
Abstract
To improve early detection of autism spectrum disorder in preventive care, a Dutch guideline was developed 5 years ago. The guideline provides preventive care physicians at well-baby clinics action-oriented advice and describes a step-by-step approach for children identified at an increased risk for autism spectrum disorder during general healthcare surveillance. This qualitative study evaluated the guideline adherence and studied barriers regarding early detection of autism spectrum disorder at well-baby clinics. Semi-structured interviews were undertaken with 12 preventive care physicians (one representative per province). Interviews were analyzed using grounded theory. It was found that the vast majority of participants did not follow-up general surveillance with an autism spectrum disorder–specific screener as prescribed by the guideline. Six barriers, to be divided in personal, guideline-related and external factors, were found regarding early detection of autism spectrum disorder and adherence to the guideline. The results of this study highlight the importance of an integrative approach, raising awareness of the benefits regarding early detection of autism spectrum disorder in preventive care, the need of continuous investment in easy and accessible training and active screening, and a closer collaboration between preventive care organizations and autism spectrum disorder experts.
Lay Abstract
To improve early detection of autism spectrum disorder in preventive care, a Dutch guideline was developed 5 years ago. The guideline provides preventive care physicians at well-baby clinics action-oriented advice and describes a step-by-step approach for children identified at an increased risk for autism spectrum disorder during general healthcare surveillance. The present qualitative study evaluated adherence to the guideline and studied barriers regarding early detection of autism spectrum disorder at well-baby clinics. Interviews were undertaken with 12 preventive care physicians (one representative per province). It was found that the vast majority of participants did not follow-up general surveillance with an autism spectrum disorder -specific screener as prescribed by the guideline. Six barriers (limited knowledge about autism spectrum disorder symptoms in infant and toddlerhood, professional attitude toward early detection, problems in discussing initial worries with parents, limited use of screening instruments, perceptions toward cultural and language differences and constraints regarding availability of healthcare services) were found. The results of this study highlight the importance of an integrative approach, raising awareness of the benefits regarding early detection of autism spectrum disorder in preventive care, the need of continuous investment in easy and accessible training and active screening, and a closer collaboration between preventive care organizations and autism spectrum disorder experts.
Autism spectrum disorders (ASD) affect about 1% of the population and are associated with lifelong impairments in functioning, substantial family burden, increased mortality, and high medical costs (Buescher et al., 2014; Elsabbagh et al., 2012). Over the past years, the importance of early detection and access to early intervention of ASD is widely recognized (French & Kennedy, 2018). Due to the dynamic and plastic nature of the brain, early interventions can alter the development in children with ASD. Early detection and intervention can increase social communication outcomes and can reduce comorbid problems, negative impact on families and lifetime costs to the individual, family, and society (Dawson et al., 2012; Fuller & Kaiser, 2020; Horlin et al., 2014). Despite these benefits, significant delays exist in access to screening, diagnosis and healthcare services for young children with ASD (Bishop-Fitzpatrick & Kind, 2017). Research has established that developmental abnormalities associated with ASD become evident in some children as early as 12 months (Jones et al., 2014) and that a reliable ASD diagnosis can be made before the age of 2 (Guthrie et al., 2013). Despite increasing awareness of the importance of early detection, in the Netherlands, the average age children with ASD are diagnosed is around 5 years (Begeer et al., 2017) and thus receiving access to appropriate intervention later than preferred.
In the Netherlands, about 15 years ago, a successful program known as the “DIANE Project” was implemented in order to improve early detection of ASD. In this program, physicians and nurses at well-baby clinics and members of special infant-toddler development teams were trained to (a) recognize early signs of autism and (b) use a specially designed referral protocol existing of a two-phase screening approach for ASD, which included a screening questionnaire, the CoSoS (Communication and Social development Signs, previously known as ESAT; Dietz et al., 2006) after concerns were raised during routine developmental screening. The strategies of the “DIANE Project” mainly led to an improvement of early detection of children with severe ASD (Oosterling, 2010). However, 8 years after the program ended, effects in early detection were not maintained in clinical practice (Pijl et al., 2017) and highlight the importance to continue studying improvement strategies for early detection of infants and toddlers at risk for ASD.
