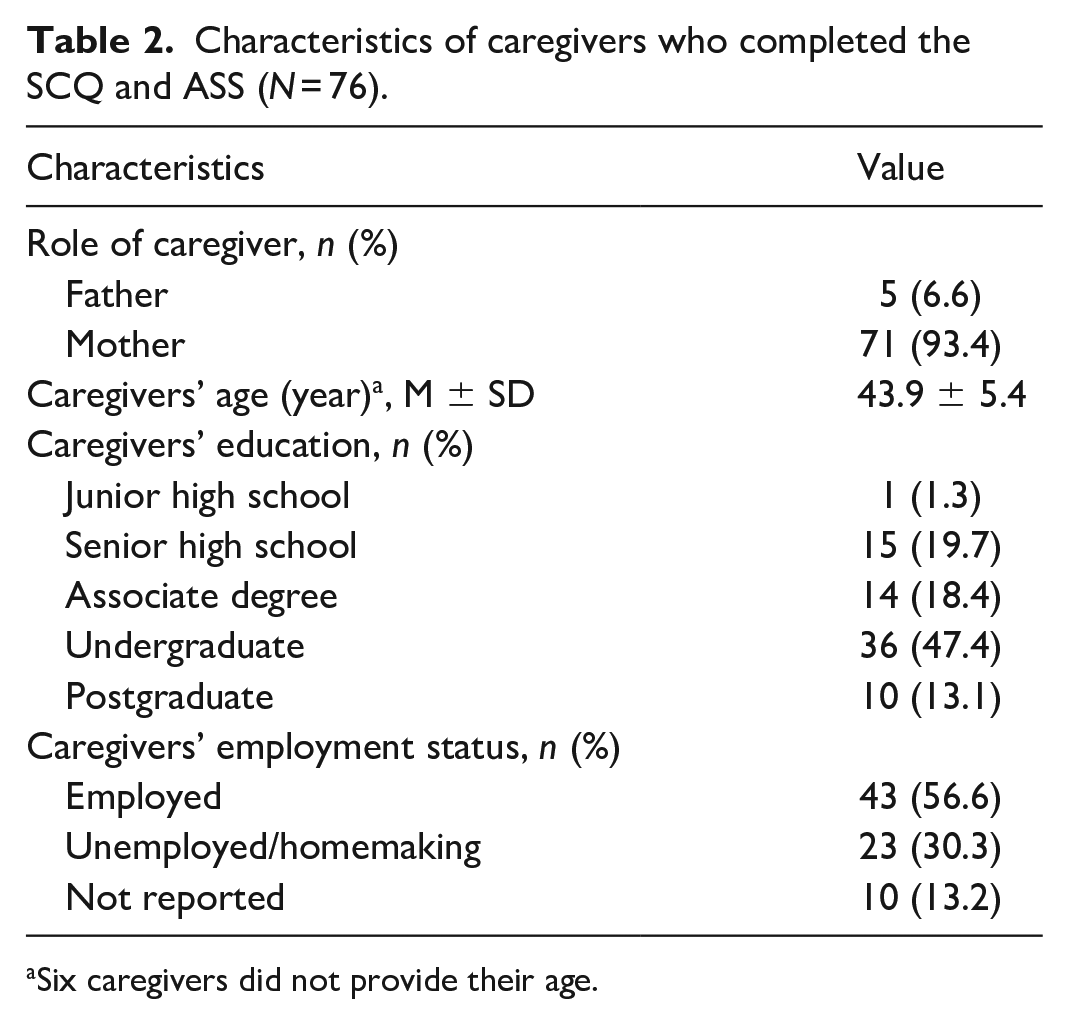
Six caregivers did not provide their age.
Instruments
Measure of real-life social experience
We measured participants’ social experiences using ESM, an ecological momentary assessment for self-report of everyday experiences, in context and over a period of time (Hektner et al., 2007; Shiffman et al., 2008). ESM is a reliable and valid method for use with individuals with ASD (Chen et al., 2014; Hare & Chen, 2019; Hare et al., 2015; Hintzen et al., 2010). We used a survey we developed in previous studies (Chen et al., 2014) to explore social interactions: which participants were interacting with at the time (i.e. “who were you talking to the most?”; see Table 2 for options) and their perceptions about, and feelings in, different social interactions (i.e. “were you enjoying yourself?”; “how interested were you?”; “did you feel lonely?”; “were you worried or anxious about what others were thinking?”; and “would you prefer to be alone?”). The survey comprised multiple-choice, “yes” or “no,” and visual analogue scale response options.
