
Abstract
Autism spectrum disorder is a neurodevelopmental condition characterized by social communication difficulties and restricted, repetitive behaviors. Autism spectrum disorder is highly co-morbid with other neuro-psychiatric disorders such as attention deficit hyperactivity disorder, anxiety, and depression. However, research on post-traumatic stress disorder among individuals with autism spectrum disorder is scarce. Furthermore, the understanding of shared mechanisms underlying autism spectrum disorder co-morbidity with other conditions may assist in both diagnostic and intervention efforts with affected individuals. This short report examined the role of brooding and reflective rumination as mediators between autism spectrum disorder and post-traumatic stress disorder. A total of 34 adults with autism spectrum disorder (with no intellectual impairment) and 66 typically developing controls, comparable on age and gender, filled out the PTSD Checklist for DSM-5 and the Rumination Response Scale. The results indicated increased post-traumatic stress disorder symptoms, as well as elevated brooding levels, in adults with autism spectrum disorder, compared to typically developing controls. Brooding, but not reflective rumination, mediated the association between autism spectrum disorder and post-traumatic stress disorder symptoms. Rumination and cognitive inflexibility, which are common in autism spectrum disorder, may exacerbate post-traumatic symptoms among traumatized individuals who have autism spectrum disorder. Interventions targeting brooding rumination and cognitive flexibility may assist in alleviating post-traumatic symptoms in individuals with autism spectrum disorder. Future studies should examine other psychological mechanisms which may underlie the autism spectrum disorder–post-traumatic stress disorder co-morbidity.
Lay abstract
Autism spectrum disorder is a neurodevelopmental condition characterized by social communication difficulties and restricted repetitive behaviors. Individuals with autism spectrum disorder are often diagnosed with other psychiatric conditions, including attention deficit hyperactivity disorder, anxiety, and depression. However, research on post-traumatic stress disorder among individuals with autism spectrum disorder is scarce. Nonetheless, studies have shown that those with autism spectrum disorder may face an increased risk of exposure to traumatic events. Separate lines of research in autism spectrum disorder and post-traumatic stress disorder have shown that the two may share several vulnerability factors. One of those is ruminative thinking, that is, one’s tendency to re-hash thoughts and ideas, in a repetitive manner. This article examined the role of two rumination types as potential factors connecting autism spectrum disorder and post-traumatic stress disorder: brooding (continuously comparing one’s current condition to one’s desired condition) and reflection (an introspective effort to cognitively solve one’s problems). A total of 34 adults with autism spectrum disorder (with no intellectual impairment) and 66 typically developing adults completed questionnaires assessing post-traumatic stress disorder symptoms and rumination. The results showed increased post-traumatic stress disorder symptoms in adults with autism spectrum disorder, compared to typically developing adults. Brooding rumination was also higher among those with autism spectrum disorder. Finally, brooding, but not reflection, served as a mechanism connecting autism spectrum disorder and post-traumatic stress disorder, that is, those with autism spectrum disorder showed increased brooding, which in turn predicted more post-traumatic stress disorder symptoms. This study has potential clinical implications. Rumination and cognitive inflexibility, which are common in autism spectrum disorder, could exacerbate post-traumatic symptoms among individuals with autism spectrum disorder who experience traumatic events. Interventions targeting brooding rumination and cognitive flexibility may assist in alleviating post-traumatic symptoms in individuals with autism spectrum disorder.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by social communication difficulties, restricted repetitive behavior patterns, and altered sensory experiences (American Psychiatric Association, 2013). Individuals with ASD are often diagnosed with other neuro-psychiatric disorders as well, including attention deficit hyperactivity disorder (ADHD), anxiety, and depression (Lord et al., 2018). However, knowledge about the co-occurrence of ASD and post-traumatic stress disorder (PTSD) has so far been limited.