In order to improve early detection of ASD, a Dutch guideline was developed for use within preventive care (van Berckelaer-Onnes et al., 2015). In the Netherlands, all infants and toddlers are systematically observed at well-baby clinics during 13 visits between 0 and 4 years (program varies slightly per well-baby clinic). Well-baby clinics are a form of preventive healthcare where physicians and nurses have regular contact with young children and their parents, mostly for routine vaccinations, medical, and developmental screening. Preventive care physicians (PCPs) have an important surveillance role in the Dutch healthcare system and can therefore play a critical part in early detection, as well as guiding children to early interventions. The Dutch ASD guideline provides PCPs action-oriented advice in early detection and screening of ASD. It describes that the development of all children should be monitored by using a general tool for health surveillance, called the Van Wiechen Scheme (Laurent de Angulo et al., 2008). The Van Wiechen Scheme provides a template to monitor developmental milestones for children from birth to 4 years of age. The surveillance tool holds eight signals, considered to be first behavioral red flags of ASD in infants and toddlers (Dietz et al., 2006). When one or more behavioral red flags are identified during general surveillance with the Van Wiechen Scheme, the Dutch guideline urges PCPs to use an ASD-specific screener (CoSoS). Figure 1 provides a schematic representation of the guideline developed by van Berckelaer-Onnes et al. (2015). In the Netherlands, there is a general rule that national guidelines must be implemented in preventive healthcare organizations within 2 years after its introduction. To realize this, the organization that oversees guideline implementation carries out a standard protocol (Dunnink et al., 2016). Although it has been 5 years since the guideline was introduced and implemented by standard methods, until now, the current state of guideline adherence has not been investigated.
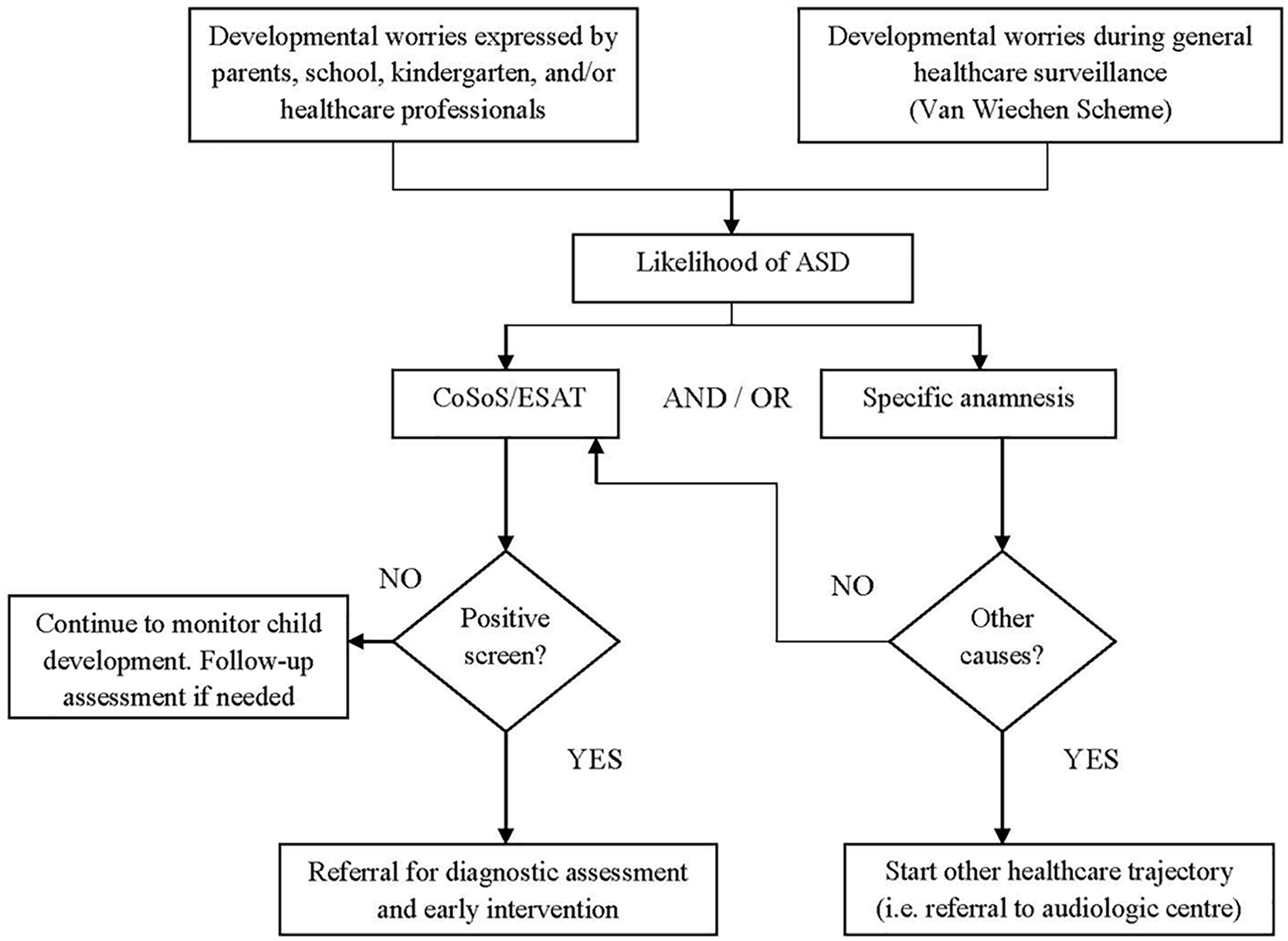
Representation of the Dutch national guideline on autism spectrum disorders by van Berckelaer-Onnes et al. (2015, translated).