Measure of ASD severity
We used the Chinese version of the SCQ – Current Form (Gau et al., 2011; Rutter et al., 2003), a caregiver-report questionnaire, to evaluate the severity of the adolescent participants’ ASD. The SCQ consists of 40 items measuring social interaction, communication, and presence of repetitive behaviors over the past 3 months. Total scores range from 0 to 39, with higher scores indicating greater ASD severity. The SCQ has evidence for sound reliability and validity for evaluating ASD severity in both English (Chandler et al., 2007) and Chinese-speaking populations (Gau et al., 2011).
Measure of stigma
We measured the level of stigma experienced by caregivers with an adapted version of the Affiliate Stigma Scale (ASS) (Mak & Cheung, 2008). The ASS was originally developed in Hong Kong (Mak & Cheung, 2008) and has been used in Taiwan (C. C. Chang et al., 2017) to measure stigma perceived by caregivers of children and adults with an ID or mental illness. To be used in the current study, we replaced the term “mental illness” with “ASD.” The ASS includes 22 items; sample items include the following: “I feel emotionally disturbed because I have a family member with ASD”; “I feel that I am inferior to others because I have a family member with ASD”; and “I dare not tell others that I have a family member with ASD.” Items are scored on a 4-point scale with higher total scores indicating greater experience of stigma. The ASS has excellent evidence for internal consistency and validity in both Hong Kong and Taiwanese samples (C. C. Chang et al., 2015; Mak & Cheung, 2008).
Procedures
We provided each adolescent participant with an iPhone used solely to respond to the surveys. The survey was loaded onto the Participation in Everyday Life (PIEL) Survey Application App (Jessup et al., 2012) on the iPhone. Use of all other mobile functions and Apps was restricted.
After we received consent from participants, the researchers in Taiwan conducted a 30- to 60-min training session with each participant at the university campus. The training included the following: (1) using the iPhone device, (2) navigating the PIEL App, and (3) completing the ESM survey with the PIEL App. Caregivers completed the SCQ and ASS during the training session. Prior to data collection, we informed participants’ teachers of their students’ involvement in this study so that the adolescents were allowed to use their iPhone during class.
To yield a representative sample of social interactions without overburdening participants (Hare & Chen, 2019; Hektner et al., 2007), the iPhone prompted participants 7 times per day, randomly, during waking hours for 7 days to respond to the ESM survey. Participants could only access the survey when they were prompted. The app went silent if there was no response within 2 minutes. If the school permitted, two survey prompts were set during breaks and five prompts occurred after school during weekdays. Otherwise, prompts were scheduled in outside-school hours. On weekends, participants received seven prompts each day during free time. Participants answered as many surveys as possible but were instructed to ignore signals during inconvenient times (e.g. bathing). Responses were time-stamped and stored for data analysis. To ensure sufficient data were collected for analysis, we required participants to complete at least 17 of 49 surveys (>33%) during 7 days (Chen et al., 2014; Hintzen et al., 2010). Participants contacted the researchers if they required assistance.
Community involvement
No community partners were involved in the development of the research question, the design of the study, its implementation, or the interpretation and dissemination of the findings. All adolescents with ASD and their parents only engaged with the study as participants.
Data analysis
To represent time spent in social interactions, we calculated the proportion of responses during which participants were interacting with particular people (i.e. social interaction partner) (Hektner et al., 2007). To describe their self-perceived experience in different social interactions, we plotted perceived levels of “enjoyment,” “interest,” “loneliness,” and “in-the-moment anxiety” against social interaction partner. To account for individual differences, we centered each experience rating at the participant’s mean before plotting the relationships between self-perceived experience and engagement in social interactions. In addition, due to the dichotomous nature of the variables, we calculated the proportion of time each participant indicated that they preferred to be alone while interacting with particular interaction partners.
We used multilevel analysis (MLA) to examine associations between adolescents’ engagement in social interactions and perceptions of social experiences, and the moderating effects of stigma experienced by caregivers and ASD severity. We chose MLA because of the hierarchical structure of ESM surveys, in which the ESM survey questions (Level 1) are nested within each participant (Level 2) (Fleeson, 2007; Schwartz & Stone, 1998). MLA considers the dependency of surveys from the same participant by identifying the variability between surveys and between participants, in turn, allowing researchers to study relationships among variables at different levels (Hox, 2018; Snijders & Bosker, 2012). Utilizing MLA also minimizes the chance of forming misleading conclusions at one level (i.e. participant) based on observed findings on another level (i.e. survey) (Hox, 2018). Accordingly, MLA enhances statistical power for detecting expected effects and thus is more appropriate than conventional ordinary least squares (OLS) approaches for ESM data (Hox, 2018). Nonetheless, considering the complexities of model estimation and determining sample size at more than one level, calculating the statistical power for MLA is complicated. Hox (2018) suggested a minimum sample size of 50 for Level 1, and 20 for level 2 (i.e. a total of 1000 surveys from 50 participants) to accurately estimate the associations between variables in Level 1 (i.e. ESM variables) and Level 2 (i.e. ASS and SCQ scores).