PTSD is a common chronic stress disorder resulting from exposure to traumatic events. It includes four symptom clusters: intrusive thoughts and re-experiencing of the trauma; cognitive and behavioral avoidance of traumatic reminders; negative alterations in cognition and mood; and increased hyper-arousal (American Psychiatric Association, 2013). Studies showed that individuals with ASD may face an increased risk of experiencing traumatic events (Kerns et al., 2015), and that the incidence of PTSD among those with ASD may be significantly higher compared to typically developing (TD) individuals (Haruvi-Lamdan et al., 2020; Rumball et al., 2021). The comorbidity between ASD and PTSD is an evolving field in research and practice (Kerns et al., 2020; Kildahl et al., 2019; Rumball et al., 2020). However, very little is known about psychological mechanisms underlying PTSD-ASD co-morbidity. Clinically, these disorders share several vulnerability factors, including compromised social cognition, impaired emotion regulation, and alterations in autobiographical memory (Haruvi-Lamdan et al., 2018). The current study examined the role of rumination in PTSD-ASD co-morbidity.
According to Nolen-Hoeksema’s (1991) well-accepted Response Styles Theory, rumination refers to repetitively thinking about the cause, consequences, and symptoms of one’s negative affect. The theory argues that there are inter-personal differences in people’s characteristic response patterns to negative mood. These patterns subsequently have an effect on the course and intensity of this mood. rumination refers to repetitively thinking about the cause, consequences, and symptoms of one’s negative affect. Nolen-Hoeksema and colleagues (2008) indicated that there is a positive association between a ruminative response style and increased negative emotions, decreased goal-directed activity, and burnout in inter-personal relationships. Rumination is typically considered as a dysfunctional emotion regulation strategy, which individuals employ in an inflexible manner. In line with Response Styles Theory, rumination was commonly associated with psychopathology, including depression and obsessive-compulsive disorder (Aldao et al., 2016). In recent years, the study of rumination was enriched by categorizing it into two sub-types: (1) brooding (continuously comparing one’s current condition to one’s desired condition) and (2) reflection (an introspective effort to cognitively solve one’s problems), with research showing the adverse effects of the former, and the positive effects of the latter (Wu et al., 2015). Repetition, which is a central component of rumination, is a defining aspect of ASD. Indeed, increased rumination was found among individuals with ASD (Gotham et al., 2014). Rumination is also associated with PTSD, with longitudinal studies showing that the endorsement of rumination shortly after a traumatic event serves as a predictor of later PTSD (Kleim et al., 2007). Both intrusions and rumination are quite common in individuals suffering from chronic PTSD (e.g. Michael et al., 2007; Williams & Moulds, 2007). An increased tendency for rumination may both facilitate the development of post-traumatic cognitions, as well as maintain them once they have developed. This may be particularly true for brooding rumination, which was found to be associated with symptoms of post-traumatic re-experiencing. As noted by Valdez and Lilly (2017), “Passively thinking about the causes and consequences of trauma can provide internal retrieval cues for intrusive trauma memories that can elicit further rumination” (p. 12). This notion also echoes Ehlers and Clark’s (2000) cognitive model of PTSD, which highlights the bidirectional association and mutual maintenance between re-experiencing and rumination. Interestingly, when looking at reflection rumination separately, this cognitive pattern was found to be associated with post-traumatic growth (PTG), which is considered a salutogenic outcome of trauma exposure (Stockton et al., 2011).
To date, rumination was hardly assessed as a possible underlying mechanism connecting ASD and PTSD. A recent study by Rumball et al. (2021) has examined the role of rumination in various mental health symptoms including PTSD, among autistic adults, though their examination did not include a TD control group. We compared rumination and PTSD symptoms between autistic and TD adults and hypothesized that (1) participants with ASD will show more PTSD symptoms, more brooding- and less reflection-rumination, compared to TD participants; (2) increased brooding and decreased reflection will mediate the association between ASD and PTSD symptoms.
Methods
Participants and procedure
The study included 100 participants comprising two groups: (1) 34 adults (41.2% female, age: M = 23.29, SD = 5.70) with ASD and no intellectual impairment (verified using WAIS vocabulary and similarities subtests). The research team reviewed the Israeli Ministry of Welfare or National Insurance Institute’s confirmation of participants’ ASD diagnosis. Confirmation is based on a DSM diagnosis given by a psychiatrist and/or a clinical psychologist; (2) 66 adults with TD (43.9% female, age: M = 23.02, SD = 3.10), who were screened-out for ASD using the Autism-Spectrum Quotient (AQ).