Previous studies show that clinical screening guidelines are often not fully applied (Arunyanart et al., 2012; Fischer et al., 2016; Wallis et al., 2020). A systematic review that proposes a model to improve guideline implementation and adherence (Knowledge–Attitude–Behavior Framework; Fischer et al., 2016) distinguishes three factors regarding barriers of guideline implementation and adherence, covering (a) personal factors related to knowledge and attitudes, (b) guideline-related factors related to barriers linked to the process of developing a guideline (e.g. evidence of made recommendations and accessibility of a guideline), and (c) external factors related to barriers such as organizational constraints, lack of resources, and lack of collaboration (Fischer et al., 2016). In order to better understand already found barriers and develop improvement strategies, this framework can also be applied specifically related to early detection of ASD.
In relation to ASD, previous research showed that personal factors as barriers in early detection include providers’ insufficient training in child development, lack of knowledge about the early risk signals of ASD and unfamiliarity with screening instruments (Dosreis et al., 2006; Pinto-Martin et al., 2005). More recent studies among primary care providers in the United States underline these findings and suggested a need for training in recognizing red flags and familiarizing with ASD specific screening tools (Crais et al., 2014). A guideline-related factor in relation to early detection of ASD is the limited use of screening tools. In order to improve early detection, two screening strategies have been proposed: universal screening for ASD of all children at 18 and 24 months (American Academy of Pediatrics (AAP; Hyman et al., 2020) or global screening of children who have been identified as high-risk (Canadianaediatric Society, 2019; van Berckelaer-Onnes et al., 2015). Although choosing an effective screening strategy might be complicated, children are more likely to be identified and connected with early intervention services when developmental concerns are followed up by a screening tool (Barger et al., 2018). Therefore, the limited use of screening instruments despite scientific evidence can be viewed as an important barrier in early detection of ASD. Another, more practical, guideline-related barrier can be found in the usage of electronic systems. For example, when an ASD-specific screening tool is not incorporated within the electronic medical record, care providers do not get a push reminder, which then might influence care providers’ decision to screen (Fenikilé et al., 2015). External factors regarding obstacles in early detection of ASD previously found (a) are lack of time and acceptable compensation to apply screening instruments and (b) waiting lists. Since long waiting lists complicate early access to mental healthcare services (Crais et al., 2014; Dosreis et al., 2006; Pinto-Martin et al., 2005), it is possible that early identification of ASD can be viewed by some PCPs as less urgent and possibly harmful if no follow-up service is available after a screen positive result. In the Netherlands (specialized), mental healthcare centers and psychologist practices perform careful and extensive diagnostic assessments and are responsible for giving psychiatric diagnoses (among which ASD). Among others, waiting lists might indeed be one of the possible barriers regarding early detection of ASD in the Netherlands, but until now, it has been unclear to what extent possible barriers found elsewhere also apply to the Dutch situation of preventive healthcare.
Although there are high standards of primary and preventive healthcare and a great amount of scientific and clinical knowledge about (the importance of) early detection and intervention of ASD in the Netherlands, signals from the clinical field give the alarming impression that children at high risk of ASD are identified too late. Furthermore, there are clinical signs that the Dutch ASD guideline is not fully applied in PCPs’ daily work, although formal knowledge regarding guideline adherence is lacking. Therefore, the aim of this study is to gain insight into the experiences and perspectives of PCPs regarding early detection of ASD at well-baby clinics. Three specific questions will be addressed: (a) what are PCPs’ observations on the current state regarding adherence to the Dutch ASD guideline, (b) which barriers do PCPs face concerning detection, screening, and referral of young children with (symptoms of) ASD, and (c) which strategies are needed, in their view, to overcome these barriers and optimize preventive care?
Methods
Study design
This study was conducted by an institute for child and adolescent psychiatry in the Netherlands. A qualitative research design was used to explore the experiences and perspectives of PCPs regarding ASD-specific healthcare (detection, screening, and referral) for children aged 0–4 years. Following informed consent, PCPs were invited to complete an individual semi-structured in-depth interview. Based on a topic list, PCPs were invited to discuss their experiences regarding early detection of ASD at well-baby clinics and working in accordance with the national guideline. The focus was on barriers and recommended facilitators. Ethical approval was obtained from local institutional review boards (CMO Radboud University Medical Centre and Karakter Child and Adolescent Psychiatry University Centre, 2018-4318). The authors followed the Consolidated Criteria for Reporting Qualitative Research (COREQ; Tong et al., 2007; see Supplementary Table 1).
Recruitment of participants
Preventive healthcare organizations, 27 in total, spread across the 12 provinces of the Netherlands were contacted by phone or through email and were informed about the aim of the study. Regional differences in healthcare organizations can be quite sizable, hence the researchers’ intent to gain participation of one PCP per province. Organizations were requested to identify PCPs willing to participate. PCPs were provided with a fact sheet about the study and received an online registration form. A total of 28 PCPs registered. Purposive sampling was used to obtain a diverse sample reflecting a broad scope of experiences and views. In total, 12 physicians (one per province) were selected. As a sign of appreciation participants received a €40-gift card.