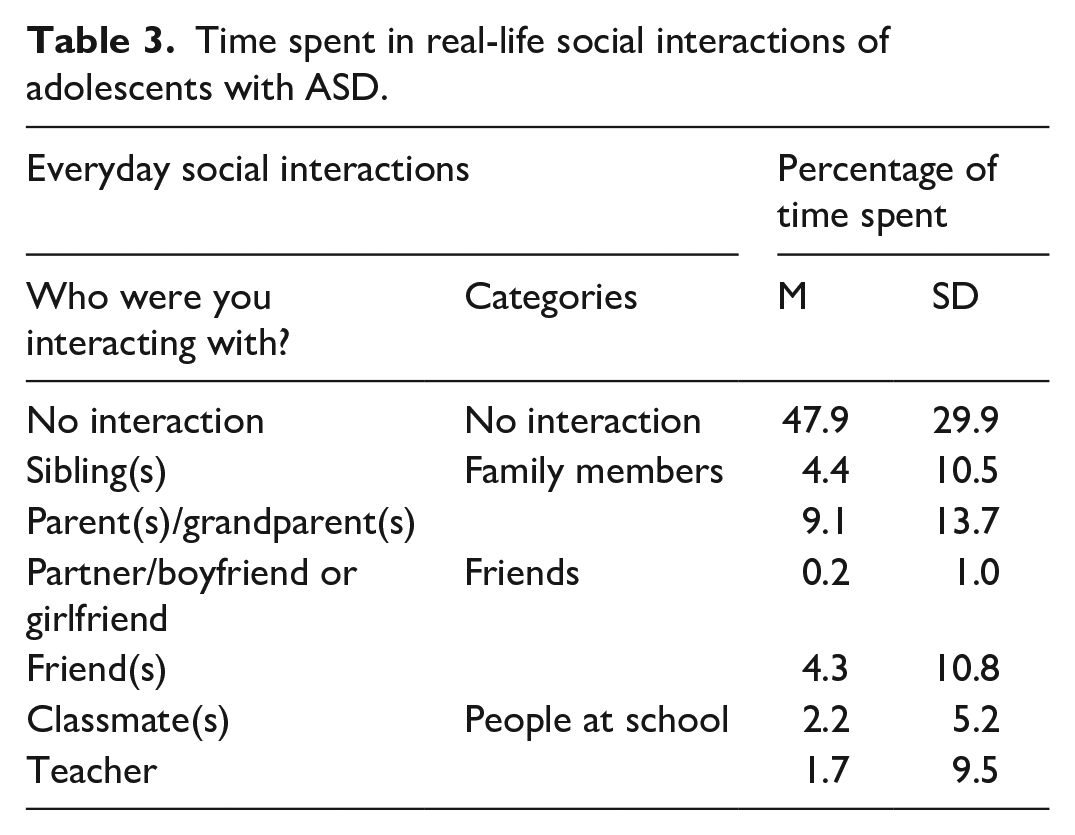
To identify how the levels of caregiver stigma and ASD severity influenced the adolescents’ engagement in social interactions, we conducted a multilevel multinomial analysis. The dependent variables were generated from the ESM data, which included three dummy variables of social interaction categories: “family members,” “friends,” and “people at school”; “no interaction” was the reference. Table 3 lists the specific social interaction partners in each category. We included caregiver stigma, measured by ASS, and ASD severity, measured by SCQ, as Level 2 independent variables. These level 2 independent variables were grand-mean-centered for comparison across participants (Hox, 2018; Snijders & Bosker, 2012).
Time spent in real-life social interactions of adolescents with ASD.
To examine the associations between self-perceived experiences and engagement in social interactions, we conducted four multilevel linear analyses for dependent variables from the ESM data: levels of “enjoyment,” “interest,” “loneliness,” and “in-the-moment anxiety.” Social interaction categories served as Level 1 independent variables represented by three dummy variables: “family members,” “friends,” and “people at school”; “no interaction” was the reference. In addition, we conducted a multilevel logistic analysis to examine the relationship between social interactions and the dependent variable “prefer to be alone.” We also included two Level 2 independent variables: caregiver stigma, measured by ASS, and participants’ level of ASD severity, measured by SCQ, in each MLA. ASS and SCQ data were grand-mean-centered (Hox, 2018; Snijders & Bosker, 2012).
To examine potential moderating effects of the levels of caregiver stigma and ASD severity on the relationships between the engagement in social interactions and self-perceived experiences, we then added the interactions between Level 1 and Level 2 independent variables to the original MLA. These additional analyses helped identify whether the Level 2 independent variables moderated the relationship between the Level 1 independent and dependent variables.