Participants of both groups were invited to take part in a life events study, using advertisements placed in students’ (TD group) and autism (ASD group) forums in social networks. Individuals with ASD were also recruited through non-government organizations (NGOs), operating employment, academic, and recreational programs for adults with ASD. Inclusion criteria for both groups were age of 18 and above, and Hebrew as a native tongue. Eligibility to participate was assessed via a telephone interview. Participants then met a member of the research team to provide written informed consent and to complete the research measures. They were compensated for their time. The study was approved by the Institutional Review Board of Bar-Ilan University. Data collection was completed prior to the COVID-19 pandemic outbreak.
Groups were comparable on age (t(43.60) = 0.26, n.s.) and gender (χ2(1) = 0.07, n.s.) and significantly differed on total AQ scores (ASD: M = 28.21, SD = 7.66; TD: M = 15.29, SD = 5.16; t(48.84) = 8.85, p < 0.001). Among the ASD and TD groups, respectively, the majority of participants reported their household to have at least average income (85.3%, 78.8%; χ2(1) = .07, n.s.). In addition, 23.5% of the ASD group and 7.6% of the TD group reported a pre-existing psychiatric diagnosis (χ2(1) = 5.05, p < 0.05), most frequently ADHD, followed by anxiety and depression. 29.4% of the ASD group and 66.7% of the TD group had post high-school education (χ2(1) = 12.54, p < 0.001). Thus, pre-existing diagnosis and education were controlled for in all relevant statistical analyses.
Measures
Socio-demographic background
This questionnaire comprised a variety of questions assessing factors such as age, education, and income.
PTSD Checklist for DSM-5
The PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013) is a self-report questionnaire comprising the 20 PTSD symptoms in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5), rated on a 0–4 scale (from “not at all” to “extremely”). Participants completed it while referring to a specific event, which they chose as “most distressing” from a comprehensive list of traumatic life events. In the ASD group, the selected event was of social nature (e.g. experiences of bullying, shunning, ridiculing, etc.) in 45.6% of the sample, followed by accidents (14.7%), physical assault (13.2%), sexual assault/harassment (10.3%), a serious medical condition (5.9%), and unexpected death, domestic violence, and other stressful life events (3.1% for each). In the TD group, the selected event was of social nature for 25% of the sample, as well as war/terror (13.3%), unexpected death (11.7%), sexual assault/harassment (11%), physical assault (9.4%), accidents, domestic violence, and serious medical condition (4.7% for each), and other stressful life events (15.5%). The PCL-5 showed excellent internal consistency (Cronbach’s alpha = 0.92).
Rumination Response Scale
The Rumination Response Scale (RSS; Nolen-Hoeksema & Morrow, 1991) is the most common measure of trait ruminative tendencies (Chiu et al., 2018). The RRS consists of 22 items assessing individuals’ coping style when dealing with depressive mood, including the extent to which one repetitively thinks about one’s symptoms, their causes and effects, and the value that one places in such thinking. For each item, the respondent is asked to rate the frequency of thoughts and behaviors at times when he or she experiences negative mood. Items are rated on a 4-point scale (“almost never” to “almost always”) with higher scores representing higher frequency of ruminative thinking. The RRS yields two factors: (1) brooding rumination and (2) reflection rumination. Previous studies have reported very good reliability and structural validity (Nolen-Hoeksema & Morrow, 1991). In the current study, the scale showed excellent internal consistency (Cronbach’s alpha = 0.93).
Community involvement
There is no community involved in this study.
Results
First, an examination of between-group differences in PTSD probable diagnosis rates revealed that the proportion of participants in the ASD group (n = 11, 32.4%) who met the PCL cutoff score of 38 was significantly higher than in the TD group (n = 9, 13.6%; χ2(1) = 4.91, p < 0.05). Figure 1 illustrates these differences.