Development of measure
The topic list was developed in two phases. During the first phase (unpublished), data from another study were used. This is a study on the effect of a Live Online educational program (van ’t Hof et al., 2020), where PCPs in a specific area were asked to prepare three complex case studies related to early detection of ASD and difficulties with referral. In order to develop the topic list, case studies were analyzed using grounded theory (Glaser & Strauss, 2017). Six global preselected themes related to difficulties in early detection of ASD were constructed during analyses: (a) screening and detection of ASD symptoms, (b) therapeutic alliance, (c) cultural background, (d) multidisciplinary teamwork and referral, (e) stigma and parental acceptance, and (f) knowledge of red flag symptoms and diagnostics. Preselected themes were critically evaluated by the authors. Based on clinical experiences, two extra probe questions about peer feedback and knowledge about available healthcare services were added. These preselected themes were only used as a guide during interviews. During the second phase of developing the topic list, a concept was pilot tested during two interviews with physicians. No changes were made after pilot testing. The full topic list is available from the corresponding author.
Interviews and participants
In total, 12 PCPs working at well-baby clinics from 12 different provinces of the Netherlands were interviewed. All were native Dutch individuals. The majority (all but one) of the participants were female with an average of 9.04 years of work experience (ranging 0.5–30 years). Two physicians had only obtained their medical degree and had yet to specialize in child development, but the majority of participants was fully trained. Most interviews (10) were held through phone and video calls. Two interviews were held face-to-face in the researcher’s workplace, where there was no one else present besides the participant and researcher. Interviews were conducted by MS, a female PhD candidate with a background in behavioral psychology, who received training on qualitative research and interviewing. Prior to the interviews, the reasons for the interview were explained to all participants. Interviews took 40–60 min and were audio-recorded upon receiving verbal consent, to ensure accuracy in data capture. Each interview started with an open question to begin the conversation. Then the question, “could you please tell me how early detection of ASD is handled within your work?” followed. The conversation flowing from this question checked all global themes included in the topic list. When themes did not flow from the conversation, probe questions were asked. Data saturation was reached after nine interviews. However, the authors chose to complete interviews with all 12 participants, due to possible regional differences. No repeat interviews were carried out and no field notes were made. Data collection took place between June 2019 and September 2019.
Data analysis
Data analysis was concurrent with data collection. Audio recordings were transcribed verbatim, de-identified, and entered into Atlas Ti Qualitative Analysis Software by a master student experienced in transcribing audio recordings. Transcripts were not returned to participants for corrections. Transcripts were coded and analyzed using grounded theory and included a systematic set of phases of open coding, axial coding, and selective coding, respectively (Corbin & Strauss, 2008; Glaser & Strauss, 2017). Participant’s quotes were hereby the starting point in constructing themes and categories, meaning a bottom-up approach. In the open coding phase, transcripts were analyzed by identifying and categorizing common segments found in the data. These segments were labeled and compared continuously with each other. During the process of axial coding, the data segments were reassembled into categories. During the last phase of selective coding, categories were compared with each other and then the themes were constructed. M.S. and S.K. coded the majority of interviews together. S.K. is a researcher experienced in qualitative research and methodology. Through discussion and agreement over discrepancies, consensus was reached.
Community involvement
The autism community was not involved during this study.
Results
Current state of adherence to the Dutch guideline
All participants were asked whether their healthcare organizations fully applied the national ASD guideline. Guideline adherence means (a) using the Van Wiechen Scheme for general surveillance and (b) using the CoSoS (ESAT) as a specific screener when red flags for ASD were found. In total, all PCPs mentioned that they use the Van Wiechen Scheme for general health surveillance. However, the vast majority of PCPs stated that, in case of suspicion, they do not follow-up with the CoSoS as a specific screen for ASD. This practice is not in accordance with the guideline and is perceived as a barrier in early detection of ASD.
Barriers in early detection of ASD and adherence to the Dutch ASD guideline
Six overall barriers in early detection of infants and toddlers with (symptoms of) ASD faced by PCPs were extracted from the data. These themes can be summarized by knowledge, professional attitude, discussing initial worries with parents, screening instruments, perceptions regarding cultural and language differences, and availability of healthcare services. A description of each theme is given below. Representative quotes are presented in Table 1.
Themes (selective codes) and categories (axial codes) representing barriers, accompanied by illustrative quotes.

Knowledge about ASD
Limited knowledge of ASD in infants and toddlers was the first theme constructed. There seems to be a variation among PCPs’ knowledge of the early signs of ASD. PCPs with less work experience express their difficulties and insecurities in recognizing the early red flags of ASD, and seem often not to be aware of the fact that symptoms can already be evident in infants and toddlers. More experienced PCPs often report a higher degree of confidence in their knowledge in recognizing early risk signals of ASD. The majority of them mention their professional intuition when it comes to early detection of ASD.