We used the HLM 7 Software (Raudenbush et al., 2011) for MLA. To evaluate the strength of associations between the independent and dependent variables, we estimated fixed regression coefficient (β) and calculated standard errors (SEs) for the MLAs. In addition, we calculated the odds ratio (OR) and corresponding 95% confidence intervals (CIs) for the multilevel nominal analysis and multilevel logistic analysis. Positive β or OR > 1 indicates a high likelihood of an association between independent and dependent variables, where negative β or OR < 1 implies a lower likelihood of the association. β = 0 or OR = 1 indicates no association between the two variables. Significance in the interaction term shows a significant moderating effect of level 2 independent variable on the association between level 1 independent and dependent variables.
Results
Over the 7-day period, participants completed an average of 36 of a possible 49 ESM surveys (M = 73.4%, SD = 16.0%, range = 34.7%–100.0%). The final sample included a total of 2768 surveys.
Time spent in real-life social interactions
Overall, participants spent 47.9% of their time “without social interactions,” followed by interacting with “family members” (13.5%). Specifically, the main people they interacted with were parents/grandparents (9.1%). Table 3 summarizes their time spent in social interactions.
ASD severity and caregiver stigma associated with real-life social interactions
MLA showed that participants with more severe ASD symptoms and those with caregivers who perceived higher levels of stigma were more likely than participants with milder ASD symptoms and those with caregivers who perceived less stigma to interact with “family members” (OR = 1.051, 1.025; 95% CI = 1.019–1.084, 1.008–1.043). There were no significant associations between ASD severity, stigma, and interactions with other social interaction partners.
Self-perceived experience associated with real-life social interactions
Figure 1 illustrates participants’ experiences in relation to interactions with different social interaction partners. Overall, participants were most interested in, and enjoyed interacting with, “friends.” They did not experience high levels of loneliness, regardless whether they were interacting with others or not. However, they experienced higher in-the-moment anxiety with “friends” and “people at school” compared with “family members.” Participants regarded “no interaction” as the least enjoyable and least interesting. When they were not engaged in social interactions, they preferred to be alone 43.3% of the time (SD = 35.5) but less frequently when interacting with “family members” (M = 24.2%, SD = 33.8), “friends” (M = 8.5%, SD = 23.8), or “people at school/work” (M = 5.9%, SD = 18.9).
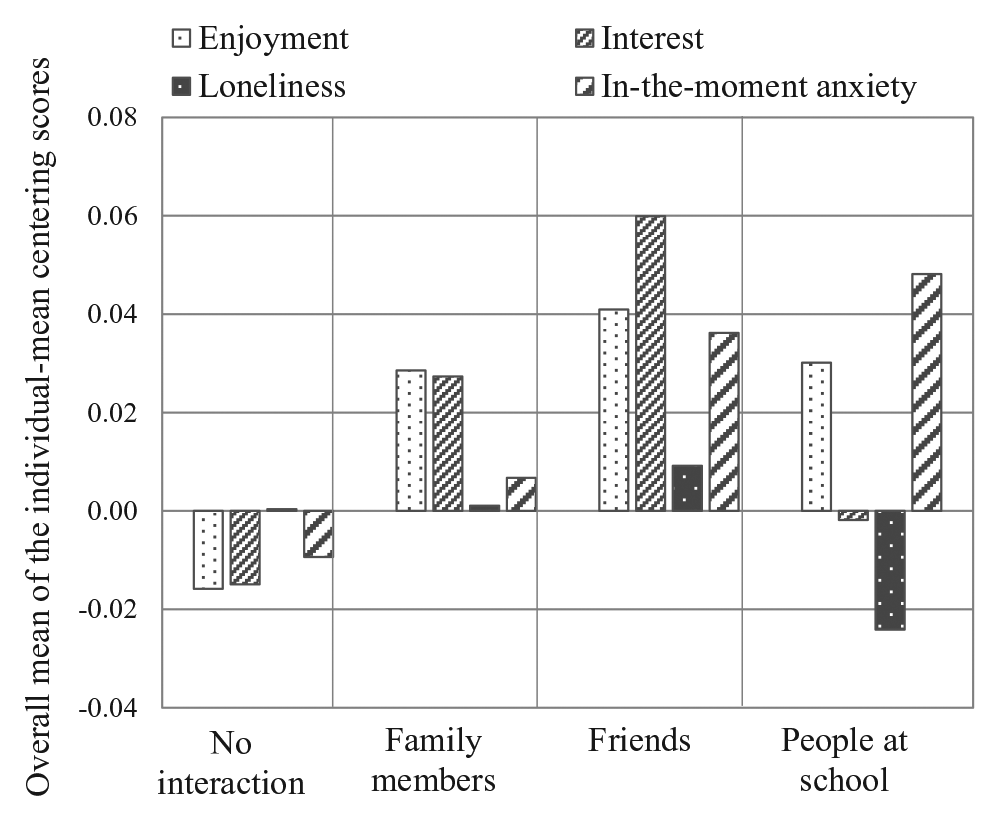
Perceived quality of social experiences in everyday social interactions.