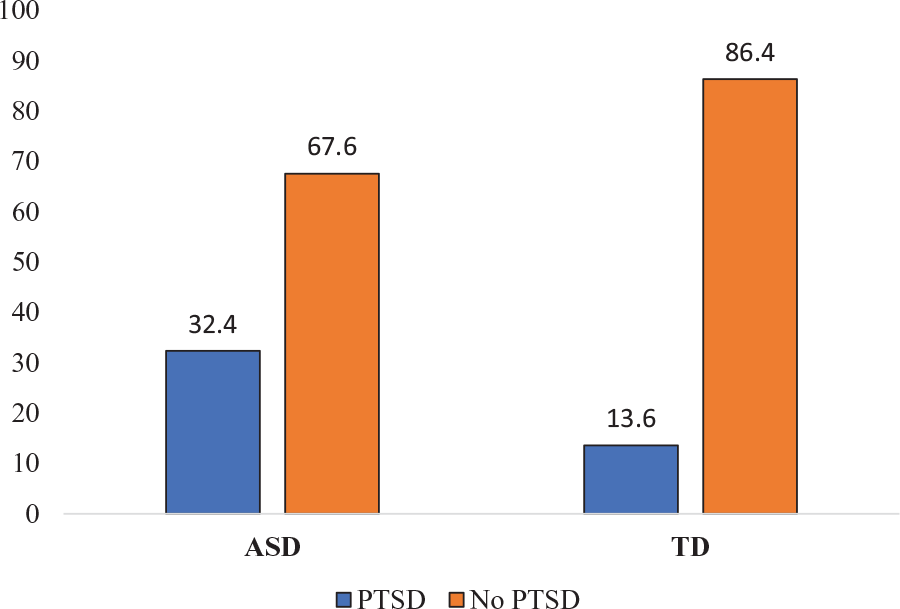
Probable PTSD rates (%) by group.
Next, a multivariate analysis of variance (MANOVA) was conducted, with group (ASD, TD) as the independent variable and rumination (reflection and brooding) scores, as well as PCL-5 scores (total score and four PTSD clusters), as dependent variables. An overall effect for group was found (F(6, 91) = 2.79, p < 0.05, η2 = 0.16). The results of univariate analyses are presented in Table 1.
Group differences in PTSD symptoms and rumination.
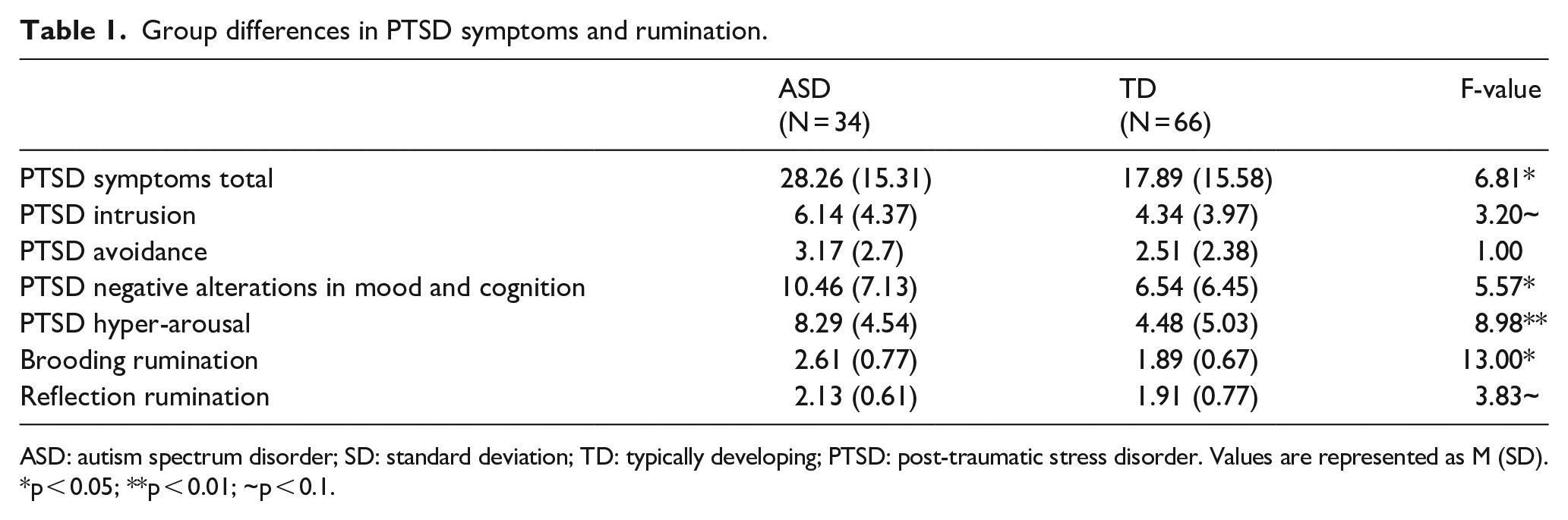
ASD: autism spectrum disorder; SD: standard deviation; TD: typically developing; PTSD: post-traumatic stress disorder. Values are represented as M (SD).
p < 0.05; **p < 0.01; ~p < 0.1.