Professional attitude
The second theme was PCPs’ professional attitude which covered (a) feelings of competence and (b) beliefs about the importance of early detection.
Feelings of competence
Some PCPs feel that they are not capable enough to recognize signs of ASD, due to their educational background and/or due to the limited time they have to examine a child. PCPs with less work experience and knowledge of the subject seem to be less confident in signaling high risk children than PCPs with more experience and knowledge. One PCP insinuated a need for peer feedback.
Beliefs about the importance of early detection
A couple of PCPs wondered whether or not it is important to identify children with possible ASD before the age of 4. PCPs who are aware of the benefits of early detection and intervention seem more likely to screen children early and discuss concerns with parents. However, some PCPs are unaware of the importance of early detection and only screen when problems have accumulated.
Discussing initial worries with parents
Discussing initial worries with parents can be divided into (a) discrepancies in worries between PCPs and parents and (b) parental recognition and perspective on diagnosis and healthcare.
Discrepancies in worries between PCPs and parents
Almost all PCPs noted that they find it difficult to express their concerns regarding ASD and motivate parents for diagnostic assessment when there are discrepancies in worries between PCPs and parents. Since parents are essential partners when proceeding referral, PCPs often choose a different strategy: they choose to express their worries about the child’s delayed language development and refer for an audiology assessment, instead of discussing their concerns about ASD and refer to a specialized mental healthcare service.
Parental recognition and perspective on diagnosis and healthcare
PCPs often describe that parents find it difficult to recognize and accept that their child’s development is compromised. Furthermore, PCPs mention parental perspective on diagnosis and healthcare: parents sometimes do not want a diagnosis for their child at such a young age, because of stigma.
Screening instruments
Notably, a minority of PCPs used an ASD-specific screener (CoSoS) when developmental worries occurred based during general surveillance. This theme covers obstacles mentioned by PCPs in the use of an ASD-specific screener.
Unfamiliarity with ASD specific screening tools
The majority of the PCPs is unfamiliar with the CoSoS. First, PCPs mentioned that they are often unaware that an ASD-specific screener is recommended (as in the guideline) when concerns are raised during general surveillance. Second, PCPs mentioned that they find the purpose of the CoSoS unclear, and that they do not know how and when to use it. For example, one PCP (mistakenly) thought that the CoSoS was part of diagnostic assessment.
Time constraints
Another obstacle in the use of screening instruments mentioned by PCPs is time constraints. Within preventive care, the use of multiple national guidelines and screening instruments are prescribed for a range of developmental and medical problems. However, due to limited time and subsequent work pressure, PCPs feel that they cannot implement guidelines in full manner.
Parental acceptance
Furthermore, PCPs are afraid that it will jolt and intimidate parents when they introduce a screening list (CoSoS) that specifically targets possible ASD.
Perceptions regarding cultural and language differences
All PCPs noted the importance of understanding and taking into account families’ cultural background, customs, parental beliefs and language. Some PCPs expressed their concerns that cultural differences make it more difficult to discuss developmental problems and suspicion of ASD. For example, one PCP expressed her thoughts about parents not truthfully telling how things are at home. Another PCP said she had the idea that parents found it more difficult to accept that there could be something going on with the child, and that parents were less likely to express concerns and ask for help. Language barriers could also contribute to poor detection of ASD, but all PCPs may contact a translator. Opinions of this service varied among PCPs. Most of them were glad to be able to communicate in the families’ language. One PCP, however, expressed her doubts regarding sharing personal information with an external party.
Availability of healthcare services
Finally, PCPs are worried about the availability of healthcare services. Waiting lists for (special) healthcare services such as audiologic centers and child psychiatry centers are often months long. Another obstacle regarding the availability of healthcare services is that the provision of healthcare is subject to the financial rules of the market. In the Netherlands, healthcare is purchased by municipalities. Because of this, the offer of healthcare services differs greatly per region. Some regions have more healthcare services available for young children with/at risk for ASD then others. One PCP who worked in a region with a restricted offer of healthcare services mentioned that she missed the ability to refer children to easy and accessible healthcare, for example, an infant team.
Strategies needed to optimize early detection of ASD in preventive care
Participants were also asked which strategies are needed to optimize early detection of ASD at well-baby clinics. Two themes were extracted from data analysis: training needs and closer collaboration between healthcare organizations. Representative quotes are presented in Table 2.
Selective codes representing strategies, accompanied by illustrative quotes.

Training needs
Most PCPs stated their need for additional training in recognizing the importance of early detection of ASD, what early risk signals are, and how to administer the CoSoS. One PCP suggests that training in motivational interviewing could possibly help in discussing concerns with parents. In addition, PCPs recommend extra training not only for themselves, but also for their colleagues and collaboration partners in preschool and kindergarten.