Table 4 contains the results of the MLA on associations between participants’ self-perceived experiences and real-life social interactions. Compared with “no interaction,” interactions with “family members” and “friends” were associated with high levels of interests and enjoyment. Interactions with “people at school” were also associated with high levels of enjoyment. However, interactions with the three social interaction partners were associated with high levels of in-the-moment anxiety and a preference for not being alone as compared to “no interaction.” There were no significant associations between loneliness and interactions with different social interaction partners.
Results of multilevel analysis for perceived quality of social experiences in everyday interactions.

β: fixed regression coefficient; SE: standard error; OR: odds ratio; CI: confidence interval.
p < 0.05; **p < 0.01.
Moderating effects of caregiver stigma and ASD severity on social interaction experiences
Figures 2 and 3 illustrate the results of the MLA regarding the moderating effects of caregiver stigma and ASD severity (presented separately) on the associations between experiences and real-life social interactions. The moderating effect of stigma was only identified in the dependent variables of interest and in-the-moment anxiety (Figure 2). Specifically, participants with higher ASS scores had a weaker relationship than those with lower ASS scores between interest and interactions with “people at school” (β = −0.012, SE = 0.004, p < 0.01). That is, participants whose caregivers perceived higher levels of stigma were less likely than those whose caregivers perceived less stigma to be interested in interacting with people at school. Conversely, participants with higher ASS scores were more likely than those with lower ASS scores to perceive in-the-moment anxiety while interacting with “family members” (β = 0.004, SE = 0.002, p < 0.05).
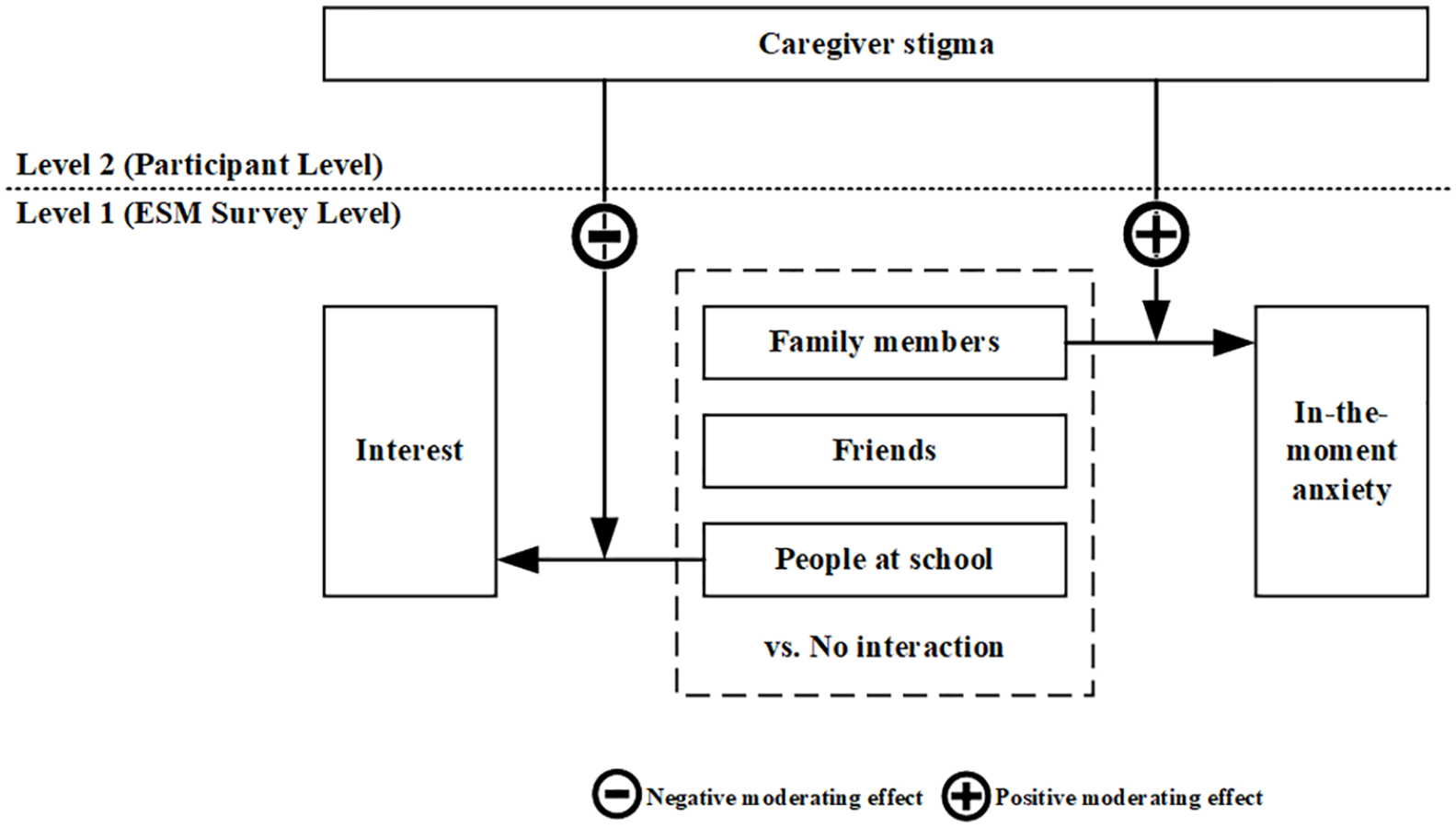
Illustration of moderating effect of caregiver stigma: interest and in-the-moment anxiety.