As shown in Table 1, compared to TD participants, those with ASD reported significantly higher total PTSD scores, as well as higher scores on the PTSD clusters of hyper-arousal and negative alterations in cognition and mood. Marginally significant differences were also found on PTSD intrusion symptoms (p = 0.077). ASD participants also reported higher levels of brooding rumination, as well as marginally significant higher reflection scores (p = 0.053).
Next, bivariate correlations were calculated for rumination scores (brooding, reflection) with Group (ASD/TD) and PCL-5 total score. Brooding rumination was significantly associated with having ASD (r = 0.44, p < 0.01) and with more severe PTSD symptoms (r = 0.55, p < 0.001). Reflection rumination was not significantly associated with having ASD or with PTSD symptoms. Notably, brooding and reflection were positively associated with each other (r = 0.45, p < 0.001).
In addition, a MANOVA was conducted with brooding and reflection rumination as the dependent variables and PCL probable diagnosis (according to a PCL cut off score of 38) as the independent variable. An overall effect was found (F(2, 95)= 8.9, p < 0.001, η2 = 0.16). Univariate analyses revealed a significant effect for brooding rumination (F(1, 96), p < 0.001, η2 = 0.15), with those above the PCL cutoff (n = 20) reporting significantly higher brooding rumination scores (M = 2.73, SD = 0.87) compared to those below the cutoff (n = 80; M = 1.98, SD = 0.68). No significant differences were found for reflection rumination.
For the mediation analysis, Model 4 of the PROCESS macro for SPSS was employed, predicting the PCL-5 total score by Group, with brooding and reflection rumination as the mediators. The predictive model (R2 = 0.33, F(4, 94) = 9.16, p < 0.001) showed a significant effect for Brooding rumination (β = 0.58, p < 0.001) but not for Reflection rumination (β = −0.11, n.s.) or Group (β = 0.20, n.s.). Estimates of the indirect effect for brooding (β = 0.43) had a confidence interval (0.16–0.74) that was significantly greater than zero, indicating that Brooding fully mediated the path between Group and PTSD symptoms (see Figure 2).
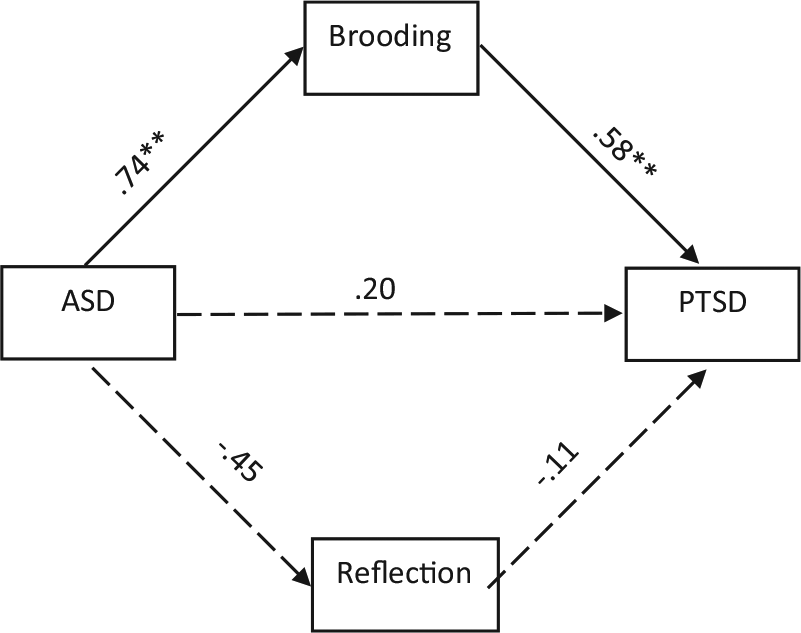
Mediation of ASD-PTSD comorbidity by rumination.
Discussion
This study examined the role of rumination in the ASD-PTSD co-morbidity. We have shown a significantly higher incidence of PTSD, as well as higher levels of some PTSD clusters, among those with ASD. Participants with ASD, as well as participants with a probable PTSD diagnosis, reported increased brooding rumination. In addition, brooding rumination, but not reflection, mediated the association between ASD and PTSD symptoms.