Closer collaboration between healthcare organizations
The majority of PCPs emphasized a closer collaboration between preventive care and more specialized healthcare centers as a strategy to improve early detection of ASD. PCPs who worked in an organization where there is a close collaboration between healthcare organizations expressed more confidence in identifying young at risk children. When asked what a good collaboration would look like, almost all PCPs agreed upon the following: receiving a confirmation after a child is referred, receiving a sign when diagnostic assessment or treatment has started, receiving a letter or report when treatment has ended and more consultation between different healthcare professionals.
Discussion
The findings in this study indicated the lack of guideline adherence 5 years after implementation. Second, PCPs revealed the following barriers in the early detection of ASD: (a) limited knowledge about ASD symptoms in infant-and toddlerhood, (b) professional attitude toward early detection, (c) problems in discussing initial worries with parents, (d) limited use of screening instruments, (e) perceptions regarding cultural and language differences, and (f) constraints regarding availability of healthcare services. To improve early identification of ASD, PCPs mention the need for additional training in recognizing the importance of early detection, recognizing early risk signals and how to administer the CoSoS as an ASD-specific screener. Furthermore, PCPs suggest that there should be a closer collaboration between healthcare organizations. The main findings will be discussed below.
State of adherence to the Dutch guideline
The Dutch ASD guideline is developed only partly in line with the leading guideline of the American Academy of Pediatrics AAP; Hyman et al., 2020. The AAP guideline alike, the Dutch guideline emphasizes systematically following child development during infancy and toddlerhood. Unlike the AAP recommendation that prescribes pediatricians to screen for ASD at 18 and 24 months in all children (i.e. universal screening), the Dutch guideline prescribes preventive healthcare physicians to screen for ASD when one or more red flags for ASD are identified during general health surveillance (i.e. screening in high risk groups) (van Berckelaer-Onnes et al., 2015). The reasons for this strategy include feasibility and current insufficient evidence to assess universal screening of ASD in all children (Siu & US Preventive Services Task Force, 2016). It appears, however, that whichever screening strategy is chosen, guideline adherence is suboptimal, for example, despite AAP guideline recommendations regarding universal screening, research estimates that little more than half of pediatricians conduct routine screening for ASD at 18 or 24 months (Arunyanart et al., 2012). This corresponds with our finding that the majority of respondents do not follow the Dutch guideline’s advice.
Barriers of early detection and adherence to the guideline
Six barriers of early detection of ASD and guideline adherence were revealed. In general, factors regarding barriers of guideline implementation and adherence can be divided into (a) personal factors, (b) guideline-related factors, and (c) external factors (Fischer et al., 2016). The current findings will be discussed within this framework. Naturally, factors do not stand alone but are interrelated and affect each other.
Most barriers to early detection and guideline adherence are related to personal factors and include limited knowledge, professional attitude toward early detection, difficulty in discussing initial worries with parents, and complications derived from cultural differences and language difficulties. Especially early on in their career, PCPs seem to have a limited knowledge about ASD symptoms in infant and toddlerhood, are not aware of the importance of early identification (and subsequently the benefits of early intervention), and experience feelings of incompetence. This finding is often cited as a barrier in early detection of ASD in previous research, and is frequently recommended to target by offering additional training (Bright et al., 2019; Fenikilé et al., 2015; Mazurek et al., 2020; Pinto-Martin et al., 2005). Based on the Knowledge–Attitude–Behavior Framework, knowledge influences personal attitudes and attitudes will subsequently influence behavior (Fischer et al., 2016). Therefore, improving knowledge about ASD symptoms (as the first personal barrier) in infant and toddlerhood can be considered as a fundamental target in improving early detection of ASD, which in turn can influence professional attitude (as the second personal barrier) toward early detection.
The third personal barrier covers the field of discussing initial worries with parents. PCPs find it difficult to discuss the possibility of the child having ASD when parents do not express any concerns. Furthermore, PCPs describe that parents find it difficult to recognize and accept that their child’s development is compromised. Since early interventions are being advised to start as quickly as possible (Zwaigenbaum et al., 2015), there is an increased possibility that parents are being confronted with their child’s disability even before they share concerns on their own initiatives. However, the statement made by PCPs in this study (that parents find it difficult to recognize and accept that their child’s development is different) is noteworthy. Previous studies conducted among parents of children with ASD suggest that parents are often the first ones to express concerns. They often start having concerns about their child’s development during the first 2 years of life (Landa et al., 2008; Zwaigenbaum et al., 2015). Despite initial worries expressed by parents, they are often met with a “wait and see” approach (Chao et al., 2018; Crane et al., 2016). So, while from the professional perspective discussing initial worries might be difficult, from a parent perspective, initial concerns are often dismissed by a PCP. However, who first raises concerns is not the main question. Instead, we must focus on how to ease parent–professional conversations regarding the early identification of ASD. Strategies to narrow the gap between parents’ and professionals’ perspectives could be additional training for PCPs in motivational interviewing and active listening strategies (Locke et al., 2020), and making use of a specific screening tool (as prescribed by the guideline, and further discussed below). However, in order to better understand and ease PCP–parent conversations, additional research is needed that investigates parents’ experiences with the early identification process and integrates their perspective with PCP’s point of view.