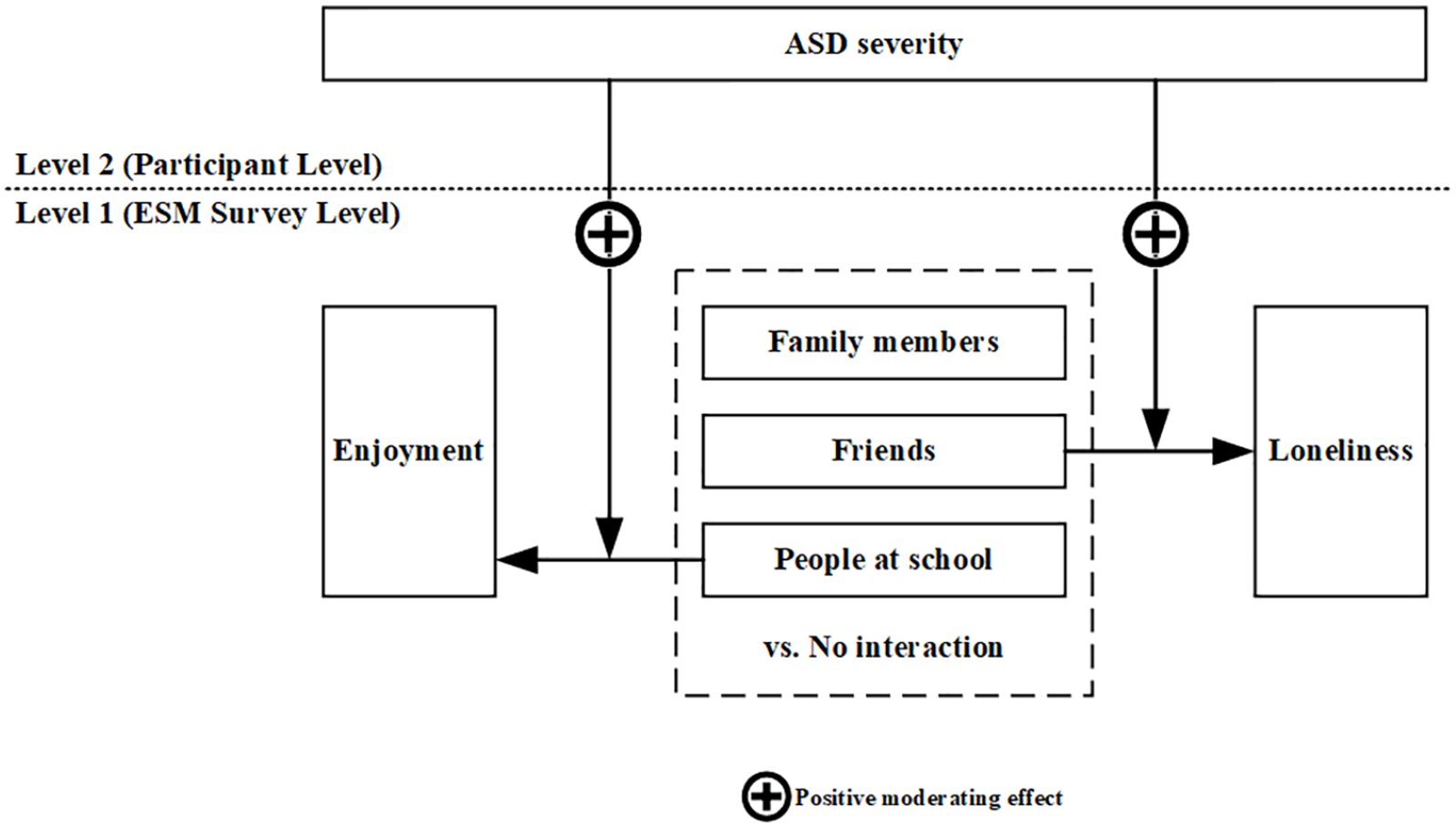
Illustration of moderating effect of ASD severity: enjoyment and loneliness.