The co-morbidity between ASD and PTSD has gained more attention in both research and clinical practice (Kerns et al., 2020; Rumball, 2019). Research has shown that a wider range of life events may be interpreted as traumatic by adults with ASD and be associated with PTSD symptoms (Rumball et al., 2020), including events of social nature such as bullying and ostracizing (Haruvi-lamdan et al., 2020). However, the psychological mechanisms connecting ASD and PTSD have received little empirical attention (though see Rumball et al., 2021). The finding that brooding rumination mediates the ASD-PTSD association may be attributed to the lack of cognitive flexibility shared by these two disorders. Those with ASD may be more inclined to get “stuck” on repeated thoughts and ideas around traumatic life events, which may increase intrusive memories, hyperarousal, and negative thoughts and feelings (Michael et al., 2007). Furthermore, brooding rumination and cognitive inflexibility may be related to an increased preference for predictability and less tolerance for ambiguity among those with ASD (Fujino et al., 2019). The experience of trauma is inherently characterized by unpredictability and lack of control, conditions which may be particularly burdensome for those with elevated rumination. Interestingly, reflection rumination was not associated with either PTSD or ASD. This is in line with other studies, which have failed to find an association between reflection and psychopathology (Schoofs et al., 2010). Thus, it may be said that while brooding corresponds with the more pathological, intrusive nature of post-traumatic thinking, reflection may represent a more benign, adaptive cognitive coping strategy.
The limitations of this study include a modest sample size, a reliance on self-report measures, and the group differences on educational level, which (although controlled for statistically) may represent group differences unrelated to diagnosis. In addition, our study is cross-sectional. Thus, while we assume that ASD, being the neurodevelopmental disorder, precedes PTSD, our study cannot establish this causality empirically. Furthermore, although psychiatric comorbidity was controlled for in the analysis, it is still possible that undiagnosed anxiety and mood symptoms within the ASD group boosted the levels of some nonspecific PTSD symptoms, for example, from the “negative alterations in mood and cognition” cluster. Individuals with ASD have been shown to suffer from various comorbid disorders, including depression and anxiety (Vannucchi et al 2014). Hence, the possibility of diagnostic overshadowing (Kerns et al., 2015) may account for at least some of our findings and should be further examined. In addition, since rumination is a trans-diagnostic mechanism of psychopathology, and is associated with other disorders beyond PTSD among those with ASD (e.g. depression; see Rumball et al., 2021), future studies are encouraged to assess its unique role in PTSD among this population, while controlling for non-specific effects related to other forms of psychopathology.
These limitations notwithstanding, this study presents a first-of-its-kind examination of possible underlying mechanisms for this co-occurrence of disorders. Brooding rumination should be considered as a target for intervention among traumatized individuals with ASD. Improving cognitive flexibility and attenuating clients’ tendency for repeated thinking may enable better processing of traumatic content and narrative, which in turn would decrease PTSD symptoms (Echiverri et al., 2011). Rumination should be targeted as part of trauma-focused therapy. For example, a metacognitive therapy protocol for PTSD (Wells & Sembi, 2004) specifically aims to eliminate ruminative worrying in order to permit natural processing of traumatic content and a return to more adaptive cognitions. Furthermore, this study highlights the need to distinguish between different types of rumination, as not every pattern of rumination seems to serve as a risk factor for post-traumatic distress among those with ASD. Future studies should expand this line of research, evaluating the ASD-PTSD connection based on longitudinal designs, larger samples, and combinations of research methods (e.g. qualitative, psychobiological). In addition, more studies are needed in order to shed light on the role of other potential psychological mechanisms, which may underly the association between ASD and PTSD. These include, among others, impaired emotion regulation, sensory hyper-sensitivity, and altered social cognition and autobiographical memory (Haruvi-Lamdan et al., 2018).
Footnotes
Acknowledgements
The authors would like to thank Meital Kraus, Shiri Lebendiger, Shani Zohar, and Gal Yedidya for helping with data collection, and the study’s participants for sharing their experiences.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was ethically approved by the Institutional Review Board of Bar-Ilan University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Finkelshtein Fund and The Autism Treatment and Research Center, Association for Children at Risk, Israel.
Informed consent
All participants provided written informed consent.