The last personal barrier is related to perceptions regarding cultural and language differences. According to PCPs, having a different cultural background and speaking a different language can make it more difficult for parents to discuss initial concerns with a professional. In addition, PCPs might experience more difficulties in discussing initial concerns of ASD. This barrier is in line with previous studies (Crais et al., 2014; Zuckerman et al., 2013), its existence shining through the results of previous studies focusing on ASD in minority groups. For example, it was found that minority families are less likely to contact a healthcare professional about their concerns, are more distrusting of the healthcare system and that their children are being diagnosed at a later age (Burkett et al., 2015; Zeleke et al., 2019). Therefore, it is essential for PCPs to be better culturally informed and take differences in mind when discussing ASD with families who have other cultural backgrounds. Also, it is of great importance that the there is an increased awareness on the risk of preconceptions on cultural and language differences in the process of early identification of ASD. Most desirable would be a broader cultural representation among PCPs. Other, more practical, improvement strategies include adapting screening instruments by translating them and make these translated versions widely available or, as with the M-CHAT, to add follow-up questions to make sure families understand the questions that are being asked (Crais et al., 2014).
A guideline-related barrier is the limited use of screening instruments in preventive care, despite scientific recommendations. Research reports that a specific screening tool can identify more children with ASD than either clinical judgment or parental reports (Miller et al., 2011) and early detection is most effective when developmental concerns are in tandem with a follow-up-specific screener (Barger et al., 2018). PCPs mentioned unfamiliarity with screening instruments, parental acceptance, and time constraints as important obstacles in the use of a screening tool. The first two obstacles are interwoven with previously described personal barriers, that is, limited knowledge and difficulty discussing initial worries with parents. Possible solutions can, as aforementioned, be training in recognizing red flags of ASD in infant and toddlerhood and motivational interviewing on how to discuss initial worries with parents without immediately deliberating an ASD diagnosis. The obstacle of time constraint has also previously been found as a barrier in early identification and can be explained by the increasing workload in preventive healthcare, since numerous different guidelines are expected to be followed (Yarnell & Polla, 2003). As an extension of the time constraints, adequate reimbursement is often not available. Without adequate reimbursement (in the form of additional training, and more time and human resources), PCPs who already feel time pressure in their daily work are unlikely to integrate a screening tool or any additional services (Dobrez et al., 2001; Pinto-Martin et al., 2005). However, research suggests that a timely investment in early detection of ASD and access to early intervention can ultimately reduce both family and society costs. For example, toddlers who had received early intervention benefited from functional gains (Dawson, 2008), but they also needed fewer services (Cidav et al., 2017). Both benefits result in overall cost savings, indicating that early intervention (and therefore early detection) has the potential to reduce costs in the long term (Cidav et al., 2017; Horlin et al., 2014; Peters-Scheffer et al., 2012), seeming worth the time and cost investment by policymakers and municipalities.
The final barrier, an external factor, in early detection of ASD and adherence to the guideline is availability of healthcare services to refer to once children are identified as being at risk. PCPs mentioned that there is no easy access available to healthcare services, due to long waiting lists or limited offer. This is alarming, since it is expected that early detection leads to improved outcomes, as a result of an early referral to adequate treatment (Zwaigenbaum et al., 2019; Zwaigenbaum & Maguire, 2019). In addition, screening at an early age (<24 months) is also likely to identify other developmental delays and disorders than ASD (Chlebowski et al., 2013) that require early and appropriate intervention. Overall, improvement in the accessibility and availability of healthcare services is a priority and will be further addressed in the section below.
Proposed improvement strategies by PCPs
In order to reach guideline adherence and overcome barriers, PCPs express their need of (a) knowledge about the content and subject of the guideline and (b) closer collaboration between healthcare organizations. Additional training in order to improve PCPs’ knowledge and professional attitude is highly likely to enhance the overall quality of care for children at risk of ASD and is therefore frequently recommended in this study and in previous studies (Fenikilé et al., 2015; Mazurek et al., 2020; Pinto-Martin et al., 2005). Indeed, availability of easy access information about ASD in infants and toddlers has increased in recent years. Examples are the development of new and accessible state-of-the-art websites, online learning modules, and the ‘Learn the Signs: Act Early” initiative by the Centers for Disease Control and Prevention. Specifically for the Dutch guideline, additional training has been provided to PCP and an accessible website has been developed for healthcare professionals and parents. Thus, there has already been an increased offer and availability of additional training and information. Therefore, we argue that the need for additional training does not come from a lack of information resources, but due to insufficient compensation leading to the absence of active investment. In order to uphold positive effects of additional training, previous research has established that active investment and maintenance are demanded (Pijl et al., 2017). In order to fulfill PCPs’ needs for additional training, improve early detection of ASD, and obtain guideline adherence, the importance of early detection of ASD should be brought to the attention of policymakers (i.e. governments/municipalities) and preventive care organizations, as reimbursement (in the form of additional training, more time and sufficient human resources) of these activities are an important condition.