The moderating effect of ASD severity was identified in the dependent variables of enjoyment and loneliness (Figure 3). Participants with more severe ASD were more likely than those with milder ASD to enjoy interacting with “people at school” (β = 0.013, SE = 0.005, p < 0.01) and feel lonely while interacting with “friends” (β = 0.011, SE = 0.004, p < 0.05).
Discussion
We investigated the impact of caregiver stigma on the real-life social experiences of Taiwanese adolescents with ASD who did not have ID. Adolescents reported enjoying their interactions; they did not prefer being alone when interacting with other people, providing evidence of their desires for social interaction (Chen et al., 2015; Müller et al., 2008). However, caregiver stigma was negatively associated with the adolescents’ time spent in social interactions and perceptions of social experiences. These findings support previous research indicating the diminished social experiences of individuals with ASD as a result of stigma (Kinnear et al., 2016; Ng et al., 2020). The results extend our understanding of the socioemotional lives of adolescents with ASD and the influence of severity of ASD symptoms played on social experiences.
One of the most unexpected findings was that the adolescents with greater caregiver stigma were more likely than those whose caregivers perceived less stigma to experience in-the-moment anxiety when interacting with family members. This finding contrasts with the role of family in supporting their child’s social needs (Guajardo et al., 2009). We postulate that the adolescents’ in-the-moment anxiety may be due to caregivers similarly experiencing anxiety in response to stigma, which has also been identified by previous researchers (Chan & Lam, 2017; Mak & Cheung, 2008). Furthermore, the belief that disability brings shame to a Chinese family (Lin et al., 2012) may have heightened caregiver stigma. That is, caregivers may seek to protect their child from negative views through close monitoring and restricting social interactions outside of home (Wood, 2006; Woodruff-Borden et al., 2002). Affrunti and Ginsburg (2012) suggested that caregivers’ protective behaviors may signal an insecure environment thus potentially increasing their child’s anxiety. Moreover, poorer parent–child relationships may develop as a result of parents’ emotional distress from being a caregiver of a child with a disability (Green, 2007).
Based on examination of expressed emotion, a quantitative measure of the criticism, hostility, and emotional overinvolvement expressed by one family member toward another (Leff & Vaugh, 1985), Griffith et al. (2015) have found that mothers were more critical and less warm toward their children with ASD than toward TD siblings. High levels of expressed emotion may lead to mental health problems in children and adolescents with ASD (Greenberg et al., 2006; Romero-Gonzalez et al., 2018). Bender and colleagues (2015) identified that an insecure parent–child attachment may be a risk factor for anxiety among adolescents. Our findings demonstrate the impact caregiver stigma may have on both parents and adolescents with ASD. Interventions, such as support groups aimed at improving caregivers’ management of stigma and their mental health, may build their resilience toward stigma and sense of inclusion within society (Chamak, 2008). This, in turn, may subsequently reduce the chance that their children develop anxiety while interacting with people outside the immediate family.
Reduced interest in interacting with people at school, in particular, with teachers and other peers, may be exacerbated by caregiver stigma. If caregivers withdraw from social interactions to cope with stigma (Mak & Cheung, 2008), they may distance themselves and their children from community activities (Lavesser & Berg, 2011; Mak & Cheung, 2008; Ng et al., 2020). Social isolation may subsequently limit their opportunities to support their children through challenges faced in the school environment. In fact, low levels of parental engagement in their children’s school has been found to be associated with increased bullying of children with ASD (Hebron & Humphrey, 2014). Negative social experiences may, in turn, diminish children’s interest in social interactions with people at school. Future research is needed to examine the impact of caregiver stigma on children’s social experiences at school. Nevertheless, this study highlights the need for developing caregivers’ coping strategies to manage stigma to support their child in social challenges. Increasing the school’s awareness, acceptance, and support toward students with ASD is also warranted.