A second strategy to improve early detection of ASD and guideline adherence is a closer collaboration between healthcare organizations. Recognizing this, Dutch researchers and clinicians formed a national, interdisciplinary network with the goal of exchanging knowledge and translating scientific results into tools for the clinical field. As an example, this network is currently developing and studying a new and innovative intervention program, called the BEAR parent training for young children at risk of ASD. The program demonstrates a close collaboration between preventive healthcare and specialized mental healthcare, as the intervention is carried out by a preventive healthcare professional and supervised by an ASD expert. Through this collaboration, preventive care is able to offer a short and semi-specialized intervention for young children at risk of ASD, without the need of referral to the specialized mental healthcare and without the need of a diagnosis. Therefore, these kinds of close collaborations are hypothesized to improve the accessibility and availability of healthcare and improve early detection of ASD.
Strengths and limitations
To capture the full range of experiences of PCPs about early detection of ASD, one representative per geographical region of the Netherlands was included and extra interviews were conducted after data saturation was reached. Therefore, the study’s results may represent the views of a larger PCP community in the Netherlands. However, participants only shared their own experiences and did not speak for their colleagues. PCPs volunteered to participate in this study, indicating their interest in screening for ASD. Thus, it is possible that there might have been a self-selection bias. Therefore, the results might not be representative for all PCPs. Next, this study was conducted in the healthcare system of The Netherlands and should therefore be viewed in this context. However, our results show a great overlap with the results of similar studies in other countries, suggesting barriers regarding early detection of ASD to be shared, at least in Western countries. Third, only physicians participated in this study and no other preventive care professionals (i.e. nurses). To completely understand barriers and views about early detection of ASD in primary care, further studies could explore the experiences and perspectives of a wider range of primary care providers. Finally, a characteristic of qualitative research is that data analysis entails coding and categorization in themes, which involves interpretation of the researchers. To limit subjectivity, the analytic process was done by multiple researchers with different educational backgrounds and extensive discussions regarding coding and developing themes were held.
Conclusion and clinical implications
In conclusion, there is no full adherence to the Dutch guideline. Based on a qualitative approach, we provide a theory about guideline-related external and personal constraints that limit PCPs’ use of the Dutch ASD guideline, and what prevents them to discuss developmental concerns and the suspicion of ASD with parents. Targeting these barriers demands a national and integrative approach and requires a close collaboration between preventive healthcare workers and ASD experts. Innovative ideas (e.g. BEAR parent training) regarding this subject are momentarily being developed and thoroughly examined. Furthermore, it is vital that the importance and benefits of early detection of ASD is brought to the attention of policymakers, governments, and municipalities. In order to improve early detection of ASD in preventive care and reach and preserve guideline adherence, continuous investment in active screening and additional training in preventive care is demanded.
Supplemental Material
sj-docx-1-aut-10.1177_13623613211009345 – Supplemental material for Early detection of young children at risk of autism spectrum disorder at well-baby clinics in the Netherlands: Perspectives of preventive care physicians
Supplemental material, sj-docx-1-aut-10.1177_13623613211009345 for Early detection of young children at risk of autism spectrum disorder at well-baby clinics in the Netherlands: Perspectives of preventive care physicians by Michelle IJ Snijder, Shireen PT Kaijadoe, Maarten van ‘t Hof, Wietske A Ester, Jan K Buitelaar and Iris J Oosterling in Autism
Footnotes
Acknowledgements
The authors thank the preventive care physicians for their time and effort in taking part in this study. Furthermore, they are grateful for the help of Prof. Dr Ina van Berckelaer-Onnes, who answered all of the authors’ questions and helped in gaining insight in the writing and implementation history of the Dutch ASD guideline.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.K.B. has been in the past 3 years a consultant to/member of advisory board of/and/or speaker for Takeda/Shire, Roche, Medice, Angelini, Janssen, and Servier. He is not an employee of any of these companies, and not a stock shareholder of any of these companies. He has no other financial or material support, including expert testimony, patents, and royalties.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korckzak Foundation (Grant No. 2018-01) and was further supported by (1) the EU-AIMS (European Autism Interventions) and AIMS-2-TRIALS Programmes which receive support from Innovative Medicines Initiative Joint Undertaking Grant Nos 115300 and 777394, the resources of which are composed of financial contributions from the European Union’s FP7 and Horizon2020 Programmes, and from the European Federation of Pharmaceutical Industries and Associations (EFPIA) companies’ in-kind contributions, and AUTISM SPEAKS, Autistica and SFARI and (2) the EU Horizon2020 Programme CANDY (Grant No. 847818).
Informed consent
Informed consent and consent for publication was obtained (both verbal and written) from all participants.
Supplemental material
Supplemental material for this article is available online.