In addition to the impact of stigma, participants with more severe ASD were more likely than those with fewer ASD symptoms to enjoy themselves when interacting with people at school. This finding is in line with previous research indicating that individuals with fewer ASD symptoms were less likely to engage in social participation (Chen et al., 2016, 2017; Sutton et al., 2005). As Sutton et al. (2005) found, individuals with fewer ASD symptoms may have heightened social awareness of their relationships and be more concerned about negative attitudes being directed toward them. With heightened awareness of their social difficulties and their peers’ negative social evaluations, these individuals may internalize the associated negative feelings (Crocker & Major, 1989), resulting in diminished self-esteem and less inclination to engage with peers. Thus, supporting adolescents with ASD, especially those with milder ASD symptoms, to develop a positive sense-of-self in social participation is critical. Equipping them with strategies to manage and counteract negative attitudes may be powerful for enhancing their quality of social experiences.
We found that adolescents with more severe ASD symptoms were more likely than those with less ASD symptoms to feel lonely when interacting with friends. Previous researchers (Bauminger et al., 2004; Bauminger & Kasari, 2000; Kasari et al., 2011; Locke et al., 2010) have found poor quality of friendship reported by children and adolescents with ASD compared with their TD peers. As those with severe ASD may present with more significant impairments in social communication skills, they may encounter greater challenges in social reciprocity in friendship (Bauminger et al., 2008; Kasari et al., 2011). When such experiences persist, they may contribute to low levels of satisfaction with social relationships, increasing their feeling of loneliness (Bauminger & Kasari, 2000; Locke et al., 2010).
In contrast to previous studies outlining high levels of loneliness among adolescents with ASD (Bauminger et al., 2004; Bauminger & Kasari, 2000; Locke et al., 2010), our participants did not report high levels of loneliness, even when alone. The discrepancy may be explained by differences in data collection approaches. In comparison with the retrospective approaches used in previous studies, we collected in-the-moment data that are less subject to recall bias (Hintzen et al., 2010; Shiffman et al., 2008). Our findings highlight the importance of collecting “in-the-moment” subjective experiences to gather contextually valid information about the individuals’ social experiences in real time.
Limitations
Several limitations of our study must be recognized. First, we utilized a cross-sectional design. We cannot assume causal relationships between caregiver stigma and the social experiences of adolescents with ASD. Future longitudinal studies are needed to establish causal relationships. Second, more males than females were involved as participants in our study. This ratio is consistent with the known higher male-to-female ratio of individuals with ASD (Loomes et al., 2017). However, literature has noted that females with ASD have higher levels of social communication skills (Head et al., 2014). Whether there is a gendered difference in social experiences and stigmatization requires further investigation. Third, approximately one-third of our participants presented with very mild ASD as reflected by low SCQ scores. This may be the result of interventions they had received previously to manage ASD symptoms. In Taiwan, children and adolescents frequently receive medical or clinical services as soon as they have a formal diagnosis. Further studies should investigate the impact of interventions on the social experience of adolescents with ASD. Fourth, we cannot generalize our findings to the total adolescent ASD population. We relied on findings from participants in Taiwan. Future studies of participants from different countries with Chinese cultural perspectives may help see how Chinese cultural characteristics influence the stigma and social experiences in the ASD population. Finally, whether adolescents with ASD who are intellectually disabled have more negative experience in social participation due to caregiver stigma is unknown. More robust sampling strategies, including those with ID, may be beneficial for future researchers to attain information about the ASD population in general. Moreover, while it has been insightful to explore caregiver stigma and children’s social experiences, to the authors’ knowledge, tools used by adolescents with ASD to measure their own perceived stigma has not been developed and/or validated. Future studies may also consider exploring the experiences of stigma experienced by the adolescents themselves to attain a wider lens of the implications of stigmatized experiences.
Conclusion
This study provides insight on the detrimental effects of caregiver stigma in restricting the quality of social experiences of adolescents with ASD. Our findings have implications for future practice. First, considering adolescents with ASD and their reduced opportunities for interacting with their peers, the implementation of support services, such as peer-support systems or teachers trained to support students with a disability, may be beneficial for adolescents with ASD for promoting social interactions. Second, practitioners should be aware of the impact of ASD severity, such that social awareness and self-esteem may play a role in lowering the quality of social experience for adolescents with fewer ASD symptoms. Interventions for adolescents with less severe ASD symptoms to promote self-confidence may thus be useful. Third, support for caregivers of adolescents with ASD in managing their own stigma is vital to improve both the caregivers’ wellbeing and adolescents’ social interactions.
Footnotes
Acknowledgements
The study was completed by V.H.T.L. as part of her BAppSc(OT) honors degree. The authors thank the people who participated in the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by the Partnership Collaboration Awards (The University of Sydney—National Taiwan University) and ECR/MCR Seeding Grant (Faculty of Health Sciences), The University of Sydney, Australia, and the Ministry of Science and Technology, Taiwan (MOST108-2410-H002-112-SS